Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MR Imaging Techniques
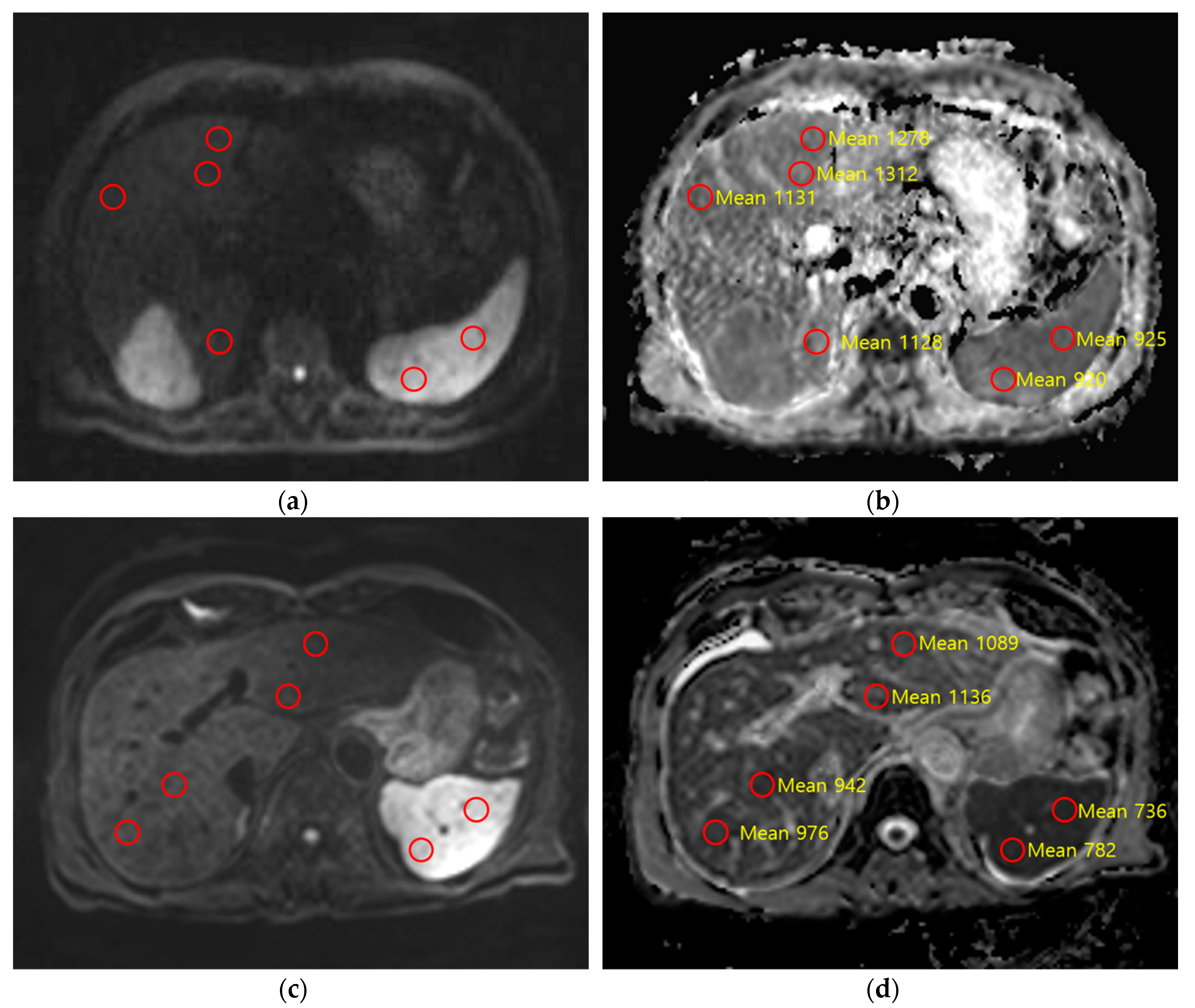
2.3. Quantitative Image Analysis
2.4. Histopathologic Evaluation
2.5. Statistical Analysis
3. Results
3.1. DWI Acquisition Methods
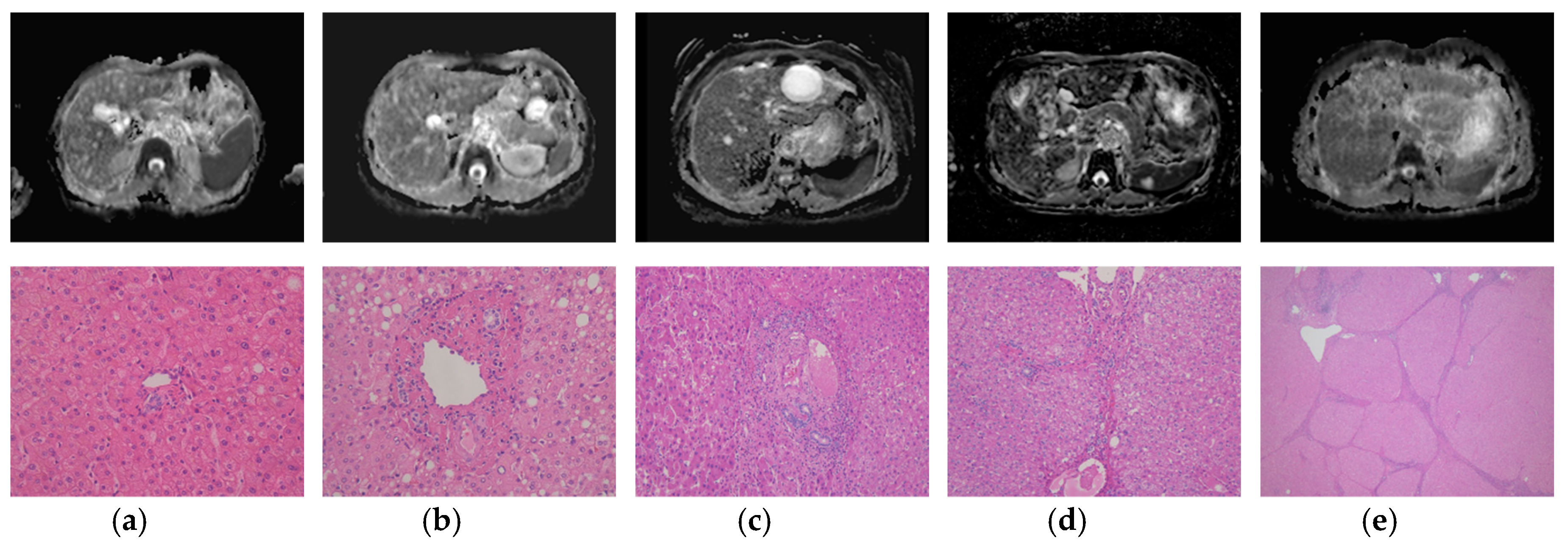
3.2. Histopathologic Results
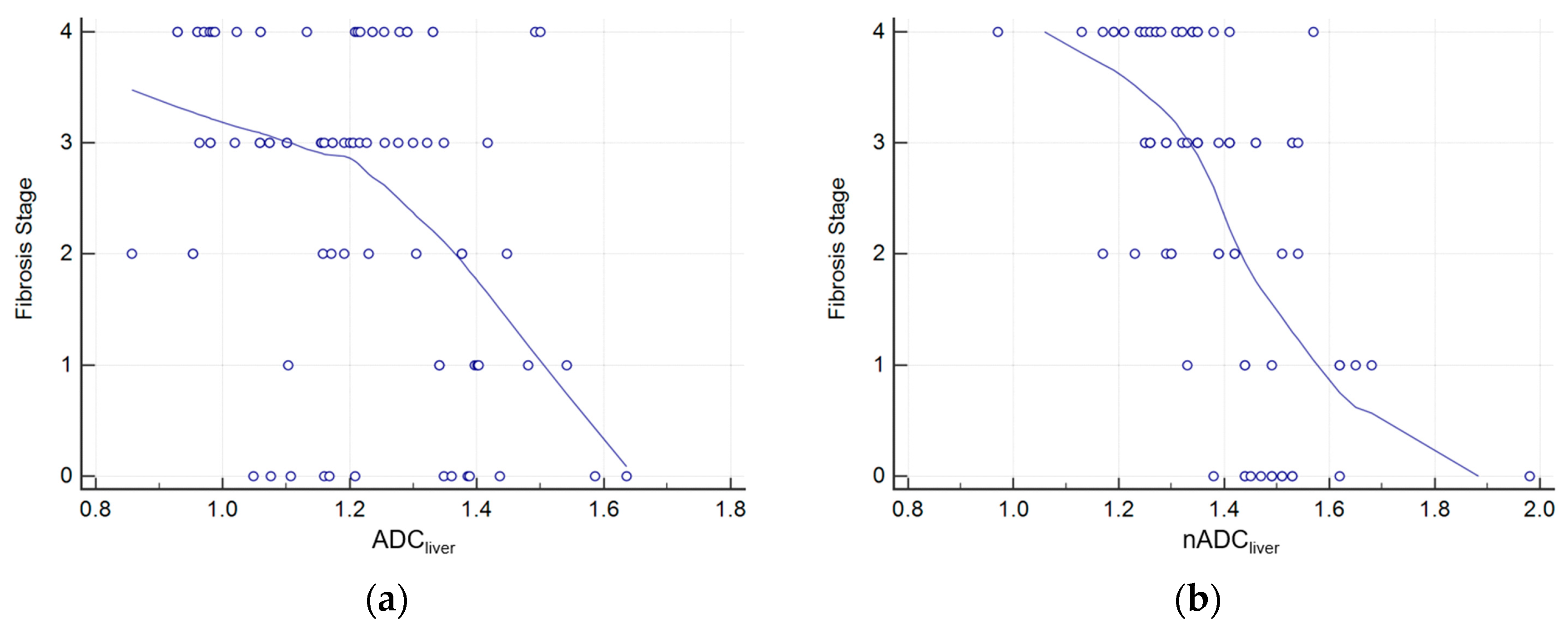
3.3. Correlations Between Fibrosis Stage, TE Value, Liver ADC and Normalized Liver ADC
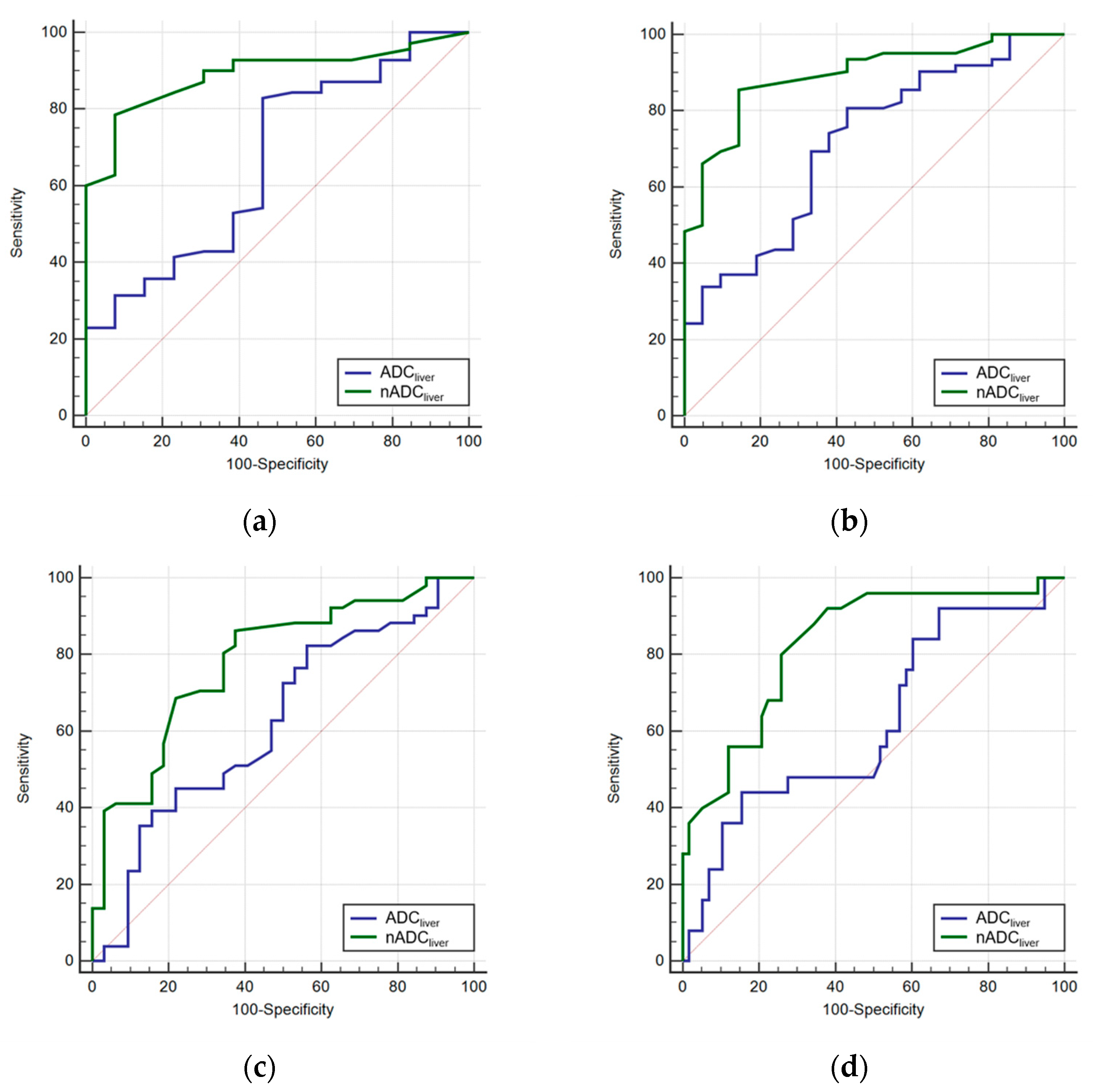
3.4. Diagnostic Performance and Cut-off Value Evaluation
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Watanabe, H.; Kanematsu, M.; Goshima, S.; Kondo, H.; Onozuka, M.; Moriyama, N.; Bae, K.T. Staging hepatic fibrosis: Comparison of gadoxetate disodium–enhanced and diffusion-weighted MR imaging—Preliminary observations. Radiology 2011, 259, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Z.D. Grading and staging systems for inflammation and fibrosis in chronic liver diseases. J. Hepatol. 2007, 47, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Taouli, B.; Chouli, M.; Martin, A.J.; Qayyum, A.; Coakley, F.V.; Vilgrain, V. Chronic hepatitis: Role of diffusion-weighted imaging and diffusion tensor imaging for the diagnosis of liver fibrosis and inflammation. J. Magn. Reson. Imaging 2008, 28, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, M.; Rusinek, H.; Lee, V.S.; Losada, M.; Bannan, M.A.; Krinsky, G.A.; Taouli, B. Advanced liver fibrosis: Diagnosis with 3D whole-liver perfusion MR imaging—Initial experience. Radiology 2008, 246, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Taksali, S.E.; Dufour, S.; Befroy, D.; Goodman, T.R.; Petersen, K.F.; Shulman, G.I.; Caprio, S.; Constable, R.T. Comparative MR study of hepatic fat quantification using single-voxel proton spectroscopy, two-point dixon and three-point IDEAL. Magn. Reson. Med. 2008, 59, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Foucher, J.; Chanteloup, E.; Vergniol, J.; Castera, L.; Le Bail, B.; Adhoute, X.; Bertet, J.; Couzigou, P.; de Ledinghen, V. Diagnosis of cirrhosis by transient elastography (FibroScan): A prospective study. Gut 2006, 55, 403–408. [Google Scholar] [CrossRef]
- Jia, J.; Hou, J.; Ding, H.; Chen, G.; Xie, Q.; Wang, Y.; Zeng, M.; Zhao, J.; Wang, T.; Hu, X.; et al. Transient elastography compared to serum markers to predict liver fibrosis in a cohort of Chinese patients with chronic hepatitis B. J. Gastroenterol. Hepatol. 2015, 30, 756–762. [Google Scholar] [CrossRef]
- Foucher, J.; Castera, L.; Bernard, P.H.; Adhoute, X.; Laharie, D.; Bertet, J.; Couzigou, P.; de Ledinghen, V. Prevalence and factors associated with failure of liver stiffness measurement using FibroScan in a prospective study of 2114 examinations. Eur. J. Gastroenterol. Hepatol. 2006, 18, 411–412. [Google Scholar] [CrossRef]
- Bonekamp, D.; Bonekamp, S.; Ou, H.Y.; Torbenson, M.S.; Corona-Villalobos, C.P.; Mezey, E.; Kamel, I.R. Assessing liver fibrosis: Comparison of arterial enhancement fraction and diffusion-weighted imaging. J. Magn. Reson. Imaging 2014, 40, 1137–1146. [Google Scholar] [CrossRef]
- Tosun, M.; Inan, N.; Sarisoy, H.T.; Akansel, G.; Gumustas, S.; Gurbuz, Y.; Demirci, A. Diagnostic performance of conventional diffusion weighted imaging and diffusion tensor imaging for the liver fibrosis and inflammation. Eur. J. Radiol. 2013, 82, 203–207. [Google Scholar] [CrossRef]
- Bulow, R.; Mensel, B.; Meffert, P.; Hernando, D.; Evert, M.; Kuhn, J.P. Diffusion-weighted magnetic resonance imaging for staging liver fibrosis is less reliable in the presence of fat and iron. Eur. Radiol. 2013, 23, 1281–1287. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Oei, M.; Babb, J.S.; Niver, B.E.; Taouli, B. Diffusion-weighted imaging of the abdomen at 3.0 Tesla: Image quality and apparent diffusion coefficient reproducibility compared with 1.5 Tesla. J. Magn. Reson. Imaging 2011, 33, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.L.; Sigmund, E.E.; Chandarana, H.; Rusinek, H.; Chen, Q.; Vivier, P.H.; Taouli, B.; Lee, V.S. Variability of renal apparent diffusion coefficients: Limitations of the monoexponential model for diffusion quantification. Radiology 2010, 254, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; Kwak, H.S.; Byon, J.H.; Jin, G.Y. Diffusion-weighted MR imaging of upper abdominal organs at different time points: Apparent diffusion coefficient normalization using a reference organ. J. Magn. Reson. Imaging 2017, 45, 1494–1501. [Google Scholar] [CrossRef] [PubMed]
- Do, R.K.; Chandarana, H.; Felker, E.; Hajdu, C.H.; Babb, J.S.; Kim, D.; Taouli, B. Diagnosis of liver fibrosis and cirrhosis with diffusion-weighted imaging: Value of normalized apparent diffusion coefficient using the spleen as reference organ. Am. J. Roentgenol. 2010, 195, 671–676. [Google Scholar] [CrossRef]
- Castera, L. Noninvasive Assessment of Liver Fibrosis. Dig. Dis. 2015, 33, 498–503. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Wang, Y.; Ganger, D.R.; Levitsky, J.; Sternick, L.A.; McCarthy, R.J.; Chen, Z.E.; Fasanati, C.W.; Bolster, B.; Shah, S.; Zuehlsdorff, S.; et al. Assessment of chronic hepatitis and fibrosis: Comparison of MR elastography and diffusion-weighted imaging. Am. J. Roentgenol. 2011, 196, 553–561. [Google Scholar] [CrossRef]
- Braithwaite, A.C.; Dale, B.M.; Boll, D.T.; Merkle, E.M. Short- and midterm reproducibility of apparent diffusion coefficient measurements at 3.0-T diffusion-weighted imaging of the abdomen. Radiology 2009, 250, 459–465. [Google Scholar] [CrossRef]
- Corona-Villalobos, C.P.; Pan, L.; Halappa, V.G.; Bonekamp, S.; Lorenz, C.H.; Eng, J.; Kamel, I.R. Agreement and reproducibility of apparent diffusion coefficient measurements of dual-b-value and multi-b-value diffusion-weighted magnetic resonance imaging at 1.5 Tesla in phantom and in soft tissues of the abdomen. J. Comput. Assist. Tomogr. 2013, 37, 46–51. [Google Scholar] [CrossRef]
- Ghany, M.G.; Strader, D.B.; Thomas, D.L.; Seeff, L.B. American Association for the Study of Liver, D. Diagnosis, management, and treatment of hepatitis C: An update. Hepatology 2009, 49, 1335–1374. [Google Scholar] [CrossRef] [PubMed]
- Taouli, B.; Tolia, A.J.; Losada, M.; Babb, J.S.; Chan, E.S.; Bannan, M.A.; Tobias, H. Diffusion-weighted MRI for quantification of liver fibrosis: Preliminary experience. Am. J. Roentgenol. 2007, 189, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Friedrich-Rust, M.; Poynard, T.; Castera, L. Critical comparison of elastography methods to assess chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Colagrande, S.; Mazzoni, L.N.; Mazzoni, E.; Pradella, S. Effects of gadoxetic acid on quantitative diffusion-weighted imaging of the liver. J. Magn. Reson. Imaging 2013, 38, 365–370. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Verio | Achieva | Skyra | ||
|---|---|---|---|---|---|
| Sequence | SE-EPI | SE-EPI | SE-EPI | SE-EPI | SE-EPI |
| Respiration | FB | NT | FB | NT | FB |
| TR/TE (msec) | 11500/67 | 2800/65 | 8750/66 | 1422/56 | 5100/66 |
| FOV (mm) | 400 × 400 | 380 × 285 | 400 × 400 | 350 × 350 | 370 × 278 |
| Matrix | 128 × 128 | 128 × 96 | 128 × 128 | 128 × 124 | 128 × 96 |
| ST (mm) | 5 | 6 | 5 | 6 | 5 |
| Intersection gap (mm) | 1 | 1.2 | 1 | 1 | 1 |
| No. of sections | 33 | 29 | 35 | 35 | 34 |
| NSA | 3 | 2 | 3 | 3 | 4 |
| b values (s/mm2) | b1, b3 | b1, b3 | b1, b2 | b1 | b1 |
| BW (Hz) | 2442 | 2298 | 3743 | 3634 | 2442 |
| PAF | GRAPPA = 2 | GRAPPA = 2 | SENSE = 2 | SENSE = 2 | GRAPPA = 2 |
| Fat saturation | SPAIR1 | SPAIR1 | SPAIR2 | SPAIR2 | SPAIR1 |
| Scan time | 5:50 | 5:15 | 5:35 | 4:00 | 3:50 |
| EPI factor | 96 | 96 | 65 | 65 | 96 |
| b Value | Verio | Achieva | Skyra | No. of Examinations | |||
|---|---|---|---|---|---|---|---|
| FB | NT | FB | NT | FB | NT | ||
| b1 | 26 | 2 | 12 | 3 | 18 | 61 (73.5%) | |
| b2 | 4 | 4 (4.8%) | |||||
| b3 | 3 | 15 | 18 (21.7%) | ||||
| 46 (55.4%) | 19 (22.9%) | 18 (21.7%) | 83 (100%) | ||||
| NT = 20 (24.1%), FB = 63 (75.9%) | |||||||
| Variable | Liver ADC | nADCliver | p Value |
|---|---|---|---|
| F1 (n = 8) | |||
| Optimal cut-off value | 1.347 (×10−3 mm2/s) | 1.443 | |
| Sensitivity (%) | 83.1 (71.2, 91.7) | 78.2 (64.7, 89.1) | |
| Specificity (%) | 57.2 (24.3, 85.3) | 91.0 (67.6, 99.2) | |
| AUC (95% CI) | 0.625 (0.501, 0.727) | 0.863 (0.755, 0.952) | 0.064 |
| F2 (n = 11) | |||
| Optimal cut-off value | 1.332 (×10−3 mm2/s) | 1.411 | |
| Sensitivity (%) | 83.4 (71.8, 90.6) | 84.3 (71.1, 91.9) | |
| Specificity (%) | 58.5 (30.7, 79.9) | 86.9 (61.2, 98.1) | |
| AUC (95% CI) | 0.631 (0.529, 0.759) | 0.877 (0.772, 0.948) | 0.031 |
| F3 (n = 26) | |||
| Optimal cut-off value | 1.330 (×10−3 mm2/s) | 1.396 | |
| Sensitivity (%) | 85.4 (71.2, 92.1) | 84.5 (69.8, 92.1) | |
| Specificity (%) | 44.2 (23.6, 65.1) | 69.2 (46.9, 85.8) | |
| AUC (95% CI) | 0.587 (0.461, 0.694) | 0.764 (0.645, 0.859) | 0.114 |
| F4 (n = 25) | |||
| Optimal cut-off value | 1.189 (×10−3 mm2/s) | 1.365 | |
| Sensitivity (%) | 43.4 (22.1, 65.7) | 90.2 (68.2, 98.9) | |
| Specificity (%) | 83.1 (68.5, 90.8) | 62.3 (46.6, 75.8) | |
| AUC (95% CI) | 0.577 (0.443, 0.689) | 0.789 (0.671, 0.882) | 0.041 |
| Variable | TE | nADCliver | p Value |
|---|---|---|---|
| F1 (n = 8) | |||
| Optimal cut-off value | 5.9 (kPa) | 1.443 | |
| Sensitivity (%) | 94.1 (84.7, 98.8) | 78.2 (64.7, 89.1) | |
| Specificity (%) | 58.2 (26.2, 88.2) | 91.0 (67.6, 99.2) | |
| AUC (95% CI) | 0.799 (0.683, 0.888) | 0.863 (0.755, 0.952) | 0.612 |
| F2 (n = 11) | |||
| Optimal cut-off value | 6.9 (kPa) | 1.411 | |
| Sensitivity (%) | 88.2 (75.8, 95.3) | 84.3 (71.1, 91.9) | |
| Specificity (%) | 68.8 (41.5, 89.2) | 86.9 (61.2, 98.1) | |
| AUC (95% CI) | 0.811 (0.718, 0.882) | 0.877 (0.772, 0.948) | 0.892 |
| F3 (n = 26) | |||
| Optimal cut-off value | 9.0 (kPa) | 1.396 | |
| Sensitivity (%) | 65.1 (49.0, 77.9) | 84.5 (69.8, 92.1) | |
| Specificity (%) | 71.2 (50.2, 87.1) | 69.2 (46.9, 85.8) | |
| AUC (95% CI) | 0.721 (0.597, 0.802) | 0.764 (0.645, 0.859) | 0.877 |
| F4 (n = 25) | |||
| Optimal cut-off value | 9.7 (kPa) | 1.365 | |
| Sensitivity (%) | 100 (83.2, 100) | 90.2 (68.2, 98.9) | |
| Specificity (%) | 69.6 (54.2, 82.3) | 62.3 (46.6, 75.8) | |
| AUC (95% CI) | 0.884 (0.787, 0.943) | 0.789 (0.671, 0.882) | 0.064 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, M.K.; Song, J.S.; Hwang, S.B.; Hwang, H.P.; Kim, Y.J.; Moon, W.S. Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ. Diagnostics 2019, 9, 107. https://doi.org/10.3390/diagnostics9030107
Shin MK, Song JS, Hwang SB, Hwang HP, Kim YJ, Moon WS. Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ. Diagnostics. 2019; 9(3):107. https://doi.org/10.3390/diagnostics9030107
Chicago/Turabian StyleShin, Min Ki, Ji Soo Song, Seung Bae Hwang, Hong Pil Hwang, Young Jun Kim, and Woo Sung Moon. 2019. "Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ" Diagnostics 9, no. 3: 107. https://doi.org/10.3390/diagnostics9030107
APA StyleShin, M. K., Song, J. S., Hwang, S. B., Hwang, H. P., Kim, Y. J., & Moon, W. S. (2019). Liver Fibrosis Assessment with Diffusion-Weighted Imaging: Value of Liver Apparent Diffusion Coefficient Normalization Using the Spleen as a Reference Organ. Diagnostics, 9(3), 107. https://doi.org/10.3390/diagnostics9030107