
Fitness Trainers’ Educational Qualification and Experience and Its Association with Their Trainees’ Musculoskeletal Pain: A Cross-Sectional Study

 ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Participant’s Recruitment Criteria
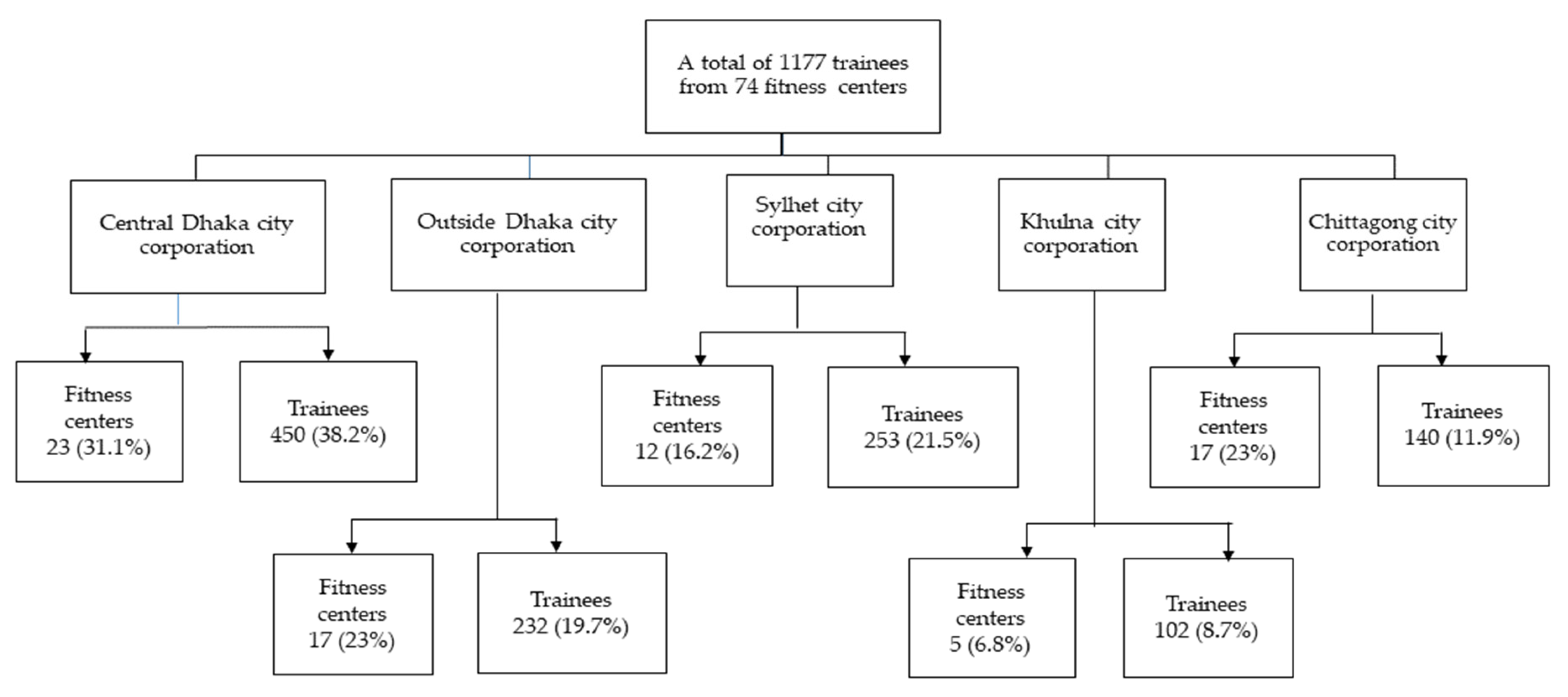
2.3. Sample and Sample Size
2.4. Survey Administration
2.5. Variables Measurement
2.5.1. Explanatory Variables
2.5.2. Outcomes
2.5.3. Covariates
2.6. Survey Validation
2.7. Ethical Statement
2.8. Statistical Analysis
3. Results
3.1. Demographic Details of the Trainees
3.2. Association of Trainers’ Educational Qualifications and Experience with Trainees’ Musculoskeletal Pain
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Riseth, L.; Nøst, T.H.; Nilsen, T.I.L.; Steinsbekk, A. Long-term members’ use of fitness centers: A qualitative study. BMC Sports Sci. Med. Rehabil. 2019, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Gerovasili, V.; Agaku, I.T.; Vardavas, C.I.; Filippidis, F.T. Levels of physical activity among adults 18–64 years old in 28 European countries. Prev. Med. 2015, 81, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Utrition, N.; Ctivity, P.H.A.; Besity, O. 2021 Physical Activity Council’s Overview Report on U.S. Participation. 2021, pp. 1–17. Available online: https://www.physicalactivitycouncil.org/ (accessed on 26 May 2021).
- Eurobarometer on Sport and Physical Activity. 2014. Available online: https://ec.europa.eu/commission/presscorner/detail/en/MEMO_14_207 (accessed on 4 June 2021).
- Waryasz, G.R.; Daniels, A.H.; Gil, J.A.; Suric, V.; Eberson, C.P. Personal trainer demographics, current practice trends and common trainee injuries. Orthop. Rev. 2016, 8, 6600. [Google Scholar] [CrossRef] [PubMed]
- Talpey, S.W.; Siesmaa, E.J. Sports Injury Prevention: The Role of the Strength and Conditioning Coach. Strength Cond. J. 2017, 39, 14–19. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Fernández-De-Las-Peñas, C.; Graven-Nielsen, T. Basic aspects of musculoskeletal pain: From acute to chronic pain. J. Man. Manip. Ther. 2011, 19, 186–193. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Nalamasu, R.; Salem, G.I.; LeQuang, J.A.K.; Pergolizzi, J.V.; Christo, P.J. Management of Musculoskeletal Pain: An Update with Emphasis on Chronic Musculoskeletal Pain. Pain Ther. 2021, 10, 181–209. [Google Scholar] [CrossRef] [PubMed]
- Melton, D.I.; Katula, J.A.; Mustian, K.M. The Current State of Personal Training: An Industry Perspective of Personal Trainers in a Small Southeast Community. J. Strength Cond. Res. 2008, 22, 883–889. [Google Scholar] [CrossRef]
- Malek, M.H.; Nalbone, D.P.; Berger, D.E.; Coburn, J.W. Importance of health science education for personal fitness trainers. J. Strength Cond. Res. 2002, 16, 19–24. [Google Scholar] [PubMed]
- Gray, S.E.; Finch, C.F. The causes of injuries sustained at fitness facilities presenting to Victorian emergency departments—Identifying the main culprits. Inj. Epidemiol. 2015, 2, 6. [Google Scholar] [CrossRef]
- Garrick, J.G.; Gillien, D.M.; Whiteside, P. The epidemiology of aerobic dance injuries. Am. J. Sports Med. 1986, 14, 67–72. [Google Scholar] [CrossRef]
- Kerr, Z.Y.; Collins, C.L.; Comstock, R.D. Epidemiology of Weight Training-Related Injuries Presenting to United States Emergency Departments, 1990 to 2007. Am. J. Sports Med. 2010, 38, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Alabbad, M.; Muaidi, Q. Incidence and prevalence of weight lifting injuries: An update. Saudi J. Sport Med. 2016, 16, 15–19. [Google Scholar]
- Shimozaki, K.; Nakase, J.; Yoshioka, K.; Takata, Y.; Asai, K.; Kitaoka, K.; Tsuchiya, H. Incidence rates and characteristics of abnormal lumbar findings and low back pain in child and adolescent weightlifter: A prospective three-year cohort study. PLoS ONE 2018, 13, e0206125. [Google Scholar] [CrossRef]
- Gray, S.E.; Finch, C.F. Epidemiology of Hospital-Treated Injuries Sustained by Fitness Participants. Res. Q. Exerc. Sport 2014, 86, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, T.; Genç, A.; Göz, E. The Nordic Musculoskeletal Questionnaire: Cross-cultural adaptation into Turkish assessing its psychometric properties. Disabil. Rehabil. 2016, 38, 2153–2160. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Ohlsson, K.; Attewell, R.G.; Johnsson, B.; Ahlm, A.; Skerfving, S. An assessment of neck and upper extremity disorders by ques-tionnaire and clinical examination. Ergonomics 1994, 37, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Gouws, C.; Millard, L.; Naude, A.; Meyer, J.-W.; Shaw, B.S.; Shaw, I. Educational Framework for Coaches on Injury Prevention in Adolescent Team Sports. Asian J. Sports Med. 2020, 11, e106617. [Google Scholar] [CrossRef]
- Saunders, N.; Otago, L.; Romiti, M.; Donaldson, A.; White, P.; Finch, C.F. Coaches’ perspectives on implementing an evidence-informed injury prevention programme in junior community netball. Br. J. Sports Med. 2010, 44, 1128–1132. [Google Scholar] [CrossRef]
- Chidile, M.; Chidiebere, N.S.; James, A.C.; Chukwuebuka, O.; Ann, N.C.; Blessing, N.I.; Adaigwe, A.I.; Arinze, O.C.; Ogochukwu, U.; Chika, E.E.; et al. Prevalence and Pattern of Musculoskeletal Injuries among Recreational Wightlifters in Nnewi, Nigeria. Int. J. Sports Exerc. Med. 2021, 7, 202. [Google Scholar] [CrossRef]
- Gabbett, T.J. The training—Injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sports Med. 2016, 50, 273–280. Available online: http://bjsm.bmj.com/content/50/5/273.abstract (accessed on 30 May 2022). [CrossRef] [PubMed]


{kind=link}
| Variable | n (%) | Missing Value (n) | No Pain, n (%) | Presence of Pain, n (%) | p-Value | |
|---|---|---|---|---|---|---|
| Total sample | 1177 (100) | 659 (56) | 518 (44) | |||
| Gender | Male | 1086 (92.3) | 0 | 595 (54.8) | 491 (45.2) | 0.004 |
| Female | 91 (7.7) | 64 (70.3) | 27 (29.7) | |||
| Age group | 15–25 | 586 (49.8) | 0 | 380 (64.8) | 206 (35.2) | <0.001 |
| 26–35 | 493 (41.9) | 246 (49.9) | 247 (50.1) | |||
| >35 | 98 (8.3) | 33 (33.7) | 65 (66.3) | |||
| BMI category A | Underweight | 317 (26.93) | 241 | 230 (72.6) | 87 (27.4) | <0.001 |
| Healthy weight | 569 (48.34) | 285 (50.1) | 284 (49.9) | |||
| Overweight/Obese | 50 (4.24) | 19 (38) | 31 (62) | |||
| Occupation | Student | 473 (40.2) | 0 | 318 (67.2) | 155 (32.8) | <0.001 |
| Employed | 634 (53.8) | 311 (49.1) | 323 (50.9) | |||
| Homemaker/Unemployed | 70 (6) | 30 (42.9) | 40 (57.1) | |||
| Purpose of GYM joining | Losing weight | 268 (22.7) | 0 | 101 (37.7) | 167 (62.3) | <0.001 |
| Physical fitness | 626 (53.2) | 373 (59.6) | 253 (40.4) | |||
| Bodybuilding | 269 (22.9) | 181 (67.3) | 88 (32.7) | |||
| Recreation | 14 (1.2) | 4 (28.6) | 10 (71.4) | |||
| Hours spent working out in a day | <1 h | 62 (5.3) | 0 | 28 (45.2) | 34 (54.8) | 0.189 |
| 1 h | 574 (48.8) | 321 (55.9) | 253 (44.1) | |||
| 2 h or more | 541 (45.9) | 310 (57.3) | 231 (42.7) | |||
| Type of exercise B | Aerobic | 187 (15.9) | 0 | 58 (31.1) | 129 (68.9) | <0.001 |
| Non-aerobic | 389 (33.0) | 230 (59.1) | 159 (40.9) | |||
| Both | 601 (51.1) | 371 (61.7) | 230 (38.3) | |||
| Over exercise | No | 886 (75.2) | 0 | 536 (60.5) | 350 (39.5) | <0.001 |
| Yes | 291 (24.8) | 123 (42.3) | 168 (57.7) | |||
| Wrong holding C | No | 947 (80.4) | 0 | 570 (60.2) | 377 (39.8) | <0.001 |
| Yes | 230 (19.6) | 89 (38.7) | 141 (61.3) | |||
| Overweight lifting | No | 918 (77.9) | 0 | 569 (62) | 349 (38) | <0.001 |
| Yes | 259 (22.1) | 90 (34.7) | 169 (65.3) | |||
| Lack of workout knowledge | No | 997 (84.8) | 1 | 624 (62.6) | 373 (37.4) | <0.001 |
| Yes | 179 (15.2) | 34 (19) | 145 (81) | |||
| Education of the trainer D | No educational degree | 450 (38.3) | 0 | 274 (60.9) | 176 (39.1) | 0.004 |
| Certificate course | 417 (35.4) | 219 (52.5) | 198 (47.5) | |||
| Diploma degree | 175 (14.8) | 83 (47.4) | 92 (52.6) | |||
| Bachelor/Master degree | 135 (11.5) | 83 (61.5) | 52 (38.5) | |||
| Experience of the trainer E | No or <1 year | 61 (5.2) | 0 | 19 (31.1) | 42 (68.9) | <0.001 |
| 1–5 years | 609 (51.7) | 330 (54.2) | 279 (45.8) | |||
| >5 years | 507 (43.1) | 310 (61.1) | 197 (38.9) | |||
| Variables | Unadjusted Analysis | Adjusted Analysis 1 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Education of the trainer A | ||||
| No educational degree | 1.77 (1.12–2.78) | 0.01 | 1.41 (0.76–2.62) | 0.28 |
| Certificate course | 1.44 (0.97–2.15) | 0.07 | 1.43 (0.81–2.52) | 0.22 |
| Diploma degree | 1.03 (0.69–1.52) | 0.90 | 0.88 (0.51–1.53) | 0.66 |
| Bachelor/Master degree | 1.00 | 1.00 | ||
| Experience of the trainer B | ||||
| No or ≤1 year | 3.48 (1.97–6.15) | <0.001 | 2.53 (1.18–5.44) | 0.02 |
| 1–5 years | 1.33 (1.05–1.69) | 0.02 | 1.12 (0.82–1.54) | 0.48 |
| >5 years | 1.00 | 1.00 | ||
| Variables | Unadjusted | Adjusted 1 | ||
|---|---|---|---|---|
| IRR (95% CI) | p-Value | IRR (95% CI) | p-Value | |
| Education of the trainer A | ||||
| No educational degree | 1.07 (0.82–1.41) | 0.581 | 0.92 (0.68–1.26) | 0.637 |
| Certificate course | 1.32 (1.01–1.72) | 0.039 | 1.16 (0.85–1.57) | 0.332 |
| Diploma degree | 1.33 (0.98–1.80) | 0.059 | 1.08 (0.76–1.53) | 0.642 |
| Bachelor/master degree | 1.00 | 1.00 | ||
| Experience of the trainer B | ||||
| No or <1 year | 1.95 (1.47–2.57) | <0.001 | 2.04 (1.50–2.79) | <0.001 |
| 1–5 years | 1.21 (1.03–1.41) | 0.020 | 1.26 (1.05–1.51) | 0.011 |
| >5 years | 1.00 | 1.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, S.; Rashid, M.; Sarkar, A.-s.; Islam, M.J.; Akter, R.; Rahman, M.; Islam, S.; Sheel, D.; Polash, S.A.; Akter, M.; et al. Fitness Trainers’ Educational Qualification and Experience and Its Association with Their Trainees’ Musculoskeletal Pain: A Cross-Sectional Study. Sports 2022, 10, 129. https://doi.org/10.3390/sports10090129
Ahmed S, Rashid M, Sarkar A-s, Islam MJ, Akter R, Rahman M, Islam S, Sheel D, Polash SA, Akter M, et al. Fitness Trainers’ Educational Qualification and Experience and Its Association with Their Trainees’ Musculoskeletal Pain: A Cross-Sectional Study. Sports. 2022; 10(9):129. https://doi.org/10.3390/sports10090129
Chicago/Turabian StyleAhmed, Sohel, Mamunur Rashid, Abu-sufian Sarkar, Mohammad Jahirul Islam, Rahemun Akter, Masudur Rahman, Shahana Islam, Devjanee Sheel, Sarwar Alam Polash, Mahfuza Akter, and et al. 2022. "Fitness Trainers’ Educational Qualification and Experience and Its Association with Their Trainees’ Musculoskeletal Pain: A Cross-Sectional Study" Sports 10, no. 9: 129. https://doi.org/10.3390/sports10090129
APA StyleAhmed, S., Rashid, M., Sarkar, A.-s., Islam, M. J., Akter, R., Rahman, M., Islam, S., Sheel, D., Polash, S. A., Akter, M., Afride, S., & Kader, M. (2022). Fitness Trainers’ Educational Qualification and Experience and Its Association with Their Trainees’ Musculoskeletal Pain: A Cross-Sectional Study. Sports, 10(9), 129. https://doi.org/10.3390/sports10090129