Diagnostic Performance of 18F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
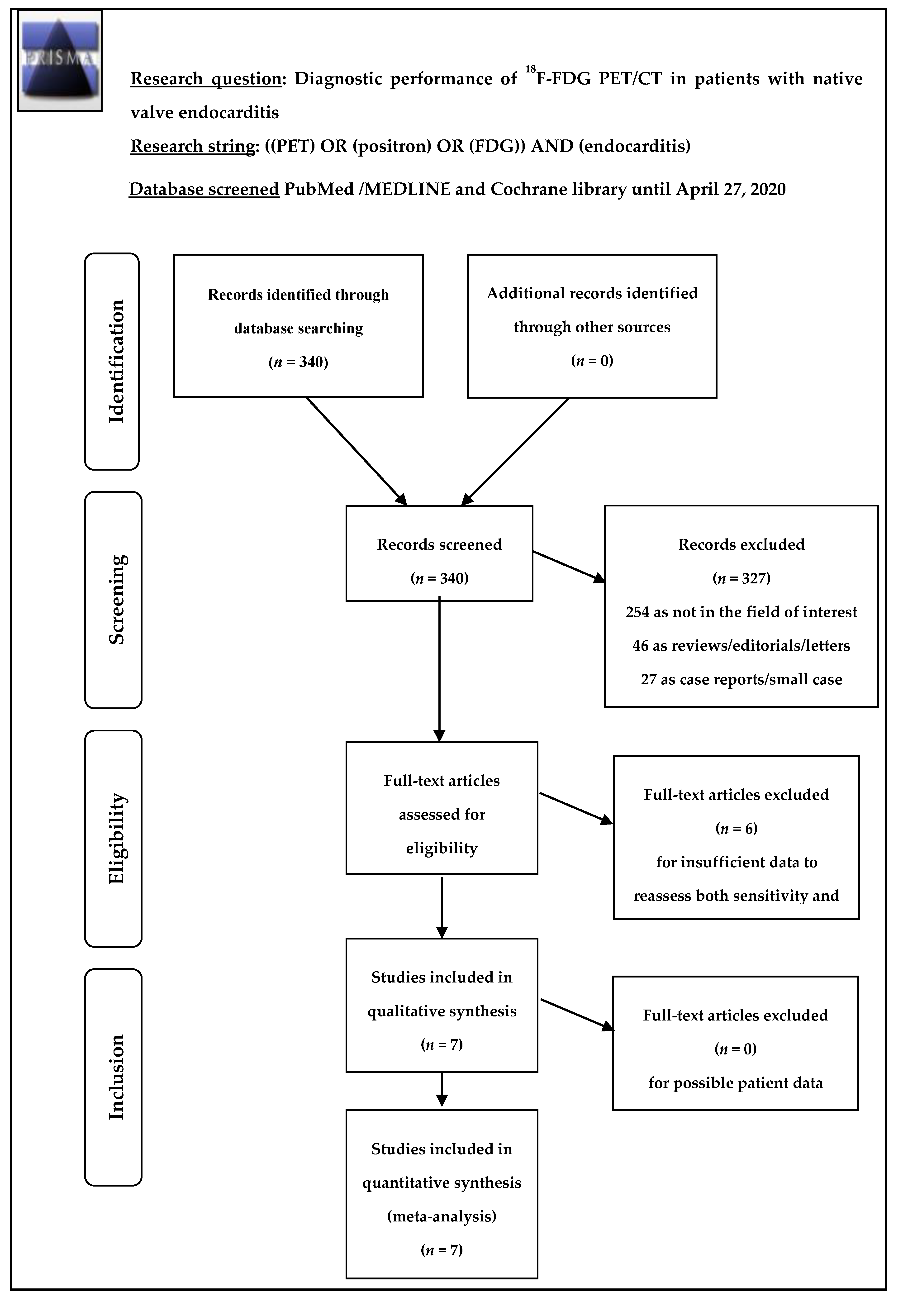
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Qualitative Analysis (Systematic Review)
3.2.1. Basic Study and Patient Characteristics
3.2.2. Technical Aspects
3.2.3. Main Findings
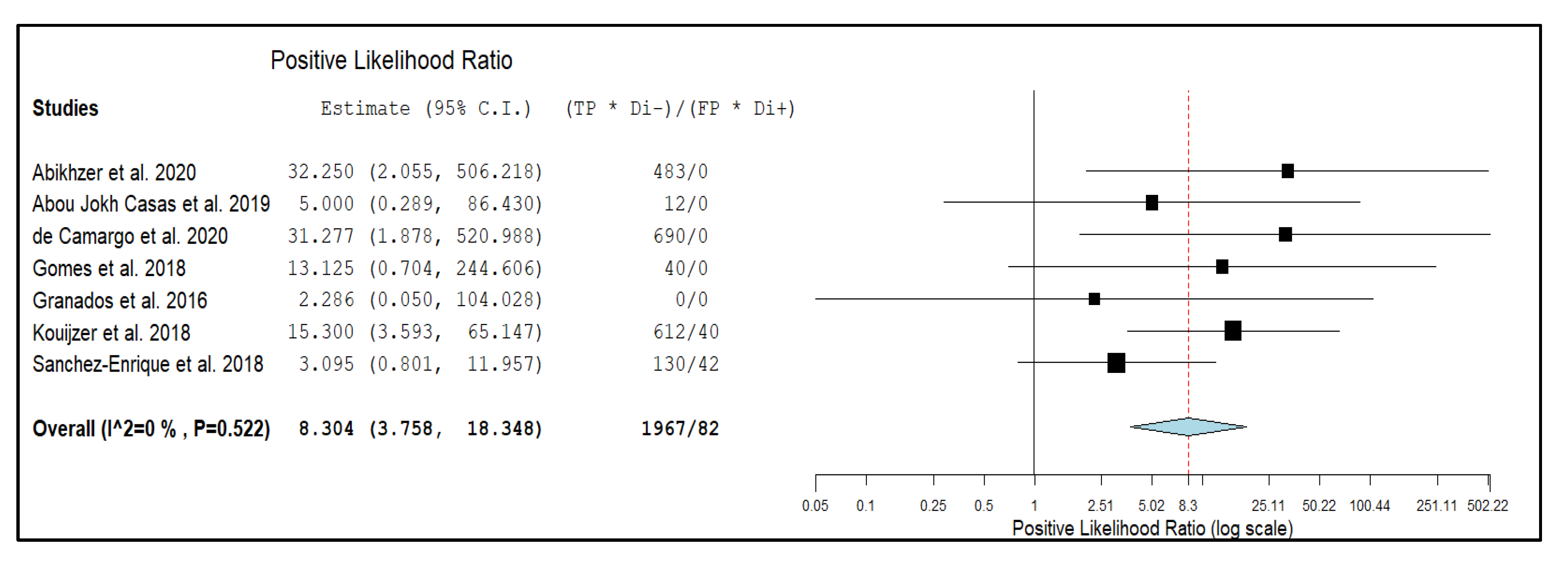
3.3. Quantitative Analysis (Meta-Analysis)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Holland, T.L.; Baddour, L.M.; Bayer, A.S.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr. Infective endocarditis. Nat. Rev. Dis. Primers 2016, 2, 16059. [Google Scholar] [CrossRef] [PubMed]
- Osler, W. The Gulstonian Lectures, on Malignant Endocarditis. Br. Med. J. 1885, 1, 5775–5779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bin Abdulhak, A.A.; Baddour, L.M.; Erwin, P.J.; Hoen, B.; Chu, V.H.; Mensah, G.A.; Tleyjeh, I.M. Global and regional burden of infective endocarditis, 19902–010: A systematic review of the literature. Glob. Heart 2014, 9, 1311–1343. [Google Scholar]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 32223–32232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 4634–4673. [Google Scholar] [CrossRef] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar]
- Habib, G.; Derumeaux, G.; Avierinos, J.F.; Casalta, J.P.; Jamal, F.; Volot, F.; Garcia, M.; Lefevre, J.; Biou, F.; Maximovitch-Rodaminoff, A.; et al. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. J. Am. Coll. Cardiol. 1999, 33, 2023–2029. [Google Scholar] [CrossRef] [Green Version]
- Fukuchi, T.; Iwata, K.; Ohji, G. Failure of early diagnosis of infective endocarditis in Japan—A retrospective descriptive analysis. Medicine (Baltimore) 2014, 93, e237. [Google Scholar] [CrossRef]
- Treglia, G. Diagnostic Performance of (18)F-FDG PET/CT in Infectious and Inflammatory Diseases according to Published Meta-Analyses. Contrast Media Mol. Imaging 2019, 2019, 3018349. [Google Scholar] [CrossRef] [Green Version]
- Saby, L.; Laas, O.; Habib, G.; Cammilleri, S.; Mancini, J.; Tessonnier, L.; Casalta, J.P.; Gouriet, F.; Riberi, A.; Avierinos, J.F.; et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: Increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J. Am. Coll. Cardiol. 2013, 61, 2374–2382. [Google Scholar] [CrossRef] [Green Version]
- Vaidyanathan, S.; Patel, C.N.; Scarsbrook, A.F.; Chowdhury, F.U. FDG PET/CT in infection and inflammation--current and emerging clinical applications. Clin. Radiol. 2015, 70, 787–800. [Google Scholar] [CrossRef]
- Mahmood, M.; Kendi, A.T.; Ajmal, S.; Farid, S.; O’Horo, J.C.; Chareonthaitawee, P.; Baddour, L.M.; Sohail, M.R. Meta-analysis of 18F-FDG PET/CT in the diagnosis of infective endocarditis. J. Nucl. Cardiol. 2019, 26, 9229–9235. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.M.; Sanchez-Nadales, A.; Igbinomwanhia, E.; Cremer, P.; Griffin, B.; Xu, B. Diagnosis of Infective Endocarditis by Subtype Using (18)F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography: A Contemporary Meta-Analysis. Circ. Cardiovasc. Imaging 2020, 13, e010600. [Google Scholar] [CrossRef]
- Gomes, A.; Glaudemans, A.W.J.M.; Touw, D.J.; van Melle, J.P.; Willems, T.P.; Maass, A.H.; Natour, E.; Prakken, N.H.J.; Borra, R.J.H.; van Geel, P.P.; et al. Diagnostic value of imaging in infective endocarditis: A systematic review. Lancet Infect. Dis. 2017, 17, e1–e14. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; the PRISMA-DTA Group; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 3883–3896. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. Group Q-. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Abikhzer, G.; Martineau, P.; Gregoire, J.; Finnerty, V.; Harel, F.; Pelletier-Galarneau, M. [(18)F]FDG-PET CT for the evaluation of native valve endocarditis. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Abou Jokh Casas, E.; Pubul Nunez, V.; Pombo Pasin, M.D.C.; Garrido Pumar, M.; Martinez, M.A.; Abou Jokh Casas, C.; Martinez de Alegria, A.; Dominguez, M.J.; Ruibal Morell, A. Advantages and limitations of 18-fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography in the diagnosis of infective endocarditis. Rev. Port. Cardiol. 2019, 38, 5735–5780. [Google Scholar] [CrossRef]
- de Camargo, R.A.; Sommer Bitencourt, M.; Meneghetti, J.C.; Soares, J.; Goncalves, L.F.T.; Buchpiguel, C.A.; Paixao, M.R.; Felicio, M.F.; de Matos Soeiro, A.; Varejao Strabelli, T.M.; et al. The Role of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Diagnosis of Left-sided Endocarditis: Native vs Prosthetic Valves Endocarditis. Clin. Infect. Dis. 2020, 70, 5835–5894. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.; van Geel, P.P.; Santing, M.; Prakken, N.H.J.; Ruis, M.L.; van Assen, S.; Slart, R.; Sinha, B.; Glaudemans, A. Imaging infective endocarditis: Adherence to a diagnostic flowchart and direct comparison of imaging techniques. J. Nucl. Cardiol. 2020, 27, 592–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granados, U.; Fuster, D.; Pericas, J.M.; Llopis, J.L.; Ninot, S.; Quintana, E.; Almela, M.; Pare, C.; Tolosana, J.M.; Falces, C.; et al. Diagnostic Accuracy of 18F-FDG PET/CT in Infective Endocarditis and Implantable Cardiac Electronic Device Infection: A Cross-Sectional Study. J. Nucl. Med. 2016, 57, 17261–17732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouijzer, I.J.E.; Berrevoets, M.A.H.; Aarntzen, E.; de Vries, J.; van Dijk, A.P.J.; Oyen, W.J.G.; de Geus-Oei, L.F.; Bleeker-Rovers, C.P. 18F-fluorodeoxyglucose positron-emission tomography combined with computed tomography as a diagnostic tool in native valve endocarditis. Nucl. Med. Commun. 2018, 39, 747–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Enrique, C.; Olmos, C.; Jimenez-Ballve, A.; Fernandez-Perez, C.; Ferrera, C.; Perez-Castejon, M.J.; Ortega Candil, A.; Delgado-Bolton, R.; Carnero, M.; Maroto, L.; et al. Usefulness of (18)F Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Infective Endocarditis in Daily Practice: Individualized Analysis of Each Potential Focus of Infection: A Prospective Cohort Study. JACC Cardiovasc. Imaging 2018, 11, 19201–19922. [Google Scholar] [CrossRef] [PubMed]
- Osborne, M.T.; Hulten, E.A.; Murthy, V.L.; Skali, H.; Taqueti, V.R.; Dorbala, S.; DiCarli, M.F.; Blankstein, R. Patient preparation for cardiac fluorine-18 fluorodeoxyglucose positron emission tomography imaging of inflammation. J. Nucl. Cardiol. 2017, 24, 86–99. [Google Scholar] [CrossRef] [Green Version]
- De Castro, S.; d’Amati, G.; Cartoni, D.; Venditti, M.; Magni, G.; Gallo, P.; Beni, S.; Fiorelli, M.; Fedele, F.; Pandian, N.G. Valvular perforation in left-sided infective endocarditis: A prospective echocardiographic evaluation and clinical outcome. Am. Heart J. 1997, 134, 656–664. [Google Scholar] [CrossRef]
- Larson, S.R.; Pieper, J.A.; Hulten, E.A.; Ficaro, E.P.; Corbett, J.R.; Murthy, V.L.; Weinberg, R.L. Characterization of a highly effective preparation for suppression of myocardial glucose utilization. J. Nucl. Cardiol. 2020, 27, 849–861. [Google Scholar] [CrossRef]
- Scholtens, A.M.; Swart, L.E.; Verberne, H.J.; Tanis, W.; Lam, M.G.; Budde, R.P. Confounders in FDG-PET/CT Imaging of Suspected Prosthetic Valve Endocarditis. JACC Cardiovasc Imaging 2016, 9, 1462–1465. [Google Scholar] [CrossRef]
- Scholtens, A.M.; van Aarnhem, E.E.; Budde, R.P. Effect of antibiotics on FDG-PET/CT imaging of prosthetic heart valve endocarditis. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1223. [Google Scholar] [CrossRef] [Green Version]
- Vos, F.J.; Bleeker-Rovers, C.P.; Kullberg, B.J.; Adang, E.M.; Oyen, W.J. Cost-effectiveness of routine (18)F-FDG PET/CT in high-risk patients with gram-positive bacteremia. J. Nucl. Med. 2011, 52, 1673–1678. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | |||||||
|---|---|---|---|---|---|---|---|
| Authors | Year | Country | Study Design | Type of Patients Evaluated | No. of Episodes with Suspicion of IE (NVE) Undergoing 18F-FDG PET/CT | ||
| Abikhzer et al. [17] | 2020 | Canada | Retrospective monocentric | Patients with clinical suspicion of NVE | 54 (54) | ||
| Abou Jokh Casas et al. [18] | 2019 | Spain | Prospective monocentric | Patients with clinical suspicion of IE, including a subgroup of patients with suspicion of NVE | 43 (12) | ||
| de Camargo et al. [19] | 2020 | Brazil | Prospective monocentric | Patients with clinical suspicion of IE, including a subgroup of patients with suspicion of NVE | 303 (115) | ||
| Gomes et al. [20] | 2018 | Netherlands | Prospective monocentric | Patients with clinical suspicion of IE, including a subgroup of patients with suspicion of NVE | 176 (27) | ||
| Granados et al. [21] | 2016 | Spain | Prospective monocentric | Patients with clinical suspicion of IE, including a subgroup of patients with suspicion of NVE | 80 (21) | ||
| Kouijzer et al. [22] | 2018 | Netherlands | Retrospective monocentric | Patients with clinical suspicion of NVE | 88 (88) | ||
| Sánchez-Enrique et al. [23] | 2018 | Spain | Prospective monocentric | Patients with clinical suspicion of IE, including a subgroup of patients with suspicion of NVE | 120 (34) | ||
| (b) | |||||||
| Authors | Age (Years) | %Male | Vegetation in TTE/TEE | Positive Blood Cultures | Presence of Fever | Value of CRP | Antibiotic Treatment Prior to the Exam (days) |
| Abikhzer et al. [17] | Mean: 63 ± 15 Range: 33–93 | 64.8% | NR | NR | 37/54 (68.5%) | 78.5 ± 43.2 (0.2–193) | Median duration: 7 (range 1–61 days). |
| Abou Jokh Casas et al. [18] | Median: 71 Range: 25–88 | 88.4% | NR | NR | NR | 76 ± 75 (0–349) | NR |
| de Camargo et al. [19] | Mean: 58 ± 17 | 58% | NR | 40/54 (74%) | 82/115 (71%) | NR | 6 ± 8 (1–62) |
| Gomes et al. [20] | Mean: 64 Range: 18–95 | 60% | 5/27 (19%) | 14/27 (51.8%) | NR | NR | Yes, length not specified |
| Granados et al. [21] | Mean: 68 ± 13 | 81% | NR | NR | NR | NR | Definite IE: 20 (12–30) Possible IE: 13 (8–25) |
| Kouijzer et al. [22] | Mean: 61 Range: 17–90 | 56.8% | 37/88 (42%) | 88/88 (100%) | NR | NR | NR |
| Sánchez-Enrique et al. [23] | NR | NR | NR | NR | NR | NR | NR |
| (a) | |||||
|---|---|---|---|---|---|
| Authors | Hybrid Imaging Modality Name of the Device | Myocardial Suppression of 18F-FDG Uptake | Protocol for Myocardial Suppression of 18F-FDG Uptake | Injection of Heparin (50 UI/Kg) 15 min Prior Injection of 18F-FDG | Mean Injected Activity |
| Abikhzer et al. [17] | PET/CT (with low-dose CT) Biograph mCT Flow 40 with TrueV, Siemens | Yes | Prolonged fasting (at least 12 h), HFLC diet in the 24 h prior injection of 18F-FDG | Yes, when not CI (10 patients excluded) | 370 MBq |
| Abou Jokh Casas et al. [18] | PET/CT (with low-dose CT) NR | Yes | Prolonged fasting (at least 6 h), HFLC diet at in the 12 h prior injection of 18F-FDG | Yes, when not CI | 370 MBq |
| de Camargo et al. [19] | PET/CT (with low-dose CT) Gemini-TF 64-Slice, Philips Medical Systems | Yes | Prolonged fasting (at least 8 h), HFLC diet in the 24 h prior injection of 18F-FDG | NR | 5 MBq/kg |
| Gomes et al. [20] | PET/CT (with low-dose CT) Biograph mCT 64-Slice, Siemens | Yes | Prolonged fasting (at least 6 h), HFLC diet in the 24 h prior injection of 18F-FDG | NR | 244 MBq (3 MBq/Kg) |
| Granados et al. [21] | PET/CT (with low-dose CT) Biograph mCT 64-Slice, Siemems | Yes | Prolonged fasting (at least 12 h) | Yes, when not CI | 4 MBq/kg |
| Kouijzer et al. [22] | PET/CT (with low-dose CT) Biograph mCT 40, Siemens | Yes | Prolonged fasting (at least 6 h), HFLC diet in the 24 h prior injection of 18F-FDG | NR | 3.3 MBq/kg |
| Sánchez-Enrique et al. [23] | PET/CT (with low-dose CT) NR | NR | NR | NR | NR |
| (b) | |||||
| Authors | Time Interval between Radiotracer Injection and Image Acquisition | Delayed PET/CT Imaging | Image Interpretation | Visual Criteria for Positive 18F-FDG PET/CT | Semi-Quantitative Analysis |
| Abikhzer et al. [17] | 60 min | in selected cases | 2 experienced physicians, blinded to the patient clinical information | Presence of focally increased 18F-FDG uptake in and around the native heart valve, excluding the papillary muscle | No |
| Abou Jokh Casas et al. [18] | 45 min | NR | 2 experienced physicians, with involvement of a third physician by disagreement | Presence of any increased 18F-FDG uptake in the native heart valve, | SUVmax |
| de Camargo et al. [19] | 60 min | NR | 2 experienced physicians, blinded to the patient clinical information | Presence of focal or heterogeneous 18F-FDG uptake that persisted in the non-corrected images | SUVmax |
| Gomes et al. [20] | 60 min | NR | 2 experienced physicians, blinded to the patient clinical information | Focal/heterogeneous 18F-FDG uptake, at least greater than uptake in mediastinum | No |
| Granados et al. [21] | 60 min | NR | 2 experienced physicians, with involvement of a third physician by disagreement | Presence of focal or heterogeneous 18F-FDG uptake that persisted in the non-corrected images | SUVmax |
| Kouijzer et al. [22] | 60 min | NR | 2 experienced physicians, blinded to the patient clinical information | Presence of any increased 18F-FDG uptake in and around the native heart valve, distinguishable from normal heart uptake | No |
| Sánchez-Enrique et al. [23] | NR | NR | NR | Presence of focal or heterogeneous 18F-FDG uptake that persisted in the non-corrected images | No |
| (a) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Authors. | Reference Standard for Diagnostic Performance Assessment | True Positive | False Positive | True Negative | False Negative | Sensitivity | Specificity | ||
| Abikhzer et al. [17] | histological analysis of valve tissue or mDC and decision of MET taking into account clinical, imaging, and microbiological findings. 18F-FDG PET/CT excluded from the final decision | 21 | 0 | 23 | 10 | 67.7% | 100% | ||
| Abou Jokh Casas et al. [18] | mDC determined by MET. 18F-FDG PET/CT excluded from the final decision | 2 | 0 | 6 | 4 | 33.3% | 100% | ||
| de Camargo et al. [19] | microbiological and histological analysis of valve tissue or modified Duke criteria determined by MET. 18F-FDG PET/CT excluded from the final decision | 10 | 0 | 69 | 36 | 22% | 100% | ||
| Gomes et al. [20] | mDC and decision of MET taking into account clinical, imaging, and microbiological findings. 18F-FDG PET/CT included in the final decision | 2 | 0 | 20 | 5 | 28.6% | 100% | ||
| Granados et al. [21] | mDC and decision of MET taking into account clinical, imaging, and microbiological findings. 18F-FDG PET/CT included in the final decision | 0 | 0 | 15 | 6 | 0% | 100% | ||
| Kouijzer et al. [22] | mDC and decision of MET taking into account clinical, imaging, and microbiological findings. 18F-FDG PET/CT included in the final decision | 9 | 2 | 66 | 11 | 45% | 97.1% | ||
| Sánchez-Enrique et al. [23] | histological analysis of valve tissue or mDC and decision of MET taking into account clinical, imaging, and microbiological findings. 18F-FDG PET/CT included in the final decision | 10 | 2 | 11 | 11 | 47.6% | 84.6% | ||
| (b) | |||||||||
| Authors | PPV | NPV | Diagnostic Accuracy | Metastatic Foci | Alternative Diagnosis/ Foci for Infection | Most Common Microbiological Findings | |||
| Abikhzer et al. [17] | 100% | 69.7% | 81.5% | 45.1% | 5 (21.7%) | NR | |||
| Abou Jokh Casas et al. [18] | 100% | 60% | 66.7% | NR | NR | 1. Staph. epidermidis/ 2. Staph. aureus / 3. Strepto. bovis | |||
| de Camargo et al. [19] | 100% | 66% | 68.7% | Identified in 47 patients with final diagnosis, but not specifically reported for NVE cases | Identified in 29 patients with excluded IE, but not specifically reported for NVE cases | 1. Strepto. sp. / 2. Staph. aureus / 3. Entero. sp. | |||
| Gomes et al. [20] | 100% | 80% | 81.5% | Identified in 6 patients with final diagnosis, but not specifically reported for NVE cases | Identified in 94% of patients with excluded IE, but not specifically reported for NVE cases | 1. Staph. aureus / 2. Staph. others groups / 3. T. Whippeli | |||
| Granados et al. [21] | NR | 71.4% | 71.4% | Identified in 8 patients with final diagnosis, but not specifically reported for NVE cases | 7 (45%) | Staph. aureus | |||
| Kouijzer et al. [22] | 81.8% | 85.7% | 85.2% | Identified in 54.5% of patients with final diagnosis | NR | 1. Staph. aureus / 2. Strepto. sp. / 3. Entero. sp. | |||
| Sánchez-Enrique et al. [23] | 83.3% | 50% | 61.8% | NR | NR | NR | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamani, C.H.; Allenbach, G.; Jreige, M.; Pavon, A.G.; Meyer, M.; Testart, N.; Firsova, M.; Fernandes Vieira, V.; Boughdad, S.; Nicod Lalonde, M.; et al. Diagnostic Performance of 18F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis. Diagnostics 2020, 10, 754. https://doi.org/10.3390/diagnostics10100754
Kamani CH, Allenbach G, Jreige M, Pavon AG, Meyer M, Testart N, Firsova M, Fernandes Vieira V, Boughdad S, Nicod Lalonde M, et al. Diagnostic Performance of 18F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis. Diagnostics. 2020; 10(10):754. https://doi.org/10.3390/diagnostics10100754
Chicago/Turabian StyleKamani, Christel H., Gilles Allenbach, Mario Jreige, Anna G. Pavon, Marie Meyer, Nathalie Testart, Maria Firsova, Victor Fernandes Vieira, Sarah Boughdad, Marie Nicod Lalonde, and et al. 2020. "Diagnostic Performance of 18F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis" Diagnostics 10, no. 10: 754. https://doi.org/10.3390/diagnostics10100754
APA StyleKamani, C. H., Allenbach, G., Jreige, M., Pavon, A. G., Meyer, M., Testart, N., Firsova, M., Fernandes Vieira, V., Boughdad, S., Nicod Lalonde, M., Schaefer, N., Guery, B., Monney, P., Prior, J. O., & Treglia, G. (2020). Diagnostic Performance of 18F-FDG PET/CT in Native Valve Endocarditis: Systematic Review and Bivariate Meta-Analysis. Diagnostics, 10(10), 754. https://doi.org/10.3390/diagnostics10100754