1. Introduction
Poor air quality is one of the leading global risk factors that can contribute to premature death and disability adjusted life years (DALYs) [
1,
2]. It has been well documented that efforts to reduce air pollution can lead to substantial health benefits, such as reducing premature deaths and the exacerbation or development of a number of respiratory- and cardiovascular-related diseases [
3,
4,
5,
6]. The assessment of the health impacts of air pollution can be beneficial to not only conveying the public health impact of poor air quality, but also when considering the potential implementation of various air quality policies. Therefore, assessments of the potential health impacts that could be achieved through improvements in air quality represent an important data point for public health and environmental specialists.
To estimate the public health impact of changes in air quality, which includes both the number of premature deaths and illnesses and often their associated economic value, numerous tools of varying complexity have been developed [
7]. Of these tools, the World Health Organization’s AirQ+ and U.S. Environmental Protection Agency’s (U.S. EPA) Environmental Benefits Mapping and Analysis Program—Community Edition (BenMAP—CE) are among the most popular. Both AirQ+ and BenMAP—CE have been used and reported in an extensive number of peer-reviewed publications and technical reports, which reflects their varying functionality in terms of the types of analyses and questions each can address. The range of countries where applications of AirQ+ and BenMAP—CE were performed covers multiple continents, with the most extensive use in Asia, North America, South America, and Europe.
BenMAP was initially released in 2003 and represented the primary tool used by the U.S. EPA to estimate the health and economic benefits of attaining current and potentially future National Ambient Air Quality Standards (NAAQS) [
8]. While the tool was used extensively by the U.S. EPA, it was also used in multiple research efforts to estimate the potential public health impacts of improving air quality [
9,
10]. Building off the original version of BenMAP, starting in 2012, the U.S. EPA transformed the tool into an open-source software platform to allow for it to be more broadly accessible to the global air pollution research community, culminating in the release of BenMAP—CE in 2015 [
8]. Similar to the original version, BenMAP—CE is extensively used by the U.S. EPA in various policy-related analyses, but its use by the broader research community has grown exponentially. This can be attributed to not only BenMAP—CE being freely available, but also the various types of analyses that can be conducted using the tool. As detailed within Sacks et al. [
8], data inputs, which can range from fine to coarse resolution in spatial scale and can include both monitored and modeled air quality data, allow for conducting analyses of varying complexity.
While BenMAP was originally developed to support U.S. air quality policy analyses, and only within the last 10 years expanded to have a global reach, WHO developed an Excel-based software tool called AirQ starting in 1999, originally targeting only European countries. The original aims of AirQ were to: (1) convey to the user the most important and best recognized health effects attributed to air pollution; (2) provide an incentive to collect and analyze data on air pollution (use of nationally/locally available air quality data); (3) share the air quality data with the WHO Regional Office for Europe; and (4) provide easily interpretable results to convey the overall health impact of air pollution, such as Attributable Fraction (AF), attributable morbidity and mortality, and Years of Life Lost (YLLs) estimates [
11].
Between 1999 and 2001, this tool was programmed to focus on health impacts attributed to short-term exposures (i.e., daily variations in air quality). From 2001 to 2004, AirQ was tested and expanded to also estimate health impacts attributed to long-term air pollution exposures, which ultimately contributed to the tool being widely used by experts internationally. Although AirQ was gaining wide acceptance within the research community, in the following years WHO recognized the tool needed to be updated to incorporate the latest scientific evidence on the health impacts attributed to air pollution and to respond to the new technological requirements of computer systems. As a result, in 2016 AirQ+ was developed building on the success of AirQ, but with the specific purposes of (1) reflecting the current state of the science on the health effects of air pollution; (2) ensuring that researchers and governmental officials worldwide could have access to a tool to inform and ultimately support actions to improve air quality; and (3) to provide a large audience with an educational tool that includes summaries of the information that needs to be gathered and organized to understand the impacts of air pollution on health. To facilitate the goal of achieving broad acceptance and use of the tool, versions of AirQ+ are currently available in English, French, and Russian with German and Spanish language versions under development.
While BenMAP—CE and AirQ+ have been two of the most extensively used tools to estimate the potential health impacts of changes in air quality, with BenMAP—CE having the additional feature of being able to estimate the potential economic benefits, the two tools have not been evaluated using a similar dataset. Within this paper, we conduct an analysis using a common, hypothetical dataset, to demonstrate how basic analyses are conducted using both BenMAP—CE and AirQ+, and highlight the differences and similarities between the two tools. Specifically, this paper highlights the underlying methodology used to estimate health impacts in both tools, the data preloaded within each tool along with the data that can be provided by the user to tailor analyses, and the differences in the processes used by U.S. EPA and WHO to identify the health impacts to estimate.
3. Results
Across the two subregions, the average annual PM2.5 concentration was 27.50 μg/m3, which equates to a population-weighted concentration of 27.69 μg/m3. When examining each of the subregions separately, Subregion 1 was found to have an arithmetic mean PM2.5 concentration of 25.47 μg/m3, while Subregion 2 was found to have an arithmetic mean PM2.5 concentration of 29.53 μg/m3.
When comparing the results of the analysis, both BenMAP—CE and AirQ+ calculated almost identical results for the central estimates at the integer level with minimal differences at the decimal digits level (
Table 3 and
Table 4). In addition to the main result, or central estimate, each tool also reports confidence intervals that bound the main result. AirQ+ calculates the 95% confidence intervals around the estimated health impacts using the 95% confidence interval associated with the risk estimate from the published epidemiologic study used in the analysis (e.g., 95% CI: 1.040–1.083 from Hoek et al. [
14]). From the 95% confidence interval, it is possible to calculate the corresponding standard error. Assuming a normal distribution, AirQ+ uses the standard error to estimate the uncertainty around the main result. In contrast, BenMAP-CE performs a Monte Carlo analysis, sampling the standard error reported in the epidemiologic study from which the beta coefficient is used. Thus, this confidence interval reflects statistical uncertainty in the epidemiologic study, but not other sources of uncertainty associated with the remaining input parameters. While the U.S. EPA commonly reports counts of air pollution-attributable deaths and illnesses rounded to two significant figures, we report unrounded values to demonstrate the consistency of the results across the two tools. The slight difference in the calculation of confidence intervals between the two tools did not result in significant differences (less than 1%) in the reported 95% confidence intervals (
Table 3 and
Table 4).
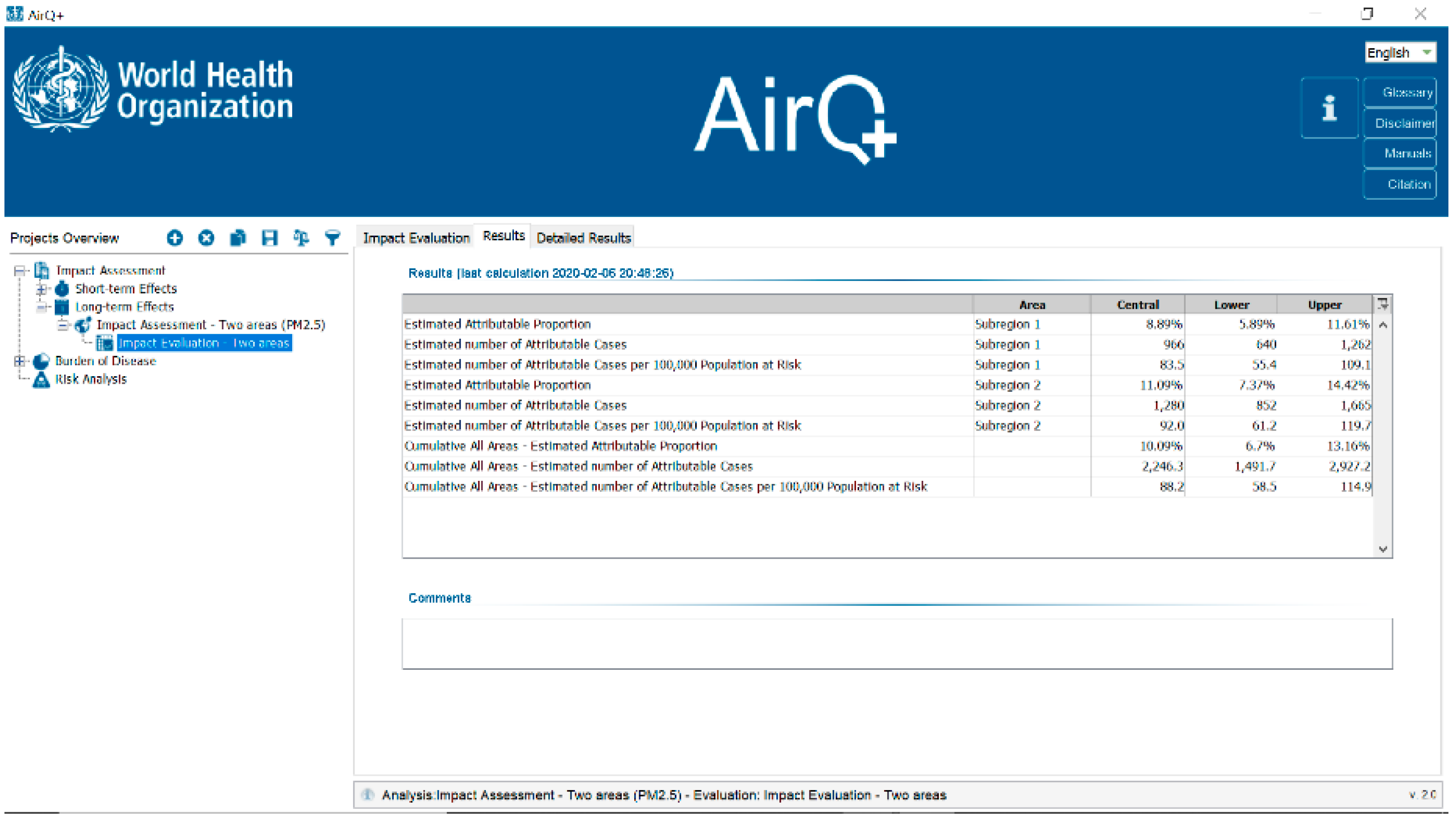
In the main analysis, where a counterfactual of 10 μg/m3 was used, which equated to the WHO AQG annual PM2.5 value, the results from Subregion 1 and Subregion 2 indicate that approximately 965 and 1280 premature deaths are attributable to long-term PM2.5 exposure, respectively. Therefore, reducing PM2.5 concentrations in Subregion 1 and Subregion 2 to an annual PM2.5 concentration of 10 μg/m3 would reduce the total number of premature deaths attributed to long-term PM2.5 exposure.
In addition to the estimated number of attributable cases, which represents the main result from both tools, each allows for the calculation of additional results that give users greater insight into the estimated health impacts. For AirQ+, the tool directly calculates these additional values and includes the estimated attributable proportion of deaths from long-term PM
2.5 exposure as well as the estimated number of attributable cases per 100,000 population at risk (
Table 3). The estimated attributable proportion is a population-normalized value that reflects the percentage of total all-cause deaths that are attributable to PM
2.5 exposure. The estimated number of attributable cases per 100,000 population at risk is also population-normalized and can be useful when comparing the health impacts attributable to air pollution across locations of different population sizes. While BenMAP—CE does not provide this information as an output in the results, it can easily be calculated using the input parameters for the analysis along with the main result presented from the analysis, i.e., the estimated number of attributable cases. As depicted in
Table 3, in Subregion 1 the estimated attributable proportion is 8.9% and in Subregion 2, 11.1%, while the estimated number of attributable cases per 100,000 population at risk is approximately 83.5 in Subregion 1, and 92.0 in Subregion 2.
Sensitivity Analysis
When conducting sensitivity analyses using alternative counterfactual values representing annual PM
2.5 concentrations of 5, 12, and 25 µg/m
3, consistent with the main analysis, both BenMAP—CE and AirQ+ produced similar results. As the counterfactual value was reduced, the number of premature deaths attributed to long-term PM
2.5 exposure increased, reflecting the increase in the difference between the baseline annual PM
2.5 concentrations and the counterfactual PM
2.5 concentration in both Subregion 1 and Subregion 2 (
Table 4). Reducing annual PM
2.5 concentrations to the counterfactual values of 25, 12, and 5 μg/m
3 was estimated in Subregion 1 to equate to approximately 30, 850, and 1260 premature deaths, respectively, and in Subregion 2, 310, 1150, and 1580 premature deaths, respectively.
4. Discussion
By using a common dataset, the main analysis, and sensitivity analyses, demonstrated that BenMAP—CE and AirQ+ produce similar results in the process of estimating the public health impact of poor air quality. The analyses further confirm that the underlying methodology used by each tool is consistent and that each tool can be used with confidence to estimate the public health impacts attributed to air pollution. Although the results obtained using both tools are similar, it is important to recognize the strengths and limitations of each tool as researchers or risk assessors embark on efforts to quantify air pollution-related health and economic impacts.
There are numerous strengths and benefits to using BenMAP—CE and AirQ+ individually, but each was originally developed for a different purpose, which is reflected in the different features of each tool. BenMAP—CE was developed for the purpose of supporting policy-related risk and benefits analyses in the process of promulgating environmental regulations at the U.S. EPA, while AirQ+ was developed as a decision support tool that also has a considerable educational focus for public health authorities [
8]. Even with the original difference in the purpose of each tool, it is important to note the commonality amongst them and that both: (1) come with an extensive history of development and maintenance that have directly contributed to the large communities of users worldwide; (2) can estimate health impacts attributed to short-term (i.e., daily) and long-term (i.e., yearly) air pollution exposures; (3) can estimate impacts for a range of health endpoints and for different pollutants (see
Table 1); and (4) offer features that are unique to each tool. Specifically, BenMAP—CE can estimate the potential economic impact associated with air pollution-related health impacts, which is a functionality not contained within AirQ+. However, AirQ+ offers the ability to estimate the health impacts attributed to household air pollution (i.e., due to solid fuel use) and an assessment of the cancer risk associated with some air pollutants, both of which are not possible in the current version of BenMAP—CE, but could potentially be included within the tool in the future. BenMAP—CE is designed to support U.S. federal, state, and local air quality policies, allowing users to assess health and economic impacts over time and space using either pre-loaded or user-specified input parameters (
Table 1). Similar to BenMAP—CE, AirQ+ can also be used to estimate health impacts at different spatial scales, and therefore, be used to inform various potential air quality actions. Both BenMAP-CE and AirQ+ are useful tools for estimating the health impacts of poor air quality with the decision regarding which tool to use at the discretion of the user based on both data availability (e.g., type and resolution of air quality data) and the research question to be examined.
Although there are commonalities between BenMAP—CE and AirQ+, the differentiation in the original purpose of both tools has factored into the process used to determine the types of information preloaded within each. This is most prominently reflected in the health impact functions available in both tools that the user can select to estimate health impacts. Because BenMAP—CE is used extensively in the rule-making process for various environmental regulations, with a prominent role within the review process of the National Ambient Air Quality Standards (NAAQS), a more rigorous approach is taken in determining the health endpoints to estimate and, subsequently, the selection of epidemiologic studies to be used to derive health impact functions. In selecting the health endpoints to quantify, the U.S. EPA relies heavily on the scientific evidence evaluated within the Integrated Science Assessments (ISAs), which form the scientific basis of the NAAQS. The ISAs represent a rigorous evaluation of the scientific evidence spanning epidemiologic, experimental (animal toxicological and controlled human exposure), dosimetry, exposure, atmospheric chemistry, and welfare effects studies using a weight-of-evidence approach to assess the causal nature of relationships between criteria pollutant exposures and health and welfare effects [
15]. It is within the ISAs that the U.S. EPA conveys their overall conclusions on the degree to which the scientific evidence supports a causal relationship between an air pollutant exposure and health effect category (e.g., respiratory effects, mortality, etc.). The conclusions for each of the health effect categories evaluated directly informs the health endpoints considered for inclusion within BenMAP—CE. Specifically, for those health effect categories where the ISA concludes that a “causal relationship” or a “likely to be causal relationship” exists, the U.S. EPA further evaluates the available epidemiologic studies that formed the basis of these conclusions to identify the studies that could be used to derive health impact functions. Within this additional assessment of epidemiologic studies, the U.S. EPA is evaluating whether the additional pieces of information needed to derive a health impact function from an epidemiologic study are readily available, such as data that corresponds to the population examined within the study (e.g., total population ≥ 65 years of age) and the baseline incidence rate for the health effect evaluated (e.g., mortality rate for the population ≥ 65 years of age).
Compared to BenMAP—CE, AirQ+ was developed with a target audience of public health specialists in mind rather than policy analysts. As a result, although WHO relied heavily on the scientific evidence evaluated within expert groups in determining the air pollutant–health outcome relationships to quantify, it also includes features that are supportive of research activities in specific scientific areas. As a result, contrary to the approach used in BenMAP—CE for selecting the health outcomes to quantify, AirQ+ quantifies the impacts for some air pollutant–health outcome relationships where the evidence base is not as strong, specifically for the air pollutants NO2, BC, and long-term ozone exposure. The philosophy behind WHO’s incorporation of these additional air pollutants and corresponding health impact functions into AirQ+ is that they can aid in identifying potential research gaps and open discussion not only with the scientific community, but also with users on the limits and benefits that should be taken into account when performing non-mainstream analyses.
While the overall process of estimating health impacts is similar between BenMAP—CE and AirQ+, there are differences in the resolution of information used in both tools, which is a function of BenMAP—CE containing GIS components. As a result, the analyses conducted within AirQ+ are at a much coarser spatial resolution, often over the spatial domain of an entire city or country. This differs from BenMAP—CE where it is possible to conduct analyses for an entire city or country, but at the grid cell level, as small as 1 km × 1 km, which can allow for a detailed analysis of how both exposures and health impacts vary across a geographic location.
In addition to the main features of BenMAP—CE and AirQ+, both contain additional features that are unique to each tool. For BenMAP—CE, this includes the Global Burden of Disease (GBD) Rollback Tool and Popsim. The Global Burden of Disease (GBD) Rollback Tool has contributed to the ability of BenMAP—CE to expand its reach to international audiences. This easy to use tool that is embedded within BenMAP—CE allows for users to estimate the potential health and economic benefits (i.e., reductions in mortality) of improving air quality in any country or region worldwide using air quality, population, baseline health, and concentration-response parameters from the GBD project. Within the tool, users can estimate the number of PM2.5-attributable premature deaths that could be reduced through “rolling back” concentrations by either: a fixed air quality increment (e.g., 5 µg/m3); a proportion (e.g., 5%); or down to various air quality standards (e.g., the U.S. EPA Particulate Matter NAAQS) or guidelines (e.g., the WHO AQG). Users can also estimate the economic value of these PM2.5-attributable premature deaths using a country-specific Value of Statistical Life. The GBD Rollback Tool is advantageous to users located in countries where it is difficult to obtain all of the underlying data needed to estimate health and economic impacts, such as baseline incidence rates and population data because it allows for the ability to gain a better understanding of the potential public health benefits of improving air quality.
The second feature within BenMAP—CE, Popsim, uses a life table to quantify the number of PM2.5-attributable life years gained, PM2.5-attributable deaths avoided, and improved life expectancy at birth as a result of reducing PM2.5 concentrations in the U.S. This tool uses country-specific life tables, thus accounting for the between-country variability in age-specific death rates. In contrast to the core BenMAP-CE program that is operated for a specific recent or future year, Popsim estimates year-to-year changes in the risk of death over a 50-to-100 year time horizon.
Compared to BenMAP—CE, AirQ+ has the added benefit of being able to conduct analyses to estimate the health impacts for different air pollution exposures that cannot be evaluated using BenMAP—CE. As is noted in the GBD project, household air pollution represents one of the top 10 risks to health worldwide, particularly in developing countries [
1]. AirQ+ allows users to estimate the health impacts attributed to household air pollution through the inclusion of health impact functions for solid fuel use. The risk estimates used for household air pollution, which is an area of scientific development that in the future may produce new methods that could potentially be included in future versions of AirQ+. Additionally, it is well characterized that air pollution contains many pollutants that have been classified as carcinogens [
16]. Building off this scientific evidence, AirQ+ contains unit risk values for arsenic, benzene, benzo[a]pyrene, chromium (VI), nickel, and vinyl chloride, allowing users to estimate cancer risks.
BenMAP—CE and AirQ+ have played leading roles in demonstrating the health and economic impacts of poor air quality, and directly contributed to the development of environmental actions to improve air quality. However, both tools continue to evolve, and institute features to expand upon their use and increase the sophistication of analyses than can be conducted. For example, AirQ+ is going through a new phase of development to increase its integration within WHO for all their ongoing air pollution activities, in particular for burden and impact analyses [
17]. AirQ+ undergoes continuous enhancements, mainly related to modifications that reflect the scientific advice from experts and the feedback received from users. This includes additional documents to clarify definitions and input of data, new user-friendly components for the calculation of DALYs and economic impacts, and additional examples of calculations. Additionally, efforts have been undertaken to increase the use of AirQ+ worldwide through the recent release of German and Spanish versions and an additional module for the economic assessment of air pollution, taking into account suggestions from expert consultations [
18]. BenMAP—CE continues to release updated versions of the tool with the most recent version released in March 2019, and ongoing efforts to institute new functionalities into the tool, such as the estimation of health impacts attributed to multipollutant exposures. Advancements in BenMAP—CE have been facilitated by the tool being an open source platform and the constant engagement with the user community through direct user feedback and the BenMAP—CE user forum (
https://forum.benmap.org). It is through the continued evolution of BenMAP—CE and AirQ+ and the institution of new and innovative features that both will continue to be at the forefront of research and policy efforts to estimate the public health impact of air pollution.

 ,
, 



{kind=link}
{kind=link}
{kind=link}