
Epidemiology and Resistance Phenotypes of Carbapenem-Resistant Klebsiella pneumoniae in Corfu General Hospital (2019–2022): A Comprehensive Time Series Analysis of Resistance Gene Dynamics


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Genotypic and Phenotypic Identification
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
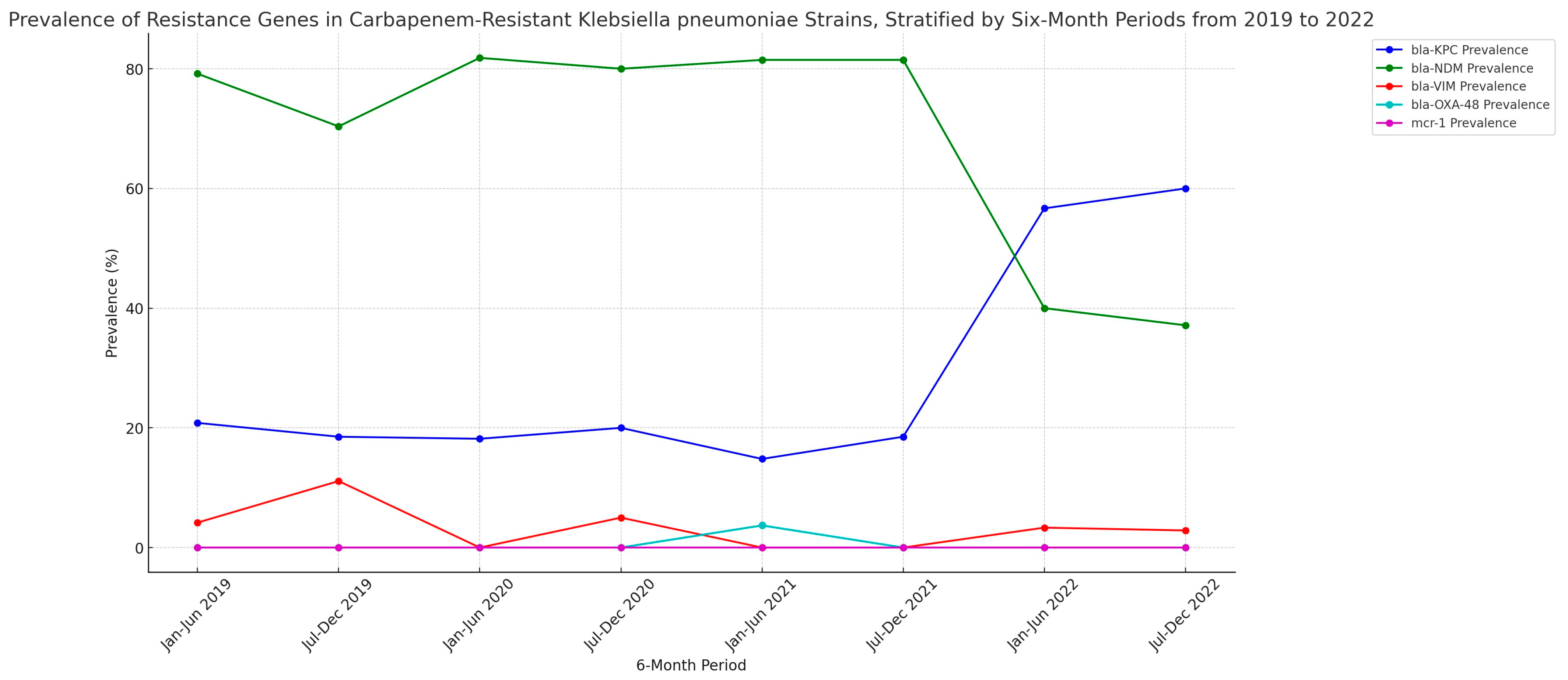
3.2. Prevalence of Resistance Genes (2019–2022)
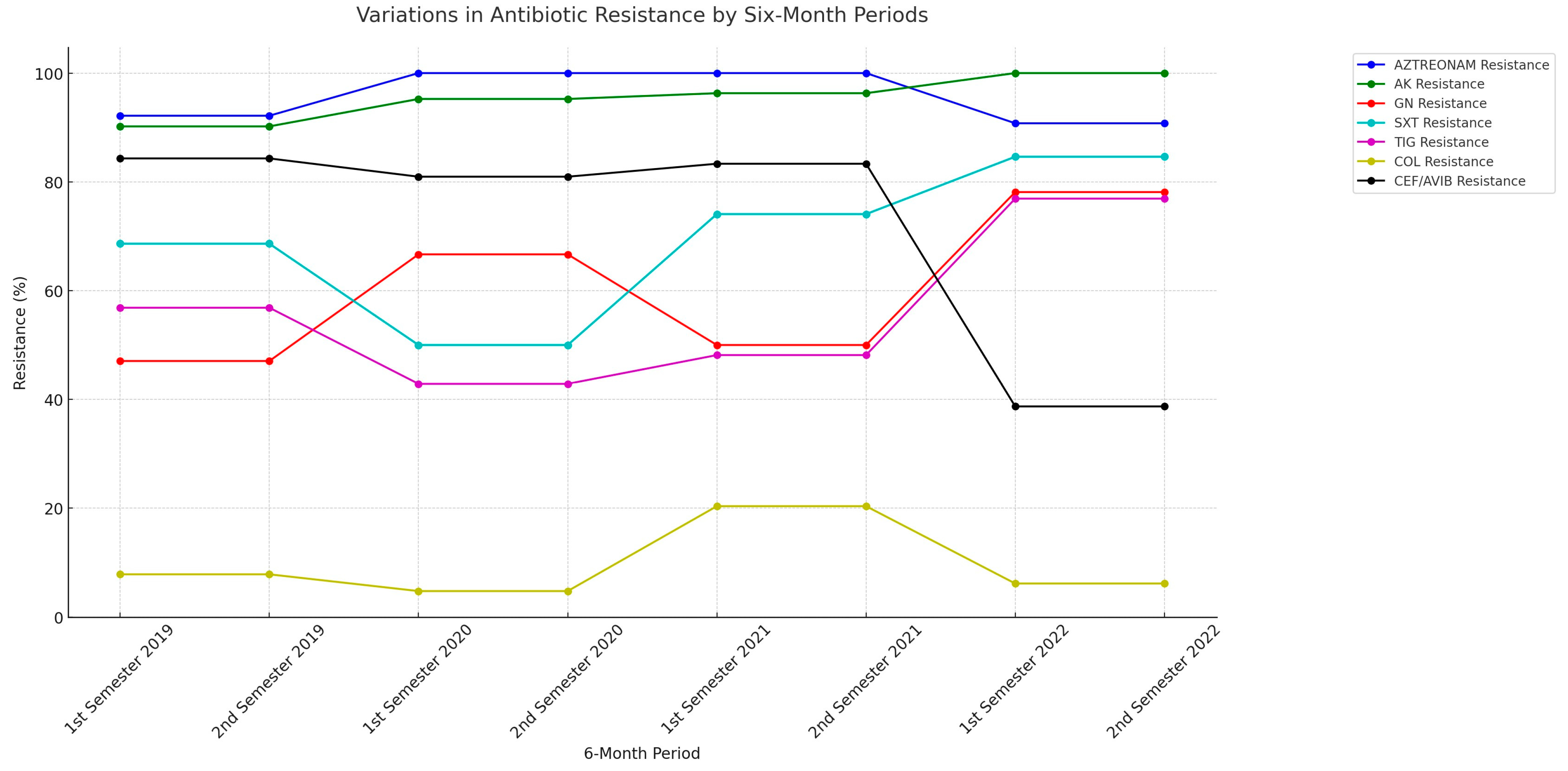
3.3. Antibiotic Resistance Patterns (2019–2022)
3.4. Resistance Genes Patterns (2019–2022)
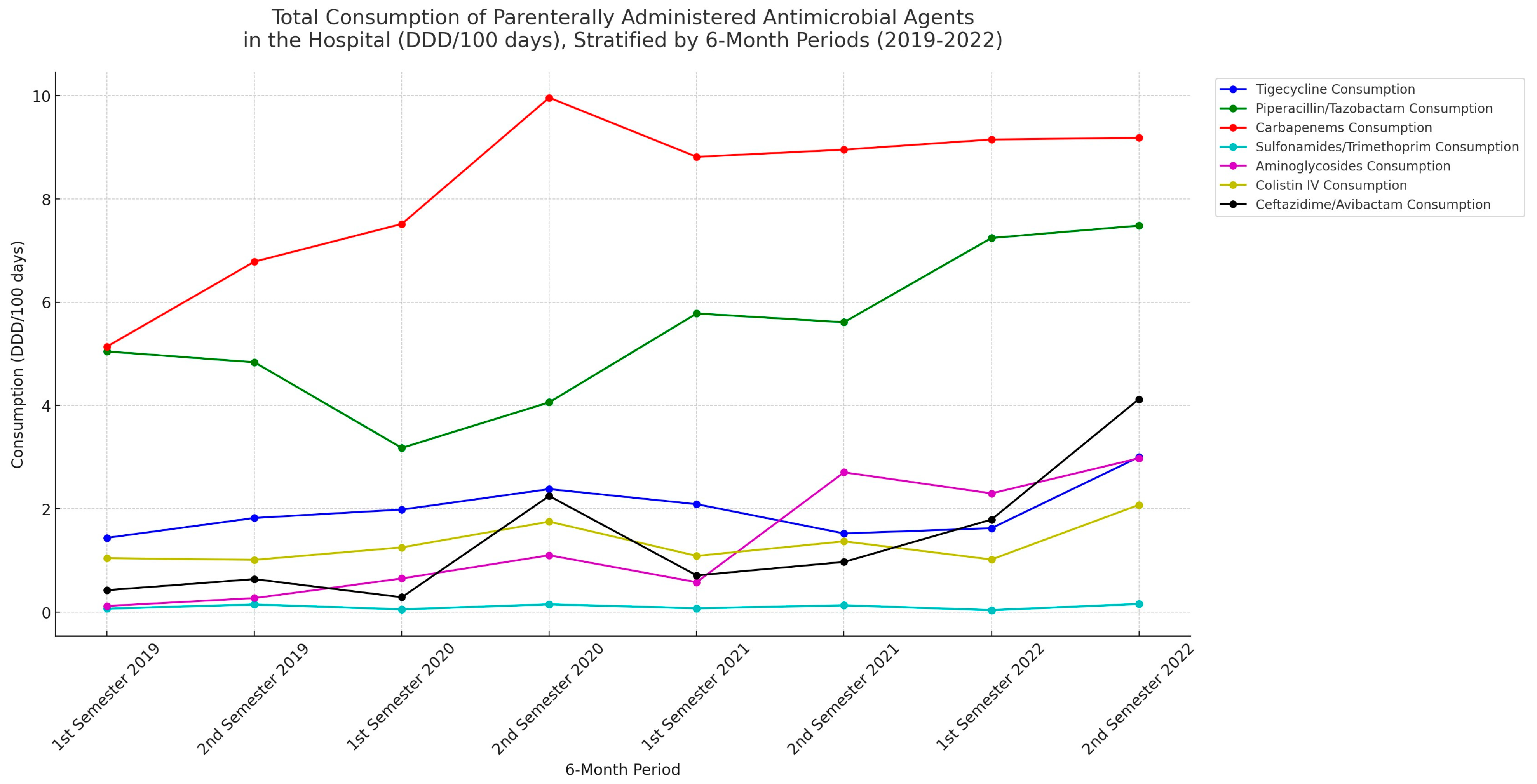
3.5. Antibiotic Consumption Patterns (2019–2022)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Pieri, A.; Aschbacher, R.; Fasani, G.B.; Mariella, J.; Tognetti, R.; Pagani, E.; Sartelli, M.; Pagani, L. Country Income Is Only One of the Tiles: The Global Journey of Antimicrobial Resistance Among Humans, Animals, and Environment. Antibiotics 2020, 9, 473. [Google Scholar] [CrossRef] [PubMed]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, C.; Anjankar, A.; Agrawal, J. Self-Medication with Antibiotics: An Element Increasing Resistance. Cureus 2022, 14, e30844. [Google Scholar] [CrossRef] [PubMed]
- Rossolini, G.M. Multidrug-Resistant and Extremely Drug-Resistant Bacteria: Are We Facing the End of the Antibiotic Era? J. Siena Acad. Sci. 2016, 7. [Google Scholar] [CrossRef]
- Bokhary, H.; Pangesti, K.N.A.; Rashid, H.; Abd El Ghany, M.; Hill-Cawthorne, G.A. Travel-Related Antimicrobial Resistance: A Systematic Review. Trop. Med. Infect. Dis. 2021, 6, 11. [Google Scholar] [CrossRef]
- Chawla, M.; Verma, J.; Gupta, R.; Das, B. Antibiotic Potentiators against Multidrug-Resistant Bacteria: Discovery, Development, and Clinical Relevance. Front. Microbiol. 2022, 13, 887251. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M. Role of Antibiotic Stewardship in Extending the Age of Modern Medicine. S. Afr. Med. J. 2015, 105, 414–418. [Google Scholar] [CrossRef] [PubMed][Green Version]
- van Duin, D.; Perez, F.; Rudin, S.D.; Cober, E.; Hanrahan, J.; Ziegler, J.; Webber, R.; Fox, J.; Mason, P.; Richter, S.S.; et al. Surveillance of carbapenem-resistant Klebsiella pneumoniae: Tracking molecular epidemiology and outcomes through a regional network. Antimicrob. Agents Chemother. 2014, 58, 4035–4041. [Google Scholar] [CrossRef] [PubMed]
- Aanensen, D.M.; Carlos, C.C.; Donado-Godoy, P.; Okeke, I.N.; Ravikumar, K.L. Implementing Whole-Genome Sequencing for Ongoing Surveillance of Antimicrobial Resistance: Exemplifying Insights into Klebsiella pneumoniae. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, S255–S257. [Google Scholar] [CrossRef]
- Fair, R.J.; Tor, Y. Antibiotics and bacterial resistance in the 21st century. Perspect. Med. Chem. 2014, 6, 25–64. [Google Scholar] [CrossRef]
- Tesfa, T.; Mitiku, H.; Edae, M.; Assefa, N. Prevalence and incidence of carbapenem-resistant K. pneumoniae colonization: Systematic review and meta-analysis. Syst. Rev. 2022, 11, 240. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, X.; Wang, J.; Ouyang, P.; Jin, C.; Wang, R.; Zhang, Y.; Jin, L.; Chen, H.; Wang, Z.; et al. Phenotypic and Genotypic Characterization of Carbapenem-resistant Enterobacteriaceae: Data from a Longitudinal Large-scale CRE Study in China (2012–2016). Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 67, S196–S205. [Google Scholar] [CrossRef]
- Xu, L.; Sun, X.; Ma, X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 18. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ma, H.; Huang, X.; Cui, Y.; Peng, W.; Zhu, F.; Ma, S.; Rao, M.; Zhang, P.; Yang, H.; et al. Risk factors and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary-care hospital in China: An eight-year retrospective study. Antimicrob. Resist. Infect. Control. 2022, 11, 161. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.L. The Role of Natural Environments in the Evolution of Resistance Traits in Pathogenic Bacteria. Proc. R. Soc. B Biol. Sci. 2009, 276, 2521–2530. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Bradford, P.A. Epidemiology of β-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33, 10–1128. [Google Scholar] [CrossRef]
- Pitout, J.D.; Nordmann, P.; Poirel, L. Carbapenemase-Producing Klebsiella pneumoniae, a Key Pathogen Set for Global Nosocomial Dominance. Antimicrob. Agents Chemother. 2015, 59, 5873–5884. [Google Scholar] [CrossRef]
- Grundmann, H.; Glasner, C.; Albiger, B.; Aanensen, D.M.; Tomlinson, C.T.; Andrasevic, A.T.; Canton, R.; Carmeli, Y.; Friedrich, A.W.; Giske, C.G.; et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): A prospective, multinational study. Lancet Infect. Dis. 2017, 17, 153–163. [Google Scholar] [CrossRef]
- Vatopoulos, A. High rates of metallo-beta-lactamase-producing Klebsiella pneumoniae in Greece—A review of the current evidence. Eurosurveillance 2008, 13, 7–8. [Google Scholar] [CrossRef]
- Giakkoupi, P.; Papagiannitsis, C.C.; Miriagou, V.; Pappa, O.; Polemis, M.; Tryfinopoulou, K.; Tzouvelekis, L.S.; Vatopoulos, A.C. An update of the evolving epidemic of blaKPC-2-carrying Klebsiella pneumoniae in Greece (2009–10). J. Antimicrob. Chemother. 2011, 66, 1510–1513. [Google Scholar] [CrossRef]
- Souli, M.; Galani, I.; Antoniadou, A.; Papadomichelakis, E.; Poulakou, G.; Panagea, T.; Vourli, S.; Zerva, L.; Armaganidis, A.; Kanellakopoulou, K.; et al. An outbreak of infection due to beta-Lactamase Klebsiella pneumoniae Carbapenemase 2-producing K. pneumoniae in a Greek University Hospital: Molecular characterization, epidemiology, and outcomes. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, E.; Gartzonika, C.; Vrioni, G.; Politi, L.; Priavali, E.; Levidiotou-Stefanou, S.; Tsakris, A. The Balkan region: NDM-1-producing Klebsiella pneumoniae ST11 clonal strain causing outbreaks in Greece. J. Antimicrob. Chemother. 2014, 69, 2091–2097. [Google Scholar] [CrossRef]
- Giakkoupi, P.; Tryfinopoulou, K.; Kontopidou, F.; Tsonou, P.; Golegou, T.; Souki, H.; Tzouvelekis, L.; Miriagou, V.; Vatopoulos, A. Emergence of NDM-producing Klebsiella pneumoniae in Greece. Diagn. Microbiol. Infect. Dis. 2013, 77, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Papagiannitsis, C.C.; Malli, E.; Florou, Z.; Sarrou, S.; Hrabak, J.; Mantzarlis, K.; Zakynthinos, E.; Petinaki, E. Emergence of sequence type 11 Klebsiella pneumoniae coproducing NDM-1 and VIM-1 metallo-beta-lactamases in a Greek hospital. Diagn. Microbiol. Infect. Dis. 2017, 87, 295–297. [Google Scholar] [CrossRef]
- Spyropoulou, A.; Bartzavali, C.; Vamvakopoulou, S.; Marangos, M.; Anastassiou, E.D.; Spiliopoulou, I.; Christofidou, M. The first NDM metallo-beta-lactamase producing Klebsiella pneumoniae isolate in a University Hospital of Southwestern Greece. J. Chemother. 2016, 28, 350–351. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, E.; Zarkotou, O.; Ranellou, K.; Karageorgopoulos, D.E.; Vrioni, G.; Mamali, V.; Themeli-Digalaki, K.; Tsakris, A. Outbreak of OXA-48 carbapenemase-producing Klebsiella pneumoniae in Greece involving an ST11 clone. J. Antimicrob. Chemother. 2013, 68, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, E.; Poulou, A.; Dimitroulia, E.; Politi, L.; Ranellou, K.; Gennimata, V.; Markou, F.; Pournaras, S.; Tsakris, A. Emergence of OXA-162 Carbapenemase- and DHA-1 AmpC Cephalosporinase-Producing Sequence Type 11 Klebsiella pneumoniae Causing Community-Onset Infection in Greece. Antimicrob. Agents Chemother. 2015, 60, 1862–1864. [Google Scholar] [CrossRef]
- Galani, I.; Anagnostoulis, G.; Chatzikonstantinou, M.; Petrikkos, G.; Souli, M. Emergence of Klebsiella pneumoniae co-producing OXA-48, CTX-M-15, and ArmA in Greece. Clin. Microbiol. Infect. 2016, 22, 898–899. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Antimicrobial Resistance Surveillance in Europe 2023. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2023-2021-data (accessed on 30 August 2023).
- Galani, I.; Karaiskos, I.; Karantani, I.; Papoutsaki, V.; Maraki, S.; Papaioannou, V.; Kazila, P.; Tsorlini, H.; Charalampaki, N.; Toutouza, M.; et al. Epidemiology and resistance phenotypes of carbapenemase-producing Klebsiella pneumoniae in Greece, 2014 to 2016. Eurosurveillance 2018, 23, 1700775. [Google Scholar] [CrossRef]
- Protonotariou, E.; Meletis, G.; Pilalas, D.; Mantzana, P.; Tychala, A.; Kotzamanidis, C.; Papadopoulou, D.; Papadopoulos, T.; Polemis, M.; Metallidis, S.; et al. Polyclonal Endemicity of Carbapenemase-Producing Klebsiella pneumoniae in ICUs of a Greek Tertiary Care Hospital. Antibiotics 2022, 11, 149. [Google Scholar] [CrossRef]
- Palacios-Baena, Z.R.; Oteo, J.; Conejo, C.; Larrosa, M.N.; Bou, G.; Fernandez-Martinez, M.; Gonzalez-Lopez, J.J.; Pintado, V.; Martinez-Martinez, L.; Merino, M.; et al. Comprehensive clinical and epidemiological assessment of colonisation and infection due to carbapenemase-producing Enterobacteriaceae in Spain. J. Infect. 2016, 72, 152–160. [Google Scholar] [CrossRef]
- Kaase, M.; Schimanski, S.; Schiller, R.; Beyreiss, B.; Thurmer, A.; Steinmann, J.; Kempf, V.A.; Hess, C.; Sobottka, I.; Fenner, I.; et al. Multicentre investigation of carbapenemase-producing Escherichia coli and Klebsiella pneumoniae in German hospitals. Int. J. Med. Microbiol. 2016, 306, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.D.; Bogaerts, P.; Berhin, C.; Hoebeke, M.; Bauraing, C.; Glupczynski, Y.; a multicentre study group. Increasing proportion of carbapenemase-producing Enterobacteriaceae and emergence of a MCR-1 producer through a multicentric study among hospital-based and private laboratories in Belgium from September to November 2015. Eurosurveillance 2017, 22, 30530. [Google Scholar] [CrossRef]
- Dortet, L.; Cuzon, G.; Ponties, V.; Nordmann, P. Trends in carbapenemase-producing Enterobacteriaceae, France, 2012 to 2014. Eurosurveillance 2017, 22, 30461. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Giamarellou, H. Multidrug-resistant and extensively drug-resistant Gram-negative pathogens: Current and emerging therapeutic approaches. Expert Opin. Pharmacother. 2014, 15, 1351–1370. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Giske, C.G.; Gramatniece, A.; Abodakpi, H.; Tam, V.H.; Leibovici, L. New beta-Lactam-beta-Lactamase Inhibitor Combinations. Clin. Microbiol. Rev. 2020, 34, 10–1128. [Google Scholar] [CrossRef]
- Wright, H.; Bonomo, R.A.; Paterson, D.L. New agents for the treatment of infections with Gram-negative bacteria: Restoring the miracle or false dawn? Clin. Microbiol. Infect. 2017, 23, 704–712. [Google Scholar] [CrossRef]
- Karaiskos, I.; Daikos, G.L.; Gkoufa, A.; Adamis, G.; Stefos, A.; Symbardi, S.; Chrysos, G.; Filiou, E.; Basoulis, D.; Mouloudi, E.; et al. Ceftazidime/avibactam in the era of carbapenemase-producing Klebsiella pneumoniae: Experience from a national registry study. J. Antimicrob. Chemother. 2021, 76, 775–783. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Lambropoulou, A.; Solomou, A.; Tsiata, E.; Anastassiou, E.D.; Fligou, F.; Marangos, M.; Spiliopoulou, I.; Christofidou, M. Reversal of carbapenemase-producing Klebsiella pneumoniae epidemiology from blaKPC- to blaVIM-harbouring isolates in a Greek ICU after introduction of ceftazidime/avibactam. J. Antimicrob. Chemother. 2019, 74, 2051–2054. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Karachalias, E.; Spiliopoulou, A.; Tsiata, E.; Siakallis, G.; Assimakopoulos, S.F.; Kolonitsiou, F.; Marangos, M. A Seven-Year Microbiological and Molecular Study of Bacteremias Due to Carbapenemase-Producing Klebsiella pneumoniae: An Interrupted Time-Series Analysis of Changes in the Carbapenemase Gene’s Distribution after Introduction of Ceftazidime/Avibactam. Antibiotics 2022, 11, 1414. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Kontopidou, F.; Dedoukou, X.; Katerelos, P.; Gourgoulis, G.M.; Tsonou, P.; Maragos, A.; Gargalianos, P.; Gikas, A.; Gogos, C.; et al. Action Plan to combat infections due to carbapenem-resistant, Gram-negative pathogens in acute-care hospitals in Greece. J. Glob. Antimicrob. Resist. 2014, 2, 11–16. [Google Scholar] [CrossRef]
- Polemis, M.; Mandilara, G.; Pappa, O.; Argyropoulou, A.; Perivolioti, E.; Koudoumnakis, N.; Pournaras, S.; Vasilakopoulou, A.; Vourli, S.; Katsifa, H.; et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance-WHONET-Greece (January 2018–March 2021). Life 2021, 11, 996. [Google Scholar] [CrossRef] [PubMed]
- Galani, I.; Nafplioti, K.; Adamou, P.; Karaiskos, I.; Giamarellou, H.; Souli, M.; Study, C. Nationwide epidemiology of carbapenem resistant Klebsiella pneumoniae isolates from Greek hospitals, with regards to plazomicin and aminoglycoside resistance. BMC Infect. Dis. 2019, 19, 167. [Google Scholar] [CrossRef]
- Köser, C.U.; Ellington, M.J.; Peacock, S.J. Whole-genome sequencing to control antimicrobial resistance. Trends Genet. TIG 2014, 30, 401–407. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Department, n (%) | |
| Medical | 161 (76) |
| ICU | 26 (12.2) |
| Surgical | 25 (11.8) |
| Male sex, n (%) | 100 (47.2) |
| Age, median (IQR) | 81 (72–88) |
| Type of samples, n (%) | |
| BAL | 11 (5.2) |
| CVC | 5 (2.4) |
| Rectal swab | 12 (5.6) |
| Sputum | 7 (3.3) |
| Trauma | 8 (3.7) |
| Urine | 154 (72.6) |
| Other | 15 (7.2) |
| Positive BCx, n (%) | 55 (25.9) |
| Comorbidities, n (%) | |
| CAD | 14 (6.6) |
| CKD | 6 (2.8) |
| CVA | 10 (4.7) |
| DM | 22 (10.4) |
| Hypertension | 17 (8) |
| HF | 5 (2.3) |
| Cancer | 9 (4.2) |
| Recent Hospitalization, n (%) | 48 (22.6) |
| Death, n (%) | 28 (13.2) |
| Year Cx obtained | |
| 2019 | 51 (24) |
| 2020 | 42 (19.8) |
| 2021 | 54 (25.6) |
| 2022 | 65 (30.6) |
| Collection Year | bla-KPC | bla-NDM | bla-VIM | bla-OXA-48 | mcr-1 |
|---|---|---|---|---|---|
| 2019 | 10 (19.61%) | 38 (74.51%) | 4 (7.84%) | 0 (0.0%) | 0 (0.0%) |
| 2020 | 8 (19.05%) | 34 (80.95%) | 1 (2.38%) | 0 (0.0%) | 0 (0.0%) |
| 2021 | 9 (16.67%) | 44 (81.48%) | 0 (0.0%) | 1 (1.85%) | 0 (0.0%) |
| 2022 | 38 (58.46%) | 25 (38.46%) | 2 (3.08%) | 0 (0.0%) | 0 (0.0%) |
| Antibiotic | Year | bla-KPC (%) | bla-NDM (%) | bla-OXA-48 (%) |
|---|---|---|---|---|
| AK Resistance | 2019 (n = 51) | 17.6 | 66.7 | 0.0 |
| 2020 (n = 42) | 16.7 | 78.6 | 0.0 | |
| 2021 (n = 54) | 16.7 | 77.8 | 1.9 | |
| 2022 (n = 65) | 58.5 | 38.5 | 0.0 | |
| Aztreonam Resistance | 2019 (n = 51) | 19.6 | 66.7 | 0.0 |
| 2020 (n = 42) | 19.0 | 81.0 | 0.0 | |
| 2021 (n = 54) | 16.7 | 81.5 | 1.9 | |
| 2022 (n = 65) | 58.5 | 29.2 | 0.0 | |
| CEF/AVIB Resistance | 2019 (n = 51) | 3.9 | 74.5 | 0.0 |
| 2020 (n = 42) | 2.4 | 78.6 | 0.0 | |
| 2021 (n = 54) | 0.0 | 81.5 | 1.9 | |
| 2022 (n = 65) | 0.0 | 33.8 | 0.0 | |
| COL Resistance | 2019 (n = 51) | 2.0 | 5.9 | 0.0 |
| 2020 (n = 42) | 0.0 | 4.8 | 0.0 | |
| 2021 (n = 54) | 7.4 | 13.0 | 0.0 | |
| 2022 (n = 65) | 3.1 | 3.1 | 0.0 | |
| GN Resistance | 2019 (n = 51) | 5.9 | 35.3 | 0.0 |
| 2020 (n = 42) | 2.4 | 64.3 | 0.0 | |
| 2021 (n = 54) | 11.1 | 38.9 | 0.0 | |
| 2022 (n = 65) | 49.2 | 24.6 | 0.0 | |
| SXT Resistance | 2019 (n = 51) | 9.8 | 52.9 | 0.0 |
| 2020 (n = 42) | 16.7 | 33.3 | 0.0 | |
| 2021 (n = 54) | 14.8 | 59.3 | 0.0 | |
| 2022 (n = 65) | 52.3 | 30.8 | 0.0 | |
| TIG Resistance | 2019 (n = 51) | 9.8 | 41.2 | 0.0 |
| 2020 (n = 42) | 9.5 | 33.3 | 0.0 | |
| 2021 (n = 54) | 11.1 | 37.0 | 0.0 | |
| 2022 (n = 65) | 43.1 | 32.3 | 0.0 |
| Antimicrobial Agents | 1st Semester 2019 | 2nd Semester 2019 | 1st Semester 2020 | 2nd Semester 2020 | 1st Semester 2021 | 2nd Semester 2021 | 1st Semester 2022 | 2nd Semester 2022 |
|---|---|---|---|---|---|---|---|---|
| Τigecycline | 1.438 | 1.823 | 1.985 | 2.381 | 2.090 | 1.523 | 1.625 | 3.001 |
| Piperacillin/Tazobactam | 5.047 | 4.838 | 3.179 | 4.062 | 5.781 | 5.612 | 7.243 | 7.482 |
| Monobactams/Aztreonam | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Carbapenems (Meropenem, Ertapenem, Doripenem, Imipenem) | 5.141 | 6.785 | 7.515 | 9.960 | 8.814 | 8.953 | 9.150 | 9.182 |
| Sulfonamides/Trimethoprim | 0.067 | 0.146 | 0.054 | 0.149 | 0.074 | 0.130 | 0.039 | 0.156 |
| Macrolides (Erythromycin, Clarithromycin, Azithromycin) | 0.914 | 0.947 | 1.582 | 1.873 | 0.565 | 0.371 | 0.655 | 0.274 |
| Clindamycin | 3.031 | 3.250 | 2.655 | 3.422 | 3.558 | 3.801 | 3.453 | 4.681 |
| Aminoglycosides (Streptomycin, Amikacin, Gentamicin, Tobramycin) | 0.118 | 0.271 | 0.651 | 1.101 | 0.579 | 2.706 | 2.298 | 2.979 |
| Quinolones (Ciprofloxacin, Levofloxacin, Ofloxacin, Moxifloxacin) | 7.410 | 4.978 | 7.731 | 7.141 | 6.512 | 11.542 | 10.474 | 3.872 |
| Glycopeptides (Vancomycin, Teicoplanin, Dalbavancin) | 2.891 | 3.988 | 4.736 | 3.374 | 4.007 | 4.297 | 4.816 | 4.975 |
| Colistin IV | 1.045 | 1.012 | 1.253 | 1.752 | 1.088 | 1.370 | 1.019 | 2.076 |
| Linezolid-Tedizolid | 1.132 | 1.083 | 1.288 | 1.194 | 1.422 | 1.255 | 1.327 | 1.189 |
| Ceftolozane/Tazobactam | 0.620 | 0.446 | 0.571 | 1.854 | 0 | 0 | 0.554 | 1.156 |
| Ceftazidime/Avibactam | 0.425 | 0.639 | 0.288 | 2.248 | 0.710 | 0.971 | 1.792 | 4.123 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorovou, G.; Schinas, G.; Pasxali, A.; Tzoukmani, A.; Tryfinopoulou, K.; Gogos, C.; Dimopoulos, G.; Akinosoglou, K. Epidemiology and Resistance Phenotypes of Carbapenem-Resistant Klebsiella pneumoniae in Corfu General Hospital (2019–2022): A Comprehensive Time Series Analysis of Resistance Gene Dynamics. Microorganisms 2023, 11, 2537. https://doi.org/10.3390/microorganisms11102537
Sorovou G, Schinas G, Pasxali A, Tzoukmani A, Tryfinopoulou K, Gogos C, Dimopoulos G, Akinosoglou K. Epidemiology and Resistance Phenotypes of Carbapenem-Resistant Klebsiella pneumoniae in Corfu General Hospital (2019–2022): A Comprehensive Time Series Analysis of Resistance Gene Dynamics. Microorganisms. 2023; 11(10):2537. https://doi.org/10.3390/microorganisms11102537
Chicago/Turabian StyleSorovou, Glykeria, Georgios Schinas, Aggeliki Pasxali, Angeliki Tzoukmani, Kyriaki Tryfinopoulou, Charalambos Gogos, George Dimopoulos, and Karolina Akinosoglou. 2023. "Epidemiology and Resistance Phenotypes of Carbapenem-Resistant Klebsiella pneumoniae in Corfu General Hospital (2019–2022): A Comprehensive Time Series Analysis of Resistance Gene Dynamics" Microorganisms 11, no. 10: 2537. https://doi.org/10.3390/microorganisms11102537
APA StyleSorovou, G., Schinas, G., Pasxali, A., Tzoukmani, A., Tryfinopoulou, K., Gogos, C., Dimopoulos, G., & Akinosoglou, K. (2023). Epidemiology and Resistance Phenotypes of Carbapenem-Resistant Klebsiella pneumoniae in Corfu General Hospital (2019–2022): A Comprehensive Time Series Analysis of Resistance Gene Dynamics. Microorganisms, 11(10), 2537. https://doi.org/10.3390/microorganisms11102537