
Reliability and Validity of the Linear Transducer “ADR Encoder” for Measuring Power and Speed of the Sit-to-Stand Tests in Older Adults

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
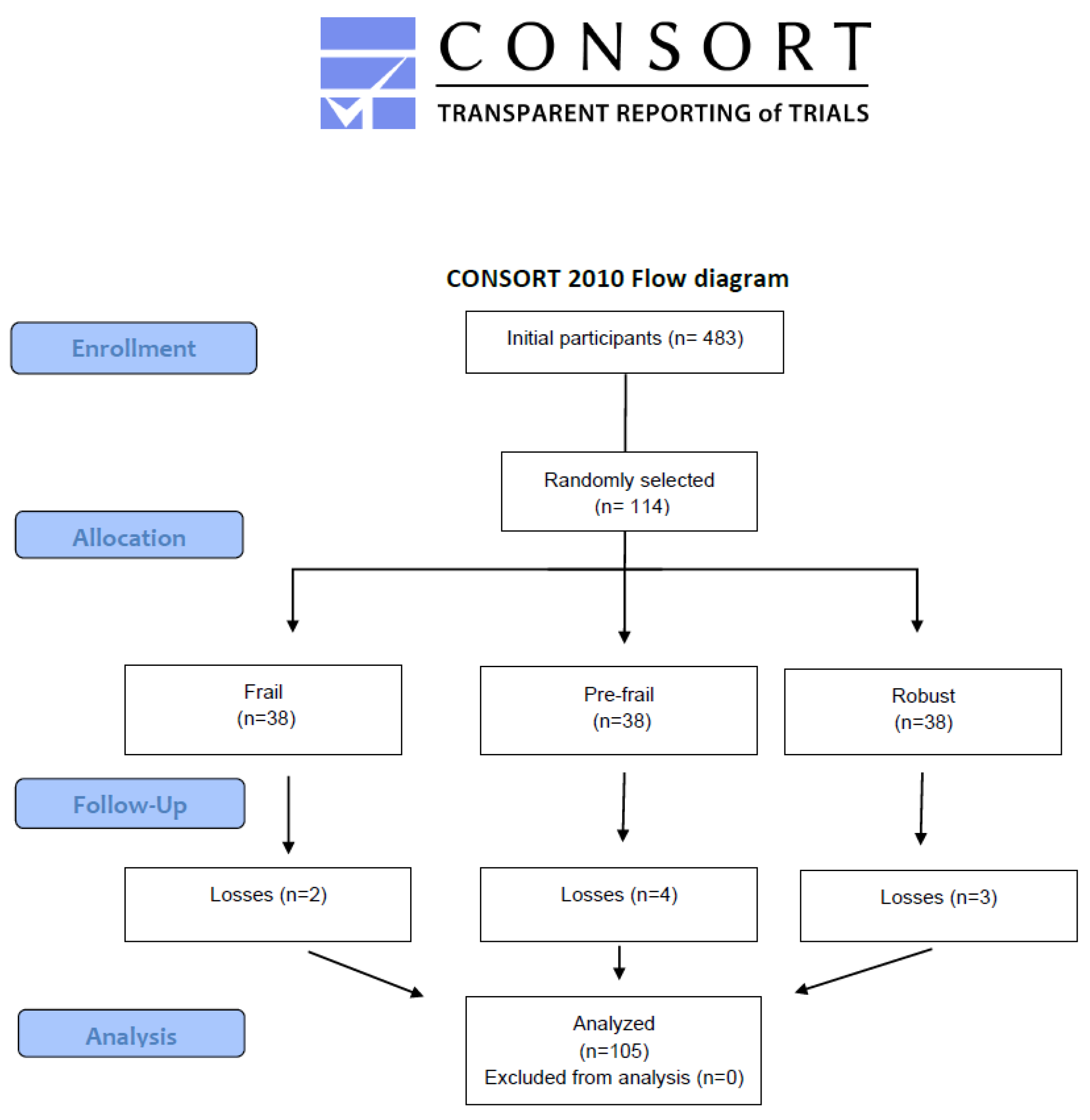
2.1. Study Design and Participants
2.2. Sample Size
2.3. Assessment and Outcomes
2.3.1. The 30-s Chair Stand Test (30CS)
2.3.2. Five Times Sit-to-Stand Test (5STS)
2.3.3. Power and Speed Measurement with the Linear Transducer
2.4. Statistical Analysis
3. Results
3.1. Baseline Results
3.2. Correlations of Speed and Power with Functional Performance in the 5STS and 30CS
3.3. Reliability of Speed and Power Measurements in 5STS and 30CS: Inter- and Intraobserver Consistency
3.4. Regression Coefficients of Speed and Power
3.5. Comparative Analysis of Frail and Non-Frail Older Adults
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 5STS | Five Times Sit-to-Stand Test |
| 30CS | 30-s Chair Stand Test |
| BMI | Body Mass Index |
| CI | Confidence Interval |
| ICC | Intraclass Correlation Coefficient |
| IQR | Interquartile Range |
| STS | Sit-to-Stand Test |
References
- Mitchell, E.; Walker, R. Global ageing: Successes, challenges and opportunities. Br. J. Hosp. Med. 2020, 81, 1–9. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Acosta-Benito, M.Á.; Martín-Lesende, I. Fragilidad en atención primaria: Diagnóstico y manejo multidisciplinar. Aten. Primaria 2022, 54, 102395. [Google Scholar] [CrossRef]
- Uysal, I.; Cetisli-Korkmaz, N.; Cavlak, U. Assessment of the musculoskeletal performance with squat tests and performance-oriented measurements in older adults. J. Back Musculoskelet. Rehabil. 2020, 33, 735–741. [Google Scholar] [CrossRef]
- Goldberg, A.; Chavis, M.; Watkins, J.; Wilson, T. The five-times-sit-to-stand test: Validity, reliability and detectable change in older females. Aging Clin. Exp. Res. 2012, 24, 339–344. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- El Hadouchi, M.; Kiers, H.; De Vries, R.; Veenhof, C.; Van Dieën, J. Effectiveness of power training compared to strength training in older adults: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2022, 19, 18. [Google Scholar] [CrossRef]
- Skelton, D.A.; Greig, C.A.; Davies, J.M.; Young, A. Strength, power and related functional ability of healthy people aged 65-89 years. Age Ageing 1994, 23, 371–377. [Google Scholar] [CrossRef]
- Lopez-Torres, O.; Fernandez-Elias, V.E.; Li, J.; Gomez-Ruano, M.A.; Guadalupe-Grau, A. Validity and Reliability of A New Low-Cost Linear Position Transducer to Measure Mean Propulsive Velocity: The ADR device. Proc. Inst. Mech. Eng. P J. Sports Eng. Technol. 2022. [CrossRef]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Kamper, R.S.; Aagaard, P.; Haddock, B.; Prescott, E.; Ara, I.; Suetta, C. Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: Validation and translation to functional performance. Sci. Rep. 2020, 10, 16337. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, U.; Farahmand, P.; Klenk, J.; Blatzonis, K.; Becker, C. Validity of linear encoder measurement of sit-to-stand performance power in older people. Physiotherapy 2015, 101, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, A.T.; Orange, S.T.; Wang, Y.; Lustin, R.; Vega, A.; Quiles, N. Comparison of two popular transducers to measure sit-to-stand power in older adults. PLoS ONE 2024, 19, e0308808. [Google Scholar] [CrossRef]
- Orange, S.T.; Metcalfe, J.W.; Liefeith, A.; Jordan, A.R. Validity of various portable devices to measure sit-to-stand velocity and power in older adults. Gait Posture 2020, 76, 409–414. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Borg, D.N.; Bach, A.J.E.; O’Brien, J.L.; Sainani, K.L. Calculating sample size for reliability studies. PM&R 2022, 14, 1018–1025. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Reid, K.F.; Fielding, R.A. Skeletal muscle power: A critical determinant of physical functioning in older adults. Exerc. Sport Sci. Rev. 2012, 40, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Bean, J.F.; Leveille, S.G.; Kiely, D.K.; Bandinelli, S.; Guralnik, J.M.; Ferrucci, L. A comparison of leg power and leg strength within the InCHIANTI study: Which influences mobility more? J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 728–733. [Google Scholar] [CrossRef] [PubMed]
- De Melo, T.A.; Duarte, A.C.M.; Bezerra, T.S.; França, F.; Soares, N.S.; Brito, D. The Five Times Sit-to-Stand Test: Safety and reliability with older intensive care unit patients at discharge. Rev. Bras. Ter. Intensiva 2019, 31, 27–33. [Google Scholar] [CrossRef]
- Ruiz-Cárdenas, J.D.; Rodríguez-Juan, J.J.; Smart, R.R.; Jakobi, J.M.; Jones, G.R. Validity and reliability of an iPhone App to assess time, velocity and leg power during a sit-to-stand functional performance test. Gait Posture 2018, 59, 261–266. [Google Scholar] [CrossRef]
- Bischoff, H.A.; Stähelin, H.B.; Monsch, A.U.; Iversen, M.D.; Weyh, A.; von Dechend, M.; Akos, R.; Conzelmann, M.; Dick, W.; Theiler, R. Identifying a cut-off point for normal mobility: A comparison of the timed “up and go” test in community-dwelling and institutionalised elderly women. Age Ageing 2003, 32, 315–320. [Google Scholar] [CrossRef]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; Di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Sherwood, J.J.; Inouye, C.; Webb, S.L.; Jenny, O. Reliability and Validity of the Sit-to-Stand as a Muscular Power Measure in Older Adults. J. Aging Phys. Act. 2019, 28, 455–466. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Mean ± SD |
|---|---|
| Female, % a | 60 (56.6%) |
| Age, years | 72.9 ± 5.0 |
| Weight, kg | 68.2 ± 10.4 |
| Height, m | 1.57 ± 0.09 |
| BMI, kg/m2 b | 27.4 (24.4, 31.3) |
| Speed, m/s b | 0.52 (0.36, 0.62) |
| Power, w b | 10.0 (7.0, 13.0) |
| Distance, cm | 49.6 ± 8.6 |
| 5STS, s b | 10.5 (7.4, 13.5) |
| 30CS | 14.0 ± 4.0 |
| 5STS | 30CS | |||||
|---|---|---|---|---|---|---|
| r | rp | p | r | rp | p | |
| Speed | −0.80 (−0.86–−0.71) | −0.71 | <0.001 | 0.80 (0.72–0.86) | 0.72 | <0.001 |
| Power | −0.76 (−0.84–−0.69) | −0.69 | <0.001 | 0.78 (0.70–0.85) | 0.70 | <0.001 |
| Variables | Interobserver ICC (95% CI) | p | Intraobserver ICC (95% CI) | p |
|---|---|---|---|---|
| Speed | 0.90 (0.86–0.93) | <0.001 | 0.85 (0.79–0.90) | <0.001 |
| Power | 0.88 (0.82–0.91) | <0.001 | 0.79 (0.71–0.85) | <0.001 |
| B 5STS (95% CI) | p | B 30CS (95% CI) | p | |
|---|---|---|---|---|
| Speed | −0.036 (−0.042–−0.03) | <0.001 | 0.024 (0.020–0.027) | <0.001 |
| Power | −0.71 (−0.83–−0.58) | <0.001 | 0.46 (0.39–0.54) | <0.001 |
| Variables | Frail (n = 36) | Non-Frail (n = 69) | p |
|---|---|---|---|
| Speed, m/s | 0.40 ± 0.04 | 0.58 ± 0.08 | <0.001 |
| Power, w | 7.8 ± 0.7 | 11.3 ± 1.8 | <0.001 |
| Distance, cm | 48.2 ± 7.8 | 47.9 ± 7.9 | 0.567 |
| 5STS, s | 14.7 ± 2.0 | 9.7 ± 1.3 | <0.001 |
| 30CS | 9.8 ± 2.0 | 15.9 ± 2.6 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polo-Ferrero, L.; Sánchez-Tocino, M.L.; Dávila-Marcos, A.; Carrera-Villegas, M.B.; Sánchez-Sánchez, M.C.; Méndez-Sánchez, R. Reliability and Validity of the Linear Transducer “ADR Encoder” for Measuring Power and Speed of the Sit-to-Stand Tests in Older Adults. Diagnostics 2025, 15, 1475. https://doi.org/10.3390/diagnostics15121475
Polo-Ferrero L, Sánchez-Tocino ML, Dávila-Marcos A, Carrera-Villegas MB, Sánchez-Sánchez MC, Méndez-Sánchez R. Reliability and Validity of the Linear Transducer “ADR Encoder” for Measuring Power and Speed of the Sit-to-Stand Tests in Older Adults. Diagnostics. 2025; 15(12):1475. https://doi.org/10.3390/diagnostics15121475
Chicago/Turabian StylePolo-Ferrero, Luis, María Luz Sánchez-Tocino, Arturo Dávila-Marcos, Marta Beatriz Carrera-Villegas, María Carmen Sánchez-Sánchez, and Roberto Méndez-Sánchez. 2025. "Reliability and Validity of the Linear Transducer “ADR Encoder” for Measuring Power and Speed of the Sit-to-Stand Tests in Older Adults" Diagnostics 15, no. 12: 1475. https://doi.org/10.3390/diagnostics15121475
APA StylePolo-Ferrero, L., Sánchez-Tocino, M. L., Dávila-Marcos, A., Carrera-Villegas, M. B., Sánchez-Sánchez, M. C., & Méndez-Sánchez, R. (2025). Reliability and Validity of the Linear Transducer “ADR Encoder” for Measuring Power and Speed of the Sit-to-Stand Tests in Older Adults. Diagnostics, 15(12), 1475. https://doi.org/10.3390/diagnostics15121475