
Does Electrical Stimulation through Nerve Conduits Improve Peripheral Nerve Regeneration?—A Systematic Review


 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
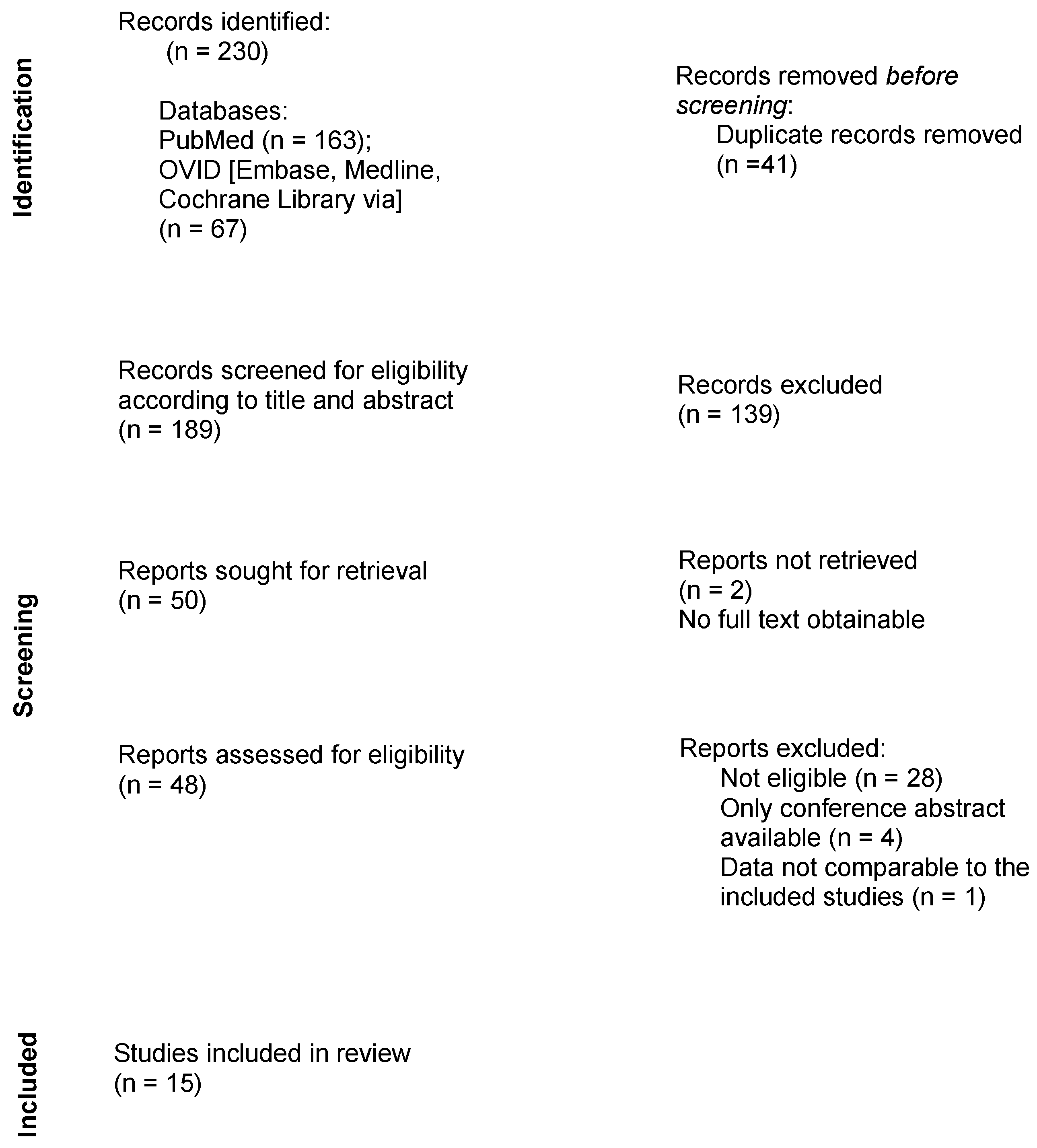
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
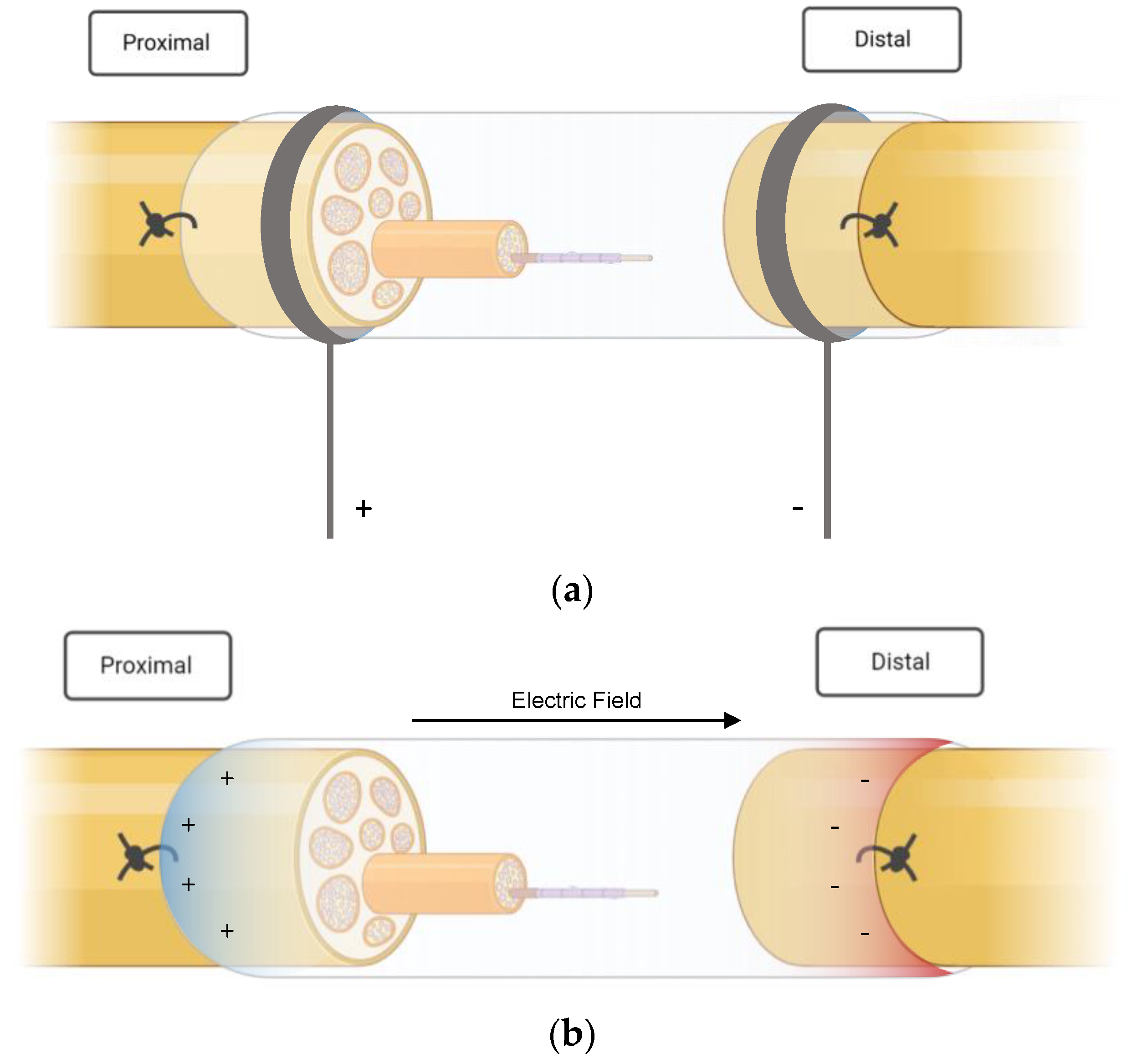
3.1. NGC Types and ES Protocols
3.2. Outcome Measures
3.2.1. Electrophysiological Tests
3.2.2. Functional Evaluation
3.2.3. Histopathological and Morphological Findings
3.2.4. Muscle Atrophy
3.3. Complications
4. Discussion
4.1. ES Protocols
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huckhagel, T.; Nüchtern, J.; Regelsberger, J.; Lefering, R. Nerve injury in severe trauma with upper extremity involvement: Evaluation of 49,382 patients from the TraumaRegister DGU® between 2002 and 2015. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 76. [Google Scholar] [CrossRef] [PubMed]
- Huckhagel, T.; Nüchtern, J.; Regelsberger, J.; Gelderblom, M.; Lefering, R. Nerve trauma of the lower extremity: Evaluation of 60,422 leg injured patients from the TraumaRegister DGU® between 2002 and 2015. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 40. [Google Scholar] [CrossRef] [PubMed]
- Grinsell, D.; Keating, C.P. Peripheral Nerve Reconstruction after Injury: A Review of Clinical and Experimental Therapies. BioMed Res. Int. 2014, 2014, 698256. [Google Scholar] [CrossRef] [PubMed]
- Elzinga, K.; Tyreman, N.; Ladak, A.; Savaryn, B.; Olson, J.; Gordon, T. Brief electrical stimulation improves nerve regeneration after delayed repair in Sprague Dawley rats. Exp. Neurol. 2015, 269, 142–153. [Google Scholar] [CrossRef]
- Arslantunali, D.; Dursun, T.; Yucel, D.; Hasirci, N.; Hasirci, V. Peripheral nerve conduits: Technology update. Med. Devices 2014, 7, 405–424. [Google Scholar] [CrossRef]
- Lee, S.K.; Wolfe, S.W. Peripheral nerve injury and repair. J. Am. Acad. Orthop. Surg. 2000, 8, 243–252. [Google Scholar] [CrossRef]
- Kubiak, C.A.; Kung, T.A.; Brown, D.L.; Cederna, P.S.; Kemp, S.W.P. State-of-The-Art techniques in treating peripheral nerve injury. Plast. Reconstr. Surg. 2018, 141, 702–710. [Google Scholar] [CrossRef]
- Ray, W.Z.; Mackinnon, S.E. Management of nerve gaps: Autografts, allografts, nerve transfers, and end-to-side neurorrhaphy. Exp. Neurol. 2010, 223, 77–85. [Google Scholar] [CrossRef]
- Konofaos, P. Nerve Repair by Means of Tubulization: Past, Present, Future. J. Reconstr. Microsurg. 2013, 29, 149–164. [Google Scholar] [CrossRef]
- Anderson, M.; Shelke, N.B.; Manoukian, O.S.; Yu, X.; McCullough, L.D.; Kumbar, S.G. Peripheral nerve regeneration strategies: Electrically stimulating polymer based nerve growth conduits. Crit. Rev.™ Biomed. Eng. 2015, 43, 2–3. [Google Scholar] [CrossRef]
- Seckel, B.R.; Chiu, T.H.; Sidman, R.L. Nerve regeneration through synthethic biodegradable nerve guides: Regulation by the target organ. Plast. Reconstr. Surg. 1984, 74, 173–181. [Google Scholar] [CrossRef]
- Williams, L.R.; Longo, F.M.; Powell, H.C.; Lundborg, G.; Varon, S. Spatial-Temporal progress of peripheral nerve regeneration within a silicone chamber: Parameters for a bioassay. J. Comp. Neurol. 1983, 218, 460–470. [Google Scholar] [CrossRef]
- Johnson, E.O.; Soucacos, P.N. Nerve repair: Experimental and clinical evaluation of biodegradable artificial nerve guides. Injury 2008, 39, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Rich, K.M.; Alexander, T.; Pryor, J. Nerve Growth Factor Enhances Regeneration through Silicone Chambers. Exp. Neurol. 1989, 170, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, A.; Schmidt, C.E. Electrical stimulation alters protein adsorption and nerve cell interactions with electrically conducting biomaterials. Biomaterials 2001, 22, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Durgam, H.; Sapp, S.; Deister, C.; Khaing, Z.; Chang, E.; Luebben, S.; Schmidt, C.E. Novel Degradable Co-polymers of Polypyrrole Support Cell Proliferation and Enhance Neurite Out-Growth with Electrical Stimulation. J. Biomater. Sci. 2010, 21, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Runge, M.B.; Dadsetan, M.; Baltrusaitis, J.; Ruesink, T.; Lu, L.; Windebank, A.J.; Yaszemski, M.J. Development of electrically conductive oligo(polyethylene glycol) fumarate-polypyrrole hydrogels for nerve regeneration. Biomacromolecules 2010, 11, 2845–2853. [Google Scholar] [CrossRef]
- Quigley, A.F.; Razal, J.M.; Thompson, B.C.; Moulton, S.E.; Kita, M.; Kennedy, E.L.; Clark, G.M.; Wallace, G.G.; Kapsa, R.M.I. A conducting-polymer platform with biodegradable fibers for stimulation and guidance of axonal growth. Adv. Mater. 2009, 21, 4393–4397. [Google Scholar] [CrossRef]
- Xu, H.; Holzwarth, J.M.; Yan, Y.; Xu, P.; Zheng, H.; Yin, Y.; Li, S.; Ma, P.X. Conductive PPY/PDLLA conduit for peripheral nerve regeneration. Biomaterials 2014, 35, 225–235. [Google Scholar] [CrossRef]
- Maeng, W.Y.; Tseng, W.L.; Li, S.; Koo, J.; Hsueh, Y.Y. Electroceuticals for peripheral nerve regeneration. Biofabrication 2022, 14, 4. [Google Scholar] [CrossRef]
- Willand, M.P. Electrical stimulation enhances reinnervation after nerve injury. Eur. J. Transl. Myol. 2015, 25, 243–248. [Google Scholar] [CrossRef]
- Fang, Z.; Ge, X.; Chen, X.; Xu, Y.; Yuan, W.E.; Ouyang, Y. Enhancement of sciatic nerve regeneration with dual delivery of vascular endothelial growth factor and nerve growth factor genes. J. Nanobiotechnol. 2020, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.M.; Curran, M.W.T.; Gordon, T. Neuroscience The use of brief post-surgical low frequency electrical stimulation to enhance nerve regeneration in clinical practice. J. Physiol. 2016, 594, 3553–3559. [Google Scholar] [CrossRef]
- Cheng, W.L.; Lin, C.C.K. The effects of different electrical stimulation protocols on nerve regeneration through silicone conduits. J. Trauma-Inj. Infect. Crit. Care 2004, 56, 1241–1246. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.F.; Hsu, S.T.; Chen, C.C.; Yao, C.H.; Lin, J.H.; Chen, Y.H.; Chen, Y.S. Effects of electrical stimulation on peripheral nerve regeneration in a silicone rubber conduit in taxol-treated rats. Materials 2020, 13, 1063. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Kao, C.H.; Cheng, Y.K.; Chen, J.J.J.; Yao, C.H.; Chen, Y.S. Current-modulated electrical stimulation as a treatment for peripheral nerve regeneration in diabetic rats. Restor. Neurol. Neurosci. 2014, 32, 437–446. [Google Scholar] [CrossRef]
- Lin, Y.C.; Kao, C.H.; Chen, C.C.; Ke, C.J.; Yao, C.H.; Chen, Y.S. Time-course effect of electrical stimulation on nerve regeneration of diabetic rats. PLoS ONE 2015, 10, e0116711. [Google Scholar] [CrossRef] [PubMed]
- MacEwan, M.R.; Zellmer, E.R.; Wheeler, J.J.; Burton, H.; Moran, D.W. Regenerated sciatic nerve axons stimulated through a chronically implanted macro-sieve electrode. Front. Neurosci. 2016, 10, 557. [Google Scholar] [CrossRef]
- Chen, X.; Liu, C.; Huang, Z.; Pu, X.; Shang, L.; Yin, G.; Xue, C. Preparation of carboxylic graphene oxide-composited polypyrrole conduits and their effect on sciatic nerve repair under electrical stimulation. J. Biomed. Mater. Res.—Part A 2019, 107, 2784–2795. [Google Scholar] [CrossRef]
- Song, J.; Sun, B.; Liu, S.; Chen, W.; Zhang, Y.; Wang, C.; Mo, X.; Che, J.; Ouyang, Y.; Yuan, W.; et al. Polymerizing pyrrole coated poly (l-lactic acid-co-ε-caprolactone) (PLCL) conductive nanofibrous conduit combined with electric stimulation for long-range peripheral nerve regeneration. Front. Mol. Neurosci. 2016, 9, 117. [Google Scholar] [CrossRef]
- Sun, Y.; Quan, Q.; Meng, H.; Zheng, Y.; Peng, J.; Hu, Y.; Feng, Z.; Sang, X.; Qiao, K.; He, W.; et al. Enhanced Neurite Outgrowth on a Multiblock Conductive Nerve Scaffold with Self-Powered Electrical Stimulation. Adv. Healthc. Mater. 2019, 8, 1900127. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, K.; Xing, Y.; Yu, Q. Lysine-doped polypyrrole/spider silk protein/poly(l-lactic) acid containing nerve growth factor composite fibers for neural application. Mater. Sci. Eng. C 2015, 56, 564–573. [Google Scholar] [CrossRef]
- Zhao, Y.; Liang, Y.; Ding, S.; Zhang, K.; Mao, H.Q.; Yang, Y. Application of conductive PPy/SF composite scaffold and electrical stimulation for neural tissue engineering. Biomaterials 2020, 255, 120164. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zhang, Y.; Lu, L.; Hu, X.; Luo, Z. Electrical stimulation accelerates nerve regeneration and functional recovery in delayed peripheral nerve injury in rats. Eur. J. Neurosci. 2013, 38, 3691–3701. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Zhao, Y.; Chen, F.; Xiao, A.; Du, Q.; Dong, Q.; Ke, M.; Liang, X.; Zhou, Q.; Chen, Y. Conductive hydroxyethyl cellulose/soy protein isolate/polyaniline conduits for enhancing peripheral nerve regeneration via electrical stimulation. Front. Bioeng. Biotechnol. 2020, 8, 709. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, W.; Xie, H.; Wang, J.; Zhang, L.; Wang, Z.; Wang, L. CNT/Sericin Conductive Nerve Guidance Conduit Promotes Functional Recovery of Transected Peripheral Nerve Injury in a Rat Model. ACS Appl. Mater. Interfaces 2020, 12, 36860–36872. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Jin, Y.; Luo, Z.; Yang, W.; Xie, H.; Huang, K.; Wang, L. A neuroprotective sericin hydrogel as an effective neuronal cell carrier for the repair of ischemic stroke. ACS Appl. Mater. Interfaces 2015, 7, 24629–24640. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, X.; Zuo, S.; Xin, J.; Zhang, P. Bridging peripheral nerves using a deacetyl chitin conduit combined with short-term electrical stimulation. Neural Regen. Res. 2014, 9, 1075–1078. [Google Scholar] [CrossRef]
- Lee, T.H.; Pan, H.; Kim, I.S.; Kim, J.K.; Cho, T.H.; Oh, J.H.; Yoon, Y.B.; Lee, J.H.; Hwang, S.J.; Kim, S.J. Functional regeneration of a severed peripheral nerve with a 7-mm gap in rats through the use of an implantable electrical stimulator and a conduit electrode with collagen coating. Neuromodulation 2010, 13, 299–305. [Google Scholar] [CrossRef]
- Wang, L.; Lu, C.; Yang, S.; Sun, P.; Wang, Y.; Guan, Y.; Liu, S.; Cheng, D.; Meng, H.; Wang, Q.; et al. A fully biodegradable and self-electrified device for neuroregenerative medicine. Sci. Adv. 2020, 6, eabc6686. [Google Scholar] [CrossRef]
- Molin, C.J.; Punga, A.R.; Punga, A.R. Compound motor action potential: Electrophysiological marker for muscle training. J. Clin. Neurophysiol. 2014, 33, 340–345. [Google Scholar] [CrossRef]
- Mitsuma, S.; Van den Bergh, P.; Rajabally, Y.A.; Van Parijs, V.; Martin-Lamb, D.; Sonoo, M.; Inaba, A.; Shimizu, T.; Isose, S.; Sato, Y.; et al. Effects of low frequency filtering on distal compound muscle action potential duration for diagnosis of CIPD: A Japanese-European multicenter prospective study. Clin. Neurophysiol. 2014, 125, 1805–1810. [Google Scholar]
- Lee, T.H.; Pan, H.; Kim, I.S.; Hwang, S.J.; Kim, S.J. Functional regeneration of severed peripheral nerve using an implantable electrical stimulator. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1511–1514. [Google Scholar] [CrossRef]
- Elabd, R.; Alabdulkarim, A.; Alsabah, S.; Hazan, J.; Alhalabi, B.; Thibaudeau, S. Role of Electrical Stimulation in Peripheral Nerve Regeneration: A Systematic Review. Plast. Reconstr. Surg.-Glob. Open 2022, 10, E4115. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.J.; Wu, M.H.; Tai, C.J. Direct electrical stimulation on the injured ulnar nerve using acupuncture needles combined with rehabilitation accelerates nerve regeneration and functional recovery—A case report. Complement. Ther. Med. 2016, 24, 103–107. [Google Scholar] [CrossRef]
- Lu, M.C.; Ho, C.Y.; Hsu, S.F.; Lee, H.C.; Lin, J.H.; Yao, C.H.; Chen, Y.S. Effects of electrical stimulation at different frequencies on regeneration of transected peripheral nerve. Neurorehabil. Neural Repair 2008, 22, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.; Lin, Y.; Tsai, F.; Huang, C. Timing of Applying Electrical Stimulation Is an Important Factor Deciding the Success Rate and Maturity of Regenerating Rat Sciatic Nerves. Neurorehabil. Neural Repair 2010, 24, 730–735. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Search Terms | OVID (Embase, Medline, Cochrane Library) | PubMed |
|---|---|---|
| Nerve conduit (1) | [1 AND 3] | [1 AND 3] |
| Nerve guidance conduit (2) | OR [1 AND 4] | OR [1 AND 4] |
| Electrical stimulation (3) | OR [1 AND 5] | OR [2 AND 3] |
| Electrically conducting (4) | OR [2 AND 3] | OR [2 AND 4] |
| Electrically conductive (5) | OR [2 AND 4] | |
| OR [2 AND 5] |
| Authors, Year. | N | Nerve Defect | NGC Type | ES Protocol | Follow-Up | (Comparative/Control) Groups | |
|---|---|---|---|---|---|---|---|
| Chen et al. [29], 2019 | 27 | Sciatic nerve, 10 mm | C-GO/PPy/PLLA | 1 V, 20 Hz 1 h/day, 7 days 30 min/day for 3 weeks | 4, 8, 12 weeks post-treatment | Autograft, same NGC-ES | |
| Huang et al. [34], 2013 | 192 | Sciatic nerve, 5 mm | Hollow NGC | Delayed ES: after 2, 4, 12, 24 weeks at 3 V, 20 Hz, 1 × 20 min | 4, 12, 24 weeks | NGC-ES | |
| Lee et al. [39], 2010 | 27 | Sciatic nerve, 7 mm; thigh level | Polyimide-based collagen -coated conduit, implanted electrical stimulator | 20 µA, 100 Hz, 100 µs duration, for 4 weeks continuously | 2, 4 weeks | NGC no collagen (I), NGC collagen (II), NGC no collagen + ES (III), NGC collagen + ES (IV) | |
| Li et al. [36], 2020 | 85–90 | Sciatic nerve, 10 mm | CNT/sericin NGC | 3 V, 20 Hz, 0.1 ms, 1 × 1 hour | 8, 12 weeks | 0 mg/mL concentration, 0.5 mg/mL, 0 mg/mL + ES, 0.5 mg/mL − ES, AG | |
| Liao et al. [25], 2020 | 40 | Sciatic nerve, 10 mm * | Silicone rubber NGC | 1 mA, 2/20/200 Hz, 3 times/week for 3 weeks | 4 weeks | Low vs. medium vs. high ES vs. no ES | |
| Lin et al. [26], 2014 (diabetic rats) | 50 | Sciatic nerve, 10 mm | Silicone rubber NGC | 1/10/20 mA, 2 Hz, 100 µs, 15 min, every other day for 3 weeks | 4 weeks | 1 mA vs. 10 mA vs. 20 mA ES (# groups C–E) vs. no ES (B#) vs. non-diabetic NGC without ES (A) | |
| Lin et al. [27], 2015 (diabetic rats) | 50 | Sciatic nerve, 10 mm | Silicone rubber NGC | 1 mA, 2 Hz, 100 µs, 15 min every other day for 2 weeks | - | ES at day 1 (A#) vs. day 8 (B#) vs. day 15 (C#) vs. no ES# (D) vs. non- diabetic no ES (E) | |
| MacEwan et al. [28], 2016 | 40 | Sciatic nerve, 4 mm | Silicone NGC + MSE | - | - | I: control, II: saline, III: GDNF, IV: MSE + saline, V: MSE + GDNF | |
| Song et al. [30], 2016 | 30 | Sciatic nerve, 15 mm; mid-thigh | PPY/PLCL | 0.1 V, 1 hour/day, 4 times, for 1 week period | 3 months | Autograft, same NGC-ES | |
| Sun et al. [31], 2019 | 20 | Sciatic nerve, 15 mm; lower limb | Pt-BC/PPY-N-CNT (self -powered ES) | Up to 0.3 V | 4, 8 weeks | Non-stimulating NGC | |
| Wang et al. [40], 2020 | 55 | Sciatic nerve, 10 mm; hind limb | PCL PLLA-PTMC bilayer conduit with galvanic cells (self-electrified) | - | 4, 8, 12 weeks | Mg group, FeMn group, hollow NGC, autograft | |
| Wu et al. [35], 2020 | 50 | Sciatic nerve, 10 mm; lateral thigh | HSPS conduit | 3 V, 1 hour every other day, 7 times total | 3, 9, 12 weeks | HSPS, HSPS with electrodes but no ES, HSPS + BDNF, AG | |
| Zhang H. et al. [32], 2015 | 24 | Sciatic nerve, 20 mm | L-PRPN | 0.6 V, 50 Hz, 2 × 2 h/day, for 3 days | 3 months | Same NGC-ES, natural regeneration group | |
| Zhang Z. et al. [38], 2014 | 32 | Sciatic nerve, 2 mm ** | Deacetyl chitin conduit | 3 V, 20 Hz, 0.1 ms 1 × 1 hour | 10 months | Same NGC-ES | |
| Zhao et al. [33], 2020 | Sciatic nerve, 10 mm; lateral thigh | PPY/SF | 3 V, 20 Hz, 1 hour, every other day, 7 times total | 6, 12 weeks | PPy-ES, PPY + ES, silicone-ES, silicone + ES, AG | ||
| Authors, Year | CMAP | NCV | SFI | Muscle Recovery (Weight) | Myelin Sheath Thickness | Axon Diameter |
|---|---|---|---|---|---|---|
| Chen et al. [29], 2019 | Higher in m NGC + ES and autograft at 8 weeks * | Higher than NGC-ES at 12 weeks * | - | Higher than NGC-ES at 12 weeks * (musculus gastrocnemius) | Higher than NGC-ES * | Higher than NCG-ES * and AG groups |
| Huang et al. [34], 2013 | Higher in ES groups * | Higher in ES groups * | - | Higher in ES groups * (m. gastrocnemius) | Higher in ES groups * | Higher in ES groups * |
| Lee et al. [39], 2010 | - | - | Higher in group IV at 4 weeks * | - | - | - |
| Li et al. [36], 2020 | Highest in 0.5 + ES, AG, 0.5 − ES at 12 weeks | Highest in 0.5 + ES and AG (at 8 weeks*) | Higher in 0.5 + ES vs. 0−ES * vs 0.5−ES, 0 + ES | Higher in 0.5 + ES vs. all * but AG | Twice as high in 0.5 + ES group vs. all but AG | Higher with 0.5 + ES * and AG * groups at 12 weeks |
| Liao et al. [25], 2020 | MAP: peak amplitude highest with low ES * | No improvement using ES | - | - | - | - |
| Lin et al. [26], 2014 # | - | Higher in groups D * and A * | - | - | - | - |
| Lin et al. [27], 2015 # | MAP area: A and B higher than D * | Higher in groups A–C * and E * | - | - | - | - |
| MacEwan et al. [28], 2016 | - | - | Improved SFI | - | - | - |
| Song et al. [30], 2016 | Higher in NGC + ES and AG at 8 weeks * (DCMAP) | Higher than NGC−ES *; comparable to AG at 4, 8 weeks | Higher in NGC + ES and AG at 4 weeks * | Higher in NGC + ES and AG * (m. triceps) | Higher in NGC + ES and AG at 4 weeks * | Higher in NGC + ES and AG * groups |
| Sun et al. [31], 2019 | - | - | Higher in stimulated group * | - | Higher in stimulated group * | Higher in stimulated group * |
| Wang et al. [40], 2020 | Improved in all groups | - | Higher with ES than other groups after 4 weeks * except AG | Higher in ES and AG * (m. gastrocnemius) | Higher with ES than in FeMn and hollow * group | Higher with ES than all groups * except AG |
| Wu et al. [35], 2020 | Higher in ES than all other groups * except AG | - | Higher in ES than all other groups * except AG (similar) | - | Highest in ES * and AG * group | Highest in ES * and AG * groups |
| Zhang H. et al. [32], 2015 | Best results with ES | Best results with ES | - | - | Best results with ES | - |
| Zhang Z. et al. [38], 2014 | - | Higher with ES at 6 *, 12 weeks | - | - | Higher with ES at 6, 12 weeks | Higher with ES at 6, 12 weeks * |
| Zhao et al. [33], 2020 | - | - | Best results in PPY + ES group after 6 months | - | Best results in PPY + ES and AG group | Best results in PPY + ES and AG groups |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasiba-Pappas, S.; Kamolz, L.-P.; Luze, H.; Nischwitz, S.P.; Holzer-Geissler, J.C.J.; Tuca, A.C.; Rienmüller, T.; Polz, M.; Ziesel, D.; Winter, R. Does Electrical Stimulation through Nerve Conduits Improve Peripheral Nerve Regeneration?—A Systematic Review. J. Pers. Med. 2023, 13, 414. https://doi.org/10.3390/jpm13030414
Hasiba-Pappas S, Kamolz L-P, Luze H, Nischwitz SP, Holzer-Geissler JCJ, Tuca AC, Rienmüller T, Polz M, Ziesel D, Winter R. Does Electrical Stimulation through Nerve Conduits Improve Peripheral Nerve Regeneration?—A Systematic Review. Journal of Personalized Medicine. 2023; 13(3):414. https://doi.org/10.3390/jpm13030414
Chicago/Turabian StyleHasiba-Pappas, Sophie, Lars-P. Kamolz, Hanna Luze, Sebastian P. Nischwitz, Judith C. J. Holzer-Geissler, Alexandru Cristian Tuca, Theresa Rienmüller, Mathias Polz, Daniel Ziesel, and Raimund Winter. 2023. "Does Electrical Stimulation through Nerve Conduits Improve Peripheral Nerve Regeneration?—A Systematic Review" Journal of Personalized Medicine 13, no. 3: 414. https://doi.org/10.3390/jpm13030414
APA StyleHasiba-Pappas, S., Kamolz, L.-P., Luze, H., Nischwitz, S. P., Holzer-Geissler, J. C. J., Tuca, A. C., Rienmüller, T., Polz, M., Ziesel, D., & Winter, R. (2023). Does Electrical Stimulation through Nerve Conduits Improve Peripheral Nerve Regeneration?—A Systematic Review. Journal of Personalized Medicine, 13(3), 414. https://doi.org/10.3390/jpm13030414