

A Qualitative Analysis and Discussion of a New Model for Optimizing Obesity and Associated Comorbidities


Abstract
1. Introduction
2. Model Formulation
- A constant recruitment rate of .
- Obesity dynamics follow the BMI classification.
- Death is due to natural mortality and comorbidity induction.
- Populations are mixing homogeneously.
- 1.
- The parameters and were assumed relative to , with the understanding that progression to more severe obesity stages tends to accelerate as BMI increases. This aligns with findings that individuals in higher obesity classes are more susceptible to further weight gain and associated complications [25].
- 2.
- The treatment rates and were assumed to be lower than , reflecting the clinical observation that weight loss becomes increasingly difficult to achieve and maintain at higher obesity stages. Individuals with more severe obesity often face greater biological and behavioral challenges to effective treatment [26].
- 3.
- A sensitivity analysis was conducted to assess how variations in the estimated parameters affected the model’s behavior. Figures 6–9 and data summarized in Table 5 illustrate that the model remained stable and responsive under changes in these assumptions, supporting the reliability of the results.
3. Key Characteristics of the Proposed Model
3.1. Positivity and Boundedness of the Proposed Model
3.2. Local Stability Analysis of the Obesity-Free Equilibrium State
3.3. Global Stability Analysis of the Obesity-Free Equilibrium State
- 1.
- Local stability conditions indicate that keeping prevention () and treatment () efforts within critical thresholds helps maintain an obesity-free state, reflecting effective public health measures to control obesity progression [28].
- 2.
- These conditions emphasize the need for strong, sustained interventions to counteract natural trends toward weight gain, consistent with evidence that early and continuous efforts are key to preventing obesity [26].
- 3.
- Global stability conditions suggest that even when obesity is widespread, coordinated strategies can restore population health, highlighting critical points where intervention efforts are most effective.
- 4.
- The results also reflect challenges faced by individuals with severe obesity, underscoring the importance of timely and ongoing intervention.
4. Controlling Deviation from the Obesity-Free Equilibrium State
- Lifestyle modifications, e.g., engaging in physical activity and balanced diet. This primarily involves lifestyle modifications focused on healthy eating, regular physical activity, and behavioral changes. A balanced, calorie-controlled diet with whole foods and reduced processed food intake is key, along with at least 150 min of moderate aerobic exercise weekly. Behavioral strategies like goal setting and self-monitoring support long-term weight management and improved overall health [29,30].
- Medication. Prescription medications to treat obesity work in different ways. For example, some medications may help one feel less hungry or full sooner. Other medications may make it harder for one’s body to absorb fat from the foods one eats. Examples of FDA-approved medications include orlistat (Xenical, Alli), phentermine–topiramate (Qsymia), naltrexone–bupropion (Contrave), and liraglutide (Saxenda). Healthcare professionals prescribe a medication to treat obesity if an adult has a BMI of 30 or greater.
5. Numerical Results and Discussions
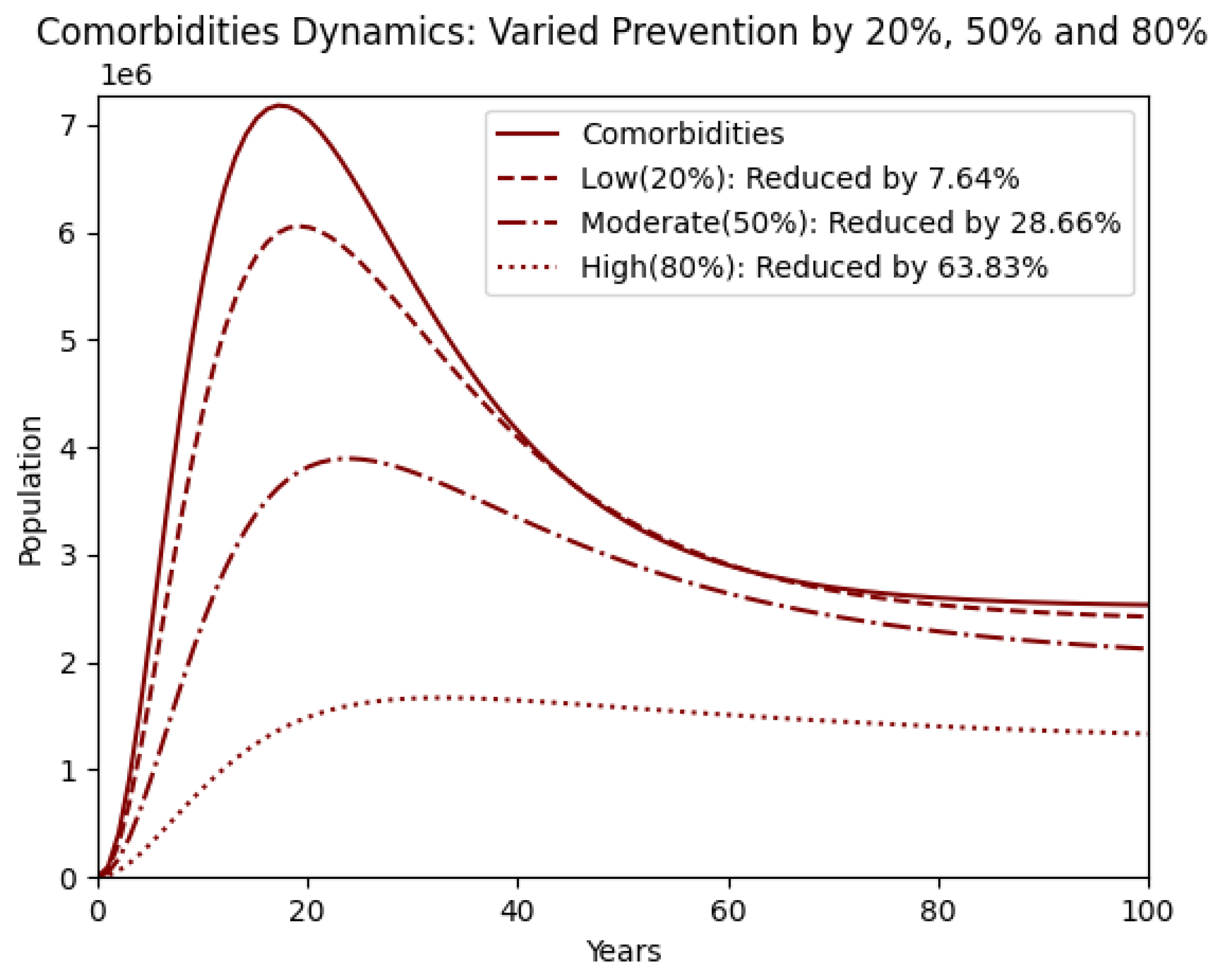
- 1.
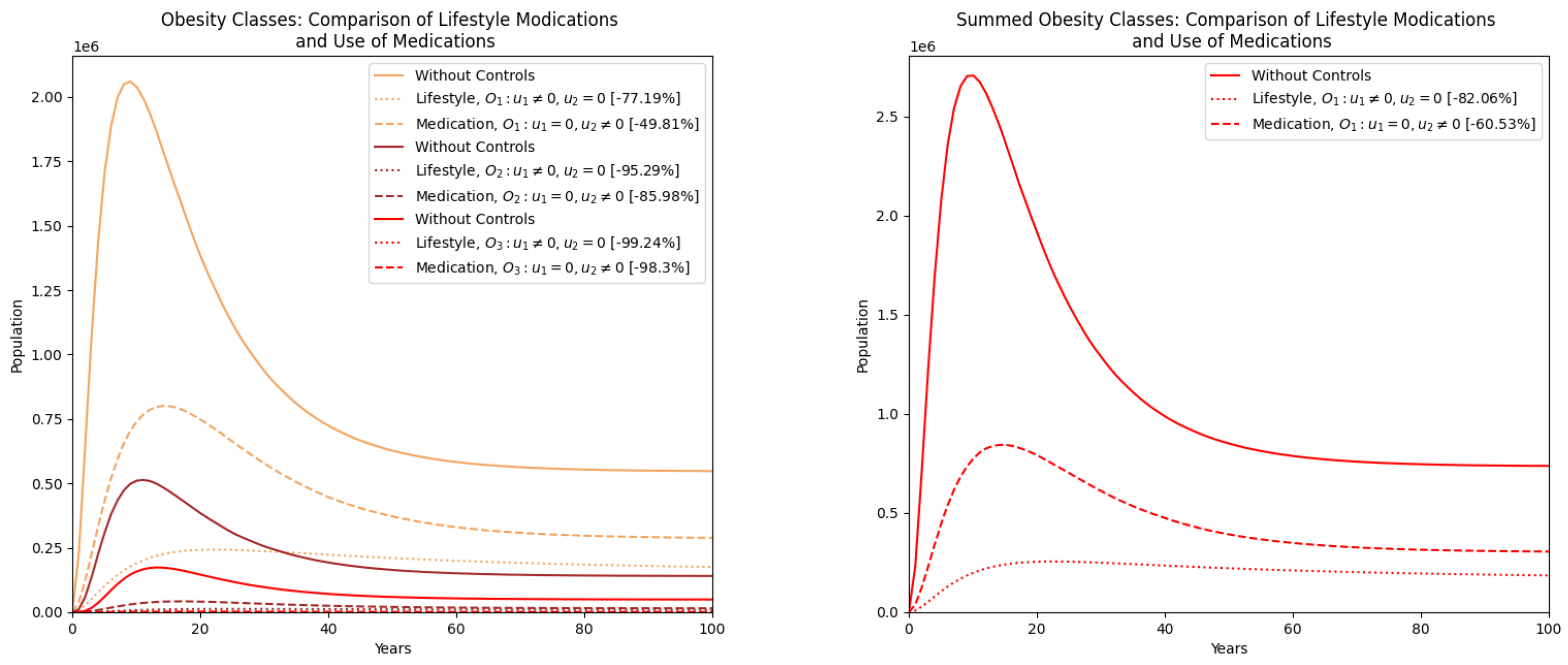
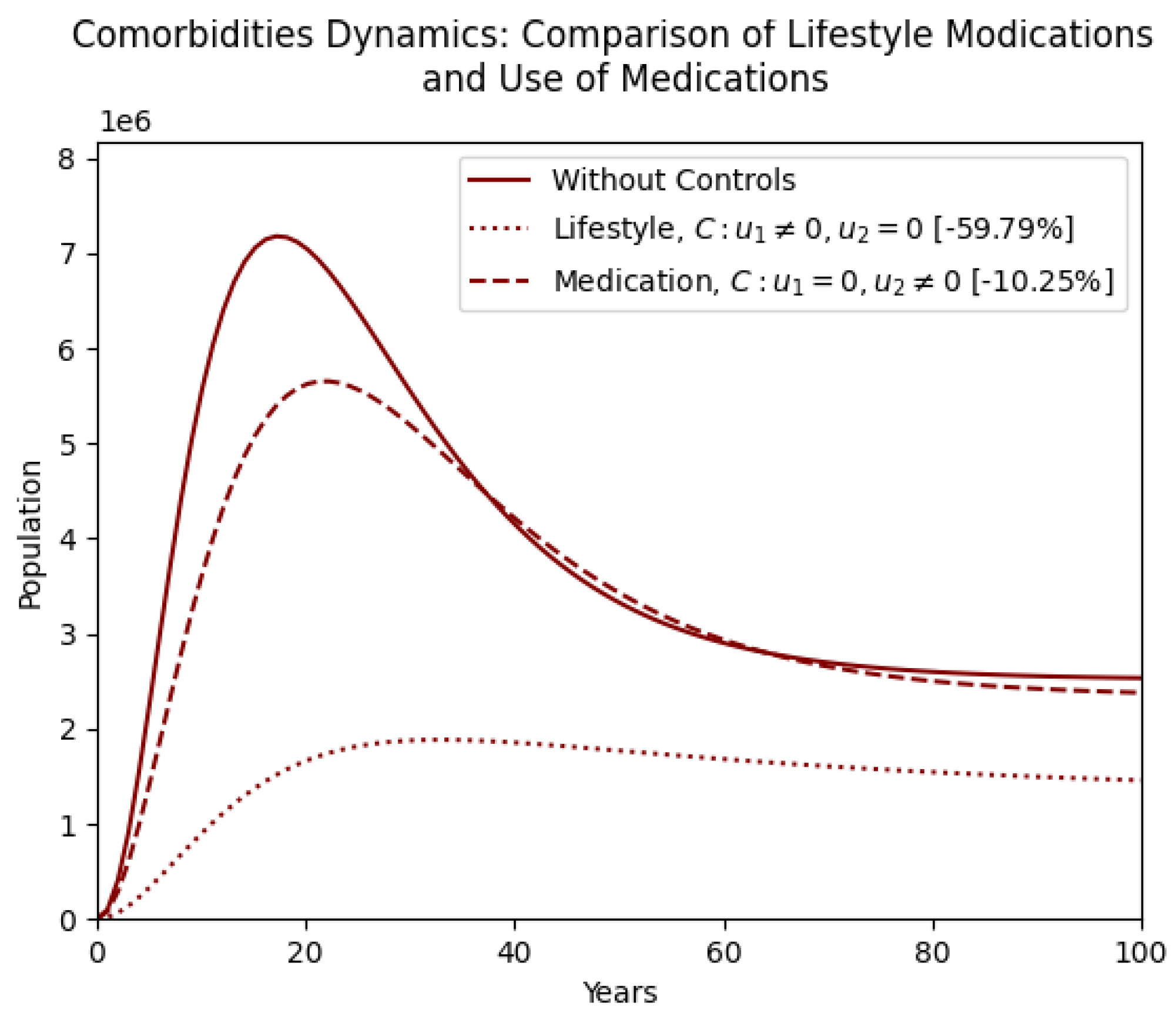
- Lifestyle interventions independently produce the highest reductions in total obesity () and comorbidities (), highlighting the effectiveness of prevention-based strategies.
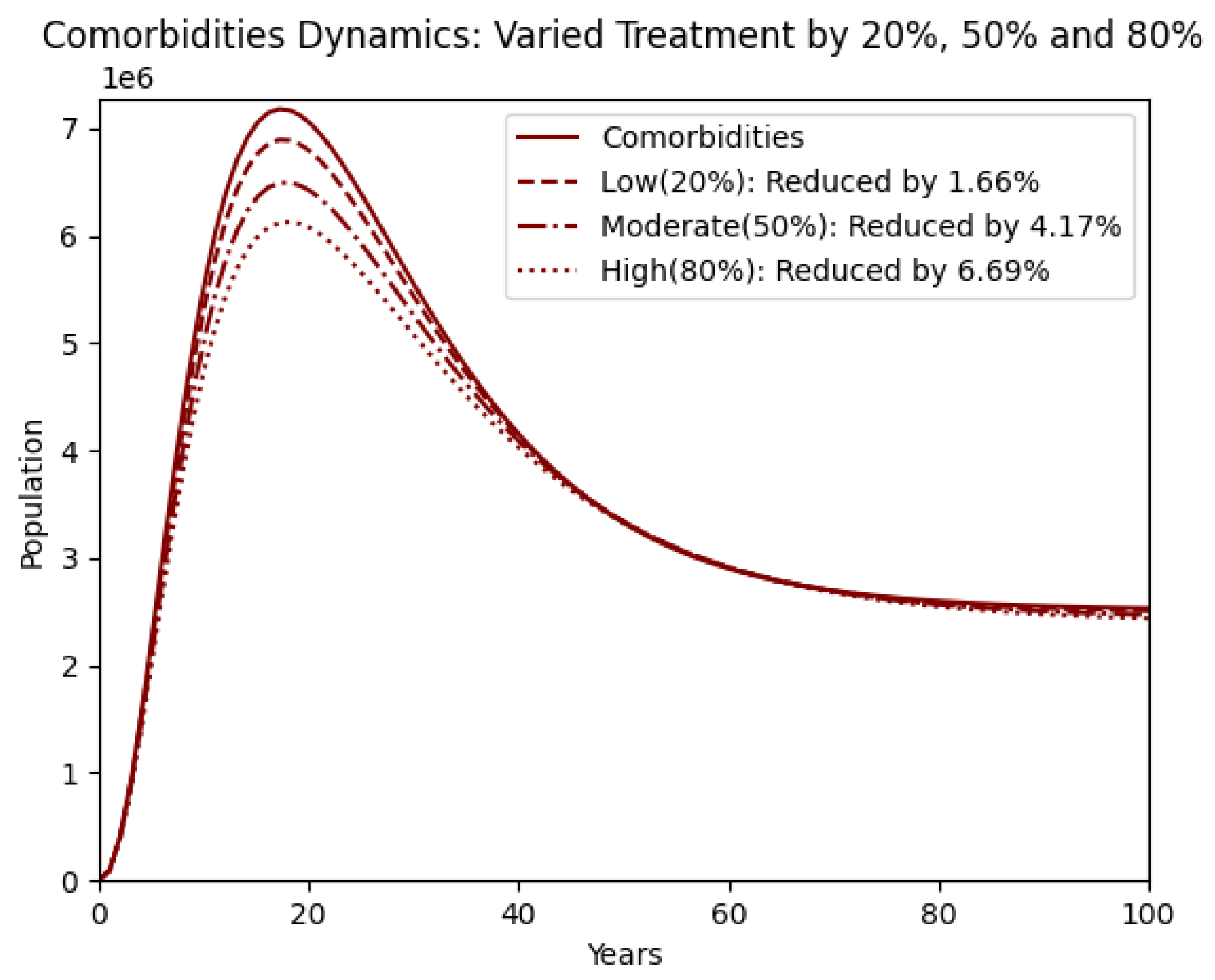
- 2.
- Medication alone demonstrates moderate efficacy, particularly in mitigating higher obesity classes, but yields a limited impact on comorbidity reduction ().
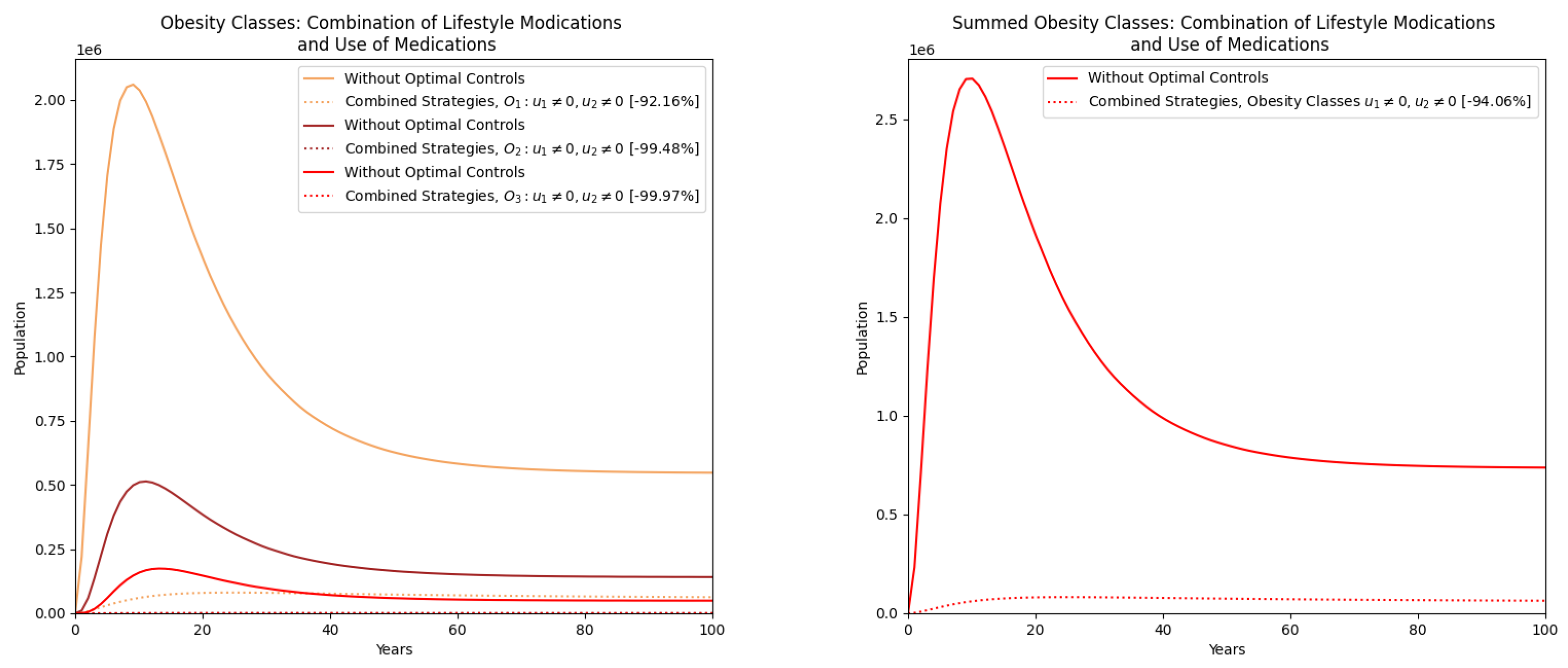
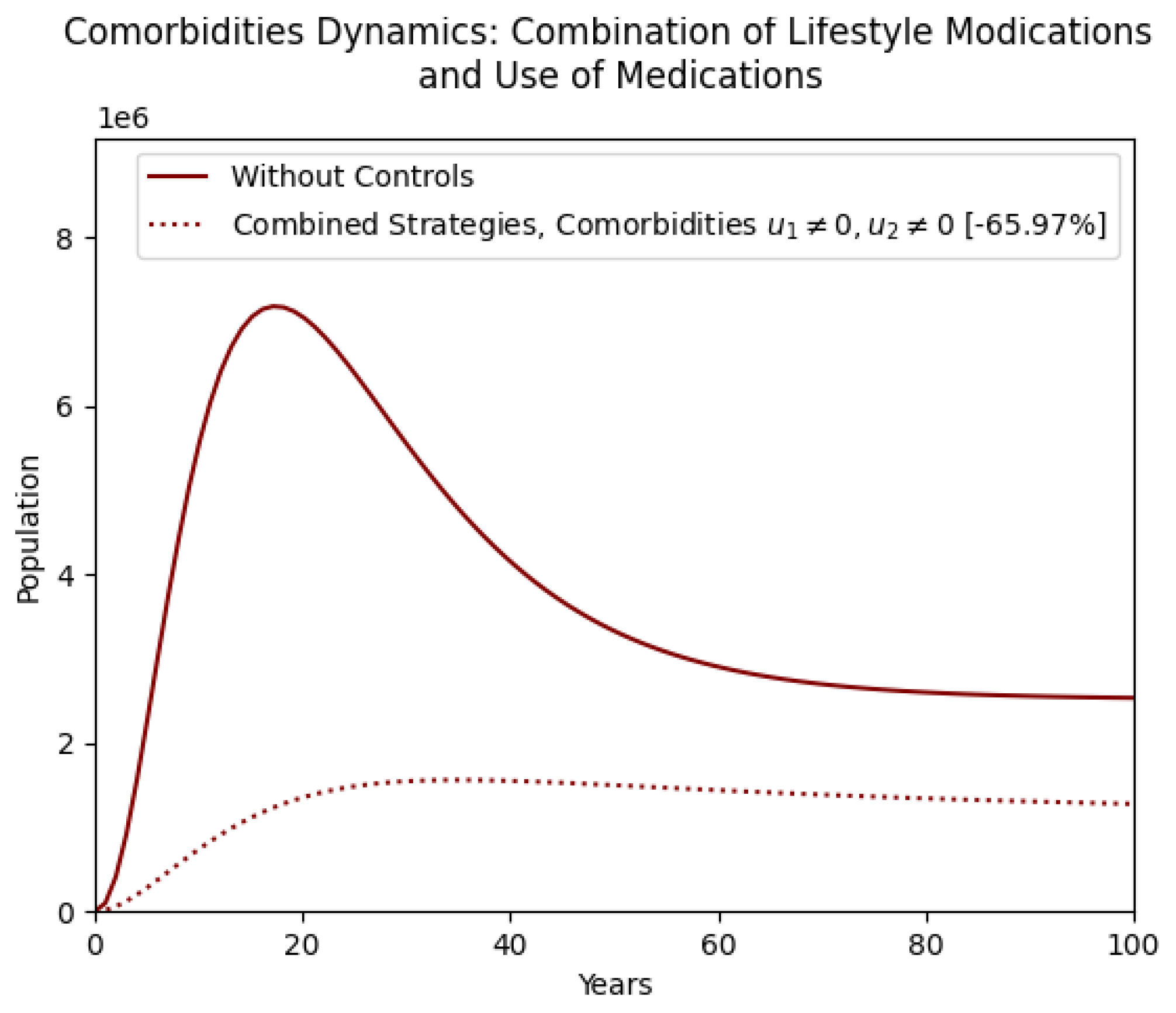
- 3.
- Combined strategies, incorporating both lifestyle modifications and medication, result in the most pronounced outcomes, reducing total obesity by and comorbidities by .
- 4.
- Integrating lifestyle and medication interventions leads to greater reductions in obesity and comorbidities than single methods, highlighting the need for comprehensive, prevention-focused public health policies.
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Obesity Federation. World Obesity Atlas. 2023. Available online: https://data.worldobesity.org/publications/?cat=19 (accessed on 21 November 2024).
- World Health Organization. Obesity and Overweight. 1 March 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 November 2024).
- Alluhidan, M.; Alsukait, R.F.; Alghaith, T.; Shekar, M.; Alazemi, N.; Herbst, C.H. Overweight and Obesity in Saudi Arabia: Consequences and Solutions; World Bank: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, distribution, and its current association with various health conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef] [PubMed]
- Al-Raddadi, R.; Bahijri, S.M.; Jambi, H.A.; Ferns, G.; Tuomilehto, J. The prevalence of obesity and overweight, associated demographic and lifestyle factors, and health status in the adult population of Jeddah, Saudi Arabia. Ther. Adv. Chronic Dis. 2019, 10, 2040622319878997. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef]
- Alsulami, S.; Baig, M.; Ahmad, T.; Althagafi, N.; Hazzazi, E.; Alsayed, R.; Alghamdi, M.; Almohammadi, T. Obesity prevalence, physical activity, and dietary practices among adults in Saudi Arabia. Front. Public Health 2023, 11, 1124051. [Google Scholar] [CrossRef]
- Jódar, L.; Santonja, F.J.; González-Parra, G. Modeling dynamics of infant obesity in the region of Valencia, Spain. Comput. Math. Appl. 2008, 56, 679–689. [Google Scholar] [CrossRef]
- Santonja, F.-J.; Villanueva, R.-J.; Jódar, L.; Gonzalez-Parra, G. Mathematical modelling of social obesity epidemic in the region of Valencia, Spain. Math. Comput. Model. Dyn. Syst. 2010, 16, 23–34. [Google Scholar] [CrossRef]
- Ejima, K.; Thomas, D.M.; Allison, D.B. A Mathematical Model for Predicting Obesity Transmission with Both Genetic and Nongenetic Heredity. Obesity 2018, 26, 927–933. [Google Scholar] [CrossRef]
- Al-Tuwairqi, S.M.; Matbouli, R.T. Modeling dynamics of fast food and obesity for evaluating the peer pressure effect and workout impact. Adv. Differ. Equ. 2021, 2021, 59. [Google Scholar] [CrossRef]
- Ku-Carrillo, R.A.; Delgadillo, S.E.; Chen-Charpentier, B.M. A mathematical model for the effect of obesity on cancer growth and on the immune system response. Appl. Math. Model. 2016, 40, 4908–4920. [Google Scholar] [CrossRef]
- Ku-Carrillo, R.A.; Delgadillo-Aleman, S.E.; Chen-Charpentier, B.M. Effects of the obesity on optimal control schedules of chemotherapy on a cancerous tumor. J. Comput. Appl. Math. 2017, 309, 603–610. [Google Scholar] [CrossRef]
- Siewe, N.; Friedman, A. A mathematical model of obesity-induced type 2 diabetes and efficacy of an anti-diabetic weight-reducing drug. J. Theor. Biol. 2024, 581, 111756. [Google Scholar] [CrossRef] [PubMed]
- Dehingia, K.; Yao, S.W.; Sadri, K.; Das, A.; Sarmah, H.K.; Zeb, A.; Inc, M. A study on cancer-obesity-treatment model with quadratic optimal control approach for better outcomes. Results Phys. 2022, 42, 105963. [Google Scholar] [CrossRef]
- Aldila, D.; Rarasati, N.; Nuraini, N.; Soewono, E. Optimal Control Problem of Treatment for Obesity in a Closed Population. Int. J. Math. Math. Sci. 2014, 2014, 273037. [Google Scholar] [CrossRef]
- Fatima, B.; Ikhlaq, M.; Zaman, G. The obesity prevention strategies in population dynamics. Adv. Model. Optim. 2017, 19, 213–225. [Google Scholar]
- Yanovski, S.Z.; Donato, K.; Gansheroff, L. The Obesity Epidemic: The Role of the National Institutes of Health. Adv. Stud. Med. 2005, 5, 122–123. [Google Scholar]
- Alshammari, F.S. A Mathematical Model to Investigate the Transmission of COVID-19 in the Kingdom of Saudi Arabia. Comput. Math. Methods Med. 2020, 2020, 9136157. [Google Scholar] [CrossRef]
- Moya, E.D.; Pietrus, A.; Bernard, S. A mathematical model for the study of obesity in a population and its impact on the growth of diabetes. Math. Model. Anal. 2023, 28, 611–635. [Google Scholar] [CrossRef]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef]
- Apovian, C.M.; Aronne, L.J.; Barenbaum, S. Obesity Comorbidities: Clinical Guidance. Healio, 2024. Available online: https://www.healio.com/clinical-guidance/obesity/obesity-related-comorbidities (accessed on 29 November 2024).
- Lartey, S.T.; Si, L.; Otahal, P.; de Graaff, B.; Boateng, G.O.; Biritwum, R.B.; Minicuci, N.; Kowal, P.; Magnussen, C.G.; Palmer, A.J. Annual transition probabilities of overweight and obesity in older adults: Evidence from World Health Organization Study on global AGEing and adult health. Soc. Sci. Med. 2020, 247, 112821. [Google Scholar] [CrossRef]
- Ahmad, S.; Kirane, M. On a fractional-order mathematical model to assess the impact of diabetes and its associated complications in the United Arab Emirates. Math. Methods Appl. Sci. 2024, 47, 6892–6902. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Holloway, S.; Sommer Matthiessen, K.; Thompson, A.; Capucci, S. Variations in healthcare costs by body mass index and obesity-related complications in a UK population: A retrospective open cohort study. Diabetes Obes. Metab. 2024, 26, 5036–5045. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Kahan, S. Maintenance of lost weight and long-term management of obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Orwa, T.O.; Mbogo, R.W.; Luboobi, L.S. Multiple-Strain Malaria Infection and Its Impacts on Plasmodium falciparum Resistance to Antimalarial Therapy: A Mathematical Modelling Perspective. Comput. Math. Methods Med. 2019, 2019, 9783986. [Google Scholar] [CrossRef]
- Skou, S.T.; Mair, F.S.; Fortin, M.; Guthrie, B.; Nunes, B.P.; Miranda, J.J.; Boyd, C.M.; Pati, S.; Mtenga, S.; Smith, S.M. Multimorbidity. Nat. Rev. Dis. Primers 2022, 8, 48. [Google Scholar] [CrossRef]
- Van Baak, M.A.; Pramono, A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of different types of regular exercise on physical fitness in adults with overweight or obesity: Systematic review and meta-analyses. Obesity Rev. 2021, 22, e13239. [Google Scholar] [CrossRef]
- Veit, M.; van Asten, R.; Olie, A.; Prinz, P. The role of dietary sugars, overweight, and obesity in type 2 diabetes mellitus: A narrative review. Eur. J. Clin. Nutr. 2022, 76, 1497–1501. [Google Scholar] [CrossRef]
- Ayele, T.K.; Goufo, E.F.D.; Mugisha, S. Mathematical modeling of HIV/AIDS with optimal control: A case study in Ethiopia. Results Phys. 2021, 26, 104263. [Google Scholar] [CrossRef]
- Cheneke, K.R. Optimal control and bifurcation analysis of HIV model. Comput. Math. Methods Med. 2023, 2023, 4754426. [Google Scholar] [CrossRef]
- Pontryagin, L.S. The Mathematical Theory of Optimal Processes; John Wilely & Sons: Hoboken, NJ, USA, 1962; Chapter 2. [Google Scholar]
- Lenhart, S.; Workman, J.T. Optimal Control Applied to Biological Models; Chapman and Hall/CRC: Boca Raton, FL, USA, 2007. [Google Scholar] [CrossRef]
- Ahmad, N.N.; Robinson, S.; Kennedy-Martin, T.; Poon, J.L.; Kan, H. Clinical outcomes associated with anti-obesity medications in real-world practice: A systematic literature review. Obes. Rev. 2021, 22, e13326. [Google Scholar] [CrossRef]
- May, A.L.; Freedman, D.; Sherry, B.; Blanck, H.M.; Centers for Disease Control and Prevention (CDC). Obesity United States, 1999–2010. MMWR Suppl. 2013, 62, 120–128. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| District | No. of Obese Participants | Ratio |
|---|---|---|
| Madinah | 84 out of 366 | |
| Baha | 52 out of 364 | |
| Jazan | 72 out of 361 | |
| Eastern Region | 106 out of 360 | |
| Jouf | 96 out of 361 | |
| Hail | 72 out of 359 | |
| Asir | 66 out of 366 | |
| Qassim | 66 out of 361 | |
| Riyadh | 98 out of 364 | |
| Mecca | 92 out of 362 | |
| Tabuk | 70 out of 362 | |
| Northern Borders | 76 out of 361 | |
| Najran | 73 out of 362 |
| Age Group | No. of Obese Participants | Ratio |
|---|---|---|
| 18–19 | 36 out of 255 | |
| 20–29 | 231 out of 1556 | |
| 30–39 | 183 out of 1009 | |
| 40–49 | 311 out of 1044 | |
| 50–59 | 182 out of 555 | |
| 60+ | 80 out of 290 |
| Parameter | Meaning | Value | Source |
|---|---|---|---|
| Recruitment rate | 0.01335 | [19] | |
| Rate of becoming overweight | 0.13 | [20] | |
| Rate of becoming obese stage 1 | 0.14 | [20] | |
| Rate of becoming obese stage 2 | 0.16 | Assumed | |
| Rate of becoming obese stage 3 | 0.18 | Assumed | |
| Comorbidity acquisition rate for overweight | 0.0392 | [21] | |
| Comorbidity acquisition rate for obese stage 1 | 0.33 | [22] | |
| Comorbidity acquisition rate for obese stage 2 | 0.38 | [22] | |
| Comorbidity acquisition rate for obese stage 3 | 0.44 | [22] | |
| Treatment rate for overweight | 0.09 | [23] | |
| Treatment rate for obese stage 1 | 0.08 | [23] | |
| Treatment rate for obese stage 2 | 0.07 | Assumed | |
| Treatment rate for obese stage 3 | 0.06 | Assumed | |
| Comorbidity-induced mortality rate | 0.1225 | [24] | |
| Natural mortality rate | 0.03 | [19] |
| Stability of | Conditions |
|---|---|
| Local asymptotic stability | (i) |
| (ii) | |
| (iii) | |
| Global asymptotic stability | (i) |
| (ii) |
| Target | Varying | O | C | |||
|---|---|---|---|---|---|---|
| Prevention | Low (20%) | 7.78% | 22.32% | 37.88% | 12.51% | 7.64% |
| Moderate (50%) | 33.88% | 74.32% | 94.31% | 45.5% | 28.66% | |
| High (80%) | 78.61% | 96.55% | 99.69% | 83.39% | 63.83% | |
| Treatment | Low (20%) | 1.71% | 3.32% | 5.51% | 2.26% | 1.66% |
| Moderate (50%) | 7.32% | 8.18% | 13.21% | 5.64% | 4.17% | |
| High (80%) | 6.97% | 12.89% | 20.28% | 8.97% | 6.69% | |
| Prevention + Treatment | Low (20%) | 10.12% | 25.68% | 41.92% | 15.16% | 9.73% |
| Moderate (50%) | 39.31% | 67.16% | 84.51% | 47.55% | 53.46% | |
| High (80%) | 83.36% | 96.25% | 99.32% | 86.85% | 71.83% |
| Controls | O | C | |||
|---|---|---|---|---|---|
| Lifestyle | |||||
| Medication | |||||
| Combining strategies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, M.I.; Maina, R.M.; Gathungu, D.K.; Radwan, A. A Qualitative Analysis and Discussion of a New Model for Optimizing Obesity and Associated Comorbidities. Symmetry 2025, 17, 1216. https://doi.org/10.3390/sym17081216
Youssef MI, Maina RM, Gathungu DK, Radwan A. A Qualitative Analysis and Discussion of a New Model for Optimizing Obesity and Associated Comorbidities. Symmetry. 2025; 17(8):1216. https://doi.org/10.3390/sym17081216
Chicago/Turabian StyleYoussef, Mohamed I., Robert M. Maina, Duncan K. Gathungu, and Amr Radwan. 2025. "A Qualitative Analysis and Discussion of a New Model for Optimizing Obesity and Associated Comorbidities" Symmetry 17, no. 8: 1216. https://doi.org/10.3390/sym17081216
APA StyleYoussef, M. I., Maina, R. M., Gathungu, D. K., & Radwan, A. (2025). A Qualitative Analysis and Discussion of a New Model for Optimizing Obesity and Associated Comorbidities. Symmetry, 17(8), 1216. https://doi.org/10.3390/sym17081216