
Development of a Built Environment–Self-Efficacy–Activity Engagement–Self-Rated Health Model for Older Adults in Urban Residential Areas


Abstract
1. Introduction
2. Literature Review
2.1. Built Environment for Active and Healthy Aging
2.2. Older People’s Self-Efficacy for Daily Activity
2.3. Features of Older People’s Activity Engagement
2.4. Older People’s Self-Rated Health
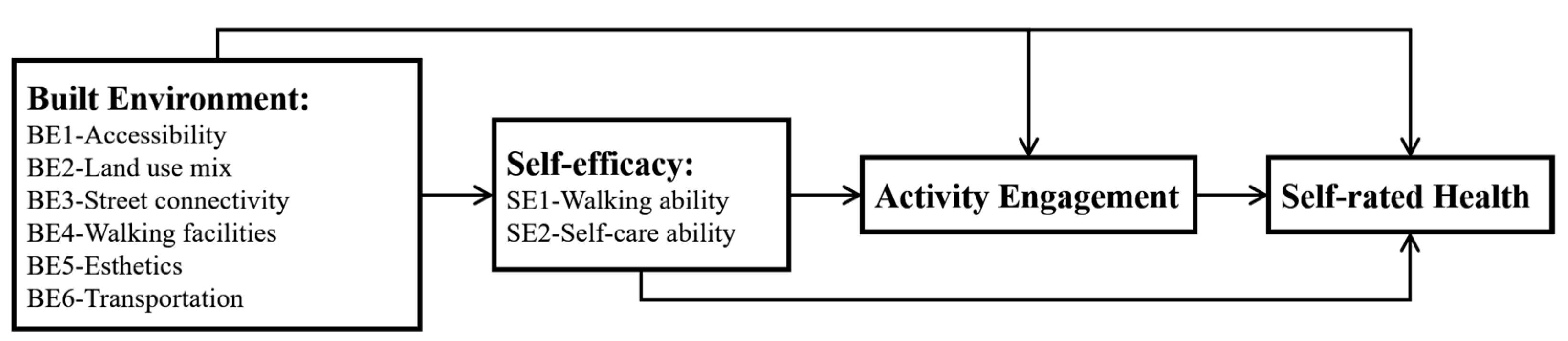
3. Conceptual Model
4. Research Methodology
4.1. Questionnaire Survey
4.2. Sample
4.3. Statistical Analysis Methods
5. Results
5.1. Factor Analysis and Reliability Test
5.2. Spearman Correlation Analysis
5.3. Hierarchical Regression Analysis
5.4. Model Establishment
6. Discussion
6.1. Effect of BE on Self-Efficacy
6.2. Effect of BE and Self-Efficacy on Activity Engagement
6.3. Effect of BE, Self-Efficacy, and Activity Engagement on Self-Rated Health
7. Recommendations
7.1. Practical Recommendations
7.2. Research Limitations and Future Study
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grinin, L.; Grinin, A.; Korotayev, A. Global aging: An integral problem of the future. How to turn a problem into a development driver? In Reconsidering the Limits to Growth: A Report to the Russian Association of the Club of Rome; Springer: Berlin/Heidelberg, Germany, 2023; pp. 117–135. [Google Scholar]
- Elnagar, E.; Düvier, C.; Batra, Z.; Christoffersen, J.; Mandin, C.; Schweiker, M.; Wargocki, P.J. Creating a comprehensive framework for design, construction and management of healthy buildings. Energy Build. 2024, 324, 114883. [Google Scholar] [CrossRef]
- Gu, T.; Li, D.; Li, L. The Elderly’s Demand for Community-Based Care Services and Its Determinants: A Comparison of the Elderly in the Affordable Housing Community and Commercial Housing Community of China. J. Healthc. Eng. 2020, 2020, 1840543. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.-C.; Lin, Y.-C.; Hung, C.-H.; Chen, B. Enhancing resilience in ageing: The role of age-friendly community and individual health in reducing seismic risk. Int. J. Disaster Risk Reduct. 2024, 111, 104733. [Google Scholar] [CrossRef]
- Ren, Z.; Nikolopoulou, M.; Mills, G.; Pilla, F. Evaluating the influence of urban trees and microclimate on residential energy consumption in Dublin neighbourhoods. Build. Environ. 2025, 269, 112441. [Google Scholar] [CrossRef]
- OECD. Ageing in Cities. Available online: https://doi.org/10.1787/9789264231160-en (accessed on 30 April 2015).
- Qi, X.; Li, Y.; Hu, J.; Meng, L.; Zeng, P.; Shi, J.; Jia, N.; Zeng, X.; Li, H.; Zhang, Q.; et al. Prevalence of social frailty and its associated factors in the older Chinese population: A national cross-sectional study. BMC Geriatr. 2023, 23, 532. [Google Scholar] [CrossRef]
- Xu, T.; Huang, Z.; Li, B.; Jin, H.; Zhang, J.; Yang, H.; Huang, Y.; Zhang, X.; Chen, C. Association between home and community-based services utilization and self-rated health among Chinese older adults with chronic diseases: Evidence from the 2018 China Health and Retirement Longitudinal Study. BMC Public. Health 2024, 24, 117. [Google Scholar] [CrossRef]
- Fernández-Jiménez, C.; Dumitrache, C.G.; Rubio, L.; Ruiz-Montero, P. Self-perceptions of ageing and perceived health status: The mediating role of cognitive functioning and physical activity. Ageing Soc. 2024, 44, 622–641. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Coulthard-Morris, L.; Zeng, Q.; Retzlaff, P. Measuring self-efficacy in people with multiple scleoris: A validation study. Arch. Phys. Med. Rehabil. 1996, 77, 394–398. [Google Scholar] [CrossRef]
- World Health Organization. Global Age-Friendly Cities: A Guide. 2007. Available online: https://www.who.int/publications/i/item/9789241547307 (accessed on 5 October 2007).
- Shi, J.; Liu, X.; Feng, Z. Age-friendly cities and communities and cognitive health among Chinese older adults: Evidence from the China Health and Retirement Longitudinal Studies. Cites 2023, 132, 104072. [Google Scholar] [CrossRef]
- Van Hoof, J.; Marston, H.R.; Kazak, J.K.; Buffel, T. Ten questions concerning age-friendly cities and communities and the built environment. Build. Environ. 2021, 199, 107922. [Google Scholar] [CrossRef]
- Brownson, R.C.; Hoehner, C.M.; Day, K.; Forsyth, A.; Sallis, J.F. Measuring the built environment for physical activity: State of the science. Am. J. Prev. Med. 2009, 36, S99–S123.e112. [Google Scholar] [CrossRef] [PubMed]
- Farmer, H.; Xu, H.; Dupre, M.E. Self-efficacy. In Encyclopedia of Gerontology and Population Aging; Springer: Berlin/Heidelberg, Germany, 2022; pp. 4410–4413. [Google Scholar] [CrossRef]
- Handy, S.L.; Boarnet, M.G.; Ewing, R.; Killingsworth, R.E. How the built environment affects physical activity: Views from urban planning. Am. J. Prev. Med. 2002, 23, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Seyedrezaei, M.; Becerik-Gerber, B.; Awada, M.; Contreras, S.; Boeing, G. Equity in the built environment: A systematic review. Build. Environ. 2023, 245, 110827. [Google Scholar] [CrossRef]
- Zheng, Z.; Liu, W.; Lu, Y.; Sun, N.; Chu, Y.; Chen, H. The influence mechanism of community-built environment on the health of older adults: From the perspective of low-income groups. BMC Geriatr. 2022, 22, 590. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, J. A Study on the Influence of an Outdoor Built Environment on the Activity Behavior of the Elderly in Small Cities in Cold Regions—A Case Study of Bei’an City. Sustainability 2025, 17, 2260. [Google Scholar] [CrossRef]
- World Health Organization. National Programmes for Age-Friendly Cities and Communities: A Guide. 2023. Available online: https://www.who.int/publications/i/item/9789240068698 (accessed on 19 April 2023).
- Cerin, E.; Saelens, B.E.; Sallis, J.F.; Frank, L.D. Neighborhood Environment Walkability Scale: Validity and development of a short form. Med. Sci. Sports Exerc. 2006, 38, 1682. [Google Scholar] [CrossRef]
- Carlsson, G.; Slaug, B.; Schmidt, S.; Norin, L.; Ronchi, E.; Gefenaite, G. A scoping review of public building accessibility. Disabil. Health J. 2022, 15, 101227. [Google Scholar] [CrossRef]
- Mitropoulos, L.; Karolemeas, C.; Tsigdinos, S.; Vassi, A.; Bakogiannis, E. A composite index for assessing accessibility in urban areas: A case study in Central Athens, Greece. J. Transp. Geogr. 2023, 108, 103566. [Google Scholar] [CrossRef]
- P Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef]
- Guo, B.; Zhang, L.; Li, Y. Research on the path of residents’ willingness to upgrade by installing elevators in old residential quarters based on safety precautions. Saf. Sci. 2019, 118, 389–396. [Google Scholar] [CrossRef]
- Hartblay, C. Good ramps, bad ramps: Centralized design standards and disability access in urban Russian infrastructure. Am. Ethnol. 2017, 44, 9–22. [Google Scholar] [CrossRef]
- Noordzij, J.M.; Beenackers, M.; Groeniger, J.O.; Timmermans, E.; Motoc, I.; Huisman, M.; Van Lenthe, F.; Activity, P. Land use mix and physical activity in middle-aged and older adults: A longitudinal study examining changes in land use mix in two Dutch cohorts. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Barnett, A.; Shaw, J.E.; Martino, E.; Knibbs, L.D.; Tham, R.; Wheeler, A.J.; Anstey, K.J. Urban neighbourhood environments, cardiometabolic health and cognitive function: A national cross-sectional study of middle-aged and older adults in Australia. Toxics 2022, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Maresova, P.; Krejcar, O.; Maskuriy, R.; Bakar, N.A.A.; Selamat, A.; Truhlarova, Z.; Horak, J.; Joukl, M.; Vítkova, L. Challenges and opportunity in mobility among older adults–key determinant identification. BMC Geriatr. 2023, 23, 447. [Google Scholar] [CrossRef]
- Liu, J.; Wang, B.; Xiao, L. Non-linear associations between built environment and active travel for working and shopping: An extreme gradient boosting approach. J. Transp. Geogr. 2021, 92, 103034. [Google Scholar] [CrossRef]
- Jia, P.; Zou, Y.; Wu, Z.; Zhang, D.; Wu, T.; Smith, M.; Xiao, Q. Street connectivity, physical activity, and childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e12943. [Google Scholar] [CrossRef]
- Song, S.; Yap, W.; Hou, Y.; Yuen, B. Neighbourhood built Environment, physical activity, and physical health among older adults in Singapore: A simultaneous equations approach. J. Transp. Health 2020, 18, 100881. [Google Scholar] [CrossRef]
- Xu, L.; Han, H.; Yang, C.; Liu, Q.J.S. The influence mechanism of the community subjectively built environment on the physical and mental health of older adults. Sustainability 2023, 15, 13211. [Google Scholar] [CrossRef]
- Chen, Y.-R.; Hanazato, M.; Koga, C.; Ide, K.; Kondo, K. The association between street connectivity and depression among older Japanese adults: The JAGES longitudinal study. Sci. Rep. 2022, 12, 13533. [Google Scholar] [CrossRef]
- Boakye, K.; Bovbjerg, M.; Schuna Jr, J.; Branscum, A.; Mat-Nasir, N.; Bahonar, A.; Barbarash, O.; Yusuf, R.; Lopez-Jaramillo, P.; Seron, P. Perceived built environment characteristics associated with walking and cycling across 355 communities in 21 countries. Cities 2023, 132, 104102. [Google Scholar] [CrossRef]
- Dogra, S.; Dunstan, D.W.; Sugiyama, T.; Stathi, A.; Gardiner, P.A.; Owen, N. Active aging and public health: Evidence, implications, and opportunities. Annu. Rev. Public. Health 2022, 43, 439–459. [Google Scholar] [CrossRef] [PubMed]
- Brady, E.; Prior, J. Environmental aesthetics: A synthetic review. People Nat. 2020, 2, 254–266. [Google Scholar] [CrossRef]
- Shen, J.; Fan, J.; Wu, S.; Xu, X.; Fei, Y.; Liu, Z.; Xiong, S. A Study on the Impact of a Community Green Space Built Environment on Physical Activity in Older People from a Health Perspective: A Case Study of Qingshan District, Wuhan. Sustainability 2025, 17, 263. [Google Scholar] [CrossRef]
- Inoue, T.; Manabe, R.; Murayama, A.; Koizumi, H. People–Place Relationships in Regenerative Urban Assemblages: Streetscape Composition and Subjective Well-Being of Older Adults. Land 2025, 14, 680. [Google Scholar] [CrossRef]
- Mercader-Moyano, P.; Flores-García, M.; Serrano-Jiménez, A. Housing and neighbourhood diagnosis for ageing in place: Multidimensional Assessment System of the Built Environment (MASBE). Sustain. Cities Soc. 2020, 62, 102422. [Google Scholar] [CrossRef]
- Yang, Y.; Sasaki, K.; Cheng, L.; Tao, S. Does the built environment matter for active travel among older adults: Insights from Chiba City, Japan. J. Transp. Geogr. 2022, 101, 103338. [Google Scholar] [CrossRef]
- Dabelko-Schoeny, H.; Maleku, A.; Cao, Q.; White, K.; Ozbilen, B. “We want to go, but there are no options”: Exploring barriers and facilitators of transportation among diverse older adults. J. Transp. Health 2021, 20, 100994. [Google Scholar] [CrossRef]
- Aghabayk, K.; Esmailpour, J.; Jafari, A.; Shiwakoti, N. Observational-based study to explore pedestrian crossing behaviors at signalized and unsignalized crosswalks. Accid. Anal. Prev. 2021, 151, 105990. [Google Scholar] [CrossRef]
- Bendak, S.; Alnaqbi, A.M.; Alzarooni, M.Y.; Aljanaahi, S.M.; Alsuwaidi, S.J. Factors affecting pedestrian behaviors at signalized crosswalks: An empirical study. J. Safety Res. 2021, 76, 269–275. [Google Scholar] [CrossRef]
- Duncan, M.; Torres, Y.V.; Gladwin, K.; Horner, M.; Wood, B. Transit-oriented development for older adults. J. Transp. Land. Use 2021, 14, 255–276. [Google Scholar] [CrossRef]
- Cervone, D.; Shadel, W.G.; Jencius, S. Social-cognitive theory of personality assessment. Pers. Soc. Psychol. Rev. 2001, 5, 33–51. [Google Scholar] [CrossRef]
- Leung, M.-Y.; Wang, C.; Famakin, I.O. Integrated model for indoor built environment and cognitive functional ability of older residents with dementia in care and attention homes. Build. Environ. 2021, 195, 107734. [Google Scholar] [CrossRef]
- Schwarzer, R.; Hallum, S. Perceived teacher self-efficacy as a predictor of job stress and burnout: Mediation analyses. Appl. Psychol. 2008, 57, 152–171. [Google Scholar] [CrossRef]
- Tadaka, E.; Kono, A.; Ito, E.; Kanaya, Y.; Dai, Y.; Imamatsu, Y.; Itoi, W. Development of a community’s self-efficacy scale for preventing social isolation among community-dwelling older people (Mimamori Scale). BMC Public. Health 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; De Vos, J.; Zhao, P.; Yang, M.; Witlox, F. Examining non-linear built environment effects on elderly’s walking: A random forest approach. Transp. Res. D Transp. Environ. 2020, 88, 102552. [Google Scholar] [CrossRef]
- Kikkert, L.H.; Vuillerme, N.; van Campen, J.P.; Hortobágyi, T.; Lamoth, C.J. Walking ability to predict future cognitive decline in old adults: A scoping review. Ageing Res. Rev. 2016, 27, 1–14. [Google Scholar] [CrossRef]
- Prescott, M.; Labbé, D.; Miller, W.C.; Borisoff, J.; Feick, R.; Mortenson, W.B. Factors that affect the ability of people with disabilities to walk or wheel to destinations in their community: A scoping review. Transp. Rev. 2020, 40, 646–669. [Google Scholar] [CrossRef]
- Lisko, I.; Kulmala, J.; Annetorp, M.; Ngandu, T.; Mangialasche, F.; Kivipelto, M. How can dementia and disability be prevented in older adults: Where are we today and where are we going? J. Int. Med. 2021, 289, 807–830. [Google Scholar] [CrossRef]
- Guo, Y.; Wang, T.; Ge, T.; Jiang, Q. Prevalence of self-care disability among older adults in China. BMC Geriatr. 2022, 22, 775. [Google Scholar] [CrossRef]
- Chica-Pérez, A.; Dobarrio-Sanz, I.; Correa-Casado, M.; Fernández-Sola, C.; Ruiz-Fernández, M.D.; Hernández-Padilla, J.M. Spanish version of the self-care self-efficacy scale: A validation study in community-dwelling older adults with chronic multimorbidity. Geriatr. Nurs. 2023, 53, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Yap, X.Y.; Wai San Wilson, T.; Tan, Y.Q.; Yanhong, D.; Loh, L.X.; Tan, P.C.; Peiying, G.; Zhang, D.; Wu, X.V. Path analysis of self-care amongst community-dwelling pre-ageing and older adults with chronic diseases: A salutogenic model. Geriatr. Nurs. 2024, 59, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Zhong, S.; Lee, C.; Foster, M.J.; Bian, J. Intergenerational communities: A systematic literature review of intergenerational interactions and older adults’ health-related outcomes. Soc. Sci. Med. 2020, 264, 113374. [Google Scholar] [CrossRef] [PubMed]
- Eckstrom, E.; Neukam, S.; Kalin, L.; Wright, J. Physical activity and healthy aging. Clin. Geriatr. Med. 2020, 36, 671–683. [Google Scholar] [CrossRef]
- Benedyk, A.; Reichert, M.; Giurgiu, M.; Timm, I.; Reinhard, I.; Nigg, C.; Berhe, O.; Moldavski, A.; von der Goltz, C.; Braun, U. Real-life behavioral and neural circuit markers of physical activity as a compensatory mechanism for social isolation. Nat. Mental Health 2024, 2, 337–342. [Google Scholar] [CrossRef]
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Mellow, M.L.; Crozier, A.J.; Dumuid, D.; Wade, A.T.; Goldsworthy, M.R.; Dorrian, J.; Smith, A.E. How are combinations of physical activity, sedentary behaviour and sleep related to cognitive function in older adults? A systematic review. Exp. Gerontol. 2022, 159, 111698. [Google Scholar] [CrossRef]
- Rodrigues, I.B.; Ching, P.; Kalra, M.; Zheng, R.; Rabinovich, A.; Papaioannou, A.; Leckie, C.; Kobsar, D.; Fang, Q.; Bray, S. Exploring the perspectives of older adults who are pre-frail and frail to identify interventions to reduce sedentary behaviour and improve mobility: A thematic content analysis. BMC Public. Health 2024, 24, 1582. [Google Scholar] [CrossRef]
- Nguyen, P.-Y.; Astell-Burt, T.; Rahimi-Ardabili, H.; Feng, X. Effect of nature prescriptions on cardiometabolic and mental health, and physical activity: A systematic review. Lancet Planet. Health 2023, 7, e313–e328. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/about/governance/constitution (accessed on 7 April 1948).
- Wilson, R.L.; Hutton, A.; Foureur, M. Promoting mental health recovery by design: Physical, procedural, and relational security in the context of the mental health built environment. Int. J. Ment. Health Nurs. 2023, 32, 147–161. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Koyanagi, A.; Meilstrup, C.; Nielsen, L.; Madsen, K.R.; Koushede, V. Formal social participation protects physical health through enhanced mental health: A longitudinal mediation analysis using three consecutive waves of the Survey of Health, Ageing and Retirement in Europe (SHARE). Soc. Sci. Med. 2020, 251, 112906. [Google Scholar] [CrossRef] [PubMed]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Christoforou, R.; Lange, S.; Schweiker, M. Individual differences in the definitions of health and well-being and the underlying promotional effect of the built environment. J. Build. Eng. 2024, 84, 108560. [Google Scholar] [CrossRef]
- Fırat Kılıç, H.; Arifoğlu, B.; Kızılkaya, N. The relationship between successful aging and health literacy in older adults. Perspect. Psychiatr. Care 2023, 2023, 1462914. [Google Scholar] [CrossRef]
- Sibarani, R.; Simanjuntak, P.; Sibarani, E.J. The role of women in preserving local wisdom Poda Na Lima ‘Five Advices of Cleanliness’ for the community health in Toba Batak at Lake Toba area. Gac. Sanit. 2021, 35, S533–S536. [Google Scholar] [CrossRef]
- Peterson, A.; Karlawish, J.; Largent, E. Supported decision making with people at the margins of autonomy. Am. J. Bioeth. 2021, 21, 4–18. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Chou, K.-L. Correlates of everyday competence in Chinese older adults. Aging Ment. Health 2003, 7, 308–315. [Google Scholar] [CrossRef]
- Wu, Z.; Schimmele, C.M. Psychological disposition and self-reported health among the ‘oldest-old’in China. Ageing Soc. 2006, 26, 135–151. [Google Scholar] [CrossRef]
- Yamada, Y.; Noriyasu, R.; Yokoyama, K.; Osaki, T.; Adachi, T.; Itoi, A.; Morimoto, T.; Oda, S.; Kimura, M. Association between lifestyle and physical activity level in the elderly: A study using doubly labeled water and simplified physical activity record. Eur. J. Appl. Physiol. 2013, 113, 2461–2471. [Google Scholar] [CrossRef]
- Pallant, J. PSS Survival Manual: A Step by Step Guide to Data Analysis Using IBM SPSS, 7th ed.; Open University Press: London, UK, 2020. [Google Scholar] [CrossRef]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis; Psychology Press: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Yates, A. Multivariate Exploratory Data Analysis: A Perspective on Exploratory Factor Analysis; State University of New York Press: New York, NY, USA, 1987. [Google Scholar]
- Nunnally, J.C. An Overview of Psychological Measurement. Clinical Diagnosis of Mental Disorders; Springer: Boston, MA, USA, 1978; pp. 97–146. [Google Scholar] [CrossRef]
- Cooper, D.R.; Schindler, P. Business Research Methods; Mcgraw-Hill: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Mjøsund, H.L.; Uhrenfeldt, L.; Burton, E.; Moe, C.F. Promotion of physical activity in older adults: Facilitators and barriers experienced by healthcare personnel in the context of reablement. BMC Health Serv. Res. 2022, 22, 956. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.-S.; Wong, K.K.; Tang, K.S.; Wai Wong, S.; Science, C. Walking accessibility to neighbourhood open space in a multi-level urban environment of Hong Kong. Environ. Plan. B Urban. Anal. City Sci. 2021, 48, 1340–1356. [Google Scholar] [CrossRef]
- Hjorthol, R.J.; Levin, L.; Sirén, A. Mobility in different generations of older persons: The development of daily travel in different cohorts in Denmark, Norway and Sweden. J. Transp. Geogr. 2010, 18, 624–633. [Google Scholar] [CrossRef]
- Wang, Y.; Chau, C.K.; Ng, W.; Leung, T. A review on the effects of physical built environment attributes on enhancing walking and cycling activity levels within residential neighborhoods. Cities 2016, 50, 1–15. [Google Scholar] [CrossRef]
- Rosa, E. Why self-care matters for Roma people and beyond. Vulnerability and the (un) making of water and sanitation infrastructure at the margins of the city. Geoforum 2019, 101, 192–201. [Google Scholar] [CrossRef]
- Wang, Z.; Lee, C. Site and neighborhood environments for walking among older adults. Health Place 2010, 16, 1268–1279. [Google Scholar] [CrossRef]
- Ramakreshnan, L.; Fong, C.S.; Sulaiman, N.M.; Aghamohammadi, N. Motivations and built environment factors associated with campus walkability in the tropical settings. Sci. Total Environ. 2020, 749, 141457. [Google Scholar] [CrossRef]
- Gong, K.; Wang, C.; Yin, J. Effects of the Natural Environment on the Subjective and Psychological Well-Being of Older People in the Community in China. Buildings 2024, 14, 2854. [Google Scholar] [CrossRef]
- Lommi, M.; Matarese, M.; Alvaro, R.; Piredda, M.; De Marinis, M.G. The experiences of self-care in community-dwelling older people: A meta-synthesis. Int. J. Nurs. Stud. 2015, 52, 1854–1867. [Google Scholar] [CrossRef]
- Xiaohelaiti, X.; Liu, X.; Li, C.; Wang, T.; Wu, J.; Peng, B.; Zhang, Y. Neighborhood environment and body mass index in community-dwelling older adults in China: The mediating role of transport-related physical activity. Geriatr. Nurs. 2024, 55, 304–310. [Google Scholar] [CrossRef]
- Southworth, M. development. Designing the walkable city. J. Urban. Plan. Dev. 2005, 131, 246–257. [Google Scholar] [CrossRef]
- Holland, C.J.; Cole, M.; Owens, J. Exercise and mental health: A vital connection. Br. J. Sports Med. 2024, 58, 691–692. [Google Scholar] [CrossRef]
- Master, H.; Annis, J.; Huang, S.; Beckman, J.A.; Ratsimbazafy, F.; Marginean, K.; Carroll, R.; Natarajan, K.; Harrell, F.E.; Roden, D.M. Association of step counts over time with the risk of chronic disease in the All of Us Research Program. Nat. Med. 2022, 28, 2301–2308. [Google Scholar] [CrossRef]
- Leung, M.-Y.; Wang, C.; Wei, X. Structural model for the relationships between indoor built environment and behaviors of residents with dementia in care and attention homes. Build. Environ. 2020, 169, 106532. [Google Scholar] [CrossRef]
- Ruza, J.; Kim, J.I.; Leung, I.; Kam, C.; Ng, S.Y.M. Sustainable, age-friendly cities: An evaluation framework and case study application on Palo Alto, California. Sustain. Cities Soc. 2015, 14, 390–396. [Google Scholar] [CrossRef]
- Sholanke, A.; Eleagu, J. Appraisal of Universal Design Strategies for Enhancing Social Inclusion in The Development of Sporting Facilities. IOP Conf. Ser. Earth Environ. Sci. 2024, 1342, 012024. [Google Scholar] [CrossRef]
- Scheiner, J.; Faust, N.; Helmer, J.; Straub, M.; Holz-Rau, C. What’s that garage for? Private parking and on-street parking in a high-density urban residential neighbourhood. J. Transp. Geogr. 2020, 85, 102714. [Google Scholar] [CrossRef]
- Flores, N.V.; Salvador, L.C.C.; dos Santos, A.C.P.; Madero, Y.S. A proposal to compare urban infrastructure using multi-criteria analysis. Land Use Policy 2021, 101, 105173. [Google Scholar] [CrossRef]
- Wang, R.; Zhao, J. Effects of evergreen trees on landscape preference and perceived restorativeness across seasons. Landsc. Res. 2020, 45, 649–661. [Google Scholar] [CrossRef]
- Tomasi, M.; Nikolopoulou, M.; Giridharan, R.; Löve, M. A design workflow for effective solar shading of pedestrian paths. Build. Environ. 2024, 261, 111718. [Google Scholar] [CrossRef]
- Jin, J. From Architectural Image to Design Intention: A Study of Architectural Art Design. Mediterr. Archaeol. Archaeom. 2024, 24, 26–38. [Google Scholar]
- Leung, M.; Wang, C.; Li, L. Impact of indoor visual environment on emotional and behavioral symptoms of older people with dementia. Build. Environ. 2024, 265, 111980. [Google Scholar] [CrossRef]
- Wong, R.; Szeto, W.; Yang, L.; Li, Y.; Wong, S. Public transport policy measures for improving elderly mobility. Transp. Policy 2018, 63, 73–79. [Google Scholar] [CrossRef]
- Van Hagen, M. Waiting Experience at Train Stations; Eburon Academic Publishers: Delft, The Netherlands, 2011. [Google Scholar]
- Spector, P.E. Method variance as an artifact in self-reported affect and perceptions at work: Myth or significant problem? J. Appl. Psychol. 1987, 72, 438. [Google Scholar] [CrossRef]
- Denzin, N.K. The Research Act: A Theoretical Introduction to Sociological Methods; Routledge: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Alam, M.K. A systematic qualitative case study: Questions, data collection, NVivo analysis and saturation. Qual. Res. Organ. Manag. 2021, 16, 1–31. [Google Scholar] [CrossRef]
- Bayat, S.; Naglie, G.; Rapoport, M.J.; Stasiulis, E.; Widener, M.J.; Mihailidis, A. A GPS-based framework for understanding outdoor mobility patterns of older adults with dementia: An exploratory study. Gerontology 2022, 68, 106–120. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, H.; Kang, S.-C.; Al-Hussein, M. Virtual reality applications for the built environment: Research trends and opportunities. Autom. Constr. 2020, 118, 103311. [Google Scholar] [CrossRef]
 —significant positive relationship confirmed by regression analysis;
—significant positive relationship confirmed by regression analysis;  —significant negative relationship confirmed by regression analysis.
—significant positive relationship confirmed by regression analysis; —significant negative relationship confirmed by regression analysis.
—significant negative relationship confirmed by regression analysis.
—significant positive relationship confirmed by regression analysis; —significant negative relationship confirmed by regression analysis.


{kind=link}
{kind=link}
{kind=link}
| Factors | Nature | S/N | Items | Factor Loading | α |
|---|---|---|---|---|---|
| Self-efficacy (KMO = 0.875) | |||||
| SE1—Walking ability | + | SE11 | I can walk 100 feet on flat ground. | 0.732 | 0.846 |
| + | SE12 | I can walk 10 steps downstairs. | 0.828 | ||
| + | SE13 | I can get in and out of the passenger side of a car without assistance from another person or physical aid. | 0.825 | ||
| + | SE14 | I can go on a trip that keeps you away from home for the whole day. | 0.685 | ||
| SE2—Self-care ability | + | SE21 | I can take good care of my home. | 0.836 | 0.916 |
| + | SE22 | I can get dressed or undressed without assistance. | 0.882 | ||
| + | SE23 | I can take a bath or shower without assistance from someone else. | 0.877 | ||
| Activity Engagement and Self-rated Health (KMO = 0.870) | |||||
| Activity Engagement | |||||
| AE—Activity engagement | + | AE1 | I regularly do these sedentary activities throughout the day (tea ceremony, knitting, chatting, playing cards, listening to music, drawing, collection, and appreciation). | 0.847 | 0.876 |
| + | AE2 | I regularly do the following indoor standing activities during the day (singing, dancing, playing instruments, exercising, and gardening). | 0.850 | ||
| + | AE3 | I regularly do the following outdoor standing activities during the day (walking, hiking, fishing, exercising, going to the park, photography, and traveling). | 0.875 | ||
| Self-rated Health | |||||
| SH—Self-rated health | + | SH1 | I like to keep my belongings neat and clean. | 0.793 | 0.887 |
| + | SH2 | I can make my own decisions concerning my personal affairs. | 0.813 | ||
| + | SH3 | I am as happy now as when I was younger. | 0.709 | ||
| + | SH4 | I have very good eyesight (wearing glasses or contact lenses). | 0.726 | ||
| + | SH5 | My hearing is very good (using hearing aids). | 0.801 | ||
| + | SH6 | I think my current health is very good. | 0.746 | ||
| Factors | Nature | S/N | Items | α |
|---|---|---|---|---|
| BE | ||||
| BE1—Accessibility | + | BE11 | Most of the houses in my neighborhood are elevator housing. | 0.790 |
| + | BE12 | Buildings in my neighborhood have wheelchair access and handrails. | ||
| + | BE13 | Public places in my neighborhood have toilets for people with disabilities. | ||
| BE2—Land use mix | + | BE21 | I can do most of my shopping at local stores. | 0.634 |
| − | BE22 | Parking is difficult in local shopping areas. | ||
| − | BE23 | There are many canyons/hillsides in my neighborhood that limit the number of routes for getting from place to place. | ||
| BE3—Street connectivity | + | BE31 | The streets in my neighborhood do not have many, or any, cul-de-sacs. | 0.745 |
| + | BE32 | The distance between intersections in my neighborhood is usually short. | ||
| + | BE33 | There are many four-way intersections in my neighborhood. | ||
| BE4—Walking facilities | + | BE41 | The sidewalks in my neighborhood are well maintained. | 0.769 |
| + | BE42 | Resting places are available during walks. | ||
| + | BE43 | There are pedestrian or bicycle trails in or near my neighborhood that are easy to get to. | ||
| BE5—Esthetics | + | BE51 | There are many attractive natural sights in my neighborhood (such as landscaping and views). | 0.857 |
| + | BE52 | There are attractive buildings/homes in my neighborhood. | ||
| + | BE53 | There is an open recreation area (e.g., park, beach, or other open space) within easy walking distance of my home. | ||
| BE6—Transportation | + | BE61 | The traffic speed on most nearby streets is usually slow (30 mph or less). | 0.776 |
| + | BE62 | There are crosswalks and pedestrian signals to help walkers cross busy streets in my neighborhood. | ||
| + | BE63 | There is a transit stop (such as a bus stop, train, trolley, or tram station) within easy walking distance of my home. |
| Factor | SE1 | SE2 | AE | SH |
|---|---|---|---|---|
| SE1—Walking ability | 1 | |||
| SE2—Self-care ability | 0.703 ** | 1 | ||
| AE—Activity engagement | 0.677 ** | 0.742 ** | 1 | |
| SH—Self-rated health | 0.625 ** | 0.722 ** | 0.717 ** | 1 |
| BE1—Accessibility | −0.036 | −0.038 | −0.028 | 0.044 |
| BE2—Land use mix | 0.132 * | 0.329 ** | 0.134 ** | 0.259 ** |
| BE3—Street connectivity | 0.351 ** | 0.456 ** | 0. 379 ** | 0.500 ** |
| BE4—Walking facilities | 0.268 ** | 0.291 ** | 0.249 ** | 0.348 ** |
| BE5—Esthetics | 0.270 ** | 0.246 ** | 0.304 ** | 0.352** |
| BE6—Transportation | 0.300 ** | 0.337 ** | 0.335 ** | 0.457 ** |
| Models | B | S.E. | Sig. | VIF | R | AR2 | ΔR2 | ANOVA | ||
|---|---|---|---|---|---|---|---|---|---|---|
| F | Sig. | |||||||||
| 1a | Walking Ability |  | Self-efficacy | |||||||
| Constant | 0.929 | 0.159 | 0.000 | 0.692 | 0.477 | 0.478 | 339.435 | 0.000 | ||
| SE2 Self-care ability | 0.700 | 0.038 | 0.000 | 1.000 | ||||||
| 1b | Walking Ability | | Self-efficacy, BE | |||||||
| Constant | 0.938 | 0.226 | 0.000 | 0.710 | 0.495 | 0.026 | 52.956 | 0.000 | ||
| SE2 Self-care ability | 0.676 | 0.044 | 0.000 | 1.386 | ||||||
| BE1 Accessibility | −0.082 | 0.037 | 0.029 | 1.577 | ||||||
| BE2 Land use mix | −0.130 | 0.041 | 0.002 | 1.258 | ||||||
| 2a | Self-care Ability | | Self-efficacy | |||||||
| Constant | 1.503 | 0.145 | 0.000 | 0.692 | 0.477 | 0.478 | 339.435 | 0.000 | ||
| SE1 Walking ability | 0.683 | 0.037 | 0.000 | 1.000 | ||||||
| 2b | Self-care Ability | | Self-efficacy, BE | |||||||
| Constant | 0.477 | 0.213 | 0.026 | 0.750 | 0.554 | 0.084 | 66.895 | 0.000 | ||
| SE1 Walking ability | 0.583 | 0.038 | 0.000 | 1.223 | ||||||
| BE2 Land use mix | 0.186 | 0.037 | 0.000 | 1.211 | ||||||
| BE3 Street connectivity | 0.136 | 0.047 | 0.004 | 1.646 | ||||||
| 3a | Activity Engagement | | Self-efficacy | |||||||
| Constant | 0.785 | 0.226 | 0.001 | 0.535 | 0.283 | 0.286 | 74.047 | 0.000 | ||
| SE1 Walking ability | 0.356 | 0.071 | 0.000 | 1.917 | ||||||
| SE2 Self-care ability | 0.322 | 0.071 | 0.000 | 1.917 | ||||||
| 3b | Activity Engagement | | Self-efficacy, BE | |||||||
| Constant | 0.811 | 0.312 | 0.010 | 0.574 | 0.315 | 0.043 | 22.298 | 0.000 | ||
| SE1 Walking ability | 0.299 | 0.071 | 0.000 | 2.018 | ||||||
| SE2 Self-care ability | 0.368 | 0.076 | 0.000 | 2.286 | ||||||
| BE2 Land use mix | −0.166 | 0.056 | 0.003 | 1.293 | ||||||
| BE5 Esthetics | 0.204 | 0.076 | 0.007 | 2.146 | ||||||
| 4a | Self-rated Health | | Activity Engagement | |||||||
| Constant | 2.232 | 0.122 | 0.000 | 0.555 | 0.306 | 0.308 | 164.445 | 0.000 | ||
| AE Activity engagement | 0.433 | 0.034 | 0.000 | 1.000 | ||||||
| 4b | Self-rated Health | | Activity Engagement, Self-efficacy | |||||||
| Constant | 0.685 | 0.137 | 0.000 | 0.767 | 0.585 | 0.280 | 175.060 | 0.000 | ||
| AE Activity engagement | 0.184 | 0.031 | 0.000 | 1.401 | ||||||
| SE1 Walking ability | 0.126 | 0.043 | 0.004 | 2.049 | ||||||
| SE2 Self-care ability | 0.471 | 0.044 | 0.000 | 2.023 | ||||||
| 4c | Self-rated Health | | Activity Engagement, Self-efficacy, BE | |||||||
| Constant | −0.080 | 0.180 | 0.655 | 0.803 | 0.636 | 0.057 | 73.054 | 0.000 | ||
| AE Activity engagement | 0.179 | 0.030 | 0.000 | 1.491 | ||||||
| SE1 Walking ability | 0.117 | 0.041 | 0.005 | 2.117 | ||||||
| SE2 Self-care ability | 0.358 | 0.045 | 0.000 | 2.434 | ||||||
| BE2 Land use mix | 0.084 | 0.032 | 0.010 | 1.325 | ||||||
| BE3 Street connectivity | 0.098 | 0.039 | 0.013 | 1.685 | ||||||
| BE6 Transportation | 0.160 | 0.041 | 0.000 | 1.610 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Chen, F.; Lin, Y.; Qiang, S.; Sun, J. Development of a Built Environment–Self-Efficacy–Activity Engagement–Self-Rated Health Model for Older Adults in Urban Residential Areas. Buildings 2025, 15, 1660. https://doi.org/10.3390/buildings15101660
Wang C, Chen F, Lin Y, Qiang S, Sun J. Development of a Built Environment–Self-Efficacy–Activity Engagement–Self-Rated Health Model for Older Adults in Urban Residential Areas. Buildings. 2025; 15(10):1660. https://doi.org/10.3390/buildings15101660
Chicago/Turabian StyleWang, Chendi, Fangyi Chen, Yujie Lin, Shaohua Qiang, and Jingsong Sun. 2025. "Development of a Built Environment–Self-Efficacy–Activity Engagement–Self-Rated Health Model for Older Adults in Urban Residential Areas" Buildings 15, no. 10: 1660. https://doi.org/10.3390/buildings15101660
APA StyleWang, C., Chen, F., Lin, Y., Qiang, S., & Sun, J. (2025). Development of a Built Environment–Self-Efficacy–Activity Engagement–Self-Rated Health Model for Older Adults in Urban Residential Areas. Buildings, 15(10), 1660. https://doi.org/10.3390/buildings15101660