
Risk Factors for Recanalization after Coil Embolization


 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Patients
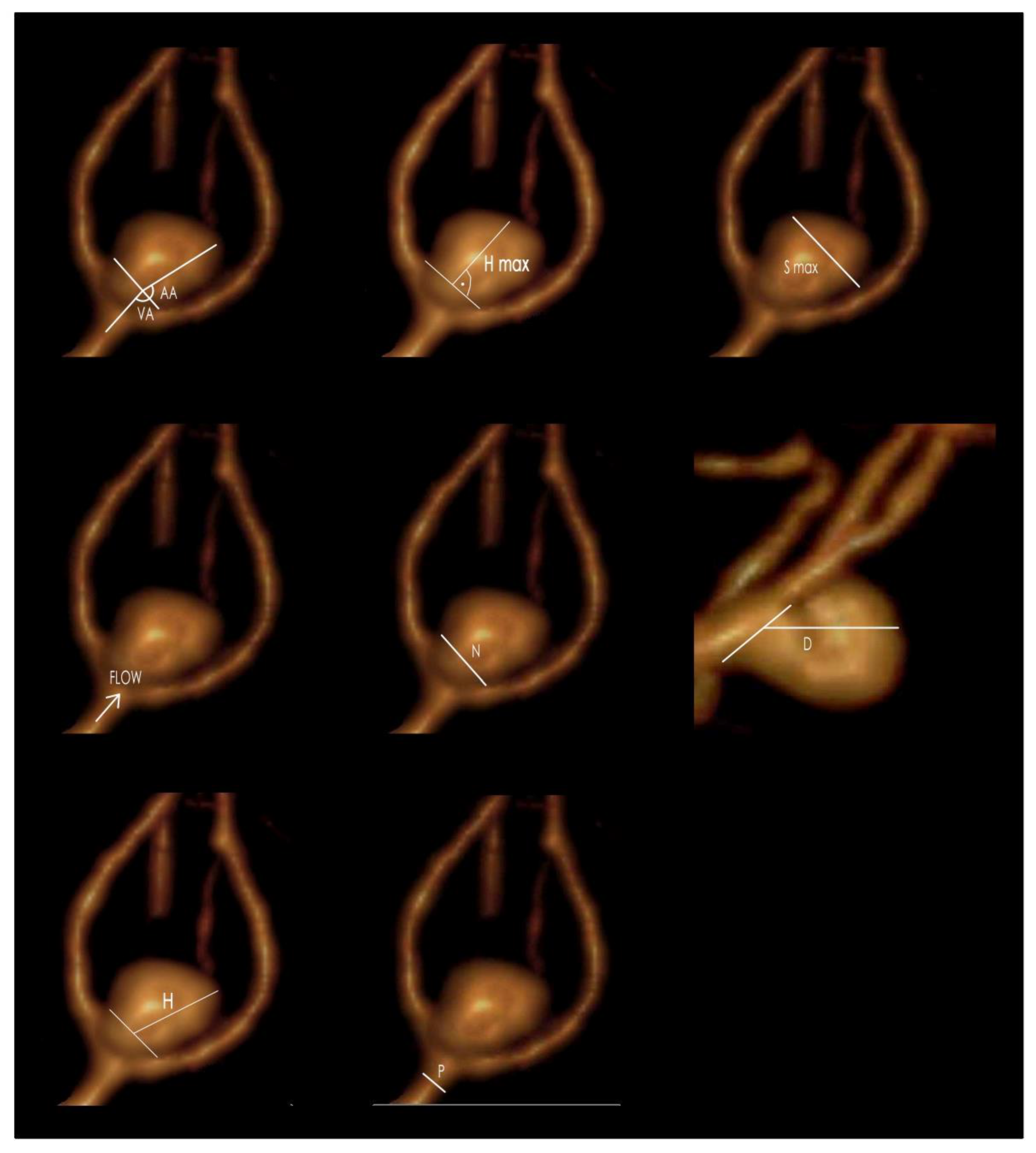
2.3. Morphometric Parameters
- Aneurysm dome size (height, width, depth);
- The maximal perpendicular height;
- Neck size;
- Parent artery size;
- Aneurysm angle;
- Vessel angle;
- Neck to parent artery ratio;
- Aneurysm depth to neck size ratio;
- Aspect ratio (AR), defined as the maximal perpendicular height (the largest perpendicular distance from the neck of the aneurysm to the dome of the aneurysm) divided by neck width;
2.4. Angiography/Embolization
2.4.1. Prevention of Thromboembolic Events
2.4.2. Assessment of Aneurysm Volume, Packing Density, Recanalization and Degree of Aneurysm Filling during the First Embolization
2.5. Statistical Analysis
2.6. Computational Fluid Dynamics Analysis
2.6.1. Model Geometry Preparation
2.6.2. 3D CFD Model Building—Other Possibilities
2.6.3. Numerical Simulations
3. Results
3.1. Patients
3.2. Laboratory Results, Morphometric Parameters, Aneurysm Volume, Packing Density of Intracranial Aneurysms and Complete Aneurysm Filling during the First Embolization
3.3. Type of Embolization Material
3.4. Aneurysm Location
3.5. Recanalization (after 6 and 12 Months)
3.6. Unruptured Aneurysm—Statistical Analysis
3.6.1. Early Recanalization (after 6 Months) in the Unruptured Aneurysm
- Aneurysm width >9.3 mm (AUC (95%CI) 0.76 (0.64–0.87); p < 0.001);
- Aneurysm height >13 mm (AUC (95%CI) 0.76 (0.64–0.87); p < 0.001);
- Aneurysm depth >11 mm (AUC (95%CI) 0.73 (0.60–0.85); p < 0.001);
- Aneurysm neck width >4 mm (AUC (95%CI) 0.82 (0.73–0.90); p < 0.001);
- Diameter of the parent artery >4.6 mm (AUC (95%CI) 0.63 (0.51–0.75); p = 0.029);
- SR ratio >2.759 (AUC (95%CI) 0.72 (0.61–0.84); p < 0.001);
- Index determining the ratio of neck width to diameter of the parent artery >1.042 (AUC (95%CI) 0.66 (0.55–0.76); p = 0.004);
- Largest aneurysm dimension perpendicular to the neck >12.7 (AUC (95%CI) 0.76 (0.65–0.87); p < 0.001);
- Index determining the ratio of the largest aneurysm dimension perpendicular to the neck to the width of the aneurysm neck (aspect ratio) >10.526 (AUC (95%CI) 0.76 (0.64–0.87); p < 0.001);
- AR ratio >10 (AUC (95%CI) 0.72 (0.60–0.84); p < 0.001);
- Packing density <23.5% (AUC (95%CI) 0.86 (0.77–0.95); p < 0.001);
- INR on embolization day >1.01 (AUC (95%CI) 0.62 (0.51–0.73); p = 0.036);
- Prothrombin index on embolization day >99.8 (AUC (95%CI) 0.62 (0.51–0.73); p = 0.036).
3.6.2. Assessment of Recanalization Depending on the Degree of Aneurysm Filling during the First Embolization
3.6.3. Assessment of Recanalization Depending on the Type of Applied Embolization Spirals
3.7. Ruptured Aneurysm—Statistical Analysis
3.7.1. Early Recanalization of Ruptured Aneurysms
- Aneurysm height >12 mm (AUC (95%CI) 0.65 (0.49–0.81); p = 0.063);
- Aneurysm neck width >3.6 mm (AUC (95%CI) 0.83 (0.72–0.95); p < 0.001);
- Packing density <27.5% (AUC (95%CI) 0.88 (0.79–0.98); p < 0.001);
- Index determining the ratio of neck width to diameter of the parent artery >1.023 (AUC (95%CI) 0.67 (0.52–0.82); p = 0.025);
- Largest aneurysm dimension perpendicular to the neck >12 mm (AUC (95%CI) 0.77 (0.62–0.92); p < 0.001);
- Index determining the ratio of the largest dimension of the aneurysm perpendicular to the neck to the width of the aneurysm neck (aspect ratio) >3.075 (AUC (95%CI) 0.68 (0.51–0.85); p = 0.039).
3.7.2. Assessment of Recanalization Depending on Aneurysm Filling during the First Embolization
3.7.3. Assessment of Recanalization Depending on Coil Types
3.8. Multifactorial Analysis for Ruptured and Unruptured Aneurysms
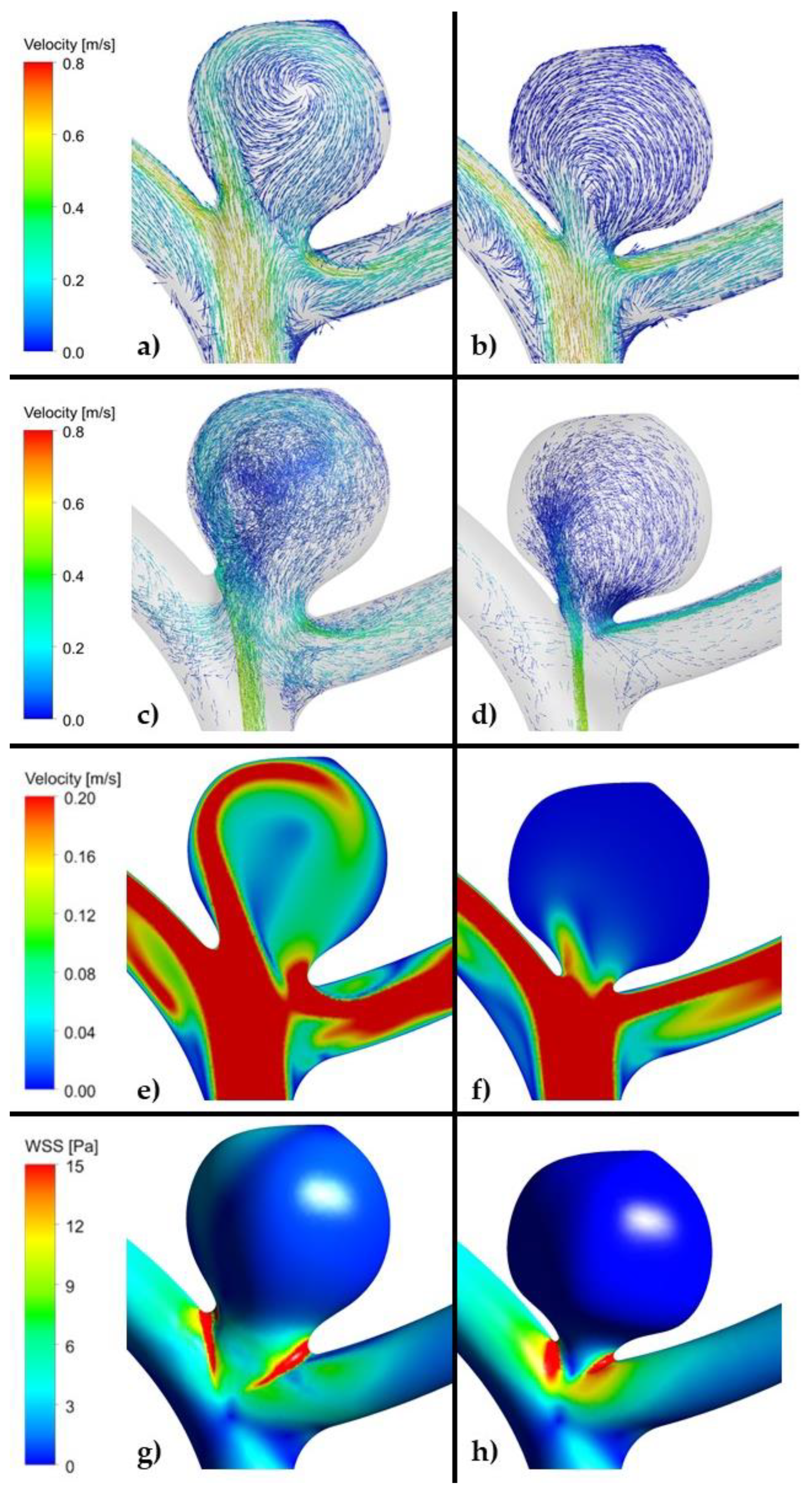
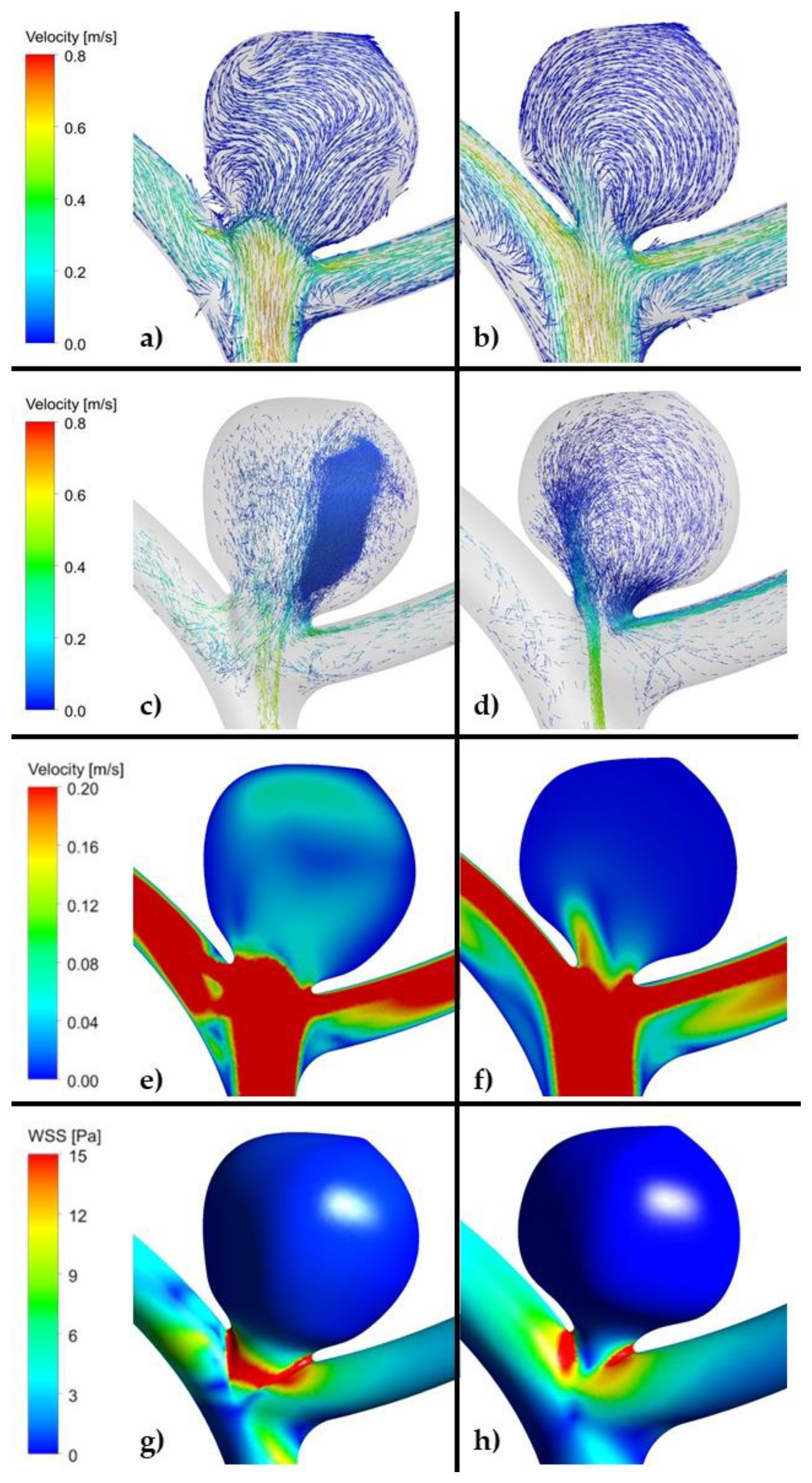
3.9. Computational Fluid Dynamics Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vlak, M.H.; Algra, A.; Brandenburg, R.; Rinkel, G.J. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011, 10, 626–636. [Google Scholar] [CrossRef]
- Steiner, T.; Juvela, S.; Unterberg, A.; Jung, C.; Frostin, M.; Rinkel, G.; European Stroke Organisation. European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage. Cerebrovasc. Dis. 2013, 35, 93–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molyneux, A.; Kerr, R.; Stratton, I.; Sandercock, P.; Clarke, M.; Shrimpton, J.; Holman, R.; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet 2002, 360, 1267–1274. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.C.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P.; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar]
- Yeon, E.K.; Cho, Y.D.; Yoo, D.H.; Lee, S.H.; Kang, H.-S.; Kim, J.E.; Cho, W.-S.; Choi, H.H.; Han, M.H. Is 3 years adequate for tracking completely occluded coiled aneurysms? J. Neurosurg. 2019, 133, 1–7. [Google Scholar] [CrossRef]
- Pandey, A.S.; Koebbe, C.; Rosenwasser, R.H.; Veznedaroglu, E. Endovascular coil embolization of ruptured and unruptured posterior circulation aneurysms: Review of a 10-year experience. Neurosurgery 2007, 60, 626–636, discussion 636–637. [Google Scholar] [CrossRef]
- Pierot, L.; Spelle, L.; Vitry, F.; ATENA Investigators. Immediate clinical outcome of patients harboring unruptured intracranial aneurysms treated by endovascular approach: Results of the ATENA study. Stroke 2008, 39, 2497–2504. [Google Scholar] [CrossRef]
- Ma, X.; Yang, Y.; Zhou, Y.; Jia, W. Endovascular treatment of ruptured intracranial aneurysms in elderly patients: Clinical features and treatment outcome. Neurosurg. Rev. 2019, 42, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Grunwald, I.Q.; Papanagiotou, P.; Struffert, T.; Politi, M.; Krick, C.; Gül, G.; Reith, W. Recanalization after endovascular treatment of intracerebral aneurysms. Neuroradiology 2007, 49, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Raymond, J.; Guilbert, F.; Weill, A.; Georganos, A.; Juravsky, L.; Lambert, A.; Lamoureux, J.; Chagnon, M.; Roy, D. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 2003, 34, 1398–1403. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, K.; Kitagawa, N.; Morikawa, M.; Horie, N.; Kawakubo, J.; Hiu, T.; Tsutsumi, K.; Nagata, I. Long-term follow-up of endovascular coil embolization for cerebral aneurysms using three-dimensional time-of-flight magnetic resonance angiography. Neurol. Res. 2009, 31, 674–680. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.P.; Cho, Y.D.; Yoo, D.H.; Moon, J.; Lee, J.; Cho, W.S.; Kang, H.S.; Kim, J.E.; Han, M.H. Risk Factor Analysis of Recanalization Timing in Coiled Aneurysms: Early versus Late Recanalization. AJNR Am. J. Neuroradiol. 2017, 38, 1765–1770. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.P.; Cho, Y.D.; Rhim, J.K.; Yoo, D.H.; Kang, H.S.; Kim, J.E.; Cho, W.S.; Han, M.H. Extended monitoring of coiled aneurysms completely occluded at 6-month follow-up: Late recanalization rate and related risk factors. Eur. Radiol. 2016, 26, 3319–3326. [Google Scholar] [CrossRef] [PubMed]
- Murayama, Y.; Nien, Y.L.; Duckwiler, G.; Gobin, Y.P.; Jahan, R.; Frazee, J.; Martin, N.; Viñuela, F. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J. Neurosurg. 2003, 98, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Cognard, C.; Weill, A.; Spelle, L.; Piotin, M.; Castaings, L.; Rey, A.; Moret, J. Long-term angiographic follow-up of 169 intracranial berry aneurysms occluded with detachable coils. Radiology 1999, 212, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Ogilvy, C.S.; Chua, M.H.; Fusco, M.R.; Griessenauer, C.J.; Harrigan, M.R.; Sonig, A.; Siddiqui, A.H.; Levy, E.I.; Snyder, K.; Avery, M.; et al. Validation of a System to Predict Recanalization After Endovascular Treatment of Intracranial Aneurysms. Neurosurgery 2015, 77, 168–173. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.C.; Birks, J.; Ramzi, N.; Yarnold, J.; Sneade, M.; Rischmiller, J.; ISAT Collaborators. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the (ISAT): Long-term follow-up. Lancet Neurol. 2009, 8, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Johnston, S.C.; Dowd, C.F.; Higashida, R.T.; Lawton, M.T.; Duckwiler, G.R.; Gress, D.R.; CARAT Investigators. Predictors of rehemorrhage after treatment of ruptured intracranial aneurysms: The Cerebral Aneurysm Rerupture after Treatment (CARAT) study. Stroke 2008, 39, 120–125. [Google Scholar] [CrossRef]
- Sluzewski, M.; van Rooij, W.J.; Beute, G.N.; Nijssen, P.C. Late rebleeding of ruptured intracranial aneurysms treated with detachable coils. AJNR Am. J. Neuroradiol. 2005, 26, 2542–2549. [Google Scholar]
- Slob, M.J.; Sluzewski, M.; van Rooij, W.J.; Roks, G.; Rinkel, G.J. Additional coiling of previously coiled cerebral aneurysms: Clinical and angiographic results. AJNR Am. J. Neuroradiol. 2004, 25, 1373–1376. [Google Scholar] [PubMed]
- Wei, Y.; Cotin, S.; Fang, L.; Allard, J.; Pan, C.; Ma, S. Toward real-time simulation of blood-coil interaction during aneurysm embolization. Med. Image Comput. Comput. Assist. Interv. 2009, 12, 198–205. [Google Scholar]
- Wiśniewski, K.; Tomasik, B.; Bobeff, E.J.; Stefańczyk, L.; Hupało, M.; Jaskólski, D.J. Predictors for ophthalmic segment aneurysms recanalization after coiling and flow diverter embolization in 6- and 12-month follow-up. J. Clin. Neurosci. 2019, 68, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Chalouhi, N.; Dumont, A.S.; Hasan, D.; Tjoumakaris, S.; Gonzalez, L.F.; Starke, R.M.; Dalyai, R.; El Moursi, S.; Rosenwasser, R.; Jabbour, P. Is packing density important in stent-assisted coiling? Neurosurgery 2012, 71, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Colby, G.P.; Paul, A.R.; Radvany, M.G.; Gandhi, D.; Gailloud, P.; Huang, J.; Tamargo, R.J.; Coon, A.L. A single center comparison of coiling versus stent assisted coiling in 90 consecutive paraophthalmic region aneurysms. J. Neurointerv. Surg. 2012, 4, 116–120. [Google Scholar] [CrossRef] [Green Version]
- CAPRIES Teering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996, 348, 1329. [Google Scholar] [CrossRef]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K.; Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar]
- Hwang, G.; Jung, C.; Park, S.Q.; Kang, H.S.; Lee, S.H.; Oh, C.W.; Chung, Y.S.; Han, M.H.; Kwon, O.K. Thromboembolic complications of elective coil embolization of unruptured aneurysms: The effect of oral antiplatelet preparation on periprocedural thromboembolic complication. Neurosurgery 2010, 67, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Kim, K.; Jeon, P.; Kim, S.; Kim, H.; Byun, H.; Cha, J.; Hong, S.; Jo, K. Thromboembolic complications in patients with clopidogrel resistance after coil embolization for unruptured intracranial aneurysms. AJNR Am. J. Neuroradiol. 2014, 35, 1786–1792. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.S.; Kwon, B.J.; Kim, J.E.; Han, M.H. Preinterventional clopidogrel response variability for coil embolization of intracranial aneurysms: Clinical implications. AJNR Am. J. Neuroradiol. 2010, 31, 1206–1210. [Google Scholar] [CrossRef] [Green Version]
- Serebruany, V.L.; Steinhubl, S.R.; Berger, P.B.; Malinin, A.I.; Bhatt, D.L.; Topol, E.J. Variability in platelet responsiveness to clopidogrel among 544 individuals. J. Am. Coll. Cardiol. 2005, 45, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado Almandoz, J.E.; Kadkhodayan, Y.; Crandall, B.M.; Scholz, J.M.; Fease, J.L.; Tubman, D.E. Variability in initial response to standard clopidogrel therapy, delayed conversion to clopidogrel hyper-response, and associated thromboembolic and hemorrhagic complications in patients undergoing endovascular treatment of unruptured cerebral aneurysms. J. Neurointerv. Surg. 2014, 6, 767–773. [Google Scholar] [CrossRef]
- Kim, M.S.; Jo, K.I.; Yeon, J.Y.; Kim, J.S.; Kim, K.H.; Jeon, P.; Hong, S.C. Association between postprocedural infarction and antiplatelet drug resistance after coiling for unruptured intracranial aneurysms. AJNR Am. J. Neuroradiol. 2016, 37, 1099–1105. [Google Scholar] [CrossRef] [Green Version]
- Hwang, G.; Huh, W.; Lee, J.S.; Villavicencio, J.B.; Villamor, R.B.V., Jr.; Ahn, S.Y.; Kim, J.; Chang, J.Y.; Park, S.J.; Park, N.M.; et al. Standard vs Modified Antiplatelet Preparation for Preventing Thromboembolic Events in Patients With High On-Treatment Platelet Reactivity Undergoing Coil Embolization for an Unruptured Intracranial Aneurysm: A Randomized Clinical Trial. JAMA Neurol. 2015, 72, 764–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, N.J.; Jones, W.H.; Sanzgiri, A.; Corona, J.; Dannenbaum, M.; Chen, P.R. Antiplatelet therapy for the prevention of pericoiling thromboembolism in high-risk patients with ruptured intracranial aneurysms. J. Neurosurg. 2017, 127, 1326–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihn, Y.K.; Shin, S.H.; Baik, S.K.; Choi, I.S. Complications of endovascular treatment for intracranial aneurysms: Management and prevention. Interv. Neuroradiol. 2018, 24, 237–245. [Google Scholar] [CrossRef]
- Aviv, R.I.; O’Neill, R.; Patel, M.C.; Colquhoun, I.R. Abciximab in patients with ruptured intracranial aneurysms. AJNR Am. J. Neuroradiol. 2005, 26, 1744–1750. [Google Scholar]
- Bruening, R.; Mueller-Schunk, S.; Morhard, D.; Seelos, K.C.; Brueckmann, H.; Schmid-Elsaesser, R.; Straube, A.; Mayer, T.E. Intraprocedural thrombus formation during coil placement in ruptured intracranial aneurysms: Treatment with systemic application of the glycoprotein IIb/IIIa antagonist tirofiban. AJNR Am. J. Neuroradiol. 2006, 27, 1326–1331. [Google Scholar]
- Park, J.H.; Kim, J.E.; Sheen, S.H.; Jung, C.K.; Kwon, B.J.; Kwon, O.K.; Oh, C.W.; Han, M.H.; Han, D.H. Intra-arterial abciximab for the treatment of thromboembolism during coil embolization of intracranial aneurysm: Outcome and fatal hemorrhagic complications. J. Neurosurg. 2008, 108, 450–457. [Google Scholar] [CrossRef]
- Yi, H.J.; Gupta, R.; Jovin, T.G.; Tayal, A.; Genevro, J.; Gologorsky, Y.; Horowitz, M. Initial experience with the use of intravenous eptifibatide bolus during endovascular treatment of intracranial aneurysms. AJNR Am. J. Neuroradiol. 2006, 27, 1856–1860. [Google Scholar]
- Rechavia, E.; Wurzel, M. Platelet glycoprotein IIb/IIIa receptor blockade in acute myocardial infarction associated with thrombotic occlusion of the left main coronary artery. Circulation 1998, 22, 1249–1250. [Google Scholar] [CrossRef] [PubMed]
- Peerlinck, K.; De Lepeleire, I.; Goldberg, M.; Farrell, D.; Barrett, J.; Hand, E.; Panebianco, D.; Deckmyn, H.; Vermylen, J.; Arnout, J. MK-383 (L-700,462), a selective nonpeptide platelet glycoprotein IIb/IIIa antagonist, is active in man. Circulation 1993, 88, 1512–1527. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.S.; Kwon, B.J.; Roh, H.G.; Yoon, S.W.; Chang, H.W.; Kim, J.E.; Han, M.H. Intra-arterial tirofiban infusion for thromboembolism during endovascular treatment of intracranial aneurysms. Neurosurgery 2008, 63, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.F.; Spencer, F.A.; Becker, R.C. Comparative efficacy of fibrinogen and platelet supplementation on the in vitro reversibility of competitive glycoprotein IIb/IIIa receptor-directed platelet inhibition. Am. Heart J. 2002, 143, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Mascelli, M.A.; Lance, E.T.; Damaraju, L.; Wagner, C.L.; Weisman, H.F.; Jordan, R.E. Pharmacodynamic profile of short-term abciximab treatment demonstrates prolonged platelet inhibition with gradual recovery from GPIIb-IIIa receptor blockade. Circulation 1998, 97, 1680–1688. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Liu, K.C. Management strategies for intraprocedural coil migration during endovascular treatment of intracranial aneurysms. J. Neurointerv. Surg. 2014, 6, 428–431. [Google Scholar] [CrossRef]
- Ding, D.; Liu, K.C. Microsurgical extraction of a malfunctioned pipeline embolization device following complete deployment. J. Cerebrovasc. Endovasc. Neurosurg. 2013, 15, 241–245. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.P.; Cho, Y.D.; Rhim, J.K.; Yoo, D.H.; Cho, W.-S.; Kang, H.-S.; Kim, J.E.; Han, M.H. Fate of coiled aneurysms with minor recanalization at 6 months: Rate of progression to further recanalization and related risk factors. AJNR Am. J. Neuroradiol. 2016, 37, 1490–1495. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Zhang, Y.; Wang, A.; Zhang, Y.; Li, Y.; Yang, X. Haemodynamic analysis for recanalisation of intracranial aneurysms after endovascular treatment: An observational registry study in China. BMJ Open 2017, 7, 014261. [Google Scholar] [CrossRef] [Green Version]
- Brillstra, E.H.; Rinkel, G.J.E.; van der Graaf, Y.; van Rooij, W.J.J.; Algra, A. Treatment of intracranial aneurysms by embolization with coils: A systematic review. Stroke 1999, 30, 470–476. [Google Scholar] [CrossRef]
- Hayakawa, M.; Murayama, Y.; Duckwiler, G.R.; Gobin, Y.P.; Guglielmi, G.; Viñuela, F. Natural history of the neck remnant of a cerebral aneurysm treated with the Guglielmi detachable coil system. J. Neurosurg. 2000, 93, 561–568. [Google Scholar] [CrossRef] [Green Version]
- Benitez, R.P.; Silva, M.T.; Klem, J.; Veznedaroglu, E.; Rosenwasser, R.H. Endovascular occlusion of wide-necked aneurysms with a new intracranial microstent (Neuroform) and detachable coils. Neurosurgery 2004, 54, 1359–1367. [Google Scholar] [CrossRef]
- Kole, M.K.; Pelz, D.M.; Kalapos, P.; Lee, D.H.; Gulka, I.B.; Lownie, S.P. Endovascular coil embolization of intracranial aneurysms: Important factors related to rates and outcomes of incomplete occlusion. J. Neurosurg. 2005, 102, 607–615. [Google Scholar] [CrossRef]
- UCAS Japan Investigators. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N. Engl. J. Med. 2012, 366, 2474–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.A.; Nichols, D.A.; Meyer, F.B.; Pichelmann, M.A.; McIver, J.I.; Toussaint, L.G., 3rd; Axley, P.L.; Brown, R.D., Jr. Guglielmi detachable coil treatment of ruptured saccular cerebral aneurysms: Retrospective review of a 10-year single-center experience. AJNR Am. J. Neuroradiol. 2003, 24, 526–533. [Google Scholar]
- Grunwald, I.Q.; Balami, J.S.; Weber, D.; Mutter, J.; Kühn, A.L.; Krick, C.; Peith, W.; Papanagiotou, P.; Shariat, K. Different factors influence recanalisation rate after coiling in ruptured and unruptured intracranial aneurysms. CNS Neurol. Disord. Drug Targets 2013, 12, 228. [Google Scholar] [CrossRef]
- Sluzewski, M.; van Rooji, W.J.; Slob, M.J.; Bescós, J.O.; Slump, C.H.; Wijnalda, D. Relation between Aneurysm Volume, Packing, and Compaction in 145 Cerebral Aneurysms Treated with Coils. Radiology 2004, 231, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.H.; Lee, S.H.; Yeon, E.K.; Yoo, D.H.; Cho, Y.D.; Cho, W.S.; Kim, J.E.; Son, Y.J.; Han, M.H.; Kang, H.S. Determination of Aneurysm Volume Critical for Stability after Coil Embolization: A Retrospective Study of 3530 Aneurysms. World Neurosurg. 2019, 132, e766–e774. [Google Scholar] [CrossRef] [PubMed]
- Pierot, L.; Cognard, C.; Anxionnat, R.; Ricolfi, F.; CLARITY Invsetigators. Ruptured intracranial aneurysms: Factors affecting the rate and outcome of endovascular treatment complications in a series of 782 patients (CLARITY study). Radiology 2010, 256, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, R.; Stefanski, M.; Rosenwasser, R.; Veznedaroglu, E. Cigarette smoking as a risk factor for recurrence of aneurysms treated by endosaccular occlusion. J. Neurosurg. 2008, 108, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hope, J.K.; Byrne, J.V.; Molyneux, A.J. Factors influencing successful angiographic occlusion of aneurysms treated by coil embolization. AJNR Am. J. Neuroradiol. 1999, 20, 391–399. [Google Scholar]
- Plowman, R.S.; Clarke, A.; Clarke, M.; Byrne, J.V. Sixteen-year single-surgeon experience with coil embolization for ruptured intracranial aneurysms: Recurrence rates and incidence of late rebleeding: Clinical article. J. Neurosurg. 2011, 114, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Ferns, S.P.; Sprengers, M.E.; van Rooij, W.J.; van Zwam, W.H.; de Kort, G.A.P.; Velthuis, B.K.; Schaafsma, J.D.; van den Berg, R.; Sluzewski, M.; Brouwer, P.A.; et al. Late reopening of adequately coiled intracranial aneurysms: Frequency and risk factors in 400 patients with 440 aneurysms. Stroke 2011, 42, 1331–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ries, T.; Siemonsen, S.; Thomalla, G.; Grzyska, U.; Zeumer, H.; Fiehler, J. Long-term follow-up of cerebral aneurysms after endovascular therapy prediction and outcome of retreatment. AJNR Am. J. Neuroradiol. 2007, 28, 1755–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.S.; Kim, M.C.; Lee, S.K.; Willinsky, R.A.; Terbrugge, K.G. Clinical and angiographic long-term follow-up of completely coiled intracranial aneurysms using endovascular technique. J. Neurosurg. 2010, 112, 575–581. [Google Scholar] [CrossRef]
- Piotin, M.; Spelle, L.; Mounayer, C.; Sallez-Rezende, M.T.; Giansante-Abud, D.; Vanzin-Santos, R.; Moret, J. Intracranial aneurysms: Treatment with bare platinum coils: Aneurysm packing, complex coils, and angiographic recurrence. Radiology 2007, 243, 500–508. [Google Scholar] [CrossRef]
- Lam, A.K.N.; Ko, M.W.L.; Leung, L.K.K.; Kwok, J.C.K.; Yuen, M.M.F.; Lam, D.C.C. Characterization of pressure reduction in coil-filled aneurysm under flow of human blood with and without anti-coagulant. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2013, 2013, 739–742. [Google Scholar]
- Cebral, J.R.; Castro, M.A.; Burgess, J.E.; Pergolizzi, R.S.; Sheridan, M.J.; Putman, C.M. Characterization of cerebral aneurysms for assessing risk of rupture by using patient-specific computational hemodynamics models. AJNR Am. J. Neuroradiol. 2005, 26, 2550–2559. [Google Scholar]
- Cebral, J.R.; Mut, F.; Weir, J.; Putman, C.M. Association of hemodynamic characteristics and cerebral aneurysm rupture. AJNR Am. J. Neuroradiol. 2011, 32, 264–270. [Google Scholar] [CrossRef]
- Park, W.; Song, Y.; Park, K.J.; Koo, H.W.; Yang, K.; Suh, D.C. Hemodynamic characteristics regarding recanalization of completely coiled aneurysms: Computational fluid dynamic analysis using virtual models comparison. Neurointervention 2016, 11, 30–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Tian, Z.; Liu, J.; Jing, L.; Paliwal, N.; Wang, S.; Zhang, Y.; Xiang, J.; Siddiqui, A.H.; Meng, H.; et al. Flow diverter effect of LVIS stent on cerebral aneurysm hemodynamics: A comparison with Enterprise stents and the Pipeline device. J. Transl. Med. 2016, 14, 199. [Google Scholar] [CrossRef] [Green Version]
- Jiang, P.; Liu, Q.; Wu, J.; Chen, X.; Li, M.; Yang, F.; Li, Z.; Yang, S.; Guo, R.; Gao, B.; et al. Hemodynamic findings associated with intraoperative appearances of intracranial aneurysms. Neurosurg. Rev. 2020, 43, 203–209. [Google Scholar] [CrossRef]
- Li, C.; Wang, S.; Chen, J.; Yu, H.; Zhang, y.; Jiang, F.; Mu, S.; Li, H.; Yang, X. Influence of hemodynamics on recanalization of totally occluded intracranial aneurysms: A patient-specific computational fluid dynamic simulation study. J. Neurosurg. 2012, 117, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Irie, K.; Anzai, H.; Kojima, M.; Honjo, N.; Ohta, M.; Hirose, Y.; Negoro, M. Computational fluid dynamic analysis following recurrence of cerebral aneurysm after coil embolization. Asian J. Neurosurg. 2012, 7, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinjikji, W.; Chung, B.J.; Jimenez, C.; Putman, C.; Kallmes, D.F.; Cerbal, J.R. Hemodynamic differences between unstable and stable unruptured aneurysms independent of size and location: A pilot study. J. Neurointerv. Surg. 2017, 9, 376–380. [Google Scholar] [CrossRef]
- Zhang, Q.; Jing, L.; Liu, J.; Wang, K.; Zhang, Y.; Paliwal, N.; Meng, H.; Wang, Y.; Wang, S.; Yang, X. Predisposing factors for recanalization of cerebral aneurysms after endovascular embolization: A multivariate study. J. Neurointerv. Surg. 2018, 10, 252–257. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, S.; Shimogonya, Y.; Yonemoto, N.; CFD ABO Study Group. Differences in Cerebral Aneurysm Rupture Rate According to Arterial Anatomies Depend on the Hemodynamic Environment. AJNR Am. J. Neuroradiol. 2019, 40, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Horowitz, M.; Jungreis, C.; Genevro, J.; Koebbe, C.; Levy, E.; Kassam, A. Periprocedural morbidity and mortality associated with endovascular treatment of intracranial aneurysms. AJNR Am. J. Neuroradiol. 2005, 26, 506–514. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
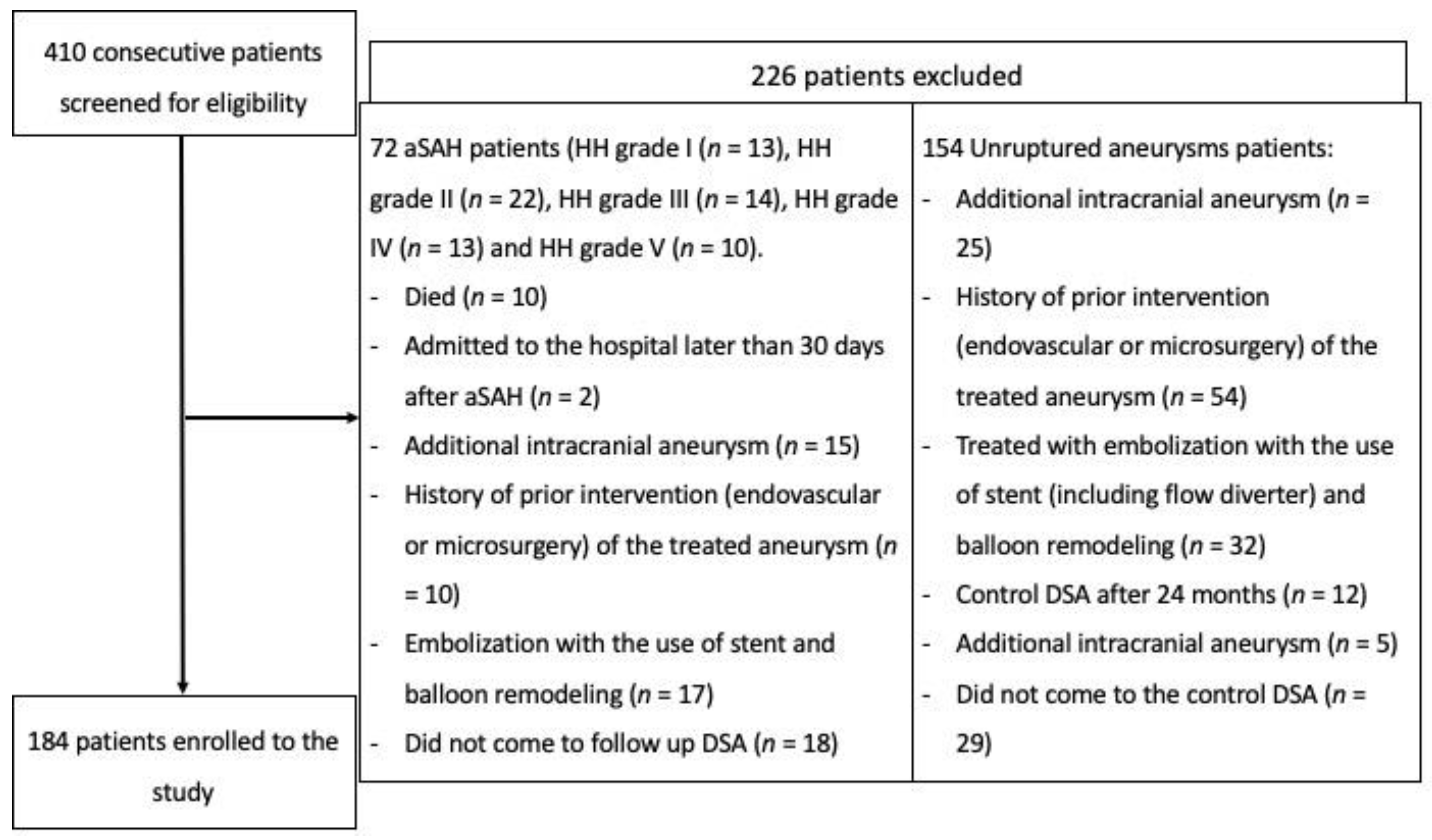
| Study Group | |
|---|---|
| Inclusion criteria | Single saccular aneurysm treated with classical embolization without the use of stent and balloon remodeling. Full medical documentation of the hospitalization period and the follow-up visits with DSA done, 6 months after the treatment. |
| Exclusion criteria | Admission to hospital later than 30 days after aSAH. History of prior intervention (endovascular or microsurgical) of the treated aneurysm. |
| Unruptured Aneurysm Group | |||
| Value | Mean ± SD without Recanalization | Mean ± SD with Recanalization | p |
| age (years) | 54.1 ± 11.6 | 56.5 ± 14.0 | 0.350 |
| depth (mm) | 6.7 ± 3.6 | 12.0 ± 6.6 | <0.001 * |
| height (mm) | 8.2 ± 4.7 | 13.8 ± 6.6 | <0.001 * |
| width (mm) | 6.6 ± 3.8 | 12.1 ± 6.8 | <0.001 * |
| neck size (mm) | 3.6 ± 1.0 | 5.0 ± 2.3 | <0.001 * |
| APTT (s) | 29.4 ± 6.2 | 29.1 ± 3.4 | 0.806 |
| INR | 1.0 ± 0.1 | 1.0 ± 0.1 | 0.849 |
| HCT (%) | 38.4 ± 9.3 | 38.9 ± 7.9 | 0.764 |
| prothrombin time (s) | 101.3 ± 6.7 | 98.2 ± 6.5 | 0.022 |
| aneurysm volume (mm3) | 426.7 ± 1287.4 | 1794.1 ± 2202.0 | <0.001 * |
| packing density | 33.3 ± 8.0% | 20.0 ± 8.9% | <0.001 * |
| parent artery diameter (mm) | 3.8 ± 0.9 | 4.3 ± 1.1 | 0.012 |
| maximum aneurysm height/parent artery diameter—SR ratio | 2.3 ± 1.3 | 3.4 ± 1.6 | <0.001 * |
| neck size/parent artery diameter | 1.0 ± 0.3 | 1.2 ± 0.5 | 0.004 |
| the maximal perpendicular height (mm) | 7.7 ± 4.3 | 12.9 ± 6.0 | <0.001 * |
| the maximal perpendicular height/neck size (aspect ratio) | 7.8 ± 4.6 | 12.7 ± 6.0 | <0.001 * |
| vessel angle (degree) | 60.7 ± 24.1 | 60.4 ± 22 | 0.943 |
| aneurysm angle (degree) | 85.1 ± 19.5 | 82.0 ± 20.8 | 0.455 |
| aneurysm depth/neck size (AR ratio) | 7.9 ± 1.0 | 11.8 ± 6.3 | 0.039 |
| Complete aneurysm filling during the first embolization (p < 0.001 *) | |||
| Modified Raymond-Roy Scale Class | (N) | ||
| I | 107 | ||
| II | 7 | ||
| IIIa | 2 | ||
| IIIb | 2 | ||
| Ruptured Aneurysm Group | |||
| Value | Mean ± SD without recanalization | Mean ± SD with recanalization | p |
| age (years) | 56.7 ± 15.3 | 56.9 ± 16.1 | 0.974 |
| depth (mm) | 5.5 ± 2.7 | 6.4 ± 3.3 | 0.229 |
| height (mm) | 6.9 ± 3.2 | 9.5 ± 5.2 | 0.016 |
| width (mm) | 5.4 ± 2.6 | 6.6 ± 3.3 | 0.111 |
| neck size (mm) | 3.3 ± 0.8 | 4.1 ± 0.7 | 0.001 * |
| APTT (s) | 30.1 ± 5.5 | 29.0 ± 2.7 | 0.473 |
| INR | 1.1 ± 0.3 | 1.1 ± 0.1 | 0.916 |
| HCT (%) | 35.5 ± 11.4 | 36.5 ± 10.1 | 0.759 |
| prothrombin time (s) | 1392.4 ± 6314.5 | 95.2 ± 8.3 | 0.389 |
| aneurysm volume (mm3) | 166.5 ± 274.3 | 349.1 ± 432.4 | 0.045 |
| packing density | 35.0 ± 10.8%, | 21.2 ± 6.6% | 0.001 * |
| parent artery diameter (mm) | 3.7 ± 0.9 | 3.9 ± 1.1 | 0.525 |
| maximum aneurysm height/parent artery diameter—SR ratio | 2.0 ± 1.1 | 2.5 ± 1.3 | 0.147 |
| neck size/parent artery diameter | 0.9 ± 0.3 | 1.2 ± 0.5 | 0.015 |
| the maximal perpendicular height (mm) | 6.9 ± 3.4 | 12.0 ± 5.1 | 0.001 * |
| the maximal perpendicular height/neck size (aspect ratio) | 2.1 ± 0.9 | 3.0 ± 1.6 | 0.006 |
| vessel angle (degree) | 62.5 ± 26.0 | 62.0 ± 22.2 | 0.934 |
| aneurysm angle (degree) | 85.3 ± 22.7 | 90.8 ± 26.9 | 0.402 |
| aneurysm depth/neck size (AR ratio) | 1.7 ± 0.8 | 1.6 ± 0.9 | 0.590 |
| Complete aneurysm filling during the first embolization (p < 0.001 *) | |||
| Modified Raymond-Roy Scale Class | (N) | ||
| I | 52 | ||
| II | 11 | ||
| IIIa | 1 | ||
| IIIb | 2 | ||
| Ruptured Aneurysms (n = 66); Anterior Part of the Circle of Willis (n = 42, 63.6%), Posterior Part (n = 24, 36.4%) | Unruptured Aneurysms (n = 118); Anterior Part of the Circle of Willis (n = 84, 71.2%), Posterior Part (n = 34, 28.8%) |
|---|---|
| ACoA (n = 13, 19.7%) | ACoA (n = 6, 5.1%) |
| MCA n = 15, 22.7% (M2 n = 14), (M1 n = 1) | MCA n = 6, 5.1% (M2 n = 3), (M1 n = 3) |
ICA (n = 12, 18.2%):
| ICA (n = 69, 58.5%):
|
| PCallA (n = 2, 3.0%) | PCallA (n = 3, 2.5%) |
| BA (n = 17, 25.8%); above (n = 7), at (n = 5) and below the level of the posterior clinoid (n = 5). | BA (n = 21, 17.8%); above (n = 9), at (n = 8) and below the level of the posterior clinoid (n = 4). |
| PICA (n = 2, 3.0%) | PICA (n = 2, 1.7%) |
| PCA (n = 1, 1.5%) | AICA (n = 2, 1.7%) |
| SCA (n = 1, 1.5%) | SCA (n = 4, 3.4%) |
| VA (n = 3, 4.5%); 2 aneurysms arising from proximal carina of fenestration at VB junction (in 1 case it involved both limbs) and 1 originating along the entire limb. | VA (n = 5, 4.2%); 3 aneurysms arising from proximal carina of fenestration at VB junction (in 2 cases it involved both limbs) and 2 originating along the entire limb. |
| Recanalization after 6 Months | Odds Ratio (95%CI) | p Value |
|---|---|---|
| aSAH group | ||
| the degree of aneurysm filling | 17.00 (2.32–124.40) | 0.005 |
| during the first embolization | ||
| packing density | 0.87 (0.79–0.97) | 0.01 |
| Unruptured group | ||
| packing density | 0.84 (0.79–0.91) | <0.001 |
| neck size (mm) | 2.16 (1.23–3.80) | 0.008 |
| Recanalization after 12 months | Odds Ratio (95%CI) | p value |
| aSAH group | ||
| the degree of aneurysm filling | 6.88 (0.98–48.29) | 0.052 |
| during the first embolization | ||
| packing density | 0.85 (0.77–0.94) | 0.002 |
| Unruptured group | ||
| packing density | 0.84 (0.78–0.91) | <0.001 |
| neck size (mm) | 5.46 (2.52–11.83) | <0.001 |
| Reference | Case1 | Case2 | Case3 | Case4 | Case5 | Case6 | Case7 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | |||
| Unruptured aneurysms group | max WSS (Pa) | 97.927 | 93.084 | 97.481 | 90.476 | 96.204 | 85.593 | 93.084 | 79.645 | 93.084 | 90.776 | 95.748 | 92.150 | 93.084 | 90.411 | 95.748 |
| areaAve WSS (Pa) | 2.538 | 2.423 | 3.071 | 1.306 | 2.024 | 3.731 | 2.423 | 2.846 | 2.423 | 1.001 | 1.373 | 2.316 | 2.423 | 1.154 | 1.373 | |
| areaAve OSI (–) | 0.160 | 0.211 | 0.200 | 0.210 | 0.201 | 0.163 | 0.211 | 0.237 | 0.211 | 0.198 | 0.198 | 0.156 | 0.211 | 0.195 | 0.198 | |
| max TAWSS (Pa) | 43.779 | 41.708 | 43.070 | 40.477 | 42.689 | 31.265 | 41.708 | 37.525 | 41.708 | 39.932 | 42.196 | 36.392 | 41.708 | 40.287 | 42.196 | |
| areaAve TAWSS (Pa) | 1.242 | 1.021 | 1.305 | 0.570 | 0.880 | 1.646 | 1.021 | 1.246 | 1.021 | 0.432 | 0.591 | 0.977 | 1.021 | 0.491 | 0.591 | |
| Ruptured aneurysms group | max WSS (Pa) | 123.535 | 95.748 | 102.925 | 101.551 | 132.148 | 93.084 | 102.925 | 92.150 | 93.084 | - | - | - | - | - | - |
| areaAve WSS (Pa) | 1.659 | 1.373 | 2.774 | 2.692 | 2.597 | 2.423 | 2.774 | 2.316 | 2.423 | - | - | - | - | - | - | |
| areaAve OSI (–) | 0.207 | 0.198 | 0.231 | 0.157 | 0.209 | 0.211 | 0.231 | 0.156 | 0.211 | - | - | - | - | - | - | |
| max TAWSS (Pa) | 54.162 | 42.196 | 46.33 | 45.18 | 53.879 | 41.708 | 46.33 | 36.392 | 41.708 | - | - | - | - | - | - | |
| areaAve TAWSS (Pa) | 0.746 | 0.591 | 1.179 | 1.223 | 1.047 | 1.021 | 1.179 | 0.977 | 1.021 | - | - | - | - | - | - | |
| Values That Increase Recanalization Risk, Based on ROC Curve Analysis | Case | Blood Velocity at Aneurysm Neck (m/s); Measurements Taken at Systole Peak | |||
|---|---|---|---|---|---|
| Reference | High Risk of Recanalization | Low Risk of Recanalization | |||
| Unruptured group | S > 9.3 mm | #1 | 0.167 | 0.104 (−38%) | 0.103 (−38%) |
| H > 13 mm | #2 | 0.110 (−34%) | 0.107 (−36%) | ||
| N > 4 mm | #3 | 0.156 (−7%) | 0.104 (−38%) | ||
| P > 4.6 mm | #4 | 0.124 (−26%) | 0.104 (−38%) | ||
| SR ratio (H/N ratio) > 2.759 | #5 | 0.104 (−38%) | 0.105 (−37%) | ||
| N/P ratio > 1.042 | #6 | 0.163 (−2%) | 0.104 (−38%) | ||
| aspect ratio (H/N ratio) > 10.526 | #7 | 0.116 (−31%) | 0.105 (−37%) | ||
| Ruptured group | H > 12 mm | #1 | 0.119 | 0.105 (−12%) | 0.106 (−11%) |
| N > 3.6 mm | #2 | 0.137 (−15%) | 0.095 (−20%) | ||
| aspect ratio (H/N ratio) > 3.075 | #3 | 0.104 (−13%) | 0.106 (−11%) | ||
| N/P ratio > 1.023 | #4 | 0.163 (37%) | 0.104 (−13%) | ||
| Major Studies of Intracranial Aneurysms. Number of Patients Included, Aneurysm Status (Ruptured or Unruptured) and Recanalization Risk Factors | |||||
|---|---|---|---|---|---|
| Risk Factors | |||||
| Study | Patients | IA Status | Patient Factors | Aneurysm Factors | Treatment Factors |
| CLARITY trial [60] | n = 782 | ruptured | age < 65 y.o. | neck size ≥ 4 mm | - |
| Ortiz et al. [61] | n = 110 | ruptured/unruptured | cigarette smoking | - | - |
| Raymond et al. [10] | n = 446 | ruptured/unruptured | - | ruptured status/aneurysms greater than 10 mm/neck size ≥ 4 mm | incomplete occlusion immediately after procedure |
| Hope et al. [62] | n = 58 | ruptured/unruptured | - | ruptured status/neck size ≥ 4 mm | incomplete occlusion immediately after procedure |
| Plowman et al. [63] | n = 570 | ruptured | - | ruptured status | - |
| Ferns et al. [64] | n = 400 | ruptured/unruptured | - | location at basilar tip | - |
| Ries et al. [65] | n = 323 | ruptured/unruptured | - | aneurysms greater than 10 mm/neck size ≥ 4 mm | - |
| Choi et al. [66] | n = 87 | ruptured/unruptured | - | neck size ≥ 4 mm | - |
| Piotin et al. [67] | n = 223 | ruptured/un ruptured | - | - | incomplete occlusion immediately after procedure |
| Grunwald et al. [9] | n = 211 | ruptured/unruptured | - | - | incomplete occlusion immediately after procedure |
| Sluzewski et al. [58] | n = 198 | ruptured/unruptured | - | - | packing density less than 24% |
| Liu et al. [50] | n = 200 | ruptured/unruptured | - | ruptured status/neck size ≥ 4 mm/those aneurysms with atherosclerotic plaques | - |
| Jeon et al. [48] | n= 898 | ruptured/unruptured | - | - | Stent deployment significantly decreased recanalization rate |
| ISAT study [17] | n = 2143 | ruptured | the patient’s young age | aneurysms greater than 10 mm | incomplete occlusion immediately after procedure |
| Brillstra et al. [51] | n = 1383 | ruptured/unruptured | - | neck size ≥ 4 mm | - |
| Hayakawa et al. [52] | n = 71 | ruptured/unruptured | - | aneurysms greater than 10 mm | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiśniewski, K.; Tyfa, Z.; Tomasik, B.; Reorowicz, P.; Bobeff, E.J.; Posmyk, B.J.; Hupało, M.; Stefańczyk, L.; Jóźwik, K.; Jaskólski, D.J. Risk Factors for Recanalization after Coil Embolization. J. Pers. Med. 2021, 11, 793. https://doi.org/10.3390/jpm11080793
Wiśniewski K, Tyfa Z, Tomasik B, Reorowicz P, Bobeff EJ, Posmyk BJ, Hupało M, Stefańczyk L, Jóźwik K, Jaskólski DJ. Risk Factors for Recanalization after Coil Embolization. Journal of Personalized Medicine. 2021; 11(8):793. https://doi.org/10.3390/jpm11080793
Chicago/Turabian StyleWiśniewski, Karol, Zbigniew Tyfa, Bartłomiej Tomasik, Piotr Reorowicz, Ernest J. Bobeff, Bartłomiej J. Posmyk, Marlena Hupało, Ludomir Stefańczyk, Krzysztof Jóźwik, and Dariusz J. Jaskólski. 2021. "Risk Factors for Recanalization after Coil Embolization" Journal of Personalized Medicine 11, no. 8: 793. https://doi.org/10.3390/jpm11080793
APA StyleWiśniewski, K., Tyfa, Z., Tomasik, B., Reorowicz, P., Bobeff, E. J., Posmyk, B. J., Hupało, M., Stefańczyk, L., Jóźwik, K., & Jaskólski, D. J. (2021). Risk Factors for Recanalization after Coil Embolization. Journal of Personalized Medicine, 11(8), 793. https://doi.org/10.3390/jpm11080793