
Association of Nonalcoholic Hepatic Fibrosis with Body Composition in Female and Male Psoriasis Patients

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
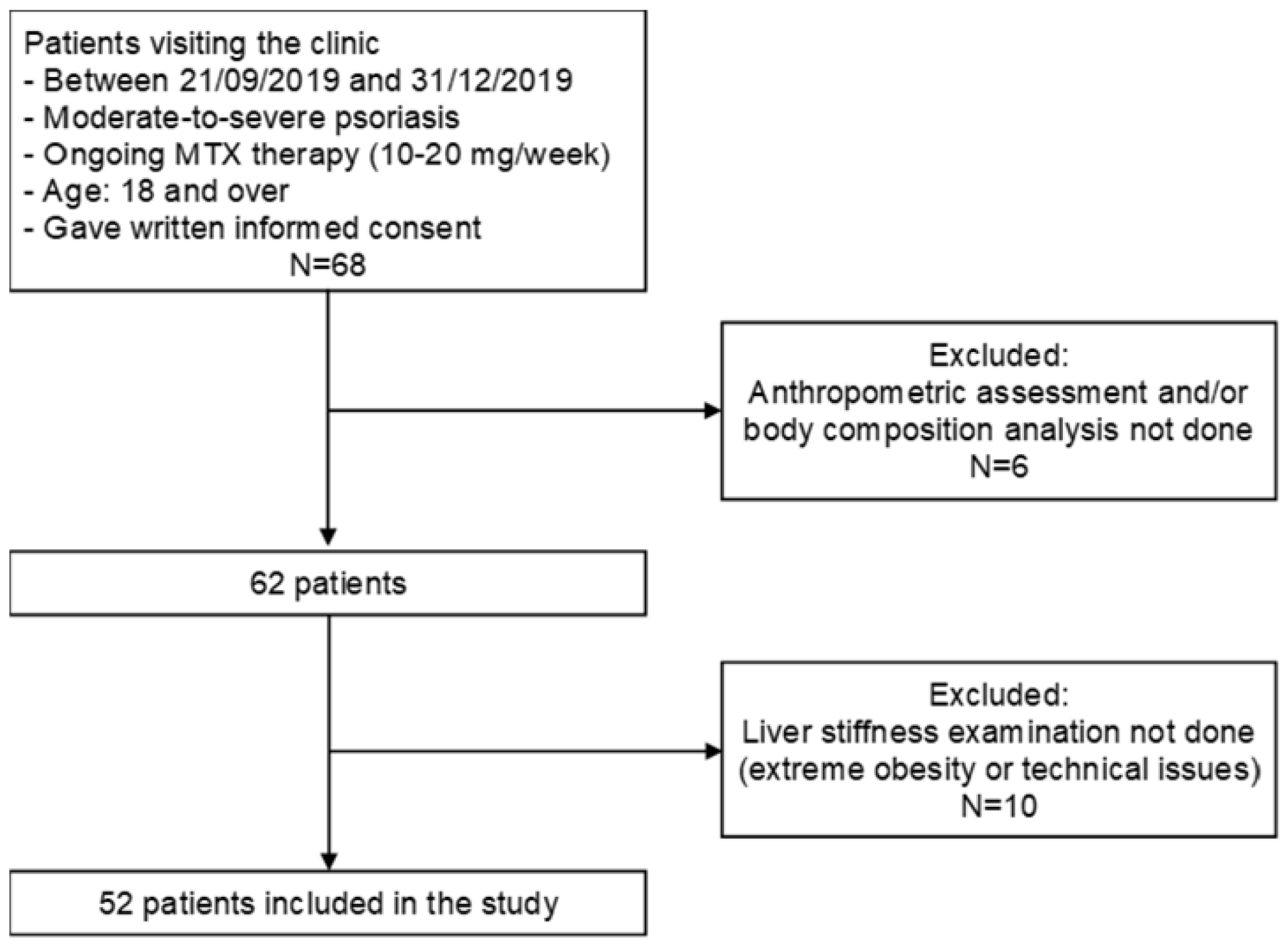
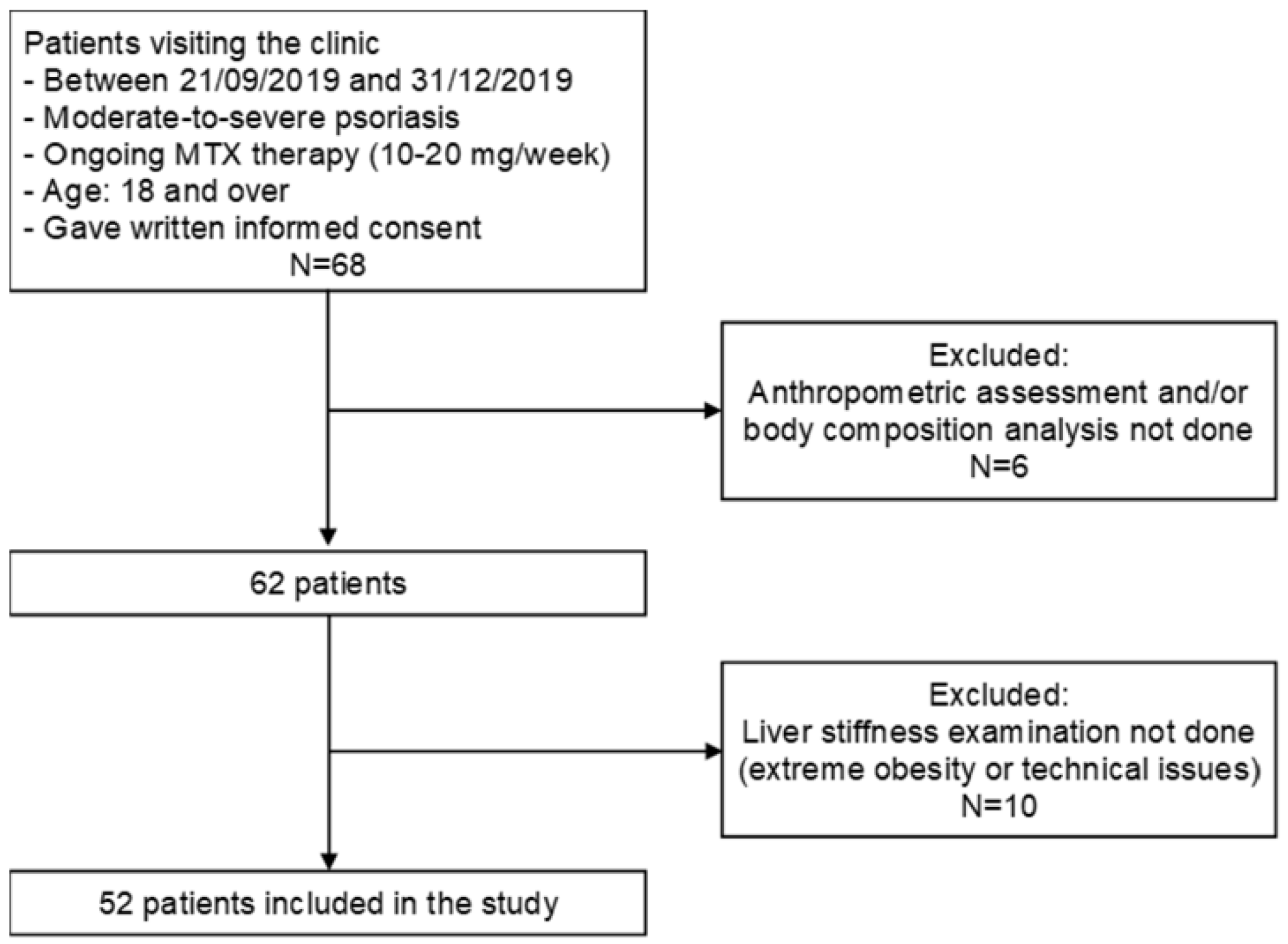
2.1. Patients
2.2. Anthropometric Assessment and Body Composition Analysis
2.3. Liver Fibrosis Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics, Anthropometric Assessment, and Body Composition Analysis
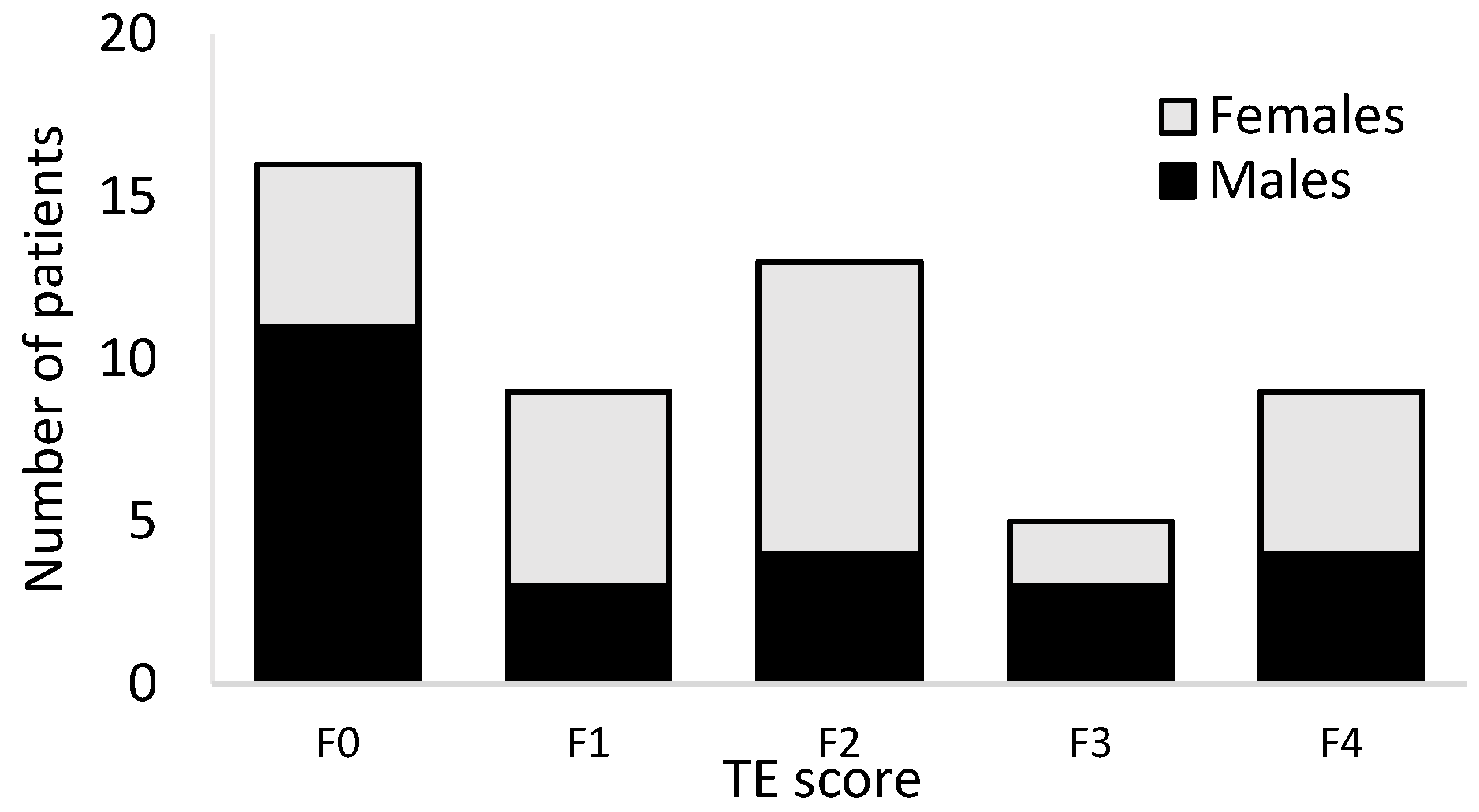
3.2. Liver Fibrosis Evaluation
3.3. Correlation of Liver Fibrosis and Cumulative Methotrexate Dose, Body Mass Index and Body Composition Values
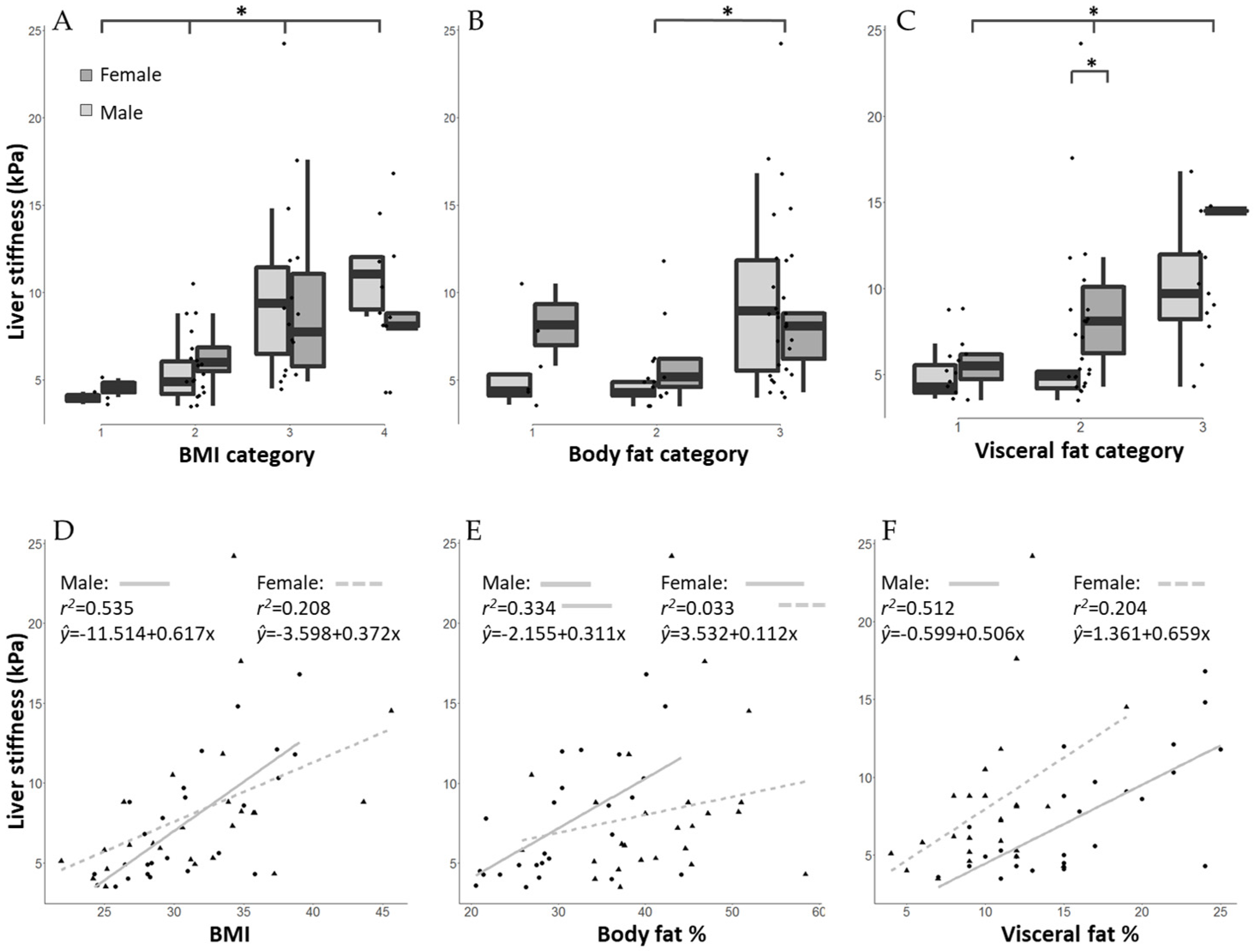
3.4. Gender-Specific Differences in the Association of Liver Fibrosis Scores with Body Mass Index and Body Composition Values
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rousset, L.; Halioua, B. Stress and psoriasis. Int. J. Dermatol. 2018, 57, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Svanström, C.; Lonne-Rahm, S.B.; Nordlind, K. Psoriasis and alcohol. Psoriasis 2019, 9, 75–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Wu, R.; Kong, Y.; Zhao, M.; Su, Y. Impact of smoking on psoriasis risk and treatment efficacy: A meta-analysis. J. Int. Med. Res. 2020, 48, 0300060520964024. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Megna, M.; Cacciapuoti, S.; Frias-Toral, E.; Fabbrocini, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Very low-calorie ketogenic diet (VLCKD) in patients with psoriasis and obesity: An update for dermatologists and nutritionists. Crit. Rev. Food Sci. Nutr. 2020, 24, 1–17. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Annunziata, G.; Megna, M.; Falco, A.; Balato, A.; Colao, A.; Savastano, S. Coffee consumption, metabolic syndrome and clinical severity of psoriasis: Good or bad stuff? Arch. Toxicol. 2018, 92, 1831–1845. [Google Scholar] [CrossRef]
- Barrea, L.; Savanelli, M.C.; Di Somma, C.; Napolitano, M.; Megna, M.; Colao, A.; Savastano, S. Vitamin D and its role in psoriasis: An overview of the dermatologist and nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 195–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Nappi, F.; Di Somma, C.; Savanelli, M.C.; Falco, A.; Balato, A.; Balato, N.; Savastano, S. Environmental Risk Factors in Psoriasis: The Point of View of the Nutritionist. Int. J. Environ. Res. Public Health 2016, 13, 743. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, A.B.; Dann, F. Comorbidities in patients with psoriasis. Am. J. Med. 2009, 122, 1150.e1–1150.e9. [Google Scholar] [CrossRef]
- Duffin, K.C. Identifying and Managing Complications and Comorbidities in Patients with Psoriasis. Semin. Cutan. Med. Surg. 2015, 34, S30–S33. [Google Scholar] [CrossRef]
- Narayanasamy, K.; Sanmarkan, A.D.; Rajendran, K.; Annasamy, C.; Ramalingam, S. Relationship between psoriasis and non-alcoholic fatty liver disease. Prz. Gastroenterol. 2016, 11, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Roberts, K.K.; Cochet, A.E.; Lamb, P.B.; Brown, P.J.; Battafarano, D.F.; Brunt, E.M.; Harrison, S.A. The prevalence of NAFLD and NASH among patients with psoriasis in a tertiary care dermatology and rheumatology clinic. Aliment. Pharmacol. Ther. 2015, 41, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maybury, C.M.; Porter, H.F.; Kloczko, E.; Duckworth, M.; Cotton, A.; Thornberry, K.; Dew, T.; Crook, M.; Natas, S.; Miquel, R.; et al. Prevalence of Advanced Liver Fibrosis in Patients With Severe Psoriasis. JAMA Dermatol. 2019, 155, 1028–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rongngern, P.; Chularojanamontri, L.; Wongpraparut, C.; Silpa-Archa, N.; Chotiyaputta, W.; Pongpaibul, A.; Charatcharoenwitthaya, P. Diagnostic performance of transient elastography for detection of methotrexate-induced liver injury using Roenigk classification in Asian patients with psoriasis: A retrospective study. Arch. Dermatol. Res. 2017, 309, 403–408. [Google Scholar] [CrossRef]
- Talme, T.; Nikamo, P.; Rosenberg, P.; Ståhle, M. Transient Elastography May Improve Detection of Liver Fibrosis in Psoriasis Patients Treated with Methotrexate. Acta Derm.Venereol. 2017, 97, 952–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.S.; Rademaker, M. Monitoring methotrexate-induced liver fibrosis in patients with psoriasis: Utility of transient elastography. Psoriasis 2018, 8, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandpur, S.; Yadav, D.; Jangid, B.; Kumar, A.; Shalimar, N.; Devasenathipathy, K.; Sharma, R.; Gupta, S.D.; Kumar, R.; Kalaivani, M. Ultrasound liver elastography for the detection of liver fibrosis in patients with psoriasis and reactive arthritis on long-term methotrexate therapy: A cross-sectional study. Indian J. Dermatol. Venereol. Leprol. 2020, 86, 508–517. [Google Scholar] [CrossRef]
- Bauer, B.; Chyou, P.H.; Stratman, E.J.; Green, C. Noninvasive Testing for Nonalcoholic Steatohepatitis and Hepatic Fibrosis in Patients With Psoriasis Receiving Long-term Methotrexate Sodium Therapy. JAMA Dermatol. 2017, 153, 977–982. [Google Scholar] [CrossRef]
- Mantovani, A.; Gisondi, P.; Lonardo, A.; Targher, G. Relationship between Non-Alcoholic Fatty Liver Disease and Psoriasis: A Novel Hepato-Dermal Axis? Int. J. Mol. Sci. 2016, 17, 217. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, T.M.; Kim, J.R.; Dummer, R.; Anzengruber, F. A Monocentric, Retrospective Analysis of 61 Patients with Generalized Granuloma Annulare. Dermatology 2020, 236, 369–374. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile And Cut Off Points. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 29 June 2021).
- Gallagher, D.; Heymsfield, S.; Heo, M.; Jebb, S.; Murgatroyd, P.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, T.; Gullick, N.J.; Hutchinson, C.E.; Barber, T.M. Psoriatic disease and body composition: A systematic review and narrative synthesis. PLoS ONE 2020, 15, e0237598. [Google Scholar] [CrossRef] [PubMed]
- Galluzzo, M.; Talamonti, M.; Perino, F.; Servoli, S.; Giordano, D.; Chimenti, S.; De Simone, C.; Peris, K. Bioelectrical impedance analysis to define an excess of body fat: Evaluation in patients with psoriasis. J. Dermatol. Treat. 2017, 28, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Cervoni, J.P.; Alby-Lepresle, B.; Weil, D.; Zhong, P.; Aubin, F.; Wendling, D.; Toussirot, E.; Vuitton, L.; Carbonnel, F.; Blondet, R.; et al. A pragmatic non-invasive assessment of liver fibrosis in patients with psoriasis, rheumatoid arthritis or Crohn’s disease receiving methotrexate therapy. Clin. Res. Hepatol. Gastroenterol. 2020, 44S, 100003. [Google Scholar] [CrossRef]
- Neema, S.; Banerjee, D.; Radhakrishnan, S.; Vasudevan, B.; Sinha, P.; Oberoi, B. Use of Transient Elastography in Detection of Liver Fibrosis in Psoriasis Patients—A Cross-Sectional Study. Indian Dermatol. Online J. 2020, 11, 387–390. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Tobin, A.M.; Hackett, C.B.; Rogers, S.; Collins, P.; Richards, H.L.; O’Shea, D.; Kirby, B. Body mass index, waist circumference and HOMA-IR correlate with the Psoriasis Area and Severity Index in patients with psoriasis receiving phototherapy. Br. J. Dermatol. 2014, 171, 436–438. [Google Scholar] [CrossRef]
- Mahajan, R.; Dogra, S.; Handa, S.; Razmi, T.M.; Narang, T.; Rathi, S.; Dhiman, R.K.; Saikia, B.; Karim, A. Metabolic syndrome and female gender, but not methotrexate, are the important associations of significant liver fibrosis in patients with moderate-to-severe psoriasis as detected by transient elastography. Indian J. Dermatol. Venereol. Leprol. 2020, 86, 649–655. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 52 | Males n = 26 | Females n = 26 | p Value * | |
|---|---|---|---|---|
| Age (years) | 54.0 ± 13.4 | 55.2 ± 13.6 | 52.9 ± 13.2 | 0.537 |
| Body weight (kg) | 91.6 ± 17.7 | 96.7 ±17.0 | 86.4 ± 17.1 | 0.034 |
| BMI (kg/m2) | 31.4 ± 5.1 | 31.1 ± 4.5 | 31.7 ± 5.7 | 0.664 |
| Body fat (%) | 36.3 ± 8.8 | 31.3 ± 7.1 | 41.2 ± 7.6 | 0.001 |
| Body fat categories | ||||
| Low | 0 | 0 | 0 | 0.668 |
| Normal | 6 | 3 | 3 | |
| High | 19 | 8 | 11 | |
| Very high | 27 | 15 | 12 | |
| Weekly MTX dose (mg) | 14.2 ± 2.6 | 14.9 ± 1.9 | 13.5 ± 3.0 | 0.071 |
| Duration of MTX treatment (years) | 4.8 ± 3.0 | 4.5 ± 2.7 | 4.9 ± 3.3 | 0.672 |
| Cumulative MTX dose (mg) | 2273.8 ± 2238.7 | 2284.8 ± 2345.0 | 2262.3 ± 2171.0 | 0.972 |
| BMI Category | Total (n = 52) | Normal (n = 4) | Pre-Obesity (n = 19) | Obese I (n = 17) | Obese II + III (n = 12) | p Value * | |
|---|---|---|---|---|---|---|---|
| Body fat (%) | Total | 36.3 ± 8.8 | 27.6 ± 7.6 | 31.1 ± 6.2 | 39.2 ± 7.7 | 43.2 ± 7.6 | <0.001 |
| Male | 31.3 ± 7.1 | 20.9 ± 0.6 | 28.3 ± 4.5 | 31.8 ± 7.5 | 38.6 ± 3.8 | 0.001 | |
| Female | 41.2 ± 7.6 | 34.1 ± 0.1 | 35.1 ± 6.1 | 43.2 ± 4.2 | 49.7 ± 6.7 | <0.001 | |
| Visceral fat score | Total | 13.3 ± 5.4 | 6.3 ± 2.2 | 10.9 ± 2.9 | 13.3 ± 4.1 | 19.3 ± 5.5 | <0.001 |
| Male | 16.3 ± 5.5 | 8.0 ± 1.4 | 12.6 ± 2.3 | 17.8 ± 3.4 | 23.1 ± 1.9 | <0.001 | |
| Female | 10.2 ± 3.2 | 4.5 ± 0.7 | 8.5 ± 1.6 | 10.9 ± 1.7 | 13.8 ± 3.7 | <0.001 | |
| Muscle mass (%) | Total | 28.0 ± 5.5 | 32.7 ± 6.0 | 30.1 ± 5.9 | 26.7 ± 4.5 | 24.6 ± 3.8 | 0.008 |
| Male | 30.3 ± 4.9 | 37.8 ± 1.2 | 31.9 ± 3.5 | 28.9 ± 6.7 | 26.7 ± 2.1 | 0.015 | |
| Female | 25.6 ± 5.1 | 27.5 ± 1.5 | 27.7 ± 7.8 | 25.4 ± 2.2 | 21.7 ± 3.9 | 0.209 | |
| Liver stiffness value (kPa) | Total | 7.8 ± 4.2 | 4.3 ± 0.6 | 5.8 ± 2.0 | 9.8 ± 5.3 | 9.8 ± 3.9 | 0.001 |
| Male | 7.5 ± 3.8 | 4.0 ± 0.5 | 5.4 ± 1.7 | 9.3 ± 3.9 | 10.7 ± 4.1 | 0.010 | |
| Female | 8.2 ± 4.7 | 4.6 ± 0.8 | 6.4 ± 2.2 | 10.1 ± 6.3 | 8.8 ± 3.7 | 0.159 | |
| R | r2 | B | CI | p Value | ||
|---|---|---|---|---|---|---|
| BMI | Total | 0.565 | 0.319 | 0.467 | 0.269–0.665 | <0.001 |
| Male | 0.731 | 0.535 | 0.617 | 0.369–0.865 | <0.001 | |
| Female | 0.456 | 0.208 | 0.311 | 0.122–0.501 | 0.002 | |
| Body fat% | Total | 0.331 | 0.110 | 0.156 | 0.027–0.285 | 0.019 |
| Male | 0.578 | 0.334 | 0.311 | 0.122–0.501 | 0.002 | |
| Female | 0.187 | 0.033 | 0.112 | −0.149–0.374 | 0.382 | |
| Visceral fat score | Total | 0.427 | 0.182 | 0.347 | 0.134–0.561 | 0.002 |
| Male | 0.716 | 0.512 | 0.506 | 0.293–0.719 | <0.001 | |
| Female | 0.452 | 0.204 | 0.659 | 0.099–1.220 | 0.023 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunner, K.; Oláh, P.; Moezzi, M.; Pár, G.; Vincze, Á.; Breitenbach, Z.; Gyulai, R. Association of Nonalcoholic Hepatic Fibrosis with Body Composition in Female and Male Psoriasis Patients. Life 2021, 11, 763. https://doi.org/10.3390/life11080763
Brunner K, Oláh P, Moezzi M, Pár G, Vincze Á, Breitenbach Z, Gyulai R. Association of Nonalcoholic Hepatic Fibrosis with Body Composition in Female and Male Psoriasis Patients. Life. 2021; 11(8):763. https://doi.org/10.3390/life11080763
Chicago/Turabian StyleBrunner, Kinga, Péter Oláh, Mehdi Moezzi, Gabriella Pár, Áron Vincze, Zita Breitenbach, and Rolland Gyulai. 2021. "Association of Nonalcoholic Hepatic Fibrosis with Body Composition in Female and Male Psoriasis Patients" Life 11, no. 8: 763. https://doi.org/10.3390/life11080763
APA StyleBrunner, K., Oláh, P., Moezzi, M., Pár, G., Vincze, Á., Breitenbach, Z., & Gyulai, R. (2021). Association of Nonalcoholic Hepatic Fibrosis with Body Composition in Female and Male Psoriasis Patients. Life, 11(8), 763. https://doi.org/10.3390/life11080763