Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Clinical Assessment–CRP, ESR, and Visual Analog Scale (VAS)
2.3. Radiological Assessment–Simultaneous FDG-PET/MRI
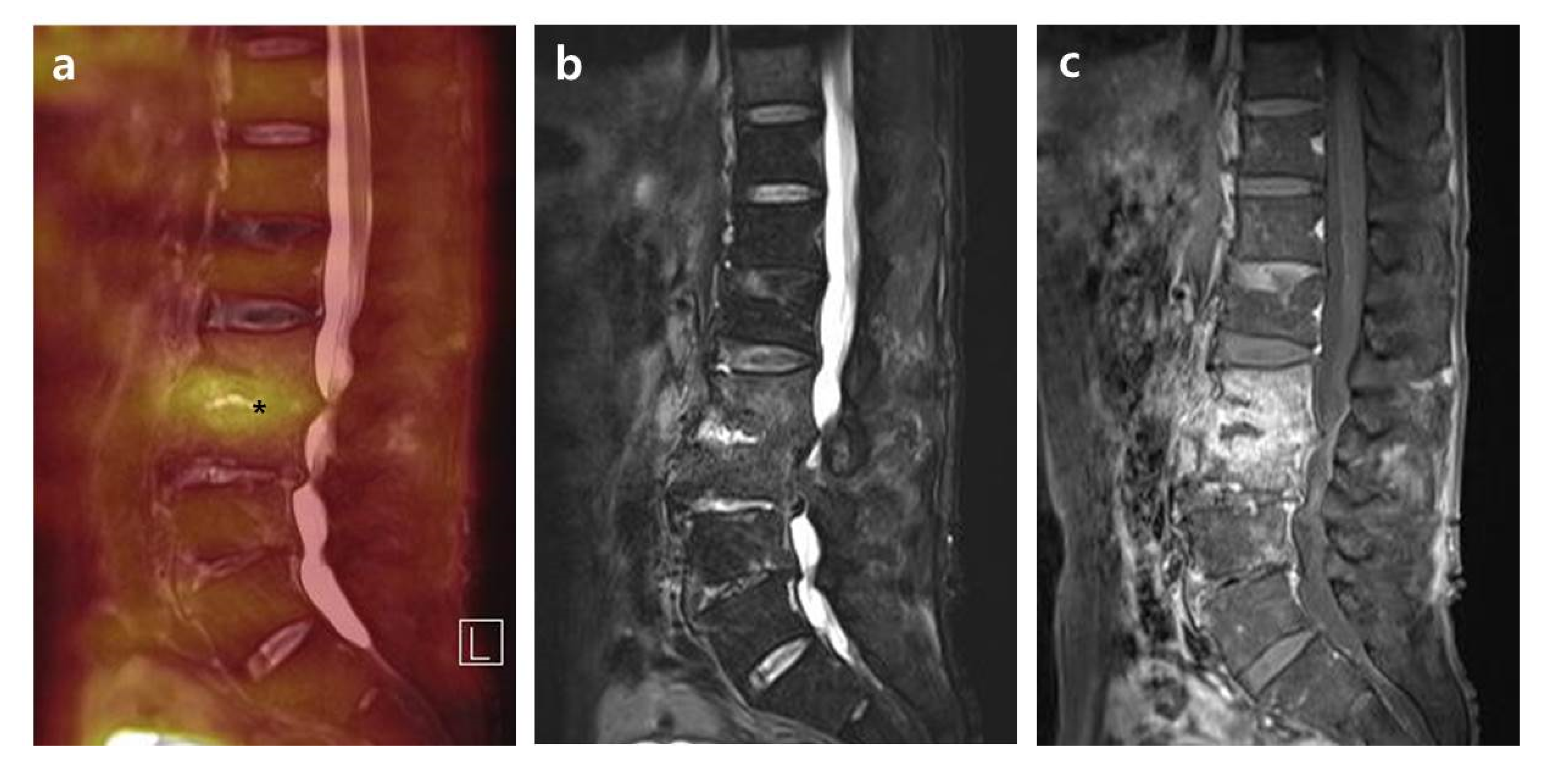
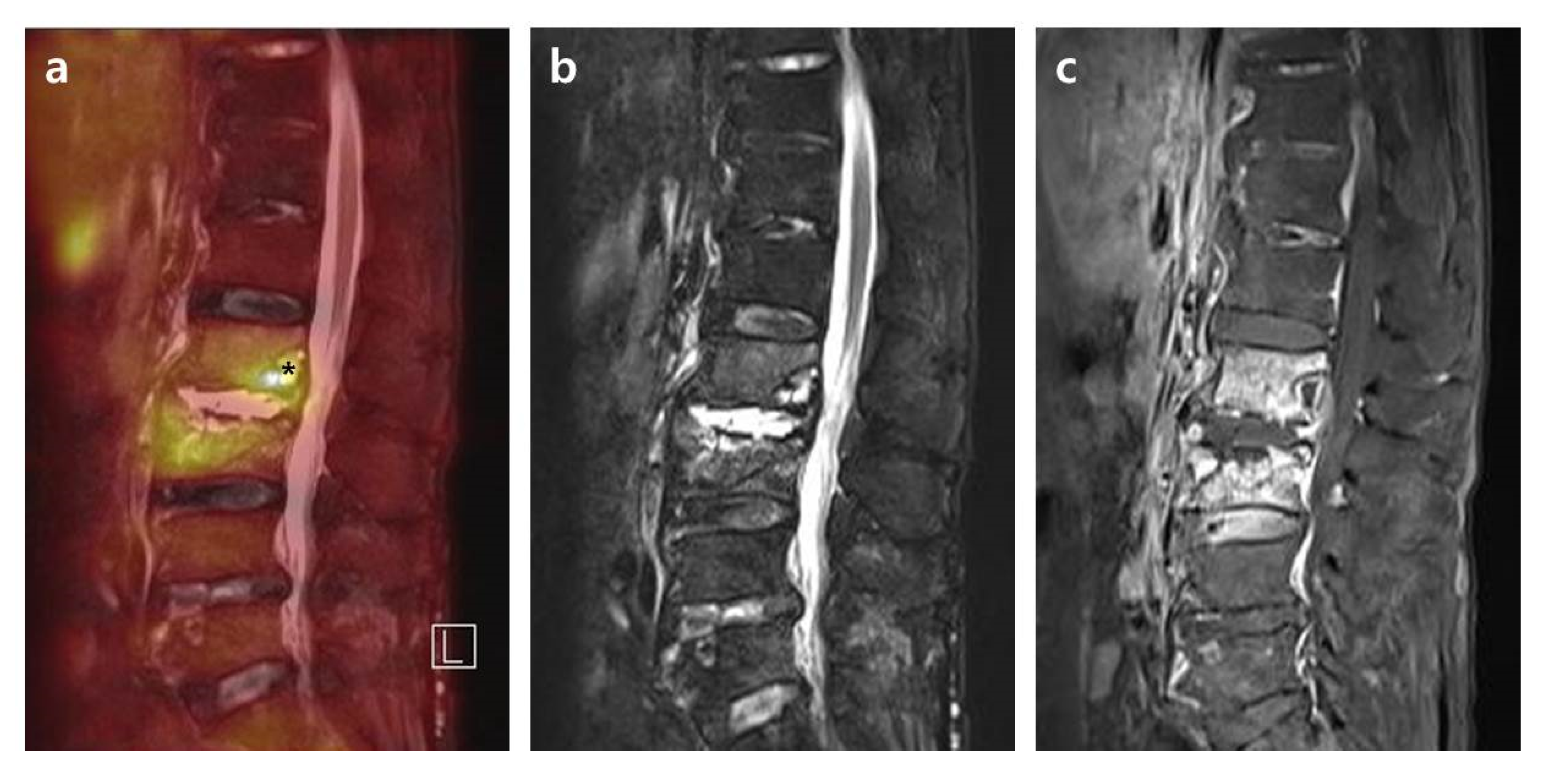
2.3.1. Intensity of FDG Uptake on FDG-PET in PVO Lesion
2.3.2. Distribution Patterns of FDG Uptake on FDG-PET, Contrast Enhancement on T1-Weighted Contrast MRI, and High Signal on T2-Weighted Fat Saturation MRI in PVO Lesion
- Grade I: Activities on the bone, soft tissue, and epidural space with intensity lower than or comparable to the reference.
- Grade II: Limited activities on the margin or bulk of a destroyed disc and endplates rather than the bone, soft tissue, and epidural space with overall higher intensity than the reference.
- Grade III: Significantly increased activities on overall bone and soft tissue than the reference.
2.4. PET/MRI Data Acquisition
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Microorganisms and Antibiotics
3.3. Clinical and Radiological Features of the Cured PVO Lesion
3.4. Distribution Patterns on FDG-PET and MRI in PVO Lesion
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M., 3rd; Petermann, G.W.; et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, Y.S.; Peck, K.R.; Kim, E.S.; Cho, S.Y.; Ha, Y.E.; Kang, C.I.; Chung, D.R.; Song, J.H. Outcome of culture-negative pyogenic vertebral osteomyelitis: Comparison with microbiologically confirmed pyogenic vertebral osteomyelitis. Semin. Arthritis Rheum. 2014, 44, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Zarghooni, K.; Rollinghoff, M.; Sobottke, R.; Eysel, P. Treatment of spondylodiscitis. Int. Orthop. 2012, 36, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Bernard, L.; Dinh, A.; Ghout, I.; Simo, D.; Zeller, V.; Issartel, B.; Le Moing, V.; Belmatoug, N.; Lesprit, P.; Bru, J.P.; et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: An open-label, non-inferiority, randomised, controlled trial. Lancet 2015, 385, 875–882. [Google Scholar] [CrossRef]
- Zimmerli, W. Clinical practice. Vertebral osteomyelitis. N. Engl. J. Med. 2010, 362, 1022–1029. [Google Scholar] [CrossRef]
- Perronne, C.; Saba, J.; Behloul, Z.; Salmon-Ceron, D.; Leport, C.; Vilde, J.L.; Kahn, M.F. Pyogenic and tuberculous spondylodiskitis (vertebral osteomyelitis) in 80 adult patients. Clin. Infect. Dis. 1994, 19, 746–750. [Google Scholar] [CrossRef]
- Zarrouk, V.; Feydy, A.; Salles, F.; Dufour, V.; Guigui, P.; Redondo, A.; Fantin, B. Imaging does not predict the clinical outcome of bacterial vertebral osteomyelitis. Rheumatology 2007, 46, 292–295. [Google Scholar] [CrossRef]
- Carragee, E.J.; Kim, D.; van der Vlugt, T.; Vittum, D. The clinical use of erythrocyte sedimentation rate in pyogenic vertebral osteomyelitis. Spine 1997, 22, 2089–2093. [Google Scholar] [CrossRef]
- Nanni, C.; Boriani, L.; Salvadori, C.; Zamparini, E.; Rorato, G.; Ambrosini, V.; Gasbarrini, A.; Tumietto, F.; Cristini, F.; Scudeller, L.; et al. FDG PET/CT is useful for the interim evaluation of response to therapy in patients affected by haematogenous spondylodiscitis. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Jeon, I.; Kong, E. Application of Simultaneous 18F-FDG PET/MRI for Evaluating Residual Lesion in Pyogenic Spine Infection: A Case Report. Infect. Chemother. 2020, 52, e47. [Google Scholar]
- Jeon, I.; Kong, E.; Kim, S.W. Simultaneous 18F-FDG PET/MRI in tuberculous spondylitis: An independent method for assessing therapeutic response—Case series. BMC Infect. Dis. 2019, 19, 845. [Google Scholar] [CrossRef] [PubMed]
- Fahnert, J.; Purz, S.; Jarvers, J.S.; Heyde, C.E.; Barthel, H.; Stumpp, P.; Kahn, T.; Sabri, O.; Friedrich, B. Use of Simultaneous 18F-FDG PET/MRI for the Detection of Spondylodiskitis. J. Nucl. Med. 2016, 57, 1396–1401. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.J.; Berbari, E.F.; Huddleston, P.M.; Steckelberg, J.M.; Osmon, D.R. Do follow-up imaging examinations provide useful prognostic information in patients with spine infection? Clin. Infect. Dis. 2006, 43, 172–179. [Google Scholar] [CrossRef]
- Yu, G.J.; Koslowsky, I.L.; Riccio, S.A.; Chu, A.K.M.; Rabin, H.R.; Kloiber, R. Diagnostic challenges in pyogenic spinal infection: An expanded role for FDG-PET/CT. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Dell’Atti, C.; Magarelli, N.; Colelli, P.; Balanika, A.; Casale, R.; Bonomo, L. Imaging of spondylodiscitis. Eur. Rev. Med. Pharm. Sci. 2012, 16, 8–19. [Google Scholar]
- Goldsmith, S.J.; Vallabhajosula, S. Clinically proven radiopharmaceuticals for infection imaging: Mechanisms and applications. Semin. Nucl. Med. 2009, 39, 2–10. [Google Scholar] [CrossRef]
- Signore, A.; Glaudemans, A.W. The molecular imaging approach to image infections and inflammation by nuclear medicine techniques. Ann. Nucl. Med. 2011, 25, 681–700. [Google Scholar] [CrossRef]
- Bj0rksten, B.; Boquist, L. Histopathological aspects of chronic recurrent multifocal osteomyelitis. J. Bone Joint Surg. 1980, 62, 376–380. [Google Scholar] [CrossRef]
- Desmouliere, A.; Redard, M.; Darby, I.; Gabbiani, G. Apoptosis mediates the decrease in cellularity during the transition between granulation tissue and scar. Am. J. Pathol. 1995, 146, 56–66. [Google Scholar]
- Gordon, B.A.; Flanagan, F.L.; Dehdashti, F. Whole-body positron emission tomography: Normal variations, pitfalls, and technical considerations. AJR Am. J. Roentgenol. 1997, 169, 1675–1680. [Google Scholar] [CrossRef]
- Garg, G.; Benchekroun, M.T.; Abraham, T. FDG-PET/CT in the Postoperative Period: Utility, Expected Findings, Complications, and Pitfalls. Semin. Nucl. Med. 2017, 47, 579–594. [Google Scholar] [CrossRef]
- Vandoorne, K.; Rohde, D.; Kim, H.Y.; Courties, G.; Wojtkiewicz, G.; Honold, L.; Hoyer, F.F.; Frodermann, V.; Nayar, R.; Herisson, F.; et al. Imaging the Vascular Bone Marrow Niche During Inflammatory Stress. Circ. Res. 2018, 123, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Lyall, A. Identifying and distinguishing treatment effects and complications from malignancy at FDG PET/CT. Radiographics 2013, 33, 1817–1834. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Chauhan, A.; Zhuang, H.; Alavi, A. Assessment of Therapy Response by Fluorine-18 Fluorodeoxyglucose PET in Infection and Inflammation. PET Clin. 2006, 1, 191–198. [Google Scholar] [CrossRef]
- Ertay, T.; Sencan Eren, M.; Karaman, M.; Oktay, G.; Durak, H. (18)F-FDG-PET/CT in Initiation and Progression of Inflammation and Infection. Mol. Imaging Radionucl. Ther. 2017, 26, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Bakheet, S.M.; Powe, J.; Kandil, A.; Ezzat, A.; Rostom, A.; Amartey, J. F-18 FDG uptake in breast infection and inflammation. Clin. Nucl. Med. 2000, 25, 100–103. [Google Scholar] [CrossRef]
- Bhargava, P.; Zhuang, H.; Kumar, R.; Charron, M.; Alavi, A. Iatrogenic artifacts on whole-body F-18 FDG PET imaging. Clin. Nucl. Med. 2004, 29, 429–439. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | Values |
|---|---|
| Age (years) | 64.58 ± 13.01 (31–85) |
| Sex | Male 28, Female 15 |
| Extent of PVO (levels) | 1.21 ± 0.64 (1–4) |
| Group A (n = 31) | 1.16 ± 0.58 |
| Group B (n = 12) | 1.33 ± 0.78 |
| Involvement of PVO | |
| Vertebral body | 18/43 (41.9%) |
| Epidural space | 23/43 (53.5%) |
| Paraspinal muscle | 21/43 (48.8%) |
| Cause of PVO | |
| Spontaneous | 19/43 (44.2%) |
| Procedure-related | 24/43 (55.8%) |
| Injection or acupuncture | 18/24 (75.0%) |
| Operation | 6/24 (25.0%) |
| Comorbidity | |
| Diabetes mellitus | 16/43 (37.2%) |
| Hypertension | 20/43 (46.5%) |
| Hemodialysis | 2/43 (4.7%) |
| Cerebrovascular disease | 3/43 (6.9%) |
| Ischemic heart disease/arrythmia (5/2) | 7/43 (16.3%) |
| Chronic obstructive lung disease | 1/43 (2.3%) |
| Previous cancer history | 2/43 (4.7%) |
| Initial clinical symptoms | |
| Fever | 25/43 (58.1%) |
| Back pain | 41/43 (95.3%) |
| Neurologic deficit | |
| Radiculopathy | 24/43 (55.8%) |
| Weakness | 7/43 (16.3%) |
| Bowel & bladder symptoms | 1/43 (2.3%) |
| Duration of follow-up (months) | 11.30 ± 7.13 (6–35) |
| Factors | Values |
|---|---|
| Bacterial identification | 21/43 (48.8%) |
| MSSA | 6 |
| MRSA | 4 |
| Enterococcus spp. | 2 |
| MRSE | 3 |
| Streptococcus spp. | 5 |
| Klebsiella pneumonia | 1 |
| Non | 22 |
| Bacterial diagnosis | |
| Blood | 6/21 (28.6%) |
| PVO lesion | 19/21 (90.5%) |
| Blood & PVO lesion | 4/21 (19.0%) |
| Duration of parenteral antibiotics (days) | 42.28 ± 14.58 (21–89) |
| Group A | 41.65 ± 14.78 (21–89) |
| Group B | 43.92 ± 14.58 (24–65) |
| Use of vancomycin | 19/43 (44.2%) |
| Culture-positive | |
| MRSA, MRSE, Enterococcus spp. | 9 |
| MSSA, Streptococcus spp. (as 2nd option) | 2 |
| Culture-negative | |
| as 1st option | 3 |
| as 2nd option | 5 |
| Factors | Group A (n = 31) | Group B (n = 12) | p Value | Total (n = 43) |
|---|---|---|---|---|
| Initial | ||||
| CRP (mg/dL) | 8.71 ± 8.63 | 11.92 ± 10.98 | 0.317 | 9.61 ± 9.32 |
| ESR (mm/h) | 61.94 ± 26.63 | 65.67 ± 37.12 | 0.715 | 62.98 ± 29.50 |
| VAS score of back pain | 7.48 ± 1.03 | 8.00 ± 0.74 | 0.121 | 7.63 ± 0.98 |
| When antimicrobial therapy discontinued | ||||
| * CRP (mg/dL) | + 0.97 ± 1.10 | + 0.51 ± 0.31 | 0.041 | + 0.85 ± 0.97 |
| ESR (mm/h) | + 50.61 ± 29.88 | + 41.17 ± 28.16 | 0.351 | + 47.98 ± 29.39 |
| * VAS score of back pain | + 4.29 ± 1.13 | + 3.50 ± 1.00 | 0.040 | + 4.07 ± 1.14 |
| * SUVmax | 4.34 ± 1.24 | 5.89 ± 1.57 | 0.001 | 4.77 ± 1.49 (2.01–8.44) |
| Imagings | Groups | Grade I | Grade II | Grade III | Total |
|---|---|---|---|---|---|
| FDG uptake on FDG-PET | Group A | 0 | 20 | 11 | 31 |
| Group B | 0 | 5 | 7 | 12 | |
| a,b Total | 0 | 25 | 18 | 43 | |
| Contrast enhancement on T1C | Group A | 0 | 4 | 27 | 31 |
| Group B | 0 | 4 | 8 | 12 | |
| a,c Total | 0 | 8 | 35 | 43 | |
| High signal on T2FS | Group A | 0 | 10 | 21 | 31 |
| Group B | 0 | 4 | 8 | 12 | |
| b,c Total | 0 | 14 | 29 | 43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, I.; Kong, E.; Yu, D.; Hong, C.P. Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response. Diagnostics 2020, 10, 861. https://doi.org/10.3390/diagnostics10110861
Jeon I, Kong E, Yu D, Hong CP. Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response. Diagnostics. 2020; 10(11):861. https://doi.org/10.3390/diagnostics10110861
Chicago/Turabian StyleJeon, Ikchan, Eunjung Kong, Dongwoo Yu, and Cheol Pyo Hong. 2020. "Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response" Diagnostics 10, no. 11: 861. https://doi.org/10.3390/diagnostics10110861
APA StyleJeon, I., Kong, E., Yu, D., & Hong, C. P. (2020). Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response. Diagnostics, 10(11), 861. https://doi.org/10.3390/diagnostics10110861