Use of Liquid-based Cytology and Cell Block Combined Technique for an Accurate Diagnosis of Oral Diffuse Large B Cell Lymphoma: A Case Report

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
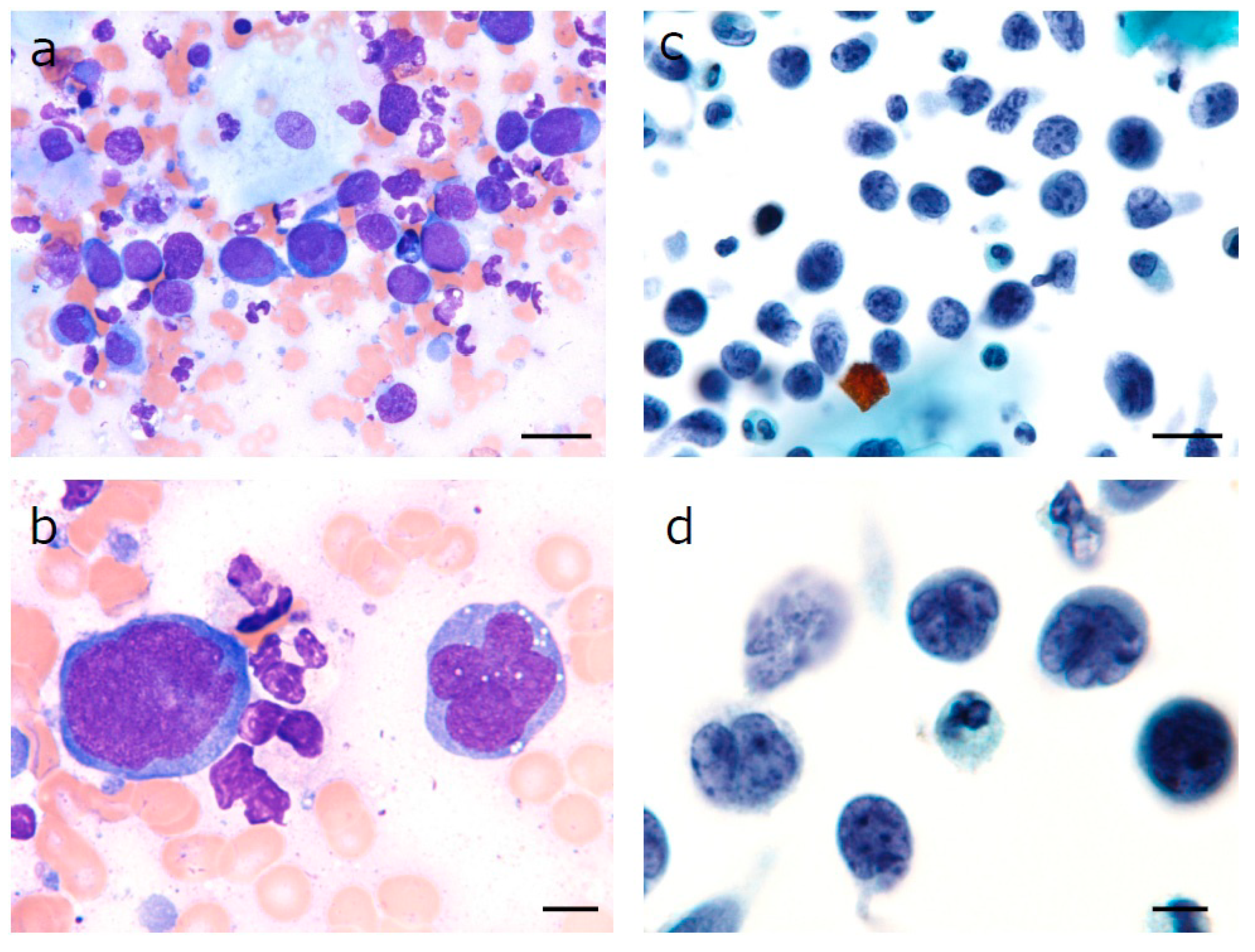
2.1. Sample Collection and Liquid-Based Cytology
2.2. Preparation of Cell Blocks
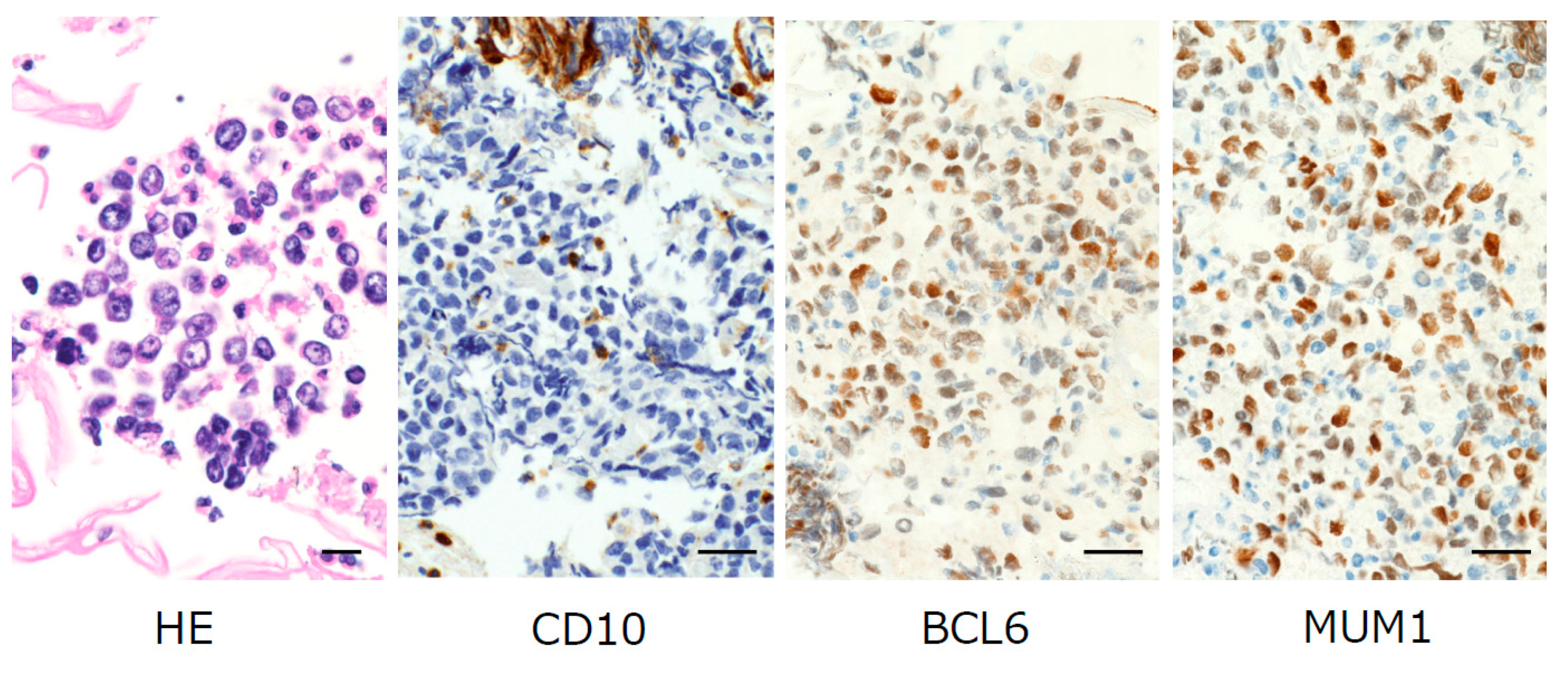
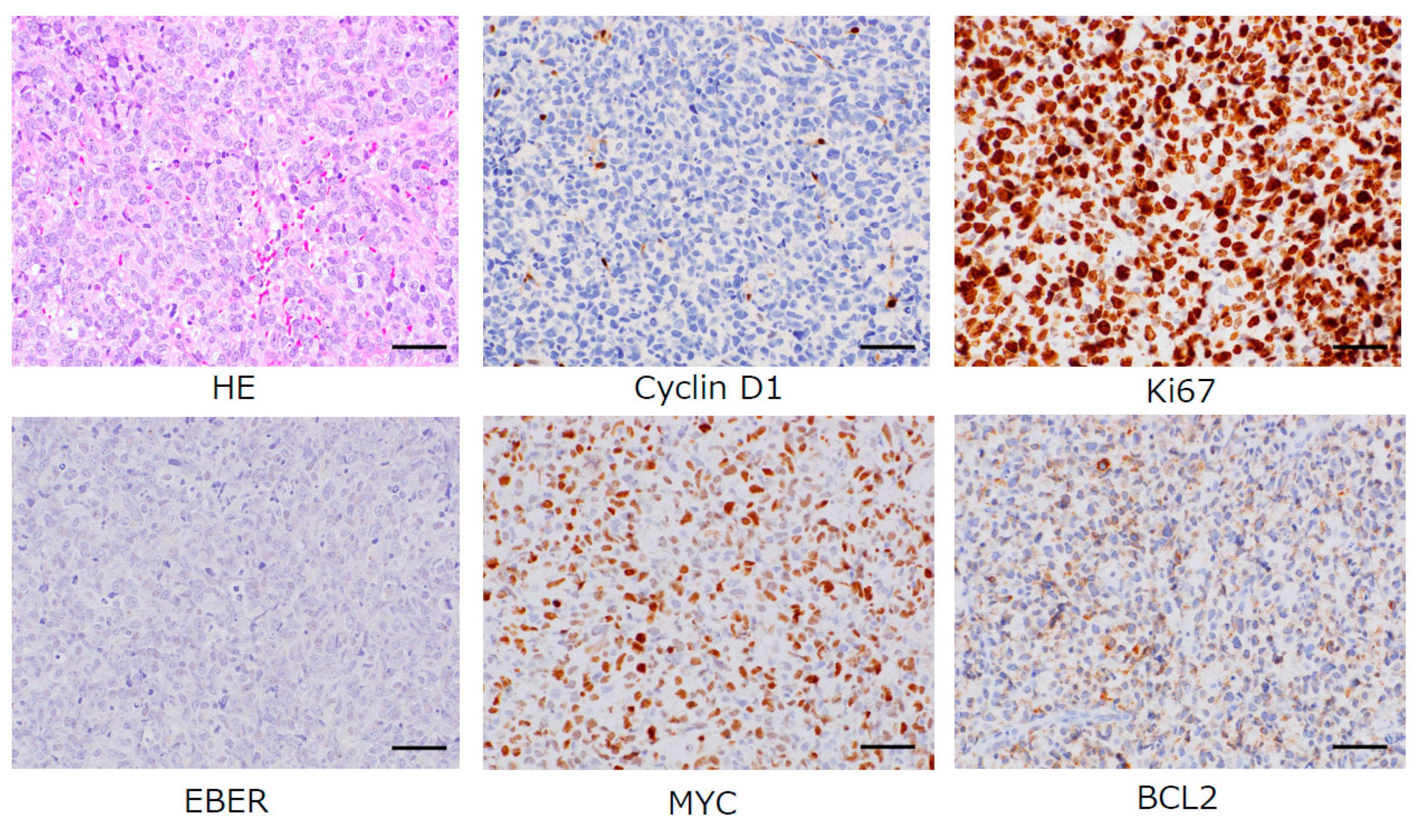
2.3. Immunocytochemical Staining
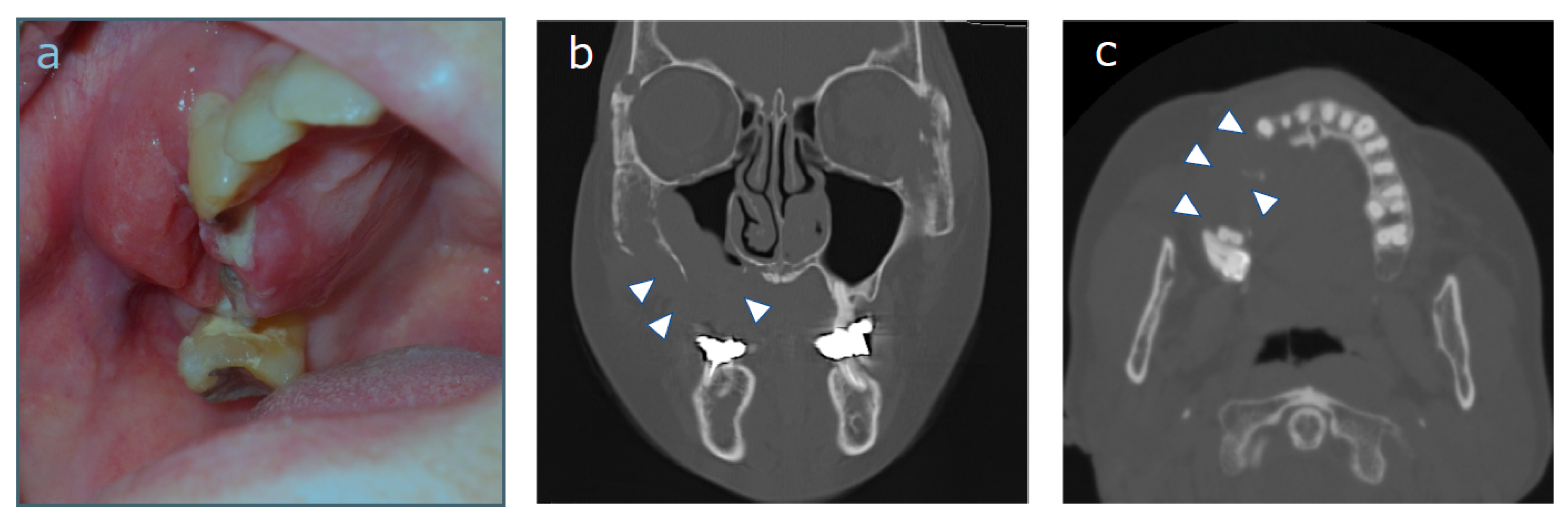
2.4. Case Description
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beham-Schmid, C. Aggressive lymphoma 2016: Revision of the WHO classification. Memo 2017, 10, 248–254. [Google Scholar] [CrossRef]
- Vannata, B.; Zucca, E. Primary extranodal B-cell lymphoma: Current concepts and treatment strategies. Chin. Clin. Oncol. 2015, 4, 10. [Google Scholar]
- Haixiao, Z.; Haili, Y.; Yuan, Z.; Lang, L.; Li, S. Primary diffuse large B-cell lymphoma in the maxilla: A case report. Medicine 2018, 97, e10707. [Google Scholar]
- Bhattacharyya, I.; Chehal, H.K.; Cohen, D.M.; AI-Quran, S.Z. Primary diffuse large B-cell lymphoma of the oral cavity: Germinal center classification. Head Neck Pathol. 2010, 4, 181–191. [Google Scholar] [CrossRef]
- Pereira, D.L.; Fernandes, D.T.; Santos-Silva, A.R.; Vargas, P.A.; Almeida, O.P.; Lopes, M.A. Intraosseous Non-Hodgkin lymphoma mimicking a periapical lesion. J. Endod. 2015, 41, 1738–1742. [Google Scholar] [CrossRef]
- Akamatsu, S.; Kodama, S.; Himeji, Y.; Ikuta, N.; Shimagaki, N. A comparison of liquid-based cytology with conventional cytology in cervical cancer screening. Acta Cytol. 2012, 56, 370–374. [Google Scholar] [CrossRef]
- Mehrotra, R. The role of cytology in oral lesions: A review of recent improvements. Diagn. Cytopathol. 2011, 40, 73–83. [Google Scholar] [CrossRef]
- Navone, R.; Burlo, P.; Pich, A.; Pentrnero, M.; Broccoletti, R.; Marsico, A.; Gandolfo, S. The impact of liquid-based oral cytology on the diagnosis of oral squamous dysplasia and carcinoma. Cytopathology 2007, 18, 356–360. [Google Scholar] [CrossRef]
- Desai, K.M.; Angadi, P.V.; Kale, A.D.; Hallikerimath, S. Assessment of cell block technique in head and neck pathology diagnoses: A preliminary study. Diagn. Cytopathol. 2019, 47, 445–451. [Google Scholar] [CrossRef]
- Shidham, V.B. CellBlockistry: Science of cell-block making as ancillary cytopathology component in the era of minimally invasive techniques with increasing role of molecular pathology. Clin. Surg. 2019, 4, 2510. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshino, A.; Ishida, S.; Nakamura, S.; Kita, R.; Seto, M.; Matsumoto, S.; Takeshita, M.; Kondo, S. Use of Liquid-based Cytology and Cell Block Combined Technique for an Accurate Diagnosis of Oral Diffuse Large B Cell Lymphoma: A Case Report. Diagnostics 2020, 10, 823. https://doi.org/10.3390/diagnostics10100823
Yoshino A, Ishida S, Nakamura S, Kita R, Seto M, Matsumoto S, Takeshita M, Kondo S. Use of Liquid-based Cytology and Cell Block Combined Technique for an Accurate Diagnosis of Oral Diffuse Large B Cell Lymphoma: A Case Report. Diagnostics. 2020; 10(10):823. https://doi.org/10.3390/diagnostics10100823
Chicago/Turabian StyleYoshino, Aya, Shintaro Ishida, Shinsuke Nakamura, Ryosuke Kita, Mika Seto, Shinji Matsumoto, Morishige Takeshita, and Seiji Kondo. 2020. "Use of Liquid-based Cytology and Cell Block Combined Technique for an Accurate Diagnosis of Oral Diffuse Large B Cell Lymphoma: A Case Report" Diagnostics 10, no. 10: 823. https://doi.org/10.3390/diagnostics10100823
APA StyleYoshino, A., Ishida, S., Nakamura, S., Kita, R., Seto, M., Matsumoto, S., Takeshita, M., & Kondo, S. (2020). Use of Liquid-based Cytology and Cell Block Combined Technique for an Accurate Diagnosis of Oral Diffuse Large B Cell Lymphoma: A Case Report. Diagnostics, 10(10), 823. https://doi.org/10.3390/diagnostics10100823