The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy




Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Subjects
2.3. Data Collection
2.3.1. Somatometric Characteristics
2.3.2. Quality of Life
2.3.3. Exercise Behavior
2.4. Statistical Analysis
3. Results
3.1. Somatometric Characteristics
3.2. Quality of Life
3.2.1. Control Group
3.2.2. Breast Cancer Group
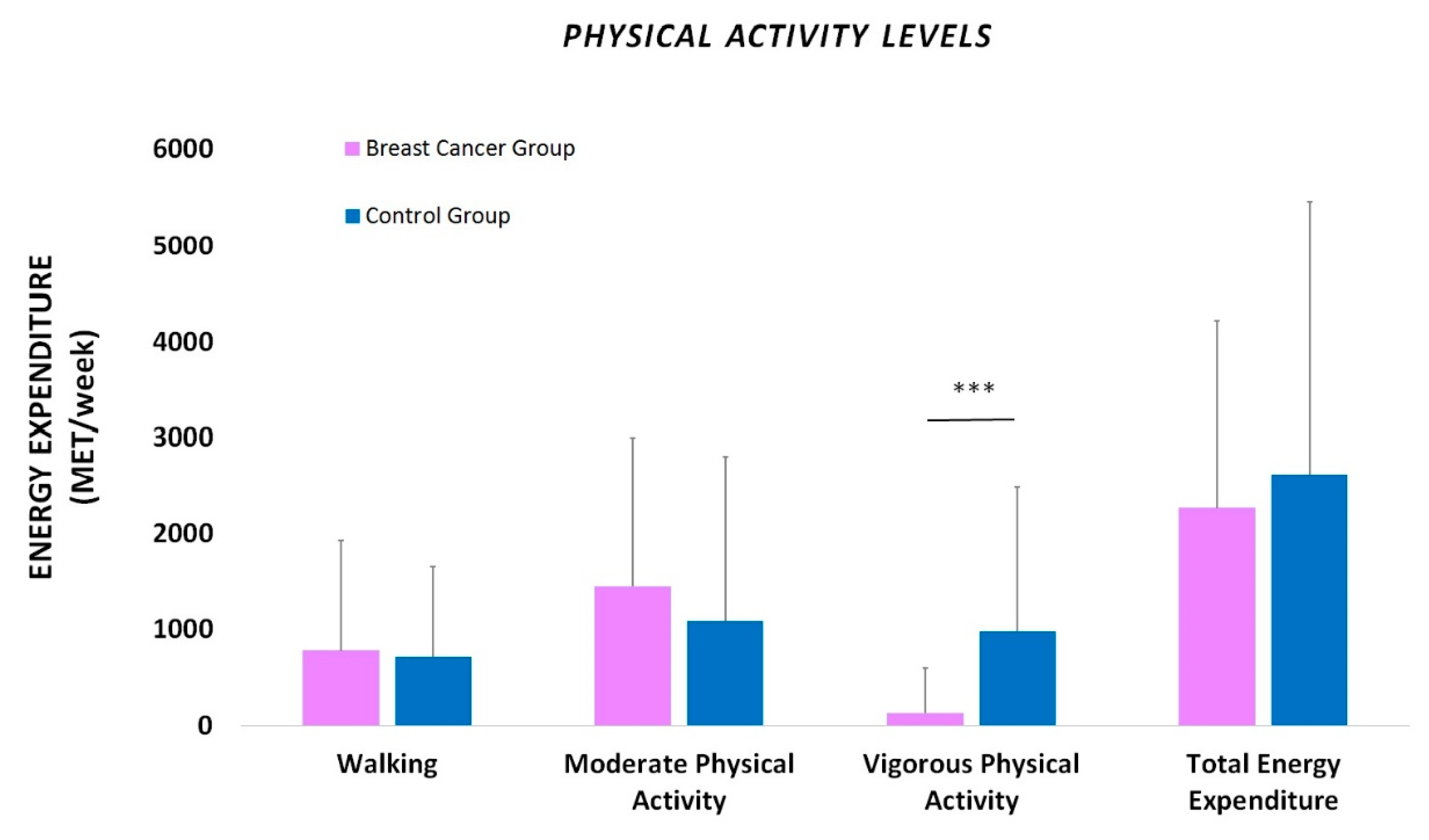
3.3. Exercise Behavior
3.4. Associations between Exercise Behavior and Quality of Life
4. Discussion
5. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Sauer, A.G.; Jemal, A.; Siegel, R.L. Breast cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Devlin, E.J.; Denson, L.A.; Whitford, H.S. Cancer Treatment Side Effects: A Meta-analysis of the Relationship between Response Expectancies and Experience. J. Pain Symptom Manag. 2017, 54, 245–258.e2. [Google Scholar] [CrossRef]
- Stefani, L.; Giorgio, G.; Klika, R. Clinical Implementation of Exercise Guidelines for Cancer Patients: Adaptation of ACSM’s Guidelines to the Italian Model. J. Funct. Morphol. Kinesiol. 2017, 2, 4. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Winters-Stone, K.M.; Bland, K.A.; Campbell, K.L. Updated systematic review of exercise studies in breast cancer survivors: Attention to the principles of exercise training. Br. J. Sports Med. 2019, 53, 504–512. [Google Scholar] [CrossRef]
- Adraskela, K.; Veisaki, E.; Koutsilieris, M.; Philippou, A. Physical Exercise Positively Influences Breast Cancer Evolution. Clin. Breast Cancer 2017, 17, 408–417. [Google Scholar] [CrossRef]
- Bao, T.; Basal, C.; Seluzicki, C.; Li, S.Q.; Seidman, A.D.; Mao, J.J. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: Prevalence, risk factors, and fall risk. Breast Cancer Res. Treat. 2016, 159, 327–333. [Google Scholar] [CrossRef]
- Howden, E.J.; Bigaran, A.; Beaudry, R.; Fraser, S.; Selig, S.; Foulkes, S.; Antill, Y.; Nightingale, S.; Loi, S.; Haykowsky, M.J.; et al. Exercise as a diagnostic and therapeutic tool for the prevention of cardiovascular dysfunction in breast cancer patients. Eur. J. Prev. Cardiol. 2019, 26, 305–315. [Google Scholar] [CrossRef]
- Schirrmacher, V. From chemotherapy to biological therapy: A review of novel concepts to reduce the side effects of systemic cancer treatment (Review). Int. J. Oncol. 2019, 54, 407–419. [Google Scholar]
- Argiles, J.M.; Stemmler, B.; López-Soriano, F.J.; Busquets, S. Inter-tissue communication in cancer cachexia. Nat. Rev. Endocrinol. 2018, 15, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Wonders, K.Y.; Wise, R.; Ondreka, D.; Seitz, T. Supervised, Individualized Exercise Mitigates Symptom Severity during Cancer Treatment. J. Adenocarcinoma Osteosarcoma 2018, 3, 1–5. [Google Scholar]
- Guo, W.; Fensom, G.K.; Reeves, G.K.; Key, T.J. Physical activity and breast cancer risk: Results from the UK Biobank prospective cohort. Br. J. Cancer 2020, 122, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Kehm, R.D.; Genkinger, J.M.; MacInnis, R.J.; John, E.M.; Phillips, K.A.; Dite, G.S.; Milne, R.L.; Zeinomar, N.; Liao, Y.; Knight, J.A.; et al. Recreational Physical Activity Is Associated with Reduced Breast Cancer Risk in Adult Women at High Risk for Breast Cancer: A Cohort Study of Women Selected for Familial and Genetic Risk. Cancer Res. 2020, 80, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Koelwyn, G.J.; Quail, D.F.; Zhang, X.; White, R.M.; Jones, L.W. Exercise-dependent regulation of the tumour microenvironment. Nat. Rev. Cancer 2017, 17, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Hojman, P.; Gehl, J.; Christensen, J.F.; Pedersen, B.K. Molecular Mechanisms Linking Exercise to Cancer Prevention and Treatment. Cell Metab. 2018, 27, 10–21. [Google Scholar] [CrossRef]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. CA Cancer J. Clin. 2016, 66, 43–73. [Google Scholar] [CrossRef]
- Durstine, J.L.; Gordon, B.; Wang, Z.; Luo, X. Chronic disease and the link to physical activity. J. Sport Health Sci. 2013, 2, 3–11. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Campbell, A.M.; Stuiver, M.M.; Pinto, B.M.; Schwartz, A.L.; Morris, G.S.; Ligibel, J.A.; Cheville, A.; Galvão, D.A.; Alfano, C.M.; et al. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef]
- Ramirez-Parada, K.; Courneya, K.S.; Muñiz, S.; Sánchez, C.; Fernández-Verdejo, R. Physical activity levels and preferences of patients with breast cancer receiving chemotherapy in Chile. Support Care Cancer 2019, 27, 2941–2947. [Google Scholar] [CrossRef]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Hong, F.; Ye, W.; Kuo, C.H.; Zhang, Y.; Qian, Y.; Korivi, M. Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 706. [Google Scholar] [CrossRef] [PubMed]
- Young-Afat, D.A.; Van Gils, C.H.; Van Den Bongard, H.J.G.D.; Verkooijen, H.M.; UMBRELLA Study Group. The Utrecht cohort for Multiple BREast cancer intervention studies and Long-term evaLuAtion (UMBRELLA): Objectives, design, and baseline results. Breast Cancer Res. Treat. 2017, 164, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Verket, N.J.; Uhlig, T.; Sandvik, L.; Andersen, M.H.; Tanbo, T.G.; Qvigstad, E. Health-related quality of life in women with endometriosis, compared with the general population and women with rheumatoid arthritis. Acta Obstet. Gynecol. Scand. 2018, 97, 1339–1348. [Google Scholar] [CrossRef]
- Irwin, M.L.; Aiello, E.J.; McTiernan, A.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L.; Gilliland, F.D.; Ballard-Barbash, R. Pre-diagnosis physical activity and mammographic density in breast cancer survivors. Breast Cancer Res. Treat. 2006, 95, 171–178. [Google Scholar] [CrossRef]
- Fassier, P.; Zelek, L.; Partula, V.; Srour, B.; Bachmann, P.; Touillaud, M.; Druesne-Pecollo, N.; Galan, P.; Cohen, P.; Hoarau, H.; et al. Variations of physical activity and sedentary behavior between before and after cancer diagnosis: Results from the prospective population-based NutriNet-Sante cohort. Medicine (Baltim.) 2016, 95, e4629. [Google Scholar] [CrossRef]
- Littman, A.J.; Tang, M.T.; Rossing, M.A. Longitudinal study of recreational physical activity in breast cancer survivors. J. Cancer Surviv. 2010, 4, 119–127. [Google Scholar] [CrossRef]
- Papadopoulos, E.; Mina, D.S. Can we HIIT cancer if we attack inflammation? Cancer Causes Control. 2018, 29, 7–11. [Google Scholar] [CrossRef]
- Harrison, S.; Hayes, S.C.; Newman, B. Level of physical activity and characteristics associated with change following breast cancer diagnosis and treatment. Psychooncology 2009, 18, 387–394. [Google Scholar] [CrossRef]
- Chan, D.S.; Norat, T. Obesity and breast cancer: Not only a risk factor of the disease. Curr. Treat. Options Oncol. 2015, 16, 22. [Google Scholar] [CrossRef]
- Meneses-Echavez, J.F.; Gonzalez-Jimenez, E.; Ramirez-Velez, R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2015, 15, 77. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Haas, M.; Viney, R.; Pearson, S.A.; Haywood, P.; Brown, C.; Ward, R. Incidence and severity of self-reported chemotherapy side effects in routine care: A prospective cohort study. PLoS ONE 2017, 12, e0184360. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.L.; de Heer, H.D.; Bea, J.W. Initiating Exercise Interventions to Promote Wellness in Cancer Patients and Survivors. Oncology (Williston Park) 2017, 31, 711–717. [Google Scholar] [PubMed]
- Kirkham, A.A.; Bland, K.A.; Sayyari, S.; Campbell, K.L.; Davis, M.K. Clinically Relevant Physical Benefits of Exercise Interventions in Breast Cancer Survivors. Curr. Oncol. Rep. 2016, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.; Ghodusi, M. The Relationship between Body Esteem and Hope and Mental Health in Breast Cancer Patients after Mastectomy. Indian J. Palliat. Care 2015, 21, 198–202. [Google Scholar]
- Cvetkovic, J.; Nenadovic, M. Depression in breast cancer patients. Psychiatry Res. 2016, 240, 343–347. [Google Scholar] [CrossRef]
- Nurgali, K.; Jagoe, R.T.; Abalo, R. Editorial: Adverse Effects of Cancer Chemotherapy: Anything New to Improve Tolerance and Reduce Sequelae? Front. Pharmacol. 2018, 9, 245. [Google Scholar] [CrossRef]
- Ruiz-Casado, A.; Martín-Ruiz, A.; Pérez, L.M.; Provencio, M.; Fiuza-Luces, C.; Lucia, A. Exercise and the Hallmarks of Cancer. Trends Cancer 2017, 3, 423–441. [Google Scholar] [CrossRef]
- Buffart, L.M.; Kalter, J.; Sweegers, M.G.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; May, A.M.; Galvão, D.A.; Chinapaw, M.J.; et al. Effects and moderators of exercise on quality of life and physical function in patients with cancer: An individual patient data meta-analysis of 34 RCTs. Cancer Treat. Rev. 2017, 52, 91–104. [Google Scholar] [CrossRef]
- Sweegers, M.G.; Altenburg, T.; Chinapaw, M.J.; Kalter, J.; Verdonck-de Leeuw, I.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.; Brug, J.; et al. Which exercise prescriptions improve quality of life and physical function in patients with cancer during and following treatment? A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2018, 52, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Short, C.E.; Rebar, A.; James, E.L.; Duncan, M.J.; Courneya, K.S.; Plotnikoff, R.C.; Crutzen, R.; Vandelanotte, C. How do different delivery schedules of tailored web-based physical activity advice for breast cancer survivors influence intervention use and efficacy? J. Cancer Surviv. 2017, 11, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.A.; Huedo-Medina, T.B.; Johnson, B.T.; Ryan, S.; Pescatello, L.S. Exercise interventions for cancer survivors: A meta-analysis of quality of life outcomes. Ann. Behav. Med. 2011, 41, 32–47. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants’ Characteristics | Breast Cancer Group (n=94) | Control Group (n=65) |
|---|---|---|
| Age (yrs) | 57.25 ± 13.59 | 49.60 ± 7.80 |
| Body Mass (kg) | 69.49 ± 12.67 | 69.04 ± 5.25 |
| Body Height (m) | 1.61 ± 0.05 | 1.65 ± 0.04 |
| Body Mass Index (kg/m2) | 26.63 ± 5.27 | 25.30 ± 3.95 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maridaki, M.; Papadopetraki, A.; Karagianni, H.; Koutsilieris, M.; Philippou, A. The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy. Sports 2020, 8, 32. https://doi.org/10.3390/sports8030032
Maridaki M, Papadopetraki A, Karagianni H, Koutsilieris M, Philippou A. The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy. Sports. 2020; 8(3):32. https://doi.org/10.3390/sports8030032
Chicago/Turabian StyleMaridaki, Maria, Argyro Papadopetraki, Helen Karagianni, Michael Koutsilieris, and Anastassios Philippou. 2020. "The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy" Sports 8, no. 3: 32. https://doi.org/10.3390/sports8030032
APA StyleMaridaki, M., Papadopetraki, A., Karagianni, H., Koutsilieris, M., & Philippou, A. (2020). The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy. Sports, 8(3), 32. https://doi.org/10.3390/sports8030032