
The Effect of Caffeine on Heart Rate Variability in Newborns: A Pilot Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
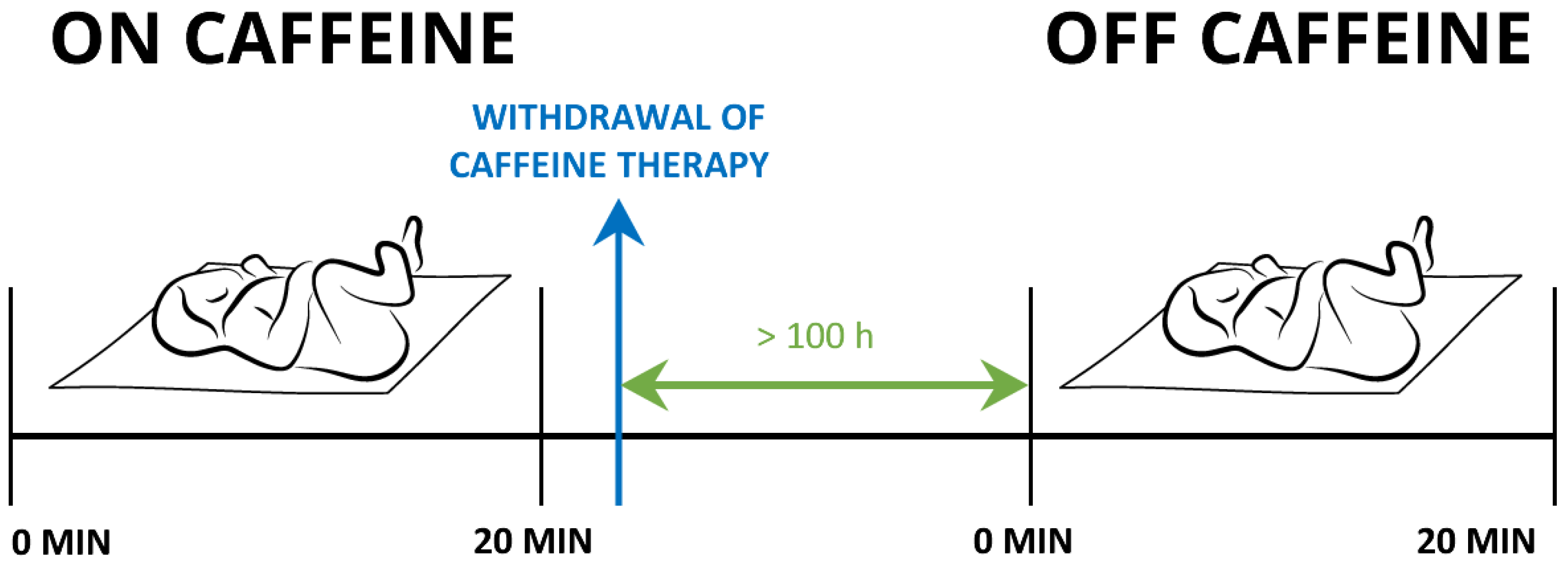
2.2. Study Setting
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. The Effect of Caffeine on the Heart Rate, Breathing Frequency, Arterial Oxygen Saturation and Body Temperature
3.2. The Effect of Caffeine on HRV
3.3. The Correlation between Postmenstrual Age and the Parameters of HRV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ulanovsky, I.; Haleluya, N.S.; Blazer, S.; Weissman, A. The Effects of Caffeine on Heart Rate Variability in Newborns with Apnea of Prematurity. J. Perinatol. 2014, 34, 620–623. [Google Scholar] [CrossRef]
- Synnes, A.; Grunau, R.E. Neurodevelopmental Outcomes after Neonatal Caffeine Therapy. Semin. Fetal Neonatal Med. 2020, 25, 101160. [Google Scholar] [CrossRef] [PubMed]
- Long, J.-Y.; Guo, H.-L.; He, X.; Hu, Y.-H.; Xia, Y.; Cheng, R.; Ding, X.-S.; Chen, F.; Xu, J. Caffeine for the Pharmacological Treatment of Apnea of Prematurity in the NICU: Dose Selection Conundrum, Therapeutic Drug Monitoring and Genetic Factors. Front. Pharmacol. 2021, 12, 681842. [Google Scholar] [CrossRef]
- Echeverri, D.; Montes, F.R.; Cabrera, M.; Galán, A.; Prieto, A. Caffeine’s Vascular Mechanisms of Action. Int. J. Vasc. Med. 2010, 2010, 834060. [Google Scholar] [CrossRef] [PubMed]
- Faudone, G.; Arifi, S.; Merk, D. The Medicinal Chemistry of Caffeine. J. Med. Chem. 2021, 64, 7156–7178. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Feely, J. Acute Effect of Caffeine on Arterial Stiffness and Aortic Pressure Waveform. Hypertension 2001, 38, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Early Caffeine in Preterm Neonates. Available online: https://clinicaltrials.gov/ct2/show/NCT03086473 (accessed on 28 March 2023).
- Shrestha, B.; Jawa, G. Caffeine Citrate—Is It a Silver Bullet in Neonatology? Pediatr. Neonatol. 2017, 58, 391–397. [Google Scholar] [CrossRef]
- Huvanandana, J.; Thamrin, C.; McEwan, A.L.; Hinder, M.; Tracy, M.B. Cardiovascular Impact of Intravenous Caffeine in Preterm Infants. Acta Paediatr. 2019, 108, 423–429. [Google Scholar] [CrossRef]
- Natarajan, G.; Lopes, J.M.; Aranda, J.V. Pharmacologic Treatment of Neonatal Apnea. In Neonatal and Pediatric Pharmacology: Therapeutic Principles in Practice, 4th ed.; Yaffe, S.J., Aranda, J.V., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; Chapter 20; pp. 241–251. [Google Scholar]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart Rate Variability: Standards of Measurement, Physiological Interpretation and Clinical Use. Circulation 1996, 93, 1043–1065. [CrossRef]
- ChuDuc, H.; NguyenPhan, K.; NguyenViet, D. A Review of Heart Rate Variability and Its Applications. APCBEE Procedia 2013, 7, 80–85. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T.J.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart Rate Variability: Origins, Methods, and Interpretive Caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The LF/HF Ratio Does Not Accurately Measure Cardiac Sympatho-Vagal Balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef]
- Reyes del Paso, G.A.; Langewitz, W.; Mulder, L.J.M.; van Roon, A.; Duschek, S. The Utility of Low Frequency Heart Rate Variability as an Index of Sympathetic Cardiac Tone: A Review with Emphasis on a Reanalysis of Previous Studies. Psychophysiology 2013, 50, 477–487. [Google Scholar] [CrossRef]
- Billman, G.E. Heart Rate Variability—A Historical Perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef]
- Soares-Miranda, L.; Sattelmair, J.; Chaves, P.; Duncan, G.E.; Siscovick, D.S.; Stein, P.K.; Mozaffarian, D. Physical Activity and Heart Rate Variability in Older Adults: The Cardiovascular Health Study. Circulation 2014, 129, 2100–2110. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Mangiulli, M.; Perrotta, A.M.; Di Lazzaro Giraldi, G.; Testorio, M.; Rosato, E.; Cianci, R.; Gigante, A. Reduction in Heart Rate Variability in Autosomal Dominant Polycystic Kidney Disease. Kidney Blood Press. Res. 2019, 44, 1142–1148. [Google Scholar] [CrossRef]
- Draghici, A.E.; Taylor, J.A. The Physiological Basis and Measurement of Heart Rate Variability in Humans. J. Physiol. Anthropol. 2016, 35, 22. [Google Scholar] [CrossRef]
- Tuzcu, V.; Nas, S.; Ulusar, U.; Ugur, A.; Kaiser, J.R. Altered Heart Rhythm Dynamics in Very Low Birth Weight Infants with Impending Intraventricular Hemorrhage. Pediatrics 2009, 123, 810–815. [Google Scholar] [CrossRef]
- Israeli-Mendlovic, H.; Mendlovic, J.; Zuk, L.; Katz-Leurer, M. Reproducibility of 24-h Heart Rate Variability Measures in Preterm Infants Born at 28–32 weeks of Gestation. Early Hum. Dev. 2020, 148, 105117. [Google Scholar] [CrossRef] [PubMed]
- Javorka, K.; Lehotska, Z.; Kozar, M.; Uhrikova, Z.; Kolarovszki, B.; Javorka, M.; Zibolen, M. Heart Rate Variability in Newborns. Physiol. Res. 2017, 66, S203–S214. [Google Scholar] [CrossRef]
- Selig, F.A.; Tonolli, E.R.; da Silva, É.V.C.M.; de Godoy, M.F. Heart Rate Variability in Preterm and Term Neonates. Arq. Bras. Cardiol. 2011, 96, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Yiallourou, S.R.; Witcombe, N.B.; Sands, S.A.; Walker, A.M.; Horne, R.S.C. The Development of Autonomic Cardiovascular Control Is Altered by Preterm Birth. Early Hum. Dev. 2013, 89, 145–152. [Google Scholar] [CrossRef]
- Takatani, T.; Takahashi, Y.; Yoshida, R.; Imai, R.; Uchiike, T.; Yamazaki, M.; Shima, M.; Nishikubo, T.; Ikada, Y.; Fujimoto, S. Relationship between Frequency Spectrum of Heart Rate Variability and Autonomic Nervous Activities during Sleep in Newborns. Brain Dev. 2018, 40, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Iyer, K.K.; Leitner, U.; Giordano, V.; Roberts, J.A.; Vanhatalo, S.; Klebermass-Schrehof, K.; Stevenson, N.J. Bedside Tracking of Functional Autonomic Age in Preterm Infants. Pediatr. Res. 2022. [Google Scholar] [CrossRef]
- Cardoso, S.; Silva, M.J.; Guimarães, H. Autonomic Nervous System in Newborns: A Review Based on Heart Rate Variability. Child’s Nerv. Syst. 2017, 33, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, R.; Campbell, K.; Hunse, C.; Patrick, J. Patterns of Human Fetal Heart Rate Accelerations from 26 Weeks to Term. Am. J. Obstet. Gynecol. 1987, 157, 743–748. [Google Scholar] [CrossRef]
- Engle, W.A. Age Terminology during the Perinatal Period. Pediatrics 2004, 114, 1362–1364. [Google Scholar] [CrossRef]
- Fister, P.; Nolimal, M.; Lenasi, H.; Klemenc, M. The Effect of Sleeping Position on Heart Rate Variability in Newborns. BMC Pediatr. 2020, 20, 156. [Google Scholar] [CrossRef]
- Monda, M.; Viggiano, A.; Vicidomini, C.; Viggiano, A.; Iannaccone, T.; Tafuri, D.; De Luca, B. Espresso Coffee Increases Parasympathetic Activity in Young, Healthy People. Nutr. Neurosci. 2009, 12, 43–48. [Google Scholar] [CrossRef]
- Notarius, C.F.; Floras, J.S. Caffeine Enhances Heart Rate Variability in Middle-Aged Healthy, but Not Heart Failure Subjects. J. Caffeine Res. 2012, 2, 77–82. [Google Scholar] [CrossRef]
- Dömötör, Z.; Szemerszky, R.; Köteles, F. Subjective and Objective Effects of Coffee Consumption—Caffeine or Expectations? Acta Physiol. Hung. 2015, 102, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Yeragani, V.K.; Krishnan, S.; Engels, H.J.; Gretebeck, R. Effects of Caffeine on Linear and Nonlinear Measures of Heart Rate Variability before and after Exercise. Depress. Anxiety 2005, 21, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Eichenwald, E.C. Apnea of Prematurity. Pediatrics 2016, 137, e20153757. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Hady, H.; Nasef, N.; Shabaan, A.E.; Nour, I. Caffeine Therapy in Preterm Infants. World J. Clin. Pediatr. 2015, 4, 81–93. [Google Scholar] [CrossRef]
- Prechtl, H.F. The Behavioural States of the Newborn Infant (a Review). Brain Res. 1974, 76, 185–212. [Google Scholar] [CrossRef]
- Davies, P.; Maconochie, I. The Relationship between Body Temperature, Heart Rate and Respiratory Rate in Children. Emerg. Med. J. 2009, 26, 641–643. [Google Scholar] [CrossRef]
- Koskela, J.K.; Tahvanainen, A.; Haring, A.; Tikkakoski, A.J.; Ilveskoski, E.; Viitala, J.; Leskinen, M.H.; Lehtimäki, T.; Kähönen, M.A.; Kööbi, T.; et al. Association of Resting Heart Rate with Cardiovascular Function: A Cross-Sectional Study in 522 Finnish Subjects. BMC Cardiovasc. Disord. 2013, 13, 102. [Google Scholar] [CrossRef]
- Ainsworth, S.B. Drugs and the Body. In Neonatal Formulary 7: Drug Use in Pregnancy and the First Year of Life; John Wiley & Sons Inc.: Chichester, UK, 2015; pp. 12–13. [Google Scholar]
- Latremouille, S.; Lam, J.; Shalish, W.; Sant’Anna, G. Neonatal Heart Rate Variability: A Contemporary Scoping Review of Analysis Methods and Clinical Applications. BMJ Open 2021, 11, e055209. [Google Scholar] [CrossRef]
- Koenig, J.; Jarczok, M.N.; Kuhn, W.; Morsch, K.; Schäfer, A.; Hillecke, T.K.; Thayer, J.F. Impact of Caffeine on Heart Rate Variability: A Systematic Review. J. Caffeine Res. 2013, 3, 22–37. [Google Scholar] [CrossRef]
- Jenni, O.J.; Carskadon, M.A. Infants to Adolescents. In SRS Basics of Sleep Guide; Opp, M.R., Ed.; Sleep Research Society: Westchester, IL, USA, 2005; pp. 11–20. [Google Scholar]
- Anders, T.F.; Sadeh, A.; Appareddy, V. Normal Sleep in Neonates and Children. In Principles and Practice of Sleep Medicine in the Child; Ferber, R., Kryger, M., Eds.; W. B. Saunders: Philadelphia, PA, USA, 1995; pp. 7–18. [Google Scholar]
- Sahni, R.; Schulze, K.F.; Kashyap, S.; Ohira-Kist, K.; Myers, M.M.; Fifer, W.P. Body Position, Sleep States, and Cardiorespiratory Activity in Developing Low Birth Weight Infants. Early Hum. Dev. 1999, 54, 197–206. [Google Scholar] [CrossRef]
- Karemaker, J.M. An Introduction into Autonomic Nervous Function. Physiol. Meas. 2017, 38, R89–R118. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.; Davidson, D.; Katz, S.; Varela, M.; Demeglio, D.; DeCristofaro, J. Apnea of Prematurity and Caffeine Pharmacokinetics: Potential Impact on Hospital Discharge. J. Perinatol. 2016, 36, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Aranda, J.V.; Beharry, K.D. Pharmacokinetics, Pharmacodynamics and Metabolism of Caffeine in Newborns. Semin. Fetal Neonatal Med. 2020, 25, 101183. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| At Birth | Measurement at the Time of Loading Dose of Caffeine | Measurement While on Maintenance Dose of Caffeine | Measurement While off Caffeine | |
|---|---|---|---|---|
| Postmenstrual age (weeks) | 34 ± 5 | 37 ± 4 | 37 ± 3 | 37 ± 2 |
| Body mass (g) | 2353 ± 914 | 2659 ± 676 | 2786 ± 560 | 2745 ± 512 |
| Head circumference (cm) | 31 ± 4 | 33 ± 3 | 34 ± 2 | 34 ± 3 |
| Caffeine dose (mg/kg BM/day) | 9.84 (5.65–9.93) | 2.55 (2.31–2.67) | ||
| Apgar score 1 min | 8.0 (7.5–9.0) | |||
| Apgar score 5 min | 9.0 (7.0–9.0) | |||
| Body length (cm) | 46 ± 7 |
| HR (Beats/min) | BF (Breaths/min) | SaO2 (%) | T (°C) | |||||
|---|---|---|---|---|---|---|---|---|
| p | p | p | p | |||||
| On caffeine | 138.6 ± 12.0 | 1 | 56.2 ± 12.5 | 0.023 * | 99 (97–100) | 0.477 | 36.7 ± 0.4 | 0.332 |
| Off caffeine | 138.6 ± 13.1 | 50.7 ± 13.2 | 99 (97–100) | 36.8 ± 0.3 | ||||
| TP (ms2) | LF (ms2) | LFnu | HF (ms2) | HFnu | LF/HF | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | p | p | p | p | p | |||||||
| On caffeine | 522 (286–1399) | 0.653 | 219 (99–357) | 0.435 | 63.9 (54.5–72.2) | 0.868 | 107 (66–272) | 0.523 | 36.1 (27.1–43.1) | 0.619 | 1.8 (1.3–2.7) | 0.877 |
| Off caffeine | 732 (228–1270) | 232 (85–598) | 69.1 (52.8–73) | 145 (57–268) | 30.9 (27–47.2) | 2.2 (1.1–2.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenasi, H.; Rihar, E.; Filipič, J.; Klemenc, M.; Fister, P. The Effect of Caffeine on Heart Rate Variability in Newborns: A Pilot Study. Life 2023, 13, 1459. https://doi.org/10.3390/life13071459
Lenasi H, Rihar E, Filipič J, Klemenc M, Fister P. The Effect of Caffeine on Heart Rate Variability in Newborns: A Pilot Study. Life. 2023; 13(7):1459. https://doi.org/10.3390/life13071459
Chicago/Turabian StyleLenasi, Helena, Eva Rihar, Jerneja Filipič, Matjaž Klemenc, and Petja Fister. 2023. "The Effect of Caffeine on Heart Rate Variability in Newborns: A Pilot Study" Life 13, no. 7: 1459. https://doi.org/10.3390/life13071459
APA StyleLenasi, H., Rihar, E., Filipič, J., Klemenc, M., & Fister, P. (2023). The Effect of Caffeine on Heart Rate Variability in Newborns: A Pilot Study. Life, 13(7), 1459. https://doi.org/10.3390/life13071459