1. Introduction
The European Union recognizes architecture as a vital cultural and life component, particularly in healthcare, where it transcends mere aesthetics to foster environments conducive to healing and well-being [
1]. In this realm, the role of architecture extends beyond visual appeal, playing a pivotal role in enhancing quality of life and contributing significantly to national wealth through thoughtful design and construction practices [
2]. However, the challenge lies in ensuring these architectural principles are consistently applied across all healthcare settings, particularly in under-resourced areas.
In healthcare systems, architectural design is instrumental in creating environments that cater to the unique needs of patients. These environments, sensitive to the needs of health-impaired individuals, prioritize comfort, safety, and therapeutic value, significantly impacting patient recovery and staff efficiency [
3]. Critically, there is a need for more empirical research to quantify the impact of architectural design on patient outcomes and staff productivity. Historically, the focus of healthcare architecture was predominantly on functionality. However, recent advancements in architectural practices have shifted the emphasis towards patient-centered design, sustainability, and adaptability. This modern approach integrates natural lighting, efficient ventilation, noise control, and energy efficiency, all contributing to improved patient outcomes and enhancing the working conditions of healthcare staff [
4,
5]. This shift represents a positive trend, but the challenge remains in balancing aesthetic appeal with practical functionality. Despite these advancements, the field of healthcare architecture faces ongoing challenges. The rapid evolution of medical technologies, shifting patient demographics, and an increasing focus on sustainable practices present a complex landscape for architects. These challenges, however, also offer opportunities to innovate and integrate evidence-based design principles, creating healthcare facilities that are more attuned to the needs of patients, staff, and the broader environment [
6]. The critical message here is the need for continuous adaptation and innovation in architectural design to meet evolving healthcare demands.
In Slovenia, the architectural landscape is marked by challenges such as widespread suburbanization, the erosion of cultural heritage, and environmental pollution. These issues lead to architectural and urban solutions that often need a long-term, strategic vision [
2]. Addressing these challenges through a strategic and integrated approach to urban planning and architectural design is imperative. Addressing these challenges is crucial and requires a commitment to inclusive architecture. This commitment involves planning diverse, accessible housing and public spaces, ensuring equal access to services, and developing new building typologies to accommodate the needs of an aging population. Inclusive architecture is not just about building design; it is a tool for democratic development, fostering active public life, social interactions, and cultural presentation and regulation [
2].
The architectural design of healthcare institutions, while crucial in realizing care concepts, has received limited attention in research. Studies like those by Steenwinkel et al. have emphasized the importance of freedom, particularly freedom of movement, and the balance between experiencing freedom and its connection with a social and physical framework. These studies highlight architectural features such as the number of residents per housing unit, spatial generosity, and physical accessibility, all of which play a significant role in patient care and staff well-being [
7]. This underscores the need for more focused research on the specific architectural elements contributing to effective healthcare environments. A comprehensive approach to planning high-quality living environments is essential. This approach must consider various environmental, sociological, functional, and cultural perspectives and view the environment as interconnected. The role of open space and green areas in enhancing the quality of life is particularly noteworthy, as confirmed by research findings [
8]. Therefore, comprehensive and holistic planning is critical in creating sustainable and livable healthcare environments.
The therapeutic benefits of nature in healthcare settings have been well-established. Prof. Roger Ulrich’s seminal work in 1984 on hospital design, which emphasized the healing power of natural views, has had a lasting impact on hospital architecture [
9,
10]. However, the increasing complexity of healthcare treatments and the aging of current infrastructure necessitates systematic investment in new, efficient infrastructures. This need is particularly acute in Slovenia, where there is a lack of comprehensive research in the health and social care infrastructure field and an absence of strategic planning documents [
2]. This highlights a critical gap in research and strategic planning in Slovenia’s healthcare infrastructure. As Ulrich and others advocate, evidence-based design improves treatment outcomes and hospital efficiency [
9,
11]. This approach requires a holistic, multidisciplinary perspective, integrating various fields such as architecture, medicine, health sciences, and gerontology. It emphasizes the importance of considering the entire ecosystem of healthcare facilities, from the layout of individual rooms to the organization of whole buildings [
11,
12]. The essential insight is the significance of evidence-based design in fostering healthcare settings that are both productive and efficient.
Today, healthcare architecture places the patient at the center, focusing on individuality and humanization. Health and social care infrastructure design is evolving to create spaces that positively influence the patients’ mood and self-image, aiding in faster recovery [
13]. The challenge for architects is to design hospitals that support modern healthcare needs while minimizing patient harm [
11]. The key conclusion imperative for patient-centered architectural design in healthcare is that which enhances patient experiences and outcomes. The University Medical Centre Ljubljana (UMCL) exemplifies the balance between preserving cultural heritage and adapting to technological advancements [
3]. The goal is to create healthcare environments that are not only efficient and accessible but also adaptable to future needs, ensuring long-term sustainability and improved quality of life for patients and residents [
13]. This example highlights the importance of balancing heritage preservation with modern healthcare needs in architectural design.
To provide a concise overview of the key themes discussed in this introduction,
Table 1 summarizes the principal aspects of healthcare architecture.
Addressing Demographic Shifts and Healthcare Challenges through Architectural Innovation
Recent demographic shifts and technological advancements in Slovenia have brought new challenges to healthcare architecture, underscoring the need for innovative design solutions that are sustainable, patient-centric, and adaptable. The aging population is a significant factor, with the proportion of those over 65 increasing from 9.9% in 1971 to 19.4% in 2018. This demographic change and extended life expectancies have profound implications for healthcare infrastructure and architectural design [
14,
15].
The objective of this study, originating from the “Targeted Research Program «CRP-2019»”, is to critically analyze the architecture of healthcare institutions. This analysis aims to develop and improve conditions for managing demographic changes and ensuring quality care. The foundation of this research lies in addressing the gap between current architectural practices and the evolving needs of healthcare systems, particularly in the context of an aging society.
In addition to demographic challenges, the evolving nature of healthcare treatments and the integration of new technologies have significantly influenced the design and functionality of healthcare environments. The project seeks to review and analyze architectural solutions in healthcare care institutions, examining how spatial and environmental factors impact patient and staff safety and well-being. This comprehensive approach is essential for proposing future architectural directions that are technically sound for and empathetic to the users’ needs.
This study aims to bridge the gap between architectural design and healthcare delivery, ensuring that the built environment effectively supports the evolving needs of the healthcare system. By focusing on sustainable, patient-centric, and adaptable design solutions, the study aims to contribute to the broader discourse on healthcare architecture and its role in enhancing the quality of life for patients and healthcare professionals alike.
Modern architectural practices prioritize the creation of environments that elevate the quality of life for their inhabitants, as Allam et al. [
16] clarify that integrating innovative technologies, such as artificial intelligence, big data, and the internet of things (IoT), can redefine urban planning and service provisioning, leading to enhanced urban efficiencies and improved quality of life. The architectural design of healthcare facilities, influenced by sustainable and evidence-based design principles, can redefine patient experiences, leading to enhanced well-being and improved quality of care [
5]. The historical context and cultural significance of healthcare facilities, as seen in Ottoman healthcare structures, emphasize the importance of preserving and adapting these spaces to contemporary needs [
4]. By enhancing the patient experience through thoughtful architectural design, we directly align with the overarching goal of creating buildings prioritizing their users’ well-being and holistic understanding [
6,
17,
18]. Thus, the intersection of architecture and healthcare becomes a pivotal domain, contributing significantly to the broader vision of sustainable, efficient, and human-centric built environments.
Understanding the connection between architecture and healthcare is crucial for designing effective and sustainable healthcare institutions, especially in the Slovenian healthcare system. Therefore, the review is structured to provide a comprehensive overview of existing literature in the field of healthcare architecture, emphasizing the importance of architectural design in enhancing healthcare delivery. The study’s methodology systematically analyzes architectural solutions in healthcare institutions, reflecting on how these environments can adapt to the changing demographic landscape and emerging healthcare challenges. Therefore, it is structured as follows:
Section 2 describes the methodology and reviews the relevant literature. This is followed by the presentation of results in
Section 3.
Section 4 includes a discussion, implementation suggestions, and the proposal of the new IHAF model.
Section 5 presents the conclusions drawn from this study.
2. Materials and Methods
Knowledge generation in the field of architectural evaluation techniques for healthcare facilities is accelerating quickly while at the same time remaining fragmented and interdisciplinary. Due to this rapid and multifaceted growth, it is difficult to stay updated with the latest advancements, lead in research innovation, and comprehensively evaluate the accumulated knowledge within this specialized field. Therefore, the literature review as a research method is more relevant than ever. By integrating findings and perspectives from multiple empirical studies, a literature review can address research questions with a power that no single study can match [
19]. Therefore, we used narrative review [
20] for the literature on the spatial location of health and social care facilities. This method allows data to be obtained from various sources, thus providing a comprehensive understanding of the area under study.
In this investigation, we systematically analyzed scientific literature and expert commentaries and conducted a cross-sectional review of articles evaluating architectural designs within healthcare institutions. Given the demographic shifts and escalating healthcare demands in Slovenia, architects, urban planners, and policymakers must thoroughly assess the architectural frameworks of healthcare institutions, emphasizing their current functionality and potential adaptability for future requirements. Our literature search was methodically conducted across three primary databases: ScienceDirect, MDPI, and Cobiss, adhering to the stringent guidelines delineated by the priority reports for systematic reviews and meta-analysis (PRISMA-P) 2015 [
21]. The inclusion and exclusion criteria for our literature search are detailed in
Table 2: Inclusion and exclusion criteria.
When this research was conducted, concluding in March 2020, the world experienced the unforeseen outbreak of the COVID-19 pandemic. This event significantly impacted all facets of society, including the healthcare sector and the architecture of healthcare institutions [
22,
23]. However, our research focused on the period before the pandemic outbreak, as it was designed and executed before this event.
The COVID-19 outbreak introduced new challenges and needs in the design of healthcare and social care institutions, which previous research could not have anticipated [
24]. Therefore, it was logical to limit the research period to 2020 to ensure consistency and relevance of the collected data.
Furthermore, 2005 to 2020 encompassed significant changes and trends in healthcare institution architecture, which were vital for our analysis [
25]. Including the COVID-19 outbreak period would have necessitated additional research and analyses, potentially altering the focus and scope of our study.
Future research will undoubtedly need to address the impact of the COVID-19 pandemic on the architecture of healthcare and social care institutions. However, this study significantly contributes to understanding trends and practices in the pre-pandemic period.
Articles published in professional, scientific journals and international documents, standards, guidelines, and research studies were reviewed. The study did not include information from editorials, letters, interviews, posters, and articles without full-text access.
Following the establishment of inclusion and exclusion criteria, our methodology progressed to the next phase as outlined in the adapted PRISMA (preferred reporting items for systematic reviews and meta-analyses) diagram. This phase involved a detailed determination, review, suitability, and inclusion process, visually represented in
Figure 1: Adapted PRISMA diagram. This figure illustrates our systematic approach to selecting and evaluating the literature, ensuring a comprehensive and systematic review.
Building upon this structured approach, we refined our methodology by employing a systematic literature selection process, as comprehensively detailed in
Table 3: The literature selected. This table overviews our search strategy across the three primary databases: ScienceDirect, MDPI, and Cobiss. It outlines the specific keywords used, the number of results obtained, and the selection process that led to the final set of articles included in our study.
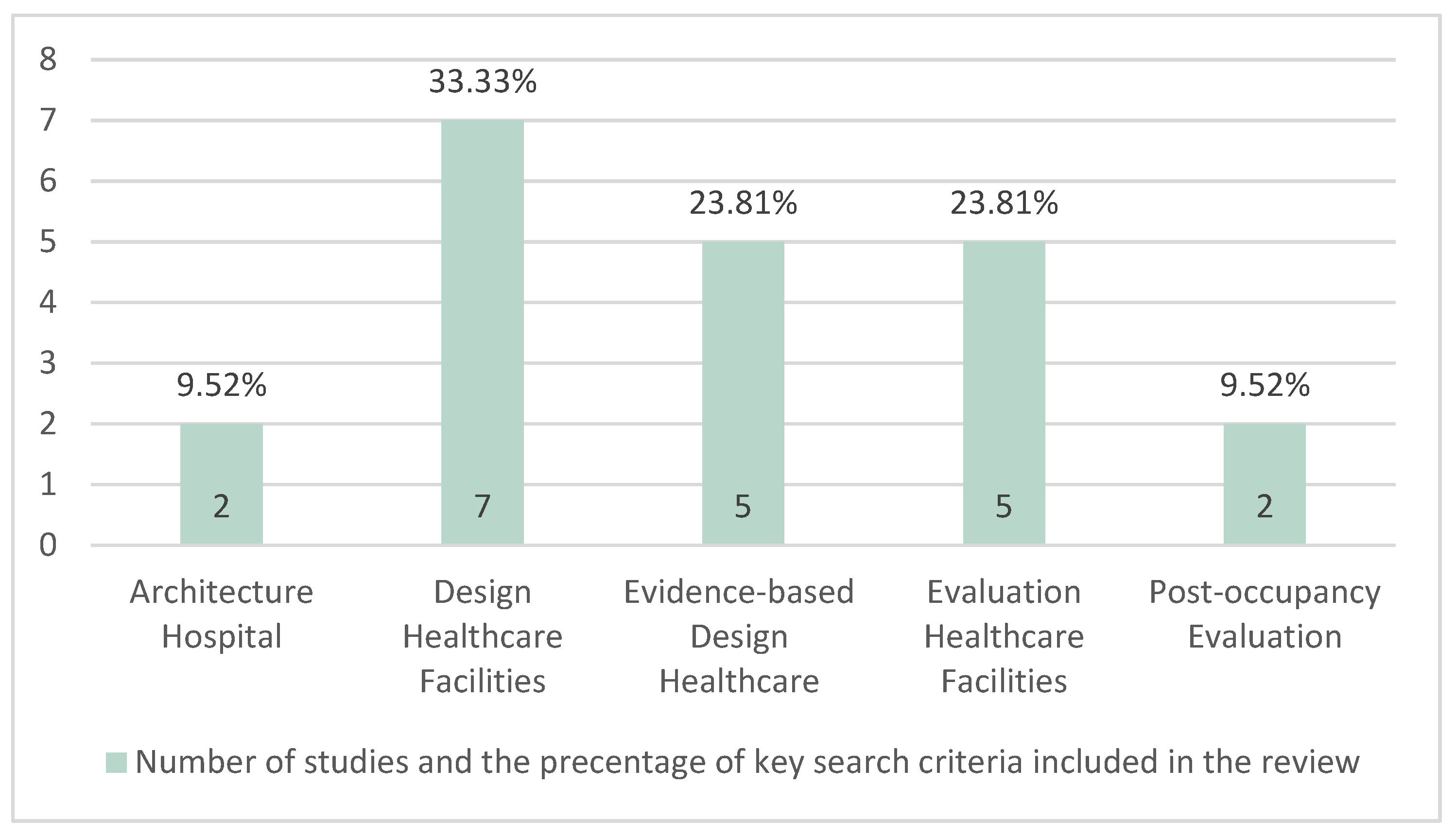
For each database, we used specific keywords relevant to our research focus. In ScienceDirect, we searched for five sets of keywords: “Architecture Hospital”, “Design Healthcare Facilities”, “Evidence-based Design Healthcare”, “Evaluation Healthcare Facilities”, and “Post-occupancy Evaluation”. These searches yielded a total of 168,467 results. We initially selected 45 articles based on their relevance to our research. After a thorough review and the removal of duplicates, we finalized a selection of 21 unique and pertinent articles.
In MDPI, the same keyword sets resulted in a smaller pool of results, ranging from 28 to 41 per keyword. The initial selection here was ten articles, further narrowed to two after careful consideration.
In the Cobiss database, the search was conducted with Slovenian equivalents of the keywords. This search yielded significantly fewer results, with the highest being 16 for “Oblikovanje Zdravstvenih Ustanov” (design of healthcare facilities). However, none of these results met our inclusion criteria for the final selection.
The selection process involved two stages: an initial screening based on titles and abstracts to assess relevance and a full-text review to ensure the articles met our specific inclusion criteria. This systematic approach ensured that the final selection of literature was highly relevant to our study’s focus on the impact of architecture in healthcare settings. The final selection of 21 articles (14 unique articles after removing duplicates) provided a comprehensive foundation for our analysis and discussion.
Analysis of Evaluation Methods for Healthcare Facilities’ Review
In this chapter, we will present the key findings of our literature review, illuminating the connection between architecture and healthcare and highlighting specific methods for evaluating healthcare facilities. To provide the reader with further information on the studies included in this review,
Table 4 outlines the author’s details, the year of publication, the purpose of the research, and critical findings.
The review was conducted using five key search terms for the review process.
Figure 2 outlines these key criteria in percentage terms for the studies that underwent full-text examination and denotes the strength of individual measures.
3. Results
The main goal of this research review was to present an overview of the studies evaluating healthcare institutions with a focus on architecture. Given the area’s specificity and analysis, we limited ourselves to reviewing the methods and tools for assessing buildings to select the most appropriate method for evaluating the architectural solutions of healthcare institutions. In the modern healthcare sector, architecture is becoming a key factor influencing the quality of care, sustainability, and the entire planning process of healthcare institutions.
In this review, the reasons mentioned in the different studies included in our results have been classified into key categories that reflect the critical aspects of evaluating healthcare institutions: architectural and design guidelines, user experience and satisfaction, and sustainability and environmental impact.
- 1.
Architectural and design guidelines for healthcare institutions:
This evaluation category focuses on specific architectural and design approaches that have been used in the planning and construction of healthcare institutions. The evaluation is based on considering particular guidelines and standards used and how they influenced the final design and functionality of the healthcare institution.
- 2.
User experience and satisfaction in healthcare institutions:
This evaluation category focuses on the experiences and satisfaction of healthcare institution users—patients, their families, healthcare staff, and other visitors. The evaluation is based on understanding how people feel in the space of a healthcare institution, how easy it is to navigate the facility, the accessibility and availability of rooms and general comfort and safety within the institution.
- 3.
Sustainability and environmental impact of healthcare institutions:
This evaluation category focuses on sustainable practices and the impact of the healthcare institution on the environment. The evaluation is based on considering energy efficiency, the use of sustainable materials, waste management, water efficiency, and other sustainable approaches used in the planning and construction of the healthcare institution.
Table 5 provides an insight into their alignment with individual study findings.
In the following, we will examine each of these categories in more detail to better understand their significance and impact on the design of healthcare institutions.
3.1. Architectural and Design Guidelines for Healthcare Institutions
With their work, skills, and potential influence, architects can significantly improve health. The architectural profession can contribute to improving the health and well-being of the population with healthier buildings and spaces. However, there needs to be more connection between architecture and public health [
39]. Hignett and Lu [
26] conducted a study focusing on the use of architectural guidelines by architects and designers of healthcare institutions. They identified two key roles: involving patients and healthcare workers in the planning process and the importance of supporting standardization in obtaining new research evidence. This approach is crucial to ensure healthcare institutions are designed to serve their users best.
Samah, Ibrahim and Amir [
29] focused on the design aspects of hospitals. Their research revealed 105 design aspects, including quality patient care, crucial in building new and renovating existing facilities. This extensive analysis emphasizes the importance of design in a healthcare environment and how it can influence the patient experience.
Verderbera et al. [
31] analyzed the role of the competition format in the design and construction of healthcare institutions. The competition is a widely accepted method that accelerates and improves innovation, creativity, theoretical discourse, and the profession. The authors introduced a two-phase model that combines creativity and knowledge. This model emphasizes the importance of combining these two aspects to achieve optimal results in healthcare planning.
Hicks et al. [
32] introduced a participatory planning method known as the “3P” model. The building design determines the layout of spaces and the mutual interactions of patients, doctors, visitors, medicines, supplies, equipment, and information, i.e., the seven flows of medicine. This approach emphasizes the importance of involving all stakeholders in planning to ensure everyone’s needs are considered. Liu et al. [
37] focused on assessing the quality of the indoor environment of hospitals. The study is based on a measurement survey conducted in two healthcare institutions in China. This study emphasizes the importance of providing a quality indoor environment for the well-being of patients.
3.2. User Experience and Satisfaction in Healthcare Institutions
Haron et al. [
27] explored the understanding of patients’ complexities when using healthcare institutions. The research survey results showed that the following usability criteria are essential for most patients: accessibility, availability, and spatial orientation. This finding emphasizes the importance of designing healthcare institutions that are intuitive and user-friendly.
Huisman et al. [
28] structured scientific research on the design of healthcare institutions based on evidence from patients, their families, and healthcare staff. The study results showed that the orientation towards the outcomes of employees in healthcare institutions is rare and insufficiently substantiated and needs to be considered in the planning stage. This finding indicates the need for greater involvement of employees in the planning process.
Bengtsson and Grahn [
30] introduced a quality evaluation tool (QET) tailored for designing outdoor environments in healthcare settings, such as healthcare gardens. This tool, developed through theory triangulation, integrates evidence from research on health/well-being and the outdoor environment. The QET identified 19 environmental qualities essential for the design of healthcare gardens. These qualities are divided into two categories: six based on the need for comfort in the outdoor environment and thirteen based on the need for access to nature and surrounding life. The tool also offers insights into user involvement in the design process and provides general design guidelines to cater to users’ diverse needs and preferences. Their work emphasizes the significance of evidence-based design and its connection to salutogenesis and pathogenesis, ensuring that outdoor healthcare environments are therapeutic and user-centric.
Djukic and Marić [
34] highlighted the pressing need for socially sustainable healthcare facilities, especially in regions like Serbia, where public hospitals are declining. Their research, centered on the most significant healthcare facility in Serbia, the Medical Military Academy (MMA), utilized qualitative and quantitative methods to assess the current design problems. Engaging with diverse stakeholders, including patients and medical staff, they identified critical issues in the existing design, particularly concerning comfort, distribution, safety, and humanization.
3.3. Sustainability and Health in Healthcare Institutions
Healthcare facilities across Europe are undergoing significant transformations to deliver efficient services amidst dwindling resources. A prevailing trend has been the shift towards more extensive, specialized hospitals, driven by the notion of achieving economies of scale. However, the article by Pantzartzis et al. [
36] challenges this prevailing notion, suggesting that the evidence supporting the cost-effectiveness of more extensive healthcare facilities is both limited and contradictory. Their comprehensive literature review delves into the factors that can lead to sustainable small healthcare facilities, emphasizing the need to consider broader sustainability issues beyond economic metrics.
The global trend towards sustainability has led the healthcare sector to adopt the “greening movement”. This has resulted in the creation of sustainability certification tools like BREEAM, LEED, and the Green Guide for Healthcare; however, Stevanovic et al. [
35] raise concerns about these tools’ subjectivity. Their research in the Flemish healthcare sector revealed limitations in the “Duurzaamheidsmeter zorg”, a local qualitative tool. Feedback indicated a need for a more quantitative sustainability assessment method. Based on professionals’ experiences, their SWOT analysis suggested the importance of a life cycle thinking perspective in developing new evaluation methods.
Hamed et al. [
33] tried to bridge the gap between sustainability and evidence-based planning research areas. The results of their research indicate that, according to patients, the most important aspects contributing to their well-being are plants and greenery, safety, and single-bed rooms. This study points to the connection between sustainability and health in architectural planning.
Brambilla and Capolongo [
38] introduced the latest tools for evaluating the hospital environment and measuring health and sustainability. Thirteen tools created between 1990 and 2017 were analyzed. This research emphasizes the importance of using tools to ensure that healthcare institutions are designed to best serve their users and the environment.
In light of these insights, it is evident that architecture plays a pivotal role in the healthcare sector, influencing care quality, user experience, and sustainability. The subsequent chapters will delve deeper into how these findings can shape the design of future healthcare institutions, ensuring they are both practical and sustainable.
4. Discussion
The literature review revealed the importance of the connection between architecture and healthcare. Quality architecture ensures high-quality living and care in healthcare institutions [
1,
2]. Healthcare institutions face numerous challenges in the modern world, from demographic changes to technological innovations [
26]. Architecture plays a crucial role in shaping the response to these challenges, as it can influence the quality of care, sustainability, and the entire planning process of healthcare institutions [
29].
When discussing the architectural and design guidelines for healthcare institutions, it is important to emphasize that these approaches are crucial for ensuring the functionality and efficiency of healthcare facilities. The policies and standards used in the planning process directly influence how a healthcare institution integrates into its environment and serves its users [
33].
Regarding user experience and satisfaction in healthcare institutions, understanding the interactions between patients, healthcare staff, and space is paramount. The design and layout of a healthcare institution can significantly influence how people feel and how effectively they can perform their tasks [
28].
In the context of sustainability and the environmental impact of healthcare institutions, it is important to note that they are at the forefront of efforts to reduce the ecological footprint. By using sustainable approaches, such as energy efficiency and environmentally friendly materials, healthcare institutions contribute to a greener and more sustainable future [
38].
These findings lay the foundation for further analysis and interpretation, as they allow us to better understand the connections between architecture, user experience, and sustainability in the context of healthcare institutions.
4.1. Contextualization and Interpretation
In the preliminary part of this article, we highlighted how quality architecture affects the quality of living and care in healthcare institutions, as defined in the Council Resolution of Europe [
1] and the Architectural Policy of Slovenia [
2]. This emphasis on the quality of architecture as a critical factor in ensuring high-quality living aligns with current trends in the architectural design of healthcare institutions.
Healthcare institutions face numerous challenges today, from demographic changes to technological innovations [
26]. In this context, architecture has become a critical factor influencing the quality of care, sustainability, and the entire planning process of healthcare institutions [
29]. However, it is crucial to note that while architecture plays a significant role, it must be integrated with other aspects, such as healthcare policies and technological advancements, to create a holistic healthcare environment.
Compared to newer scientific articles, such as those by Giudici et al. [
22] and Howarth et al. [
23], which focused on the impact of the COVID-19 pandemic on the architectural design of healthcare institutions, our research emphasizes the importance of a sustainable and user-centered approach to architectural planning. While the pandemic brought new challenges and needs in healthcare and social care institutions, our findings indicate that the guidelines and principles we discussed remain relevant and crucial for designing quality healthcare institutions. This highlights the enduring nature of these principles, even in the face of unprecedented challenges such as a global pandemic.
Why do specific patterns appear in the architectural design of healthcare institutions? One of the fundamental mechanisms is the response to changes in the healthcare environment. Changes in demographics, technological advancements, and increased awareness of sustainable practices have influenced how healthcare institutions are designed and managed [
28]. For example, the aging population in Slovenia and elsewhere has increased the need for healthcare institutions tailored to older patients [
26]. This demographic shift necessitates a re-evaluation of existing architectural designs to better cater to the specific needs of this growing patient demographic.
Additionally, with the rise in technological innovations, there has been an increased need for healthcare institutions that can support advanced medical equipment and technology. This has led to design guidelines that emphasize the flexibility and adaptability of spaces [
29]. Integrating technology in healthcare architecture is not just a trend but a necessity, underscoring the need for designs to accommodate future technological advancements.
The influence of architecture on user experience is another crucial aspect. The design of a healthcare institution can affect how patients, their families, and healthcare staff feel and how effectively they can operate within that institution. For instance, well-designed hospitals can reduce stress in patients and enhance their overall treatment experience [
33]. This underscores the importance of a patient-centric approach in architectural design, where the well-being of patients and staff is a primary consideration.
Lastly, with the growing awareness of the impact of human activities on the environment, sustainable practices have also become of paramount importance in the architecture of healthcare institutions. Designing a healthcare institution that considers energy efficiency, uses sustainable materials, and other sustainable approaches reduces its environmental impact. It can decrease operational costs and improve the quality of care [
38]. Sustainability in healthcare architecture is not just an environmental concern but also a practical one, influencing long-term operational efficiency and patient well-being.
4.2. Comparison with Previous Research
Our initial discussion highlighted the role of architecture in healthcare and its impact on the quality of living and care in healthcare institutions [
1,
2]. In this light, Hignett and Lu [
26] emphasized the value of involving patients and healthcare staff in the planning process, echoing our initial findings on the importance of user participation in the design process.
Furthermore, in the introductory segment, we also mentioned various design guidelines, user experience, sustainability, and environmental impact as critical factors in designing healthcare institutions [
2,
8,
10,
11]. This aligns with the findings of Samah, Ibrahim and Amir [
29], who identified 105 design aspects crucial for the construction and renovation of healthcare facilities, and with the results of Hignett and Lu, who emphasized the importance of supporting standardization in obtaining new research evidence in planning processes [
26].
The initial chapter also discussed the importance of innovation, fresh, and especially holistic approaches in architectural planning [
2,
12,
13]. This aligns with the analysis of Verderber and colleagues [
31], who researched the role of the competition format in planning healthcare institutions. Furthermore, this is confirmed by Brambilla and Capolongo, who argue that in modern evaluation tools, health is now three times more important as a criterion than in those tools developed in the nineties [
38].
Lastly, in the context of the Slovenian healthcare system, we found in the initial section that there needs to be more research focusing on evaluating the architecture of healthcare institutions [
2]. This emphasizes the need for further research in this area and aligns with our findings in this review article.
4.3. Implications—Integrated Healthcare Architecture Framework (IHAF)
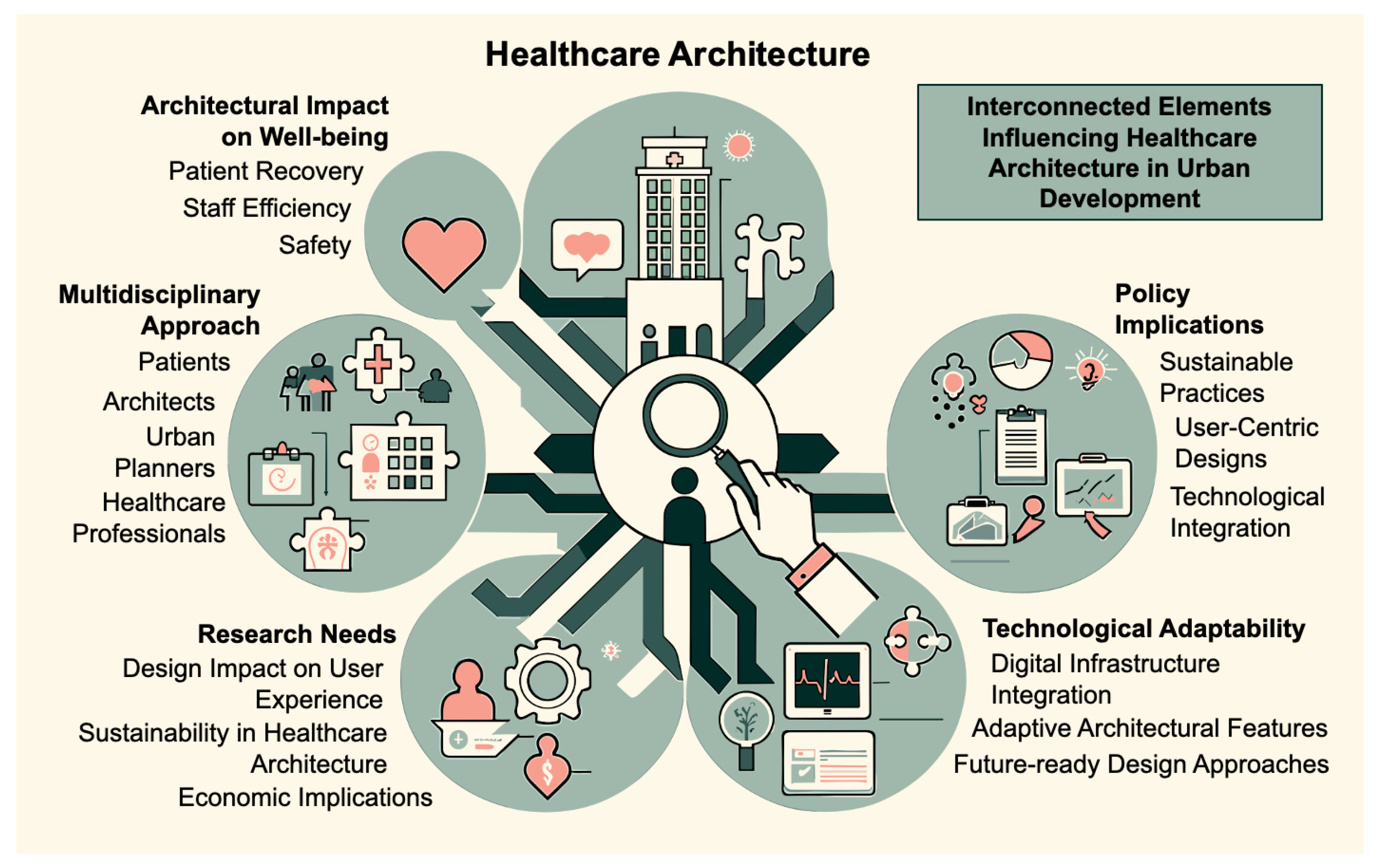
The synthesis of our findings highlights the profound interplay between healthcare architecture and the broader objectives of building design and urban development, which is at a critical juncture, facing multilayered challenges that stem from evolving healthcare needs, technological advancements, and a growing emphasis on sustainability and user experience. A visual representation of the interconnected elements influencing healthcare architecture in urban development is presented in
Figure 3. The central part emphasizes the core focus on healthcare architecture, while the radiating branches highlight the multifaceted implications discussed in the study. Traditional architectural approaches often need to be more holistically addressing these contemporary demands, by considering users’ emotional and psychological well-being and the environmental sustainability of healthcare facilities. This gap emphasizes the need for a new, integrative framework to navigate modern healthcare architecture’s complexities.
The integrated healthcare architecture framework (IHAF) responds to this need. It is a comprehensive model designed to encapsulate the diverse aspects of healthcare architecture, including the critical categories defined in our review: architectural and design guidelines, user experience and satisfaction, and sustainability and environmental impact. These ensure that facilities are functionally efficient but also patient-centric, sustainable, and adaptable to future needs. The IHAF is a novel, multidimensional, holistic approach developed from our comprehensive review of healthcare architecture. The IHAF model is presented in
Table 6 below, providing insight into the framework.
The IHAF addresses the needs by encapsulating the key categories’ diverse aspects of healthcare architecture.
Architectural and Design Guidelines
Inclusive design process: IHAF’s inclusive design process ensures that the voices of all stakeholders are heard and integrated. This approach leads to creating spaces that are not just architecturally sound but also empathetic to the needs of patients, healthcare workers, and visitors. It fosters a collaborative design environment, resulting in more effective and user-friendly healthcare facilities.
Adaptive and flexible spaces: The emphasis on adaptive and flexible spaces allows healthcare facilities to remain relevant and functional in the face of rapid technological advancements and changing healthcare demands. This component ensures that healthcare architecture is not static but evolves, accommodating new treatments, technologies, and patient care models.
User Experience and Satisfaction
Patient-centric design: By prioritizing patient-centric design, IHAF ensures that healthcare facilities are not just places for treatment but also spaces that promote healing and well-being. This aspect of the framework focuses on creating a supportive and comforting environment for patients, which is crucial for their recovery and overall experience.
Staff efficiency and well-being: Recognizing the critical role of healthcare staff, IHAF places equal importance on designing spaces that enhance staff efficiency and well-being. Efficiently designed workspaces can significantly reduce stress and burnout among healthcare professionals, leading to improved patient care and staff satisfaction.
Sustainability and Environmental Impact
Eco-friendly practices: IHAF’s commitment to eco-friendly practices ensures that healthcare facilities contribute positively to the environment. This approach aligns with global sustainability goals and can lead to cost savings in the long run through the efficient use of resources.
Green spaces: Integrating green spaces within healthcare settings under IHAF enhances the aesthetic appeal and provides therapeutic benefits to patients and staff. These spaces serve as areas for relaxation and respite, contributing to the overall healing environment.
Implementing the IHAF has the potential of extensive implications for future healthcare architecture projects, policymaking, and research. It could set a new standard for designing healthcare facilities that are resilient, patient-focused, and environmentally responsible. In policymaking, the IHAF could serve as a guideline for developing regulations and standards that could ensure holistic designs for healthcare facilities. From the research point of view, the IHAF opens new avenues to explore the impact of architectural design on patient outcomes, staff efficiency, and environmental sustainability.
4.4. Assessing IHAF against Existing Approaches
The proposed IHAF is a step forward in the expanding environment of healthcare architecture. This subsection compares the IHAF to the existing architectural methods assessed in this review. It places the IHAF in the context of current methodologies and clarifies its possible contributions, innovations, benefits, and applications within the three key categories defined in our review.
Architectural and Design Guidelines
Existing approaches: Traditionally, healthcare architecture has focused on functional and operational efficiency, adhering to standard architectural guidelines and regulations. These approaches often prioritize technical and operational aspects, sometimes overlooking the diverse needs of end-users [
26].
IHAF: The IHAF introduces an inclusive design process, actively involving patients, healthcare workers, and architects. This approach ensures that facilities are operationally efficient and cater to all stakeholders’ diverse needs. The IHAF’s emphasis on adaptability accommodates evolving technologies and patient needs, marking a significant shift from traditional, more rigid design methodologies [
29,
37].
User Experience and Satisfaction
Existing approaches: Conventional designs often prioritize operational efficiency and cost-effectiveness, compromising patient comfort and staff well-being. The focus is typically on the physical layout and technical aspects, with less consideration for the experiential aspects of the users [
28].
IHAF: Places a strong emphasis on patient-centric design, ensuring facilities are functional, comforting, and stress-reducing. The IHAF equally values the well-being of healthcare staff, advocating for efficient and positive work environments. This holistic approach to design under the IHAF contrasts sharply with the more practical focus of traditional methods [
27,
30].
Sustainability and Environmental Impact
Existing approaches: Sustainability in traditional healthcare architecture often comes as an afterthought, focusing primarily on energy efficiency and operational cost reduction. While these are important aspects, they only encompass part of the spectrum of sustainability [
35,
36].
IHAF: Integrates eco-friendly practices and green spaces as fundamental components of the design process. This comprehensive approach to sustainability extends beyond mere energy efficiency, encompassing a broader environmental perspective that includes patient and staff well-being, offering a more holistic approach to sustainable healthcare architecture [
33,
38].
This comparative analysis underscores the innovative aspects of IHAF, highlighting its comprehensive, user-centric, and sustainable approach. IHAF addresses the functional requirements of healthcare facilities and prioritizes the well-being of users and the environment, setting a new standard in healthcare architecture.
4.5. Empirical Insights from Evidence-Based Hospital Room Design
This review underscores the intrinsic relationship between architectural design and healthcare quality; therefore, to strengthen the conclusions, we incorporated real data gathered from comprehensive questionnaires focused on healthcare-facility design in the study by Quan et al. [
40]. They offer empirical insights that resonate with our findings, particularly emphasizing the role of evidence-based design in enhancing patient care and staff efficiency in healthcare environments.
Quan et al. developed and validated tools like design checklists and post-occupancy evaluation (POE) tools tailored explicitly for hospital inpatient rooms [
38]. These tools focus on optimizing room layouts to improve patient mobility and reduce falls, aligning seamlessly with our integrated healthcare architecture framework (IHAF), which emphasizes patient-centric and staff-friendly designs. The study’s approach to room layout, ensuring clear, barrier-free access to amenities like bathrooms and accommodating patient needs, is a testament to the importance of thoughtful design in healthcare settings. The usability tests involving healthcare professionals and designers further validate these tools, demonstrating their practical applicability in real-world settings. This aspect of practical implementation is particularly relevant to our discussion on the IHAF model, highlighting the need for theoretical and practical designs.
Moreover, the study’s emphasis on continuous optimization and adaptation in response to evolving research and design practices resonates with our call for innovative and adaptable solutions in healthcare architecture. Quan et al. highlighted that developing evidence-based design (EBD) tools are critical to integrating research evidence in design practices to achieve optimal outcomes [
40]. This reflects our encouragement for a multidisciplinary approach in designing healthcare facilities, which is crucial for addressing the multifaceted challenges healthcare institutions face today.
In conclusion, the findings from Quan et al.’s study provide robust empirical support to our manuscript’s conclusions. They emphasize the significance of adopting evidence-based, user-centric, and adaptable design approaches in healthcare architecture. This approach is not just a theoretical ideal but a practical necessity, as demonstrated by the effective implementation of EBD tools in enhancing healthcare facilities. As we look to the future, fostering collaborative interactions between architects, healthcare professionals, and other vital stakeholders remains instrumental in designing healthcare infrastructures that holistically cater to patient and staff needs, thereby contributing to the vision of sustainable and inclusive architectural practices.
4.6. Limitations and Recommendations for Future Research
Despite extensive research in architecture and health, there are still gaps in the literature. One of the fundamental limitations is the need for more research on the impact of architecture on healthcare in Slovenia, as identified in the Architectural Policy of Slovenia [
2]. Moreover, as stated by Kristl [
3], building a hospital is one of the most challenging tasks for an architect, yet there needs to be more research focused on this specific topic.
Some studies have primarily focused on design aspects, while others have emphasized the importance of sustainability and environmental impact, which can lead to inconsistencies in the literature [
33,
38]. For further research, it would be beneficial to examine how architectural practices can adapt to the specific needs of the Slovenian healthcare system. Additionally, it would be valuable to explore how architecture can address challenges faced by the Slovenian healthcare sector, such as an aging population, the need for sustainable solutions, and the demand for better quality of care.
Integrating advanced technological systems, such as those highlighted by Kumari et al. [
41] and Tanwar et al. [
42] necessitates the re-evaluation of architectural design in healthcare settings. These technologies, including fog computing, cloud computing, and EMRs, are not just peripheral additions but central components that can significantly influence healthcare facilities’ physical architecture and spatial planning. For instance, enhanced digital infrastructure may require redesigning spaces to accommodate advanced computing systems. Similarly, ensuring data privacy through spatial design becomes crucial when integrating EMRs, requiring architects to consider secure, private areas for data handling. Incorporating smart technologies into healthcare environments also demands innovative architectural solutions that seamlessly blend technology with human-centric design [
41,
42].
In light of the COVID-19 pandemic, future research should also explore how this global health crisis has influenced the architecture of healthcare facilities. A post-COVID-19 analysis could provide valuable insights into the necessary architectural adaptations for handling such pandemics, including designing more flexible, adaptable spaces and enhanced infection control measures. Comparing pre- and post-COVID-19 architectural strategies would offer a comprehensive understanding of the changes and adaptations required in healthcare facilities, informed by the lessons learned during the pandemic.
Another critical area for future research involves empirically validating the proposed IHAF model in the Slovenian context. Conducting a comprehensive questionnaire or survey among healthcare professionals, architects, and patients could provide real data to support the conclusions drawn in this study. Such research would assess the practical applicability, effectiveness, and user satisfaction of the IHAF model, offering a grounded perspective on its relevance and impact in actual healthcare settings.
These recommendations aim to bridge the gap between theoretical architectural concepts and practical, real-world applications, ensuring that future healthcare architecture research is comprehensive and contextually relevant.
5. Conclusions
The extensive literature review conducted in this study illuminates the intrinsic relationship between architecture and healthcare, particularly underscoring architecture’s pivotal role in enhancing the quality of care and overall patient experience within healthcare institutions. This relationship is especially relevant within the Slovenian context, where a noticeable gap exists and it highlights an urgent need for more comprehensive and nuanced research in this domain.
Our review has distinctly emphasized three central facets crucial for evaluating healthcare institutions. Firstly, the significance of specific architectural and design approaches was highlighted, noting the profound impact of adhering to established guidelines on healthcare facilities’ final design and functionality. This aspect was further enriched by introducing the integrated healthcare architecture framework (IHAF) which offers a novel and comprehensive approach to healthcare architecture, encompassing user experience, sustainability, and adaptability to technological advancements.
Secondly, the evaluation prioritized the experience and satisfaction of healthcare institution users, including patients, their families, staff, and visitors. The focus was on creating an ambiance that facilitates navigational ease, accessibility, and overall comfort and safety of the spaces. The IHAF model particularly emphasizes patient-centric and staff-friendly designs, ensuring that healthcare facilities are functional but also supportive and comforting environments.
Lastly, the review underscored the importance of sustainable practices in healthcare architecture. These encompass energy efficiency, sustainable material utilization, waste management, and water conservation in the planning and construction phases. The IHAF model integrates these sustainable practices as fundamental components, advocating for environmentally responsible healthcare facilities.
As the architectural landscape evolves, healthcare institutions face multifaceted challenges, ranging from demographic shifts to rapid technological advancements. Addressing these challenges necessitates innovative architectural solutions that cater to immediate healthcare needs while aligning with broader objectives of creating sustainable, efficient, and user-centric built environments. This review highlights the significance of adopting a multidisciplinary approach in designing, planning, and evaluating healthcare facilities. Collaboration between architects, healthcare professionals, and other key stakeholders will be instrumental in creating healthcare infrastructures that holistically cater to the needs of patients and healthcare personnel. This approach contributes to the overarching vision of sustainable and inclusive architectural practices, setting a new standard in healthcare architecture.








{kind=link}
{kind=link}
{kind=link}