
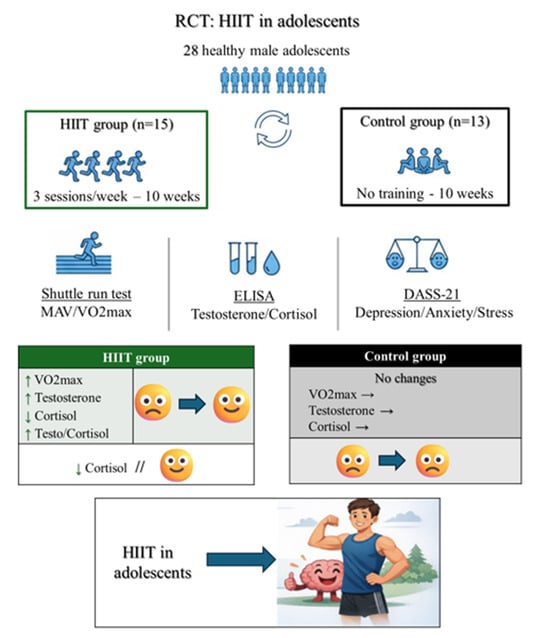
Effects of High-Intensity Interval Training on Steroid Hormones and Psychological Outcomes in Healthy Male Adolescents: A Randomized Controlled Trial

 , , , , ,
, , , , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Ethical Approval
2.3. Sample Size Calculation
2.4. Participants
2.5. Aerobic Performance Measurement
2.6. High-Intensity Interval Training Intervention
2.7. Psychological Evaluations
2.8. Blood Sampling and Laboratory Analysis
2.9. Statistical Analysis
3. Results
3.1. Cardiorespiratory Fitness
3.2. Hormonal Parameters
3.3. Mental Health Measures
3.4. Between-Group Changes in Aerobic Fitness, Hormonal, and Psychological Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CRF | Cardiorespiratory fitness |
| CG | Control group |
| DASS-21 | Depression Anxiety Stress Scales |
| HIIT | High-intensity interval training |
| HIITG | High-intensity interval training group |
| MAS | Maximal aerobic speed |
| VO2max | Maximal oxygen consumption |
References
- Abreu, A.P.; Kaiser, U.B. Pubertal development and regulation. Lancet Diabetes Endocrinol. 2016, 4, 254–264. [Google Scholar] [CrossRef]
- Leahy, A.A.; Mavilidi, M.F.; Smith, J.J.; Hillman, C.H.; Eather, N.; Barker, D.; Lubans, D.R. Review of High-Intensity Interval Training for Cognitive and Mental Health in Youth. Med. Sci. Sports Exerc. 2020, 52, 2224–2234. [Google Scholar] [CrossRef]
- Boisseau, N.; Delamarche, P. Metabolic and hormonal responses to exercise in children and adolescents. Sports Med. 2000, 30, 405–422. [Google Scholar] [CrossRef]
- Spiering, B.A.; Kraemer, W.J.; Vingren, J.L.; Ratamess, N.A.; Anderson, J.M.; Armstrong, L.E.; Nindl, B.C.; Volek, J.S.; Häkkinen, K.; Maresh, C.M. Elevated endogenous testosterone concentrations potentiate muscle androgen receptor responses to resistance exercise. J. Steroid Biochem. Mol. Biol. 2009, 114, 195–199. [Google Scholar] [CrossRef]
- Duke, S.A.; Balzer, B.W.; Steinbeck, K.S. Testosterone and its effects on human male adolescent mood and behavior: A systematic review. J. Adolesc. Health 2014, 55, 315–322. [Google Scholar] [CrossRef]
- Christiansen, J.J.; Djurhuus, C.B.; Gravholt, C.H.; Iversen, P.; Christiansen, J.S.; Schmitz, O.; Weeke, J.; Jørgensen, J.O.; Møller, N. Effects of cortisol on carbohydrate, lipid, and protein metabolism: Studies of acute cortisol withdrawal in adrenocortical failure. J. Clin. Endocrinol. Metab. 2007, 92, 3553–3559. [Google Scholar] [CrossRef]
- Jones, C.; Gwenin, C. Cortisol level dysregulation and its prevalence-Is it nature’s alarm clock? Physiol. Rep. 2021, 8, e14644. [Google Scholar] [CrossRef]
- Janssen, J.A. Impact of physical exercise on endocrine aging. Front. Horm. Res. 2016, 47, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Zouhal, H.; Jayavel, A.; Parasuraman, K.; Hayes, L.D.; Tourny, C.; Rhibi, F.; Laher, I.; Abderrahman, A.B.; Hackney, A.C. Effects of exercise training on anabolic and catabolic hormones with advanced age: A systematic review. Sports Med. 2022, 52, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Wiklund, C.A.; Ekblom, M.M.; Wang, R.; Ekblom, Ö. Associations between physical activity and symptoms of mental health disorders in adolescence: Evidence from the longitudinal Swedish Twin Register. J. Adolesc. Health 2025, 76, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Martin-Smith, R.; Cox, A.; Buchan, D.S.; Baker, J.S.; Grace, F.; Sculthorpe, N. High intensity interval training (HIIT) improves cardiorespiratory fitness (CRF) in healthy, overweight and obese adolescents: A systematic review and meta-analysis of controlled studies. Int. J. Environ. Res. Public Health 2020, 17, 2955. [Google Scholar] [CrossRef]
- Farzad, B.; Gharakhanlou, R.; Agha-Alinejad, H.; Curby, D.G.; Bayati, M.; Bahraminejad, M.; Mäestu, J. Physiological and performance changes from the addition of a sprint interval program to wrestling training. J. Strength Cond. Res. 2011, 25, 2392–2399. [Google Scholar] [CrossRef] [PubMed]
- Zinner, C.; Wahl, P.; Achtzehn, S.; Reed, J.L.; Mester, J. Acute hormonal responses before and after 2 weeks of HIT in well-trained junior triathletes. Int. J. Sports Med. 2014, 35, 316–322. [Google Scholar] [CrossRef]
- Sheykhlouvand, M.; Khalili, E.; Agha-Alinejad, H.; Gharaat, M. Hormonal and physiological adaptations to high-intensity interval training in professional male canoe polo athletes. J. Strength Cond. Res. 2016, 30, 859–866. [Google Scholar] [CrossRef]
- Herbert, P.; Hayes, L.D.; Sculthorpe, N.F.; Grace, F.M. HIIT produces increases in muscle power and free testosterone in male masters athletes. Endocr. Connect. 2017, 6, 430–436. [Google Scholar] [CrossRef]
- Sylta, Ø.; Tønnessen, E.; Sandbakk, Ø.; Hammarström, D.; Danielsen, J.; Skovereng, K.; Rønnestad, B.R.; Seiler, S. Effects of high-intensity training on physiological and hormonal adaptations in well-trained cyclists. Med. Sci. Sports Exerc. 2017, 49, 1137–1146. [Google Scholar] [CrossRef]
- Song, T.; Jilikeha; Deng, Y. Physiological and biochemical adaptations to a sport-specific sprint interval training in male basketball athletes. J. Sports Sci. Med. 2023, 22, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xue, K. Optimizing short sprint interval training for young soccer players: Unveiling optimal rest distributions to maximize physiological adaptations. J. Sports Sci. Med. 2024, 23, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Dote-Montero, M.; Carneiro-Barrera, A.; Martinez-Vizcaino, V.; Ruiz, J.R.; Amaro-Gahete, F.J. Acute effect of HIIT on testosterone and cortisol levels in healthy individuals: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2021, 31, 1722–1744. [Google Scholar] [CrossRef]
- Tao, Y.; Lu, J.; Lv, J.; Zhang, L. Effects of high-intensity interval training on depressive symptoms: A systematic review and meta-analysis. J. Psychosom. Res. 2024, 180, 111652. [Google Scholar] [CrossRef]
- Gaia, J.W.P.; Schuch, F.B.; Ferreira, R.W.; Souza, E.L.; Ferreira, V.M.S.; Pires, D.A. Effects of high-intensity interval training on depressive and anxiety symptoms in healthy individuals: A systematic review and meta-analysis of randomized clinical trials. Scand. J. Med. Sci. Sports 2024, 34, e14618. [Google Scholar] [CrossRef]
- Abassi, W.; Ouerghi, N.; Hammami, M.B.; Jebabli, N.; Feki, M.; Bouassida, A.; Weiss, K.; Knechtle, B. High-intensity interval training reduces liver enzyme levels and improves MASLD-related biomarkers in overweight/obese girls. Nutrients 2025, 17, 164. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.M.; Whitehouse, R.H.; Takaishi, M. Standards from birth to maturity for height, weight, height velocity, and weight velocity: British children, 1965. I. Arch. Dis. Child. 1966, 41, 454–471. [Google Scholar] [CrossRef]
- Léger, L.A.; Lambert, J. A maximal multistage 20-m shuttle run test to predict VO2max. Eur. J. Appl. Physiol. Occup. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef]
- Ouerghi, N.; Fradj, M.K.B.; Bezrati, I.; Khammassi, M.; Feki, M.; Kaabachi, N.; Bouassida, A. Effects of high-intensity interval training on body composition, aerobic and anaerobic performance, and plasma lipids in overweight/obese and normal-weight young men. Biol. Sport 2017, 34, 385–392. [Google Scholar] [CrossRef]
- Buchan, D.S.; Ollis, S.; Thomas, N.E.; Buchanan, N.; Cooper, S.M.; Malina, R.M.; Baker, J.S. Physical activity interventions: Effects of duration and intensity. Scand. J. Med. Sci. Sports 2011, 21, e341–e350. [Google Scholar] [CrossRef]
- Moussa, M.T.; Lovibond, P.; Laube, R.; Megahead, H.A. Psychometric properties of an Arabic version of the depression anxiety stress scales (DASS). Res. Soc. Work. Pract. 2016, 27, 375–386. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Martland, R.; Mondelli, V.; Gaughran, F.; Stubbs, B. Can high-intensity interval training improve physical and mental health outcomes? A meta-review of 33 systematic reviews across the lifespan. J. Sports Sci. 2020, 38, 430–469. [Google Scholar] [CrossRef]
- Belanger, M.J.; Rao, P.; Robbins, J.M. Exercise, physical activity, and cardiometabolic health: Pathophysiologic insights. Cardiol. Rev. 2022, 30, 134–144. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Vélez, R.; García-Alonso, Y.; Alonso-Martínez, A.M.; Izquierdo, M. Association of cardiorespiratory fitness levels during youth with health risk later in life: A systematic review and meta-analysis. JAMA Pediatr. 2020, 174, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.G.R.; Heigenhauser, G.J.F.; Bonen, A.; Spriet, L.L. High-intensity aerobic interval training increases fat and carbohydrate metabolic capacities in human skeletal muscle. Appl. Physiol. Nutr. Metab. 2008, 33, 1112–1123. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Allen, R.P.; Roberson, D.W.; Jurancich, M. Effect of high-intensity interval training on cardiovascular function, VO2max, and muscular force. J. Strength Cond. Res. 2012, 26, 138–145. [Google Scholar] [CrossRef]
- Hossain, M.N.; Lee, J.; Choi, H.; Kwak, Y.S.; Kim, J. The impact of exercise on depression: How moving makes your brain and body feel better. Phys. Act. Nutr. 2024, 28, 43–51. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005, 35, 339–361. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A.; Tworoger, S.S.; Ulrich, C.M.; Yasui, Y.; Irwin, M.L.; Rajan, K.B.; Sorensen, B.; Rudolph, R.E.; Bowen, D.; Stanczyk, F.Z.; et al. Effect of exercise on serum estrogens in postmenopausal women: A 12-month randomized clinical trial. Cancer Res. 2004, 64, 2923–2928. [Google Scholar] [CrossRef]
- Brownlee, K.K.; Moore, A.W.; Hackney, A.C. Relationship between circulating cortisol and testosterone: Influence of physical exercise. J. Sports Sci. Med. 2005, 4, 76–83. [Google Scholar] [PubMed]
- Duclos, M.; Tabarin, A. Exercise and the hypothalamo-pituitary-adrenal axis. Front. Horm. Res. 2016, 47, 12–26. [Google Scholar] [CrossRef]
- Handziski, Z.; Maleska, V.; Petrovska, S.; Nikolik, S.; Mickoska, E.; Dalip, M.; Kostova, E. The changes of ACTH, cortisol, testosterone and testosterone/cortisol ratio in professional soccer players during a competition half-season. Bratisl. Lek. Listy 2006, 107, 259–263. [Google Scholar] [PubMed]
- Romero-Martínez, A.; González-Bono, E.; Lila, M.; Moya-Albiol, L. Testosterone/cortisol ratio in response to acute stress: A possible marker of risk for marital violence. Soc. Neurosci. 2013, 8, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Olds, T.; Curtis, R.; Dumuid, D.; Virgara, R.; Watson, A.; Szeto, K.; O’Connor, E.; Ferguson, T.; Eglitis, E.; et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. Br. J. Sports Med. 2023, 57, 1203–1209. [Google Scholar] [CrossRef]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Hillman, C.H.; Lubans, D.R. High-intensity interval training for cognitive and mental health in adolescents. Med. Sci. Sports Exerc. 2016, 48, 1985–1993. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, X.; Zhang, Y.; Zhang, H. The impact of high-intensity interval training on anxiety: A scoping review. Front. Psychiatry 2025, 16, 1515266. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week of Training | |||||
|---|---|---|---|---|---|
| 1–2 | 3–4 | 5–6 | 7–8 | 9–10 | |
| Number of sets | 3 | 3 | 3 | 3 | 3 |
| Number of races per set | 4 | 6 | 6 | 8 | 6 |
| Run/Active recovery time (s) | 30/30 | 30/30 | 30/30 | 30/30 | 30/30 |
| % MAS (Run/Active recovery) | 100%/50% | 100%/50% | 110%/50% | 100%/50% | 100%/50% |
| Passive recovery time (min) | 5 | 5 | 5 | 5 | 5 |
| Training load (ATU) | 900 | 1350 | 1440 | 1800 | 1350 |
| Weekly training load (ATU) | 2700 | 4050 | 4320 | 5400 | 4050 |
| Control Group (n = 13) | HIIT Group (n = 15) | p a | Time Effect b | Group Effect b | Interaction (Time × Group) b | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | F | ηp2 | F | ηp2 | F | ηp2 | ||
| MAS (km/h) | 11.1 ± 0.55 | 11.2 ± 0.72 | 11.2 ± 0.62 | 11.9 ± 0.64 ***† | 0.707 | 33.5 ### | 0.563 | 1.87 | 0.067 | 6.45 # | 0.199 |
| VO2max (mL/kg/min) | 43.6 ± 3.40 | 44.0 ± 4.03 | 43.7 ± 3.65 | 47.4 ± 3.70 ***† | 0.926 | 28.9 ### | 0.527 | 1.02 | 0.038 | 11.0 ## | 0.298 |
| Testosterone, nmol/L | 14.5 ± 6.48 | 15.1 ± 5.54 | 13.0 ± 7.15 | 16.9 ± 8.29 ** | 0.567 | 14.6 ## | 0.359 | 0.78 | 0.029 | 8.74 ## | 0.252 |
| Cortisol, nmol/L | 408 ± 67.0 | 389 ± 91.8 | 431 ± 78.1 | 374 ± 81.4 * | 0.417 | 18.5 ### | 0.415 | 0.14 | 0.005 | 5.92 # | 0.185 |
| T/C ratio | 0.039 ± 0.02 | 0.042 ± 0.01 | 0.032 ± 0.01 | 0.048 ± 0.02 ** | 0.402 | 14.8 ### | 0.363 | 0.34 | 0.013 | 5.21 # | 0.167 |
| Depression score | 3.85 ± 1.21 | 3.54 ± 1.05 | 3.93 ± 1.03 | 3.40 ± 1.18 | 0.839 | 4.89 # | 0.158 | 0.010 | 0.004 | 1.02 | 0.038 |
| Anxiety score | 2.92 ± 1.12 | 2.62 ± 0.87 | 3.13 ± 1.06 | 2.40 ± 0.83 ** | 0.614 | 12.4 ## | 0.323 | 0.29 | 0.011 | 4.12 | 0.137 |
| Stress score | 4.85 ± 1.95 | 4.54 ± 1.66 | 5.07 ± 1.58 | 3.80 ± 1.21 * | 0.744 | 13.8 ## | 0.347 | 0.11 | 0.004 | 5.78 # | 0.182 |
| Mean (95% Confidence Interval) | p-Value | ||
|---|---|---|---|
| Control Group | HIIT Group | ||
| MAS (km/h) | 0.08 (−0.17, +0.32) | 0.67 (+0.50, +0.84) | <0.001 |
| VO2max (mL/kg/min) | 0.05 (−0.89, +1.80) | 3.77 (+2.78, +4.75) | <0.001 |
| Testosterone, nmol/L | 0.62 (−1.77, +3.00) | 3.94 (+1.55, +6.33) | 0.044 |
| Cortisol, nmol/L | −18.6 (−84.7, +47.5) | −56.6 (−114, +1.26) | 0.357 |
| Testosterone-to-cortisol ratio | 0.003 (−0.007, +0.013) | 0.015 (+0.006, +0.023) | 0.075 |
| Depression score | −0.31 (−0.88, +0.26) | −0.53 (−0.34, +0.27) | 0.637 |
| Anxiety score | −0.31 (−1.06, +0.45) | −0.73 (−1.27, −0.20) | 0.318 |
| Stress score | −0.31 (−1.02, +0.41) | −1.27 (−1.94, −0.59) | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Ouerghi, N.; Abassi, W.; Jebabli, N.; Hammami, M.B.; Bouassida, A.; Weiss, K.; Rosemann, T.; Feki, M.; Knechtle, B. Effects of High-Intensity Interval Training on Steroid Hormones and Psychological Outcomes in Healthy Male Adolescents: A Randomized Controlled Trial. Sports 2026, 14, 209. https://doi.org/10.3390/sports14050209
Ouerghi N, Abassi W, Jebabli N, Hammami MB, Bouassida A, Weiss K, Rosemann T, Feki M, Knechtle B. Effects of High-Intensity Interval Training on Steroid Hormones and Psychological Outcomes in Healthy Male Adolescents: A Randomized Controlled Trial. Sports. 2026; 14(5):209. https://doi.org/10.3390/sports14050209
Chicago/Turabian StyleOuerghi, Nejmeddine, Wissal Abassi, Nidhal Jebabli, Mohamed Bessem Hammami, Anissa Bouassida, Katja Weiss, Thomas Rosemann, Moncef Feki, and Beat Knechtle. 2026. "Effects of High-Intensity Interval Training on Steroid Hormones and Psychological Outcomes in Healthy Male Adolescents: A Randomized Controlled Trial" Sports 14, no. 5: 209. https://doi.org/10.3390/sports14050209
APA StyleOuerghi, N., Abassi, W., Jebabli, N., Hammami, M. B., Bouassida, A., Weiss, K., Rosemann, T., Feki, M., & Knechtle, B. (2026). Effects of High-Intensity Interval Training on Steroid Hormones and Psychological Outcomes in Healthy Male Adolescents: A Randomized Controlled Trial. Sports, 14(5), 209. https://doi.org/10.3390/sports14050209