
The Contribution of Mediastinal Transbronchial Nodal Cryobiopsy to Morpho-Histological and Molecular Diagnosis

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
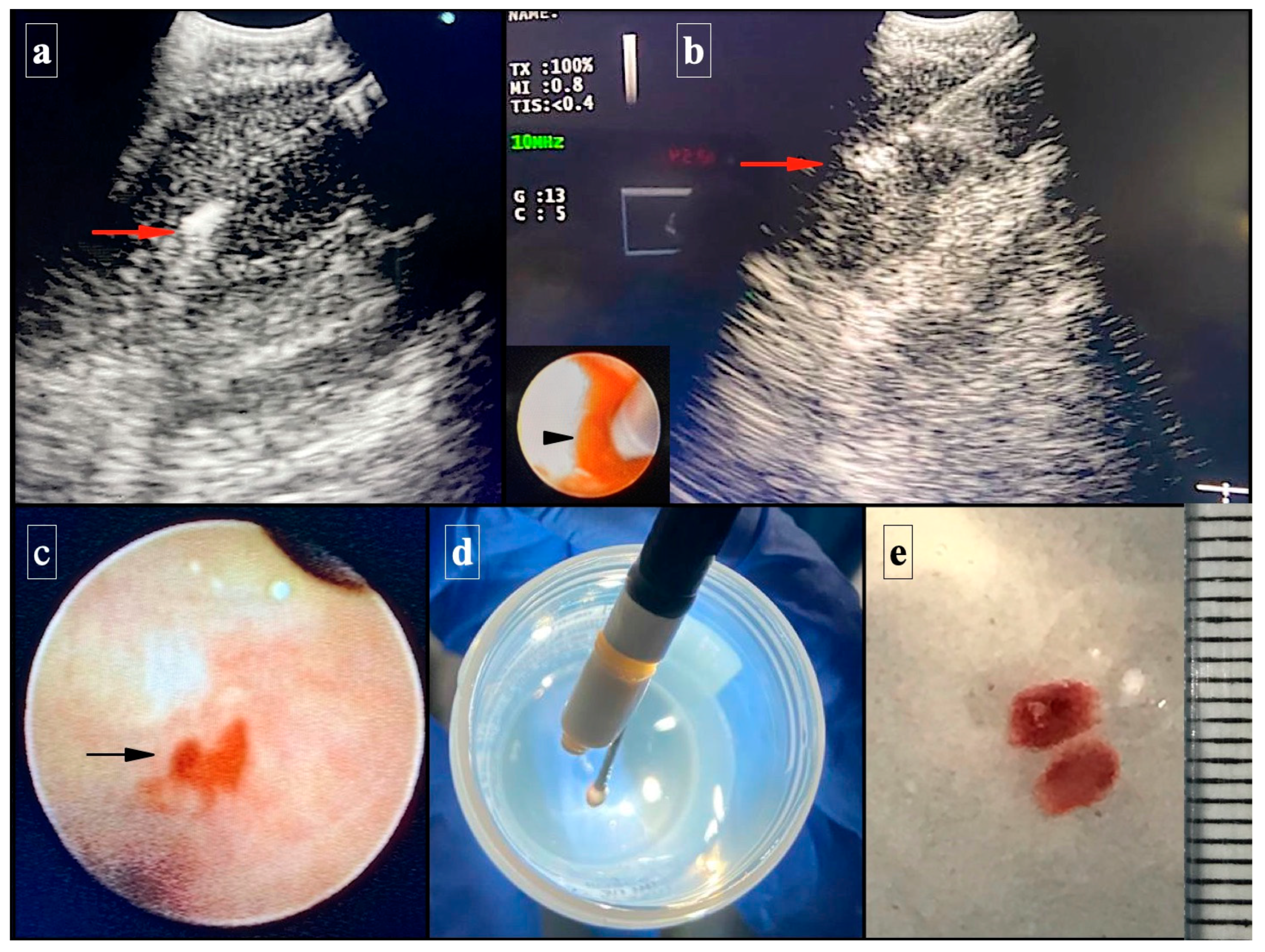
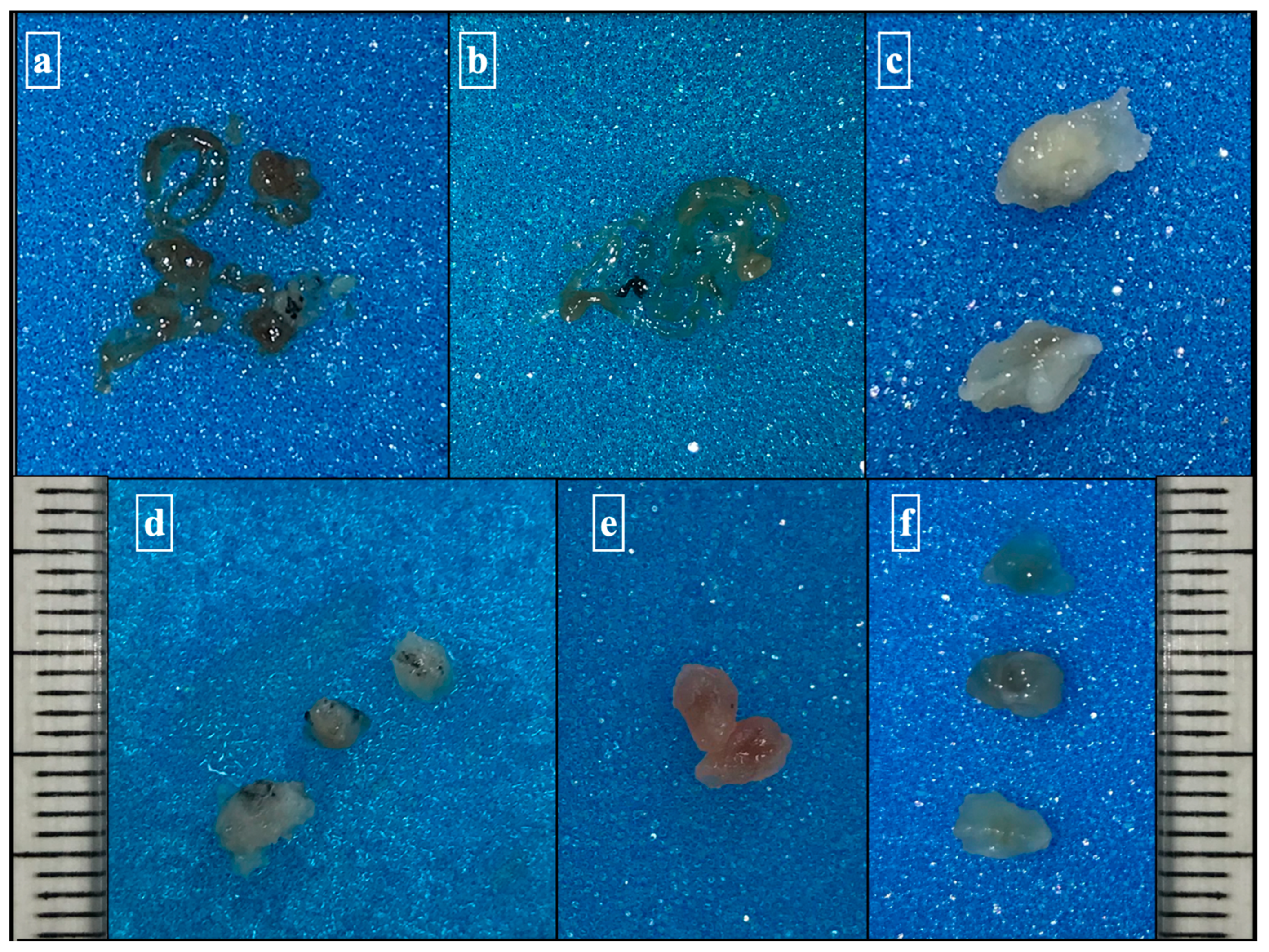
2.1. Technical EBUS-TBCNB Procedure
2.2. Molecular Study
2.3. Statistical Analysis
2.4. Ethical Aspects
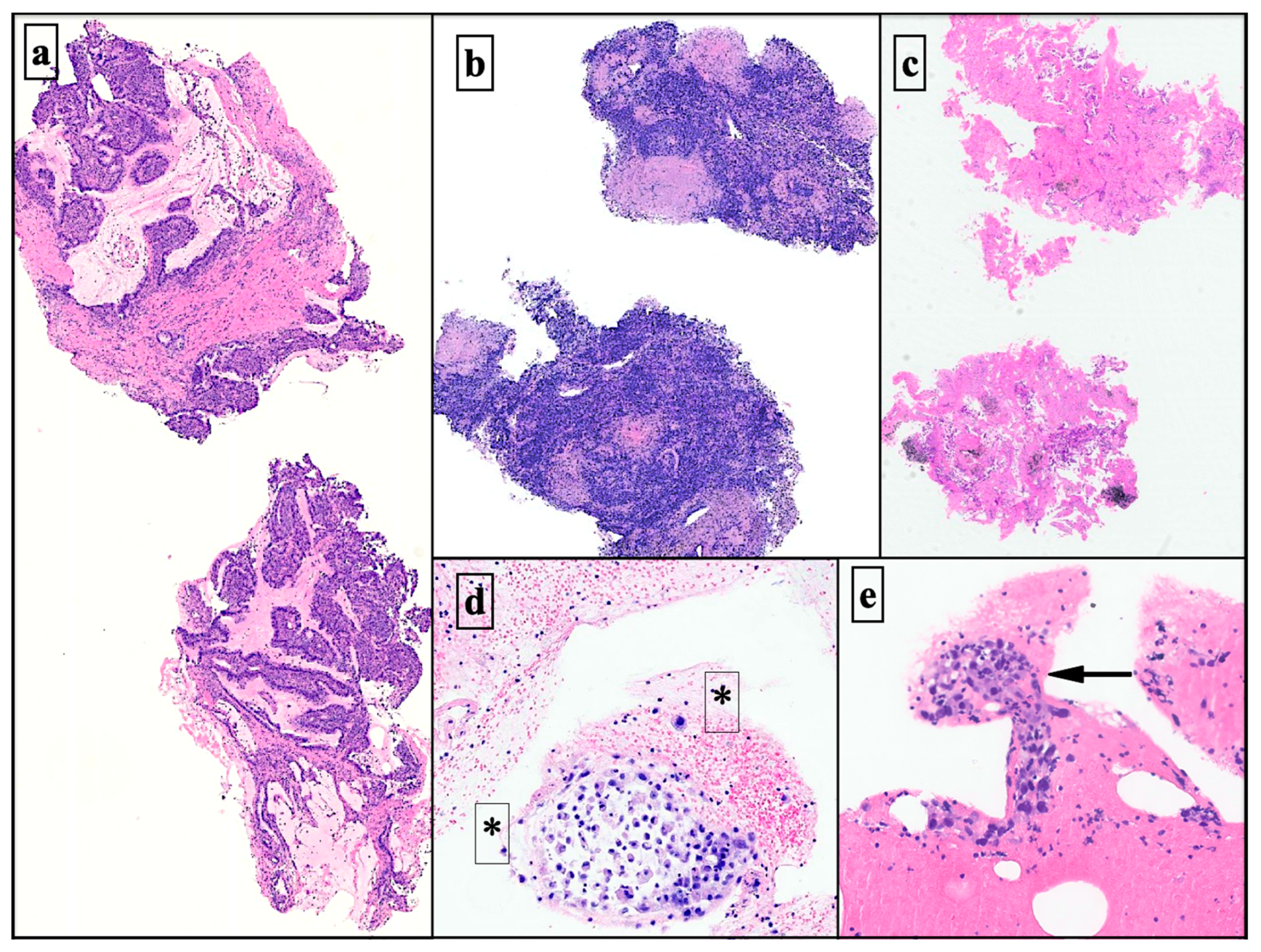
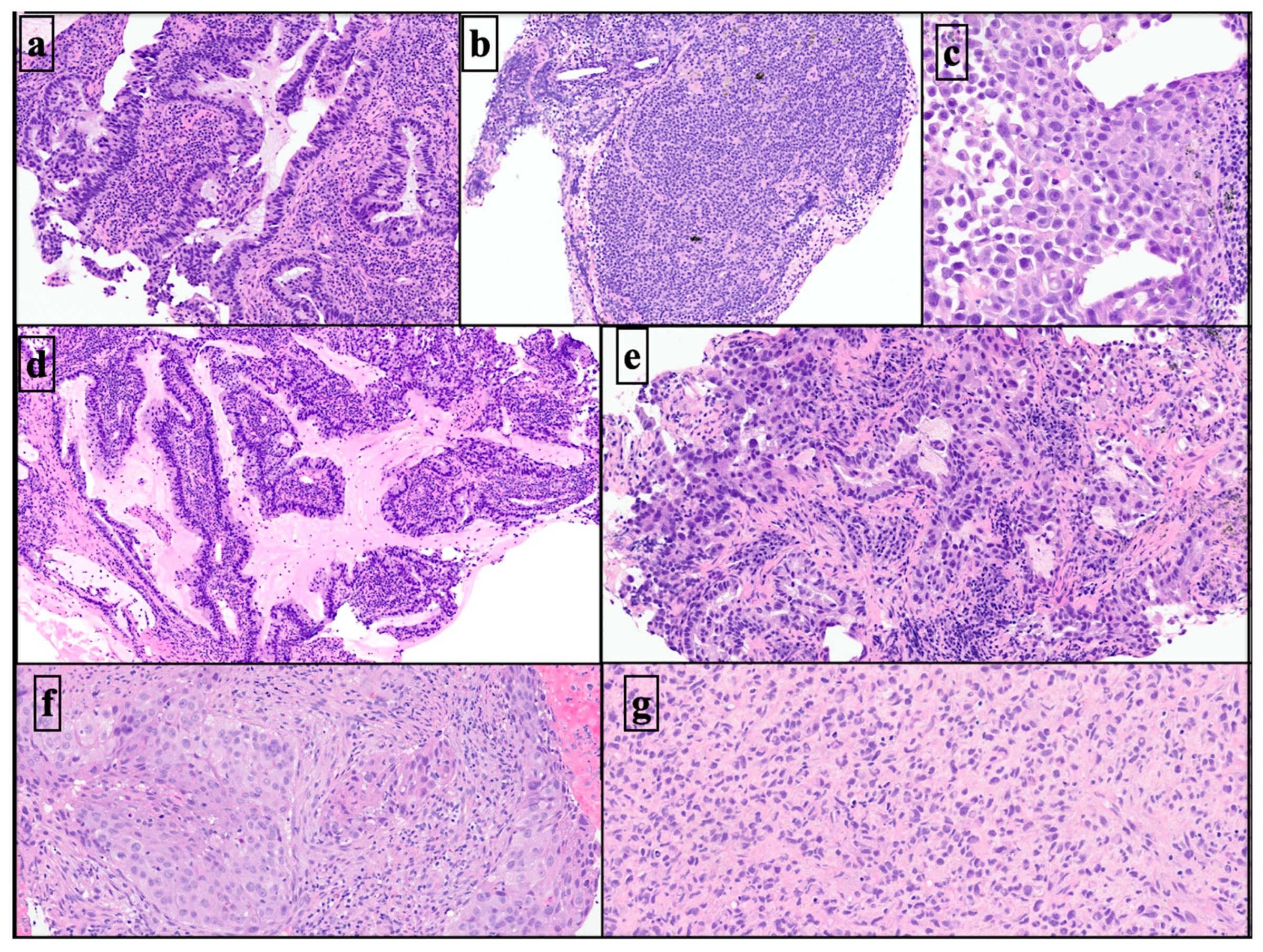
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roden, A.C.; Moreira, A.L. (Eds.) Mediastinal Lesions; Springer International Publishing: Cham, Switzerland, 2017; ISBN 978-3-319-48377-1. [Google Scholar]
- Roy-Chowdhuri, S.; Dacic, S.; Ghofrani, M.; Illei, P.B.; Layfield, L.J.; Lee, C.; Michael, C.W.; Miller, R.A.; Mitchell, J.W.; Nikolic, B.; et al. Collection and Handling of Thoracic Small Biopsy and Cytology Specimens for Ancillary Studies: Guideline From the College of American Pathologists in Collaboration With the American College of Chest Physicians, Association for Molecular Pathology, American Society of Cytopathology, American Thoracic Society, Pulmonary Pathology Society, Papanicolaou Society of Cytopathology, Society of Interventional Radiology, and Society of Thoracic Radiology. Arch. Pathol. Lab. Med. 2020, 144, 933–958. [Google Scholar] [CrossRef]
- Lozano, M.D.; Benito, A.; Labiano, T.; Pijuan, L.; Tejerina, E.; Torres, H.; Gómez-Román, J. Recommendations for Optimizing the Use of Cytology in the Diagnosis and Management of Patients with Lung Cancer. Rev. Española Patol. 2023, 56, 58–68. [Google Scholar] [CrossRef]
- Organisation Mondiale de la Santé; Centre International de Recherche sur le Cancer (Eds.) Thoracic Tumours, 5th ed.; World Health Organization Classification of Tumours; International Agency for Research on Cancer: Lyon, France, 2021; ISBN 978-92-832-4506-3. [Google Scholar]
- Nicholson, A.G.; Tsao, M.S.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Cooper, W.A.; Dacic, S.; Jain, D.; Kerr, K.M.; Lantuejoul, S.; et al. The 2021 WHO Classification of Lung Tumors: Impact of Advances Since 2015. J. Thorac. Oncol. 2022, 17, 362–387. [Google Scholar] [CrossRef]
- Isla, D.; Lozano, M.D.; Paz-Ares, L.; Salas, C.; De Castro, J.; Conde, E.; Felip, E.; Gómez-Román, J.; Garrido, P.; Enguita, A.B. New Update to the Guidelines on Testing Predictive Biomarkers in Non-Small-Cell Lung Cancer: A National Consensus of the Spanish Society of Pathology and the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2022, 25, 1252–1267. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.; Lozano, M.D. Molecular/Biomarker Testing in Lung Cytology: A Practical Approach. Diagn. Cytopathol. 2023, 51, 59–67. [Google Scholar] [CrossRef]
- Qvick, A.; Stenmark, B.; Carlsson, J.; Isaksson, J.; Karlsson, C.; Helenius, G. Liquid Biopsy as an Option for Predictive Testing and Prognosis in Patients with Lung Cancer. Mol. Med. 2021, 27, 68. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Lederer, D.J.; Rabe, K.F. Cryobiopsy for Interstitial Lung Disease: The Heat Is On. Am. J. Respir. Crit. Care Med. 2019, 199, 1183–1184. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Ghori, U.; Chaddha, U.; Murgu, S. Combined EBUS-IFB and EBUS-TBNA vs. EBUS-TBNA Alone for Intrathoracic Adenopathy: A Meta-Analysis. Ann. Thorac. Surg. 2022, 114, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Prota, M.; Pérez-Pallarés, J.; Fernández-Fernández, A.; García-Alfonso, L.; Cascón, J.A.; Torres-Rivas, H.; Fernández-Fernández, L.; Sánchez, I.; Gil, M.; García-Clemente, M.; et al. Endobronchial Ultrasound-Guided Transbronchial Mediastinal Cryobiopsy in the Diagnosis of Mediastinal Lesions: Safety, Feasibility and Diagnostic Yield—Experience in 50 Cases. ERJ Open Res. 2023, 9, 00448–02022. [Google Scholar] [CrossRef] [PubMed]
- Genova, C.; Tagliabue, E.; Mora, M.; Aloè, T.; Dono, M.; Salvi, S.; Zullo, L.; Barisione, E. Potential Application of Cryobiopsy for Histo-Molecular Characterization of Mediastinal Lymph Nodes in Patients with Thoracic Malignancies: A Case Presentation Series and Implications for Future Developments. BMC Pulm. Med. 2022, 22, 5. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Prota, M.A.; Pérez-Pallarés, J.; Fernández-Fernández, A.; López-González, F.; Cascón, J.A.; García-Alfonso, L.; Torres-Rivas, H.; Fernández-Fernández, L.; Sánchez, I.; Gil, M.; et al. Transbronchial Mediastinal Cryobiopsy in the Diagnosis of Mediastinal Lymph Nodes: A Case Series—How to Do It. Arch. Bronconeumol. 2022, 58, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Gonuguntla, H.K.; Shah, M.; Gupta, N.; Agrawal, S.; Poletti, V.; Nacheli, G.C. Endobronchial Ultrasound-guided Transbronchial Cryo-nodal Biopsy: A Novel Approach for Mediastinal Lymph Node Sampling. Respirol. Case Rep. 2021, 9, e00808. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Folch, E.; Jantz, M.; Mehta, H.J.; Majid, A.; Fernandez-Bussy, S. Adequacy of Samples Obtained by Endobronchial Ultrasound with Transbronchial Needle Aspiration for Molecular Analysis in Patients with Non–Small Cell Lung Cancer. Systematic Review and Meta-Analysis. Ann. Am. Thorac. Soc. 2018, 15, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Maturu, V.N.; Prasad, V.P.; Vaddepally, C.R.; Dommata, R.R.; Sethi, S. Endobronchial Ultrasound-Guided Mediastinal Lymph Nodal Cryobiopsy in Patients With Nondiagnostic/Inadequate Rapid On-Site Evaluation: A New Step in the Diagnostic Algorithm. J. Bronchol. Interv. Pulmonol. 2023, 6, 10–97. [Google Scholar] [CrossRef]
- Mondoni, M.; Sotgiu, G. Optimizing the Endoscopic Diagnosis of Mediastinal Lymphadenopathy: A Glimpse on Cryobiopsy. BMC Pulm. Med. 2022, 22, 355. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Kim, R.Y.; McGrath, C.M.; Andronov, M.; Haas, A.R.; Ma, K.C.; Lanfranco, A.R.; Hutchinson, C.T.; Morrissette, J.J.D.; DiBardino, D.M. The Performance of an Extended Next Generation Sequencing Panel Using Endobronchial Ultrasound-Guided Fine Needle Aspiration Samples in Non-Squamous Non-Small Cell Lung Cancer: A Pragmatic Study. Clin. Lung Cancer 2023, 24, e105–e112. [Google Scholar] [CrossRef]
- Zhang, J.; Guo, J.-R.; Huang, Z.-S.; Fu, W.-L.; Wu, X.-L.; Wu, N.; Kuebler, W.M.; Herth, F.J.F.; Fan, Y. Transbronchial Mediastinal Cryobiopsy in the Diagnosis of Mediastinal Lesions: A Randomised Trial. Eur. Respir. J. 2021, 58, 2100055. [Google Scholar] [CrossRef] [PubMed]
- Layfield, L.J.; Baloch, Z. (Eds.) The Papanicolaou Society of Cytopathology System for Reporting Respiratory Cytology: Definitions, Criteria, Explanatory Notes, and Recommendations for Ancillary Testing; Springer International Publishing: Cham, Switzerland, 2019; ISBN 978-3-319-97234-3. [Google Scholar]
- Torre, M.; Reda, M.; Musso, V.; Danuzzo, F.; Mohamed, S.; Conforti, S. Diagnostic Accuracy of Endobronchial Ultrasound-Transbronchial Needle Aspiration (EBUS-TBNA) for Mediastinal Lymph Node Staging of Lung Cancer. Mediastinum 2021, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Asano, F.; Aoe, M.; Ohsaki, Y.; Okada, Y.; Sasada, S.; Sato, S.; Suzuki, E.; Semba, H.; Fukuoka, K.; Fujino, S.; et al. Complications Associated with Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration: A Nationwide Survey by the Japan Society for Respiratory Endoscopy. Respir. Res. 2013, 14, 50. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%)/Mean ± SD | ||
|---|---|---|
| Gender | Male | 20 (74.07%) |
| Female | 7 (25.93%) | |
| Total | 27 (100%) | |
| Age | 56.1 ± 14.6 | |
| Tobacco | Smoker | 6 (22.22%) |
| Non-smoker | 11 (40.74%) | |
| Former smoker | 10 (37.04%) | |
| Total | 27 (100%) | |
| ROSE 1 | Yes | 22 (81.48%) |
| No | 5 (18.52%) | |
| Total | 27 (100%) |
| N (%) | ||
|---|---|---|
| Needle size | 19 G | 4 (14.81%) |
| 21 G | 4 (14.81%) | |
| 22 G | 19 (70.37%) | |
| Total | 27 (100%) | |
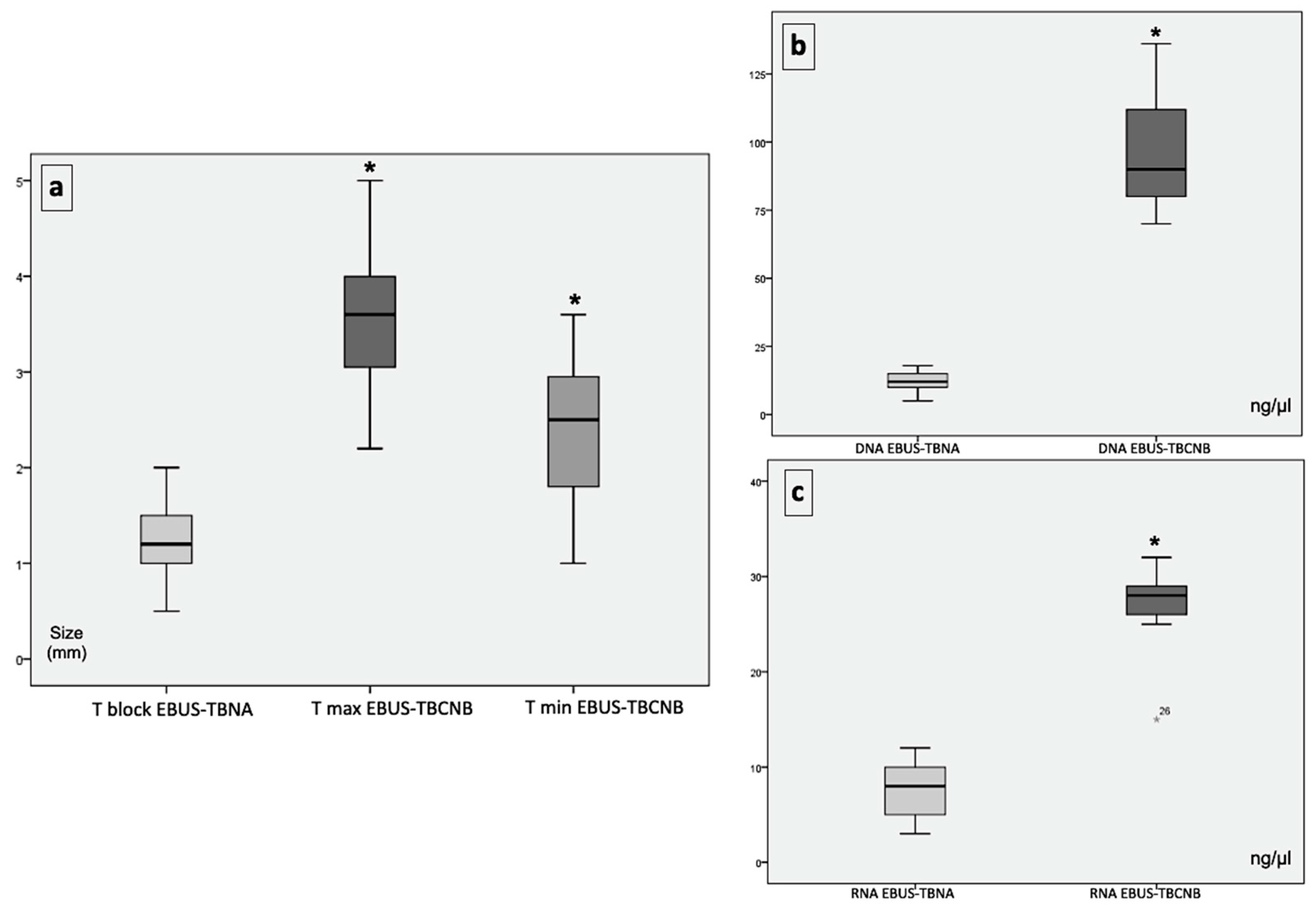
| Number of cryobiopsy fragments | 3.4 ± 1.4 | |
| EBUS-TBCNB maximum fragment sizes (mm) | 3.5 ± 0.7 | |
| EBUS-TBCNB minimum fragment sizes (mm) | 2.3 ± 0.7 | |
| EBUS-TBNA cell block sizes (mm) | 1.2 ± 0.5 |
| N (%) | ||
|---|---|---|
| Diagnostic categories in EBUS-TBNA 1 | I | 0 (0%) |
| II | 9 (33.33%) | |
| III | 0 (0%) | |
| IV | 0 (0%) | |
| V | 0 (0%) | |
| VI | 18 (66.67%) | |
| Total | 27 (100%) | |
| Histological diagnoses in EBUS-TBCNB | Adenocarcinoma metastases | 8 (29.63%) |
| Squamous cell carcinoma metastases | 1 (3.70%) | |
| Small cell neuroendocrine carcinoma metastases | 2 (7.41%) | |
| Large cell neuroendocrine carcinoma metastases | 1 (3.70%) | |
| Melanoma metastasis | 3 (11.11%) | |
| Lymphoma | 1 (3.70%) | |
| Sarcoma | 1 (3.70%) | |
| Urothelial carcinoma metastases | 1 (3.70%) | |
| Granulomatous lymphadenitis * | 5 (18.52%) | |
| Reactive lymphadenitis ** | 2 (7.41%) | |
| Not valid for diagnosis | 2 (7.41%) | |
| Total | 27 (100%) | |
| Malignant neoplastic processes | Yes | 18 (66.67%) |
| No | 9 (33.33%) | |
| Total | 27 (100%) | |
| Lung primary origin | Yes | 12 (66.67%) |
| No | 6 (33.33%) | |
| Total | 18 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasco-Albendea, F.J.; Cruz-Rueda, J.J.; Gil-Belmonte, M.J.; Pérez-Rodríguez, Á.; López-Pardo, A.; Agredano-Ávila, B.; Lozano-Paniagua, D.; Nievas-Soriano, B.J. The Contribution of Mediastinal Transbronchial Nodal Cryobiopsy to Morpho-Histological and Molecular Diagnosis. Diagnostics 2023, 13, 3476. https://doi.org/10.3390/diagnostics13223476
Velasco-Albendea FJ, Cruz-Rueda JJ, Gil-Belmonte MJ, Pérez-Rodríguez Á, López-Pardo A, Agredano-Ávila B, Lozano-Paniagua D, Nievas-Soriano BJ. The Contribution of Mediastinal Transbronchial Nodal Cryobiopsy to Morpho-Histological and Molecular Diagnosis. Diagnostics. 2023; 13(22):3476. https://doi.org/10.3390/diagnostics13223476
Chicago/Turabian StyleVelasco-Albendea, Francisco Javier, Juan José Cruz-Rueda, María Jesús Gil-Belmonte, Álvaro Pérez-Rodríguez, Andrés López-Pardo, Beatriz Agredano-Ávila, David Lozano-Paniagua, and Bruno José Nievas-Soriano. 2023. "The Contribution of Mediastinal Transbronchial Nodal Cryobiopsy to Morpho-Histological and Molecular Diagnosis" Diagnostics 13, no. 22: 3476. https://doi.org/10.3390/diagnostics13223476
APA StyleVelasco-Albendea, F. J., Cruz-Rueda, J. J., Gil-Belmonte, M. J., Pérez-Rodríguez, Á., López-Pardo, A., Agredano-Ávila, B., Lozano-Paniagua, D., & Nievas-Soriano, B. J. (2023). The Contribution of Mediastinal Transbronchial Nodal Cryobiopsy to Morpho-Histological and Molecular Diagnosis. Diagnostics, 13(22), 3476. https://doi.org/10.3390/diagnostics13223476