
Neuroprotection Is in the Air—Inhaled Gases on Their Way to the Neurons


Abstract
:
1. Introduction
2. Pathophysiology of Ischemia and Reperfusion Injury
3. Inhaled Gases Providing Protection against Neuronal Ischemia
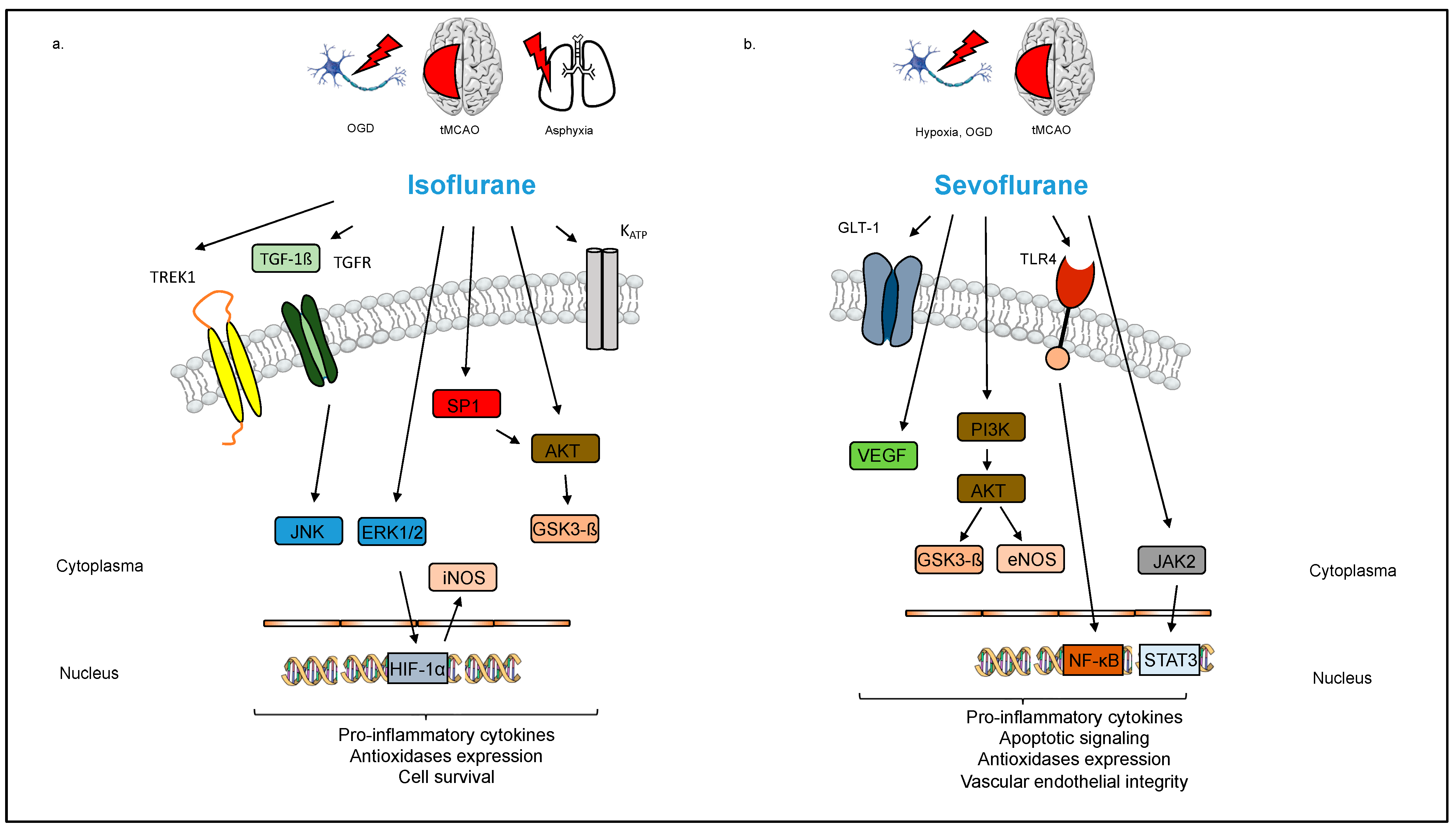
3.1. Volatile Anesthetics: Isoflurane, Sevoflurane, and Desflurane
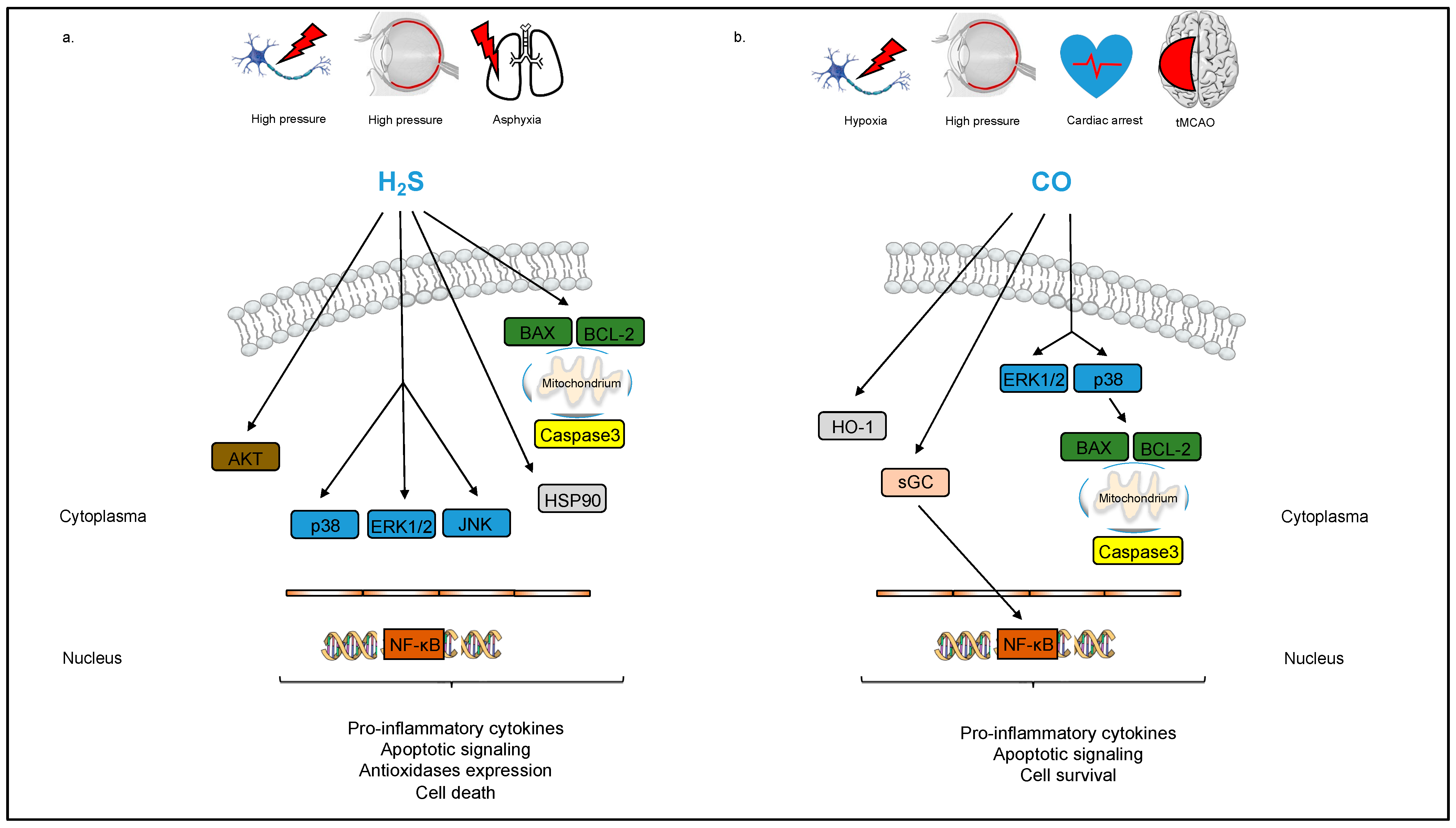
3.2. Gaseous Molecules
3.2.1. Hydrogen Sulfide (H2S)
3.2.2. Carbon Monoxide (CO)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance | Setting | Timing/Dosage | Mechanism | Publication |
|---|---|---|---|---|
| Sevoflurane | Neuronal glial cells (rat), OGD | 3.4 mM Sevo during ODG | Anti-excitotoxic properties | [30] |
| via GLT1, decrease in ROS | ||||
| MCAO (rat) | PrC, 2.7% Sevo/97% O2 | Activation of Akt, GSK3-ß | [33] | |
| (45 min) | phosphorylation | |||
| Hypoxia–ischemia brain | PoC, 2.5% Sevo/30% O2 | PI3K/Akt/eNOS, PI3K/Akt/ | [31] | |
| damage (rat) | (30 min) | GSK3-ß | ||
| Cerebral I/R (rat) | PoC, 2% Sevo/40% O2 | JAK-STAT pathway, | [34] | |
| (2 × 10 min) | reduction in apoptosis | |||
| MCAO (rat) | PoC, 2.5% Sevo (90 min) | Astrocyte protection, | [35] | |
| decrease in GFAP, | ||||
| neuro-, phosphoscan | ||||
| Hypoxia/reoxygenation | PoC, 2.5% Sevo/21% O2 | Endothelial barrier function | [28] | |
| in endothelial cells (rat) | (4 h) | (VEGF) | ||
| Cerebral I/R in rats | PoC, 2% Sevo (15 min) | TLR4/NF-ĸB | [25] | |
| Isoflurane | Focal cerebral ischemia (rat) | PrC, 2% Iso/98% O2 | KATP channel | [40] |
| (1 h/d for 5 d) | ||||
| Hippocampal neurons (rat), OGD | PoC, 2% Iso/95% air (1 h) | Erk1/2, HIF-1α, iNOS | [37] | |
| Neonatal hypoxia–ischemia (rat) | PoC, 2% Iso/30% O2 (1 h) | Sphingosine-1-phosphate/ | [43] | |
| PI3K/Akt pathway | ||||
| MCAO (rat) | PoC, 2% Iso (1 h) | Akt/GSK3-ß pathway | [45] | |
| Spinal cord ischemia (rat) | PrC, Iso 15 mL/L (1 h/d for 5 d) | TREK1 | [39] | |
| Cerebral I/R (rat) | PoC, 1.5% Iso/85% O2 (1 h) | JNK signaling pathway | [42] | |
| Desflurane | Perinatal hypoxic/ischemic brain injury (rat) | PoC, 4.8% Des (1 h) | TRPA1 | [48] |
| H2S | Retinal I/R injury (rat) Cellular neuronal injury (rat) Retinal I/R injury (rat) Retinal I/R injury (rat) | PrC, 80 ppm H2S (1 h) PrC, NaHS (30 min) PoC, 80 ppm H2S (1 h) PoC, 80 ppm H2S (1 h) | NF-ĸB, Erk1/2, JNK, HSP-90 PI3K/Akt/Nrf2, ROS reduction NF-ĸB, Akt, Bcl-2, Bax p38/Erk1/2 pathway | [71] [70] [72] [73] |
| CO | Hypoxia in neuronal cells (human) | PrC, CORM ALF186 (50 µmol/L) | sGC activation | [86] |
| Retinal I/R injury (rat) | PoC, CORM ALF186 (10 mg/kg) | p38, Erk1/2, Bax, Bcl-2 | [88] | |
| Retinal I/R injury (rat) | PoC, CORM ALF186 (10 mg/kg) | sGC, NF-ĸB, CREB | [87] | |
| tMCAO (mouse) | PoC, CORM-3 (4 mg/kg) | Iba-1, TNF-α, IL-1ß | [85] | |
| Cardiac arrest in pigs | CORM | Iba-1, Caspase-3, HO-1 | [89] | |
| Helium | Neonatal hypoxia–ischemia model (rat) Neonatal hypoxia–ischemia model (rat) Neonatal hypoxia–ischemia model (rat) | PrC, 70% He/30% O2 (3 × 5 min) PrC, 70% He/30% O2 (3 × 5 min) PrC, 70% He/30% O2 (3 × 5 min) | Inhibition of apoptosis iNOS, Nrf-2, SOD-1, HO-1 Inhibition of inflammation | [93] [94] [95] |
| Xenon | Patch-clamp recordings, cell culture Primary neuronal cell culture, OGD/ Hypoxic–ischemic injury (mouse) Patch-clamp recordings, cell culture tMCAO (mouse) | - PrC, 70% Xe/30% O2 (2 h) - PrC, 70% Xe/30% O2 (2 h) | Activation of TREK-1 BAX, BCL-2 Inhibition of NMDA receptor Increase in KATP currents HIF-1α | [96] [97] [98] [99] [100] |
| Argon | Retinal I/R injury (rat) | PoC, up to 75% Ar/21% O2 (1 h) | NF-ĸB, Caspase-3 | [101] |
| Cellular neuronal injury (human) | PoC, 75% Ar/21% O2 (1 h) | Erk1/2 | [102] | |
| Retinal I/R injury (rat) | PoC, 74% Ar/21% O2 (1 h) | TLR-2, TLR-4 | [103] | |
| Neuronal cell culture, neonatal hypoxia–ischemia brain injury (rat) | Cells: 75% Ar/20% O2 (2 h) Rats: 70% Ar/30% O2 (2 h) | HO-1, PI3K/Akt, NF-ĸB | [104] | |
| Retinal I/R injury (rat) Retinal I/R injury (rat) | PoC, 75% Ar/21% O2 (1 h) PoC, 75% Ar/21% O2 (1 h) | TLR-2, TLR-4, Interleukin-8 Cytokine reduction | [105] [106] |
3.3. Noble Gases
3.3.1. Neon
3.3.2. Helium
3.3.3. Xenon
3.3.4. Argon
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin, L.J. Neuronal cell death in nervous system development, disease, and injury (Review). Int. J. Mol. Med. 2001, 7, 455–478. [Google Scholar] [CrossRef] [PubMed]
- Sas, A.R.; Carbajal, K.S.; Jerome, A.D.; Menon, R.; Yoon, C.; Kalinski, A.L.; Giger, R.J.; Segal, B.M. A new neutrophil subset promotes CNS neuron survival and axon regeneration. Nat. Immunol. 2020, 21, 1496–1505. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Cronberg, T.; Sekhon, M. Brain injury after cardiac arrest: Pathophysiology, treatment, and prognosis. Intensiv. Care Med. 2021, 47, 1393–1414. [Google Scholar] [CrossRef]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef]
- O’Collins, V.E.; Macleod, M.R.; Donnan, G.A.; Horky, L.L.; van der Worp, B.H.; Howells, D.W. 1,026 Experimental treatments in acute stroke. Ann. Neurol. 2006, 59, 467–477. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensiv. Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]
- Gardner, A.J.; Menon, D.K. Moving to human trials for argon neuroprotection in neurological injury: A narrative review. Br. J. Anaesth. 2018, 120, 453–468. [Google Scholar] [CrossRef] [PubMed]
- Vats, K.; Sarmah, D.; Datta, A.; Saraf, J.; Kaur, H.; Pravalika, K.; Wanve, M.; Kalia, K.; Borah, A.; Dave, K.R.; et al. Intra-arterial Stem Cell Therapy Diminishes Inflammasome Activation After Ischemic Stroke: A Possible Role of Acid Sensing Ion Channel 1a. J. Mol. Neurosci. 2021, 71, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell biology of ischemia/reperfusion injury. Int. Rev. Cell Mol. Biol. 2012, 298, 229–317. [Google Scholar] [PubMed]
- Lai, T.W.; Zhang, S.; Wang, Y.T. Excitotoxicity and stroke: Identifying novel targets for neuroprotection. Prog. Neurobiol. 2014, 115, 157–188. [Google Scholar] [CrossRef]
- Dawson, L.A.; Djali, S.; Gonzales, C.; Vinegra, M.A.; Zaleska, M.M. Characterization of transient focal ischemia-induced increases in extracellular glutamate and aspartate in spontaneously hypertensive rats. Brain Res. Bull. 2000, 53, 767–776. [Google Scholar] [CrossRef]
- Jancsó, G.; Karcsú, S.; Király, E.; Szebeni, A.; Tóth, L.; Bácsy, E.; Joó, F.; Párducz, Á. Neurotoxin induced nerve cell degeneration: Possible involvement of calcium. Brain Res. 1984, 295, 211–216. [Google Scholar] [CrossRef]
- Li, J.; Yuan, J. Caspases in apoptosis and beyond. Oncogene 2008, 27, 6194–6206. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J. The immunology of stroke: From mechanisms to translation. Nat. Med. 2011, 17, 796–808. [Google Scholar] [CrossRef]
- De Meyer, S.F.; Denorme, F.; Langhauser, F.; Geuss, E.; Fluri, F.; Kleinschnitz, C. Thromboinflammation in Stroke Brain Damage. Stroke 2016, 47, 1165–1172. [Google Scholar] [CrossRef]
- Jayaraj, R.L.; Azimullah, S.; Beiram, R.; Jalal, F.Y.; Rosenberg, G.A. Neuroinflammation: Friend and foe for ischemic stroke. J. Neuroinflamm. 2019, 16, 142. [Google Scholar] [CrossRef]
- Nour, M.; Scalzo, F.; Liebeskind, D.S. Ischemia-Reperfusion Injury in Stroke. Interv. Neurol. 2013, 1, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef]
- McDonald, B.; Pittman, K.; Menezes, G.B.; Hirota, S.A.; Slaba, I.; Waterhouse, C.C.M.; Beck, P.L.; Muruve, D.A.; Kubes, P. Intravascular danger signals guide neutrophils to sites of sterile inflammation. Science 2010, 330, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Nader, N.D.; Li, C.M.; Khadra, W.Z.; Reedy, R.; Panos, A.L. Anesthetic myocardial protection with sevoflurane. J. Cardiothorac. Vasc. Anesth. 2004, 18, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.X.; Ding, Y.B.; Jin, F.Y.J.; Li, T.; Ma, J.H.; Qiao, L.Y.; Pan, W.Z.; Li, K.Z. Effects of sevoflurane post-conditioning in cerebral ischemia-reperfusion injury via TLR4/NF-kappaB pathway in rats. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1770–1775. [Google Scholar]
- Hwang, J.W.; Jeon, Y.T.; Lim, Y.J.; Park, H.P. Sevoflurane Postconditioning-Induced Anti-Inflammation via Inhibition of the Toll-Like Receptor-4/Nuclear Factor Kappa B Pathway Contributes to Neuroprotection against Transient Global Cerebral Ischemia in Rats. Int. J. Mol. Sci. 2017, 18, 2347. [Google Scholar] [CrossRef]
- Schallner, N.; Ulbrich, F.; Engelstaedter, H.; Biermann, J.; Auwaerter, V.; Loop, T.; Goebel, U. Isoflurane but not sevoflurane or desflurane aggravates injury to neurons in vitro and in vivo via p75NTR-NF-kB activation. Anesth. Analg. 2014, 119, 1429–1441. [Google Scholar] [CrossRef]
- Restin, T.; Kajdi, M.E.; Schläpfer, M.; Roth Z’graggen, B.; Booy, C.; Dumrese, C.; Beck-Schimmer, B. Sevoflurane protects rat brain endothelial barrier structure and function after hypoxia-reoxygenation injury. PLoS ONE 2017, 12, e0184973. [Google Scholar] [CrossRef]
- Beck-Schimmer, B.; Baumann, L.; Restin, T.; Eugster, P.; Hasler, M.; Booy, C.; Schläpfer, M. Sevoflurane attenuates systemic inflammation compared with propofol, but does not modulate neuro-inflammation: A laboratory rat study. Eur. J. Anaesthesiol. 2017, 34, 764–775. [Google Scholar] [CrossRef]
- Canas, P.T.; Velly, L.J.; Labrande, C.N.; Guillet, B.A.; Sautou-Miranda, V.; Masmejean, F.M.; Nieoullon, A.L.; Gouin, F.M.; Bruder, N.J.; Pisano, P.S. Sevoflurane protects rat mixed cerebrocortical neuronal–glial cell cultures against transient oxygen–glucose deprivation: Involvement of glutamate uptake and reactive oxygen species. Anesthesiology 2006, 105, 990–998. [Google Scholar] [CrossRef]
- Lai, Z.; Zhang, L.; Su, J.; Cai, D.; Xu, Q. Sevoflurane postconditioning improves long-term learning and memory of neonatal hypoxia-ischemia brain damage rats via the PI3K/Akt-mPTP pathway. Brain Res. 2016, 1630, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhou, X.; Yang, L.; Miao, X.; Lu, D.H.; Yang, X.Y.; Zhou, Z.B.; Kang, W.B.; Chen, K.Y.; Zhou, L.H.; et al. Neonatal Exposure to Low-Dose (1.2%) Sevoflurane Increases Rats’ Hippocampal Neurogenesis and Synaptic Plasticity in Later Life. Neurotox. Res. 2018, 34, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Nie, H.; Tian, L.; Tong, L.; Deng, J.; Zhang, Y.; Dong, H.; Xiong, L. Sevoflurane preconditioning-induced neuroprotection is associated with Akt activation via carboxy-terminal modulator protein inhibition. Br. J. Anaesth. 2015, 114, 327–335. [Google Scholar] [CrossRef]
- Kim, H.-C.; Kim, E.; Bae, J.I.; Lee, K.H.; Jeon, Y.-T.; Hwang, J.-W.; Lim, Y.-J.; Min, S.-W.; Park, H.-P. Sevoflurane Postconditioning Reduces Apoptosis by Activating the JAK-STAT Pathway After Transient Global Cerebral Ischemia in Rats. J. Neurosurg. Anesthesiol. 2017, 29, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.-M.; Gao, X.; Ni, Y.; Li, W.; Kent, T.A.; Qiao, S.-G.; Wang, C.; Xu, X.-X.; Zhang, H.-L. Sevoflurane postconditioning attenuates reactive astrogliosis and glial scar formation after ischemia–reperfusion brain injury. Neuroscience 2017, 356, 125–141. [Google Scholar] [CrossRef]
- Edwards, D.A.; Shah, H.P.; Cao, W.; Gravenstein, N.; Seubert, C.N.; Martynyuk, A.E. Bumetanide alleviates epileptogenic and neurotoxic effects of sevoflurane in neonatal rat brain. Anesthesiology 2010, 112, 567–575. [Google Scholar] [CrossRef]
- Li, Q.F.; Zhu, Y.S.; Jiang, H. Isoflurane preconditioning activates HIF-1alpha, iNOS and Erk1/2 and protects against oxygen-glucose deprivation neuronal injury. Brain Res. 2008, 1245, 26–35. [Google Scholar] [CrossRef]
- Jung, F.; Palmer, L.A.; Zhou, N.; Johns, R.A. Hypoxic Regulation of Inducible Nitric Oxide Synthase via Hypoxia Inducible Factor-1 in Cardiac Myocytes. Circ. Res. 2000, 86, 319–325. [Google Scholar] [CrossRef]
- Wang, K.; Kong, X. Isoflurane Preconditioning Induces Neuroprotection by Up-Regulation of TREK1 in a Rat Model of Spinal Cord Ischemic Injury. Biomol. Ther. 2016, 24, 495–500. [Google Scholar] [CrossRef]
- Xiong, L.; Zheng, Y.; Wu, M.; Hou, L.; Zhu, Z.; Zhang, X.; Lu, Z. Preconditioning with isoflurane produces dose-dependent neuroprotection via activation of adenosine triphosphate-regulated potassium channels after focal cerebral ischemia in rats. Anesth. Analg. 2003, 96, 233–237. [Google Scholar] [CrossRef]
- Xu, X.; Kim, J.A.; Zuo, Z. Isoflurane preconditioning reduces mouse microglial activation and injury induced by lipopolysaccharide and interferon-gamma. Neuroscience 2008, 154, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yin, J.; Ge, M.; Dai, Z.; Li, Y.; Si, J.; Ma, K.; Li, L.; Yao, S. Transforming growth-beta 1 contributes to isoflurane postconditioning against cerebral ischemia-reperfusion injury by regulating the c-Jun N-terminal kinase signaling pathway. Biomed. Pharmacother. 2016, 78, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Lekic, T.; Fathali, N.; Ostrowski, R.P.; Martin, R.D.; Tang, J.; Zhang, J.H. Isoflurane Posttreatment Reduces Neonatal Hypoxic-Ischemic Brain Injury in Rats by the Sphingosine-1-Phosphate/Phosphatidylinositol-3-Kinase/Akt Pathway. Stroke 2010, 41, 1521–1527. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, G.; Galluzzi, L.; Brenner, C. Mitochondrial Membrane Permeabilization in Cell Death. Physiol. Rev. 2007, 87, 99–163. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zuo, Z. Isoflurane postconditioning induces neuroprotection via Akt activation and attenuation of increased mitochondrial membrane permeability. Neuroscience 2011, 199, 44–50. [Google Scholar] [CrossRef]
- Haelewyn, B.; Yvon, A.; Hanouz, J.L.; MacKenzie, E.T.; Ducouret, P.; Gerard, J.L.; Roussel, S. Desflurane affords greater protection than halothane against focal cerebral ischaemia in the rat. Br. J. Anaesth. 2003, 91, 390–396. [Google Scholar] [CrossRef]
- Tsai, S.-K.; Lin, S.-M.; Hung, W.-C.; Mok, M.S.; Chih, C.-L.; Huang, S.-S. The effect of desflurane on ameliorating cerebral infarction in rats subjected to focal cerebral ischemia-reperfusion injury. Life Sci. 2004, 74, 2541–2549. [Google Scholar] [CrossRef]
- Zhou, T.; Li, J.; Cheng, A.; Zuo, Z. Desflurane Post-treatment Reduces Hypoxic-ischemic Brain Injury via Reducing Transient Receptor Potential Ankyrin 1 in Neonatal Rats. Neuroscience 2023, 522, 121–131. [Google Scholar] [CrossRef]
- Garcia-Anoveros, J.; Nagata, K. Trpa1. Handb. Exp. Pharmacol. 2007, 179, 347–362. [Google Scholar]
- McAuliffe, J.J.; Loepke, A.W.; Miles, L.; Joseph, B.; Hughes, E.; Vorhees, C.V. Desflurane, Isoflurane, and Sevoflurane Provide Limited Neuroprotection against Neonatal Hypoxia-Ischemia in a Delayed Preconditioning Paradigm. Anesthesiology 2009, 111, 533–546. [Google Scholar] [CrossRef]
- Jayaraman, K.; Liu, M.; Zipfel, G.J.; Athiraman, U. Sevoflurane and Desflurane Exposures Following Aneurysmal Subarachnoid Hemorrhage Confer Multifaceted Protection against Delayed Cerebral Ischemia. Biomedicines 2021, 9, 820. [Google Scholar] [CrossRef] [PubMed]
- Diprose, W.K.; Wang, M.T.M.; Campbell, D.; Sutcliffe, J.A.; McFetridge, A.; Chiou, D.; Lai, J.; Barber, P.A. Intravenous Propofol Versus Volatile Anesthetics For Stroke Endovascular Thrombectomy. J. Neurosurg. Anesthesiol. 2021, 33, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Schoen, J.; Husemann, L.; Tiemeyer, C.; Lueloh, A.; Sedemund-Adib, B.; Berger, K.-U.; Hueppe, M.; Heringlake, M. Cognitive function after sevoflurane- vs propofol-based anaesthesia for on-pump cardiac surgery: A randomized controlled trial. Br. J. Anaesth. 2011, 106, 840–850. [Google Scholar] [CrossRef]
- Kuzkov, V.V.; Obraztsov, M.Y.; Ivashchenko, O.Y.; Ivashchenko, N.Y.; Gorenkov, V.M.; Kirov, M.Y. Total Intravenous Versus Volatile Induction and Maintenance of Anesthesia in Elective Carotid Endarterectomy: Effects on Cerebral Oxygenation and Cognitive Functions. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1701–1708. [Google Scholar] [CrossRef]
- Landoni, G.; Lomivorotov, V.V.; Neto, C.N.; Monaco, F.; Pasyuga, V.V.; Bradic, N.; Lembo, R.; Gazivoda, G.; Likhvantsev, V.V.; Lei, C.; et al. Volatile Anesthetics versus Total Intravenous Anesthesia for Cardiac Surgery. N. Engl. J. Med. 2019, 380, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Raub, D.; Platzbecker, K.; Grabitz, S.D.; Xu, X.; Wongtangman, K.; Pham, S.B.; Murugappan, K.R.; Hanafy, K.A.; Nozari, A.; Houle, T.T.; et al. Effects of Volatile Anesthetics on Postoperative Ischemic Stroke Incidence. J. Am. Hear. Assoc. 2021, 10, e018952. [Google Scholar] [CrossRef]
- Lee, J.W.; Woo, J.H.; Baik, H.J.; Kim, D.Y.; Chae, J.S.; Yang, N.R.; Seo, E.K. The effect of anesthetic agents on cerebral vasospasms after subarachnoid hemorrhage: A retrospective study. Medicine 2018, 97, e11666. [Google Scholar] [CrossRef]
- Athiraman, U.; Aum, D.; Vellimana, A.K.; Osbun, J.W.; Dhar, R.; Tempelhoff, R.; Zipfel, G.J. Evidence for a conditioning effect of inhalational anesthetics on angiographic vasospasm after aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2019, 1–7. [Google Scholar] [CrossRef]
- Varughese, S.; Ahmed, R. Environmental and Occupational Considerations of Anesthesia: A Narrative Review and Update. Anesth. Analg. 2021, 133, 826–835. [Google Scholar] [CrossRef]
- Gaya da Costa, M.; Kalmar, A.F.; Struys, M. Inhaled Anesthetics: Environmental Role, Occupational Risk, and Clinical Use. J. Clin. Med. 2021, 10, 1306. [Google Scholar] [CrossRef]
- Wallace, J.L.; Wang, R. Hydrogen sulfide-based therapeutics: Exploiting a unique but ubiquitous gasotransmitter. Nat. Rev. Drug Discov. 2015, 14, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.D.; Snyder, S.H. H2S: A Novel Gasotransmitter that Signals by Sulfhydration. Trends Biochem. Sci. 2015, 40, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.D.; Snyder, S.H. Modes of Physiologic H2S Signaling in the Brain and Peripheral Tissues. Antioxid. Redox Signal. 2015, 22, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Kimura, H. Hydrogen sulfide protects neurons from oxidative stress. FASEB J. 2004, 18, 1165–1167. [Google Scholar] [CrossRef]
- Kimura, Y.; Goto, Y.-I.; Kimura, H. Hydrogen Sulfide Increases Glutathione Production and Suppresses Oxidative Stress in Mitochondria. Antioxid. Redox Signal. 2010, 12, 1–13. [Google Scholar] [CrossRef]
- Florian, B.; Vintilescu, R.; Balseanu, A.T.; Buga, A.-M.; Grisk, O.; Walker, L.C.; Kessler, C.; Popa-Wagner, A. Long-term hypothermia reduces infarct volume in aged rats after focal ischemia. Neurosci. Lett. 2008, 438, 180–185. [Google Scholar] [CrossRef]
- Wang, Y.; Jia, J.; Ao, G.; Hu, L.; Liu, H.; Xiao, Y.; Du, H.; Alkayed, N.J.; Liu, C.; Cheng, J. Hydrogen sulfide protects blood–brain barrier integrity following cerebral ischemia. J. Neurochem. 2014, 129, 827–838. [Google Scholar] [CrossRef]
- Liu, H.; Wang, Y.; Xiao, Y.; Hua, Z.; Cheng, J.; Jia, J. Hydrogen Sulfide Attenuates Tissue Plasminogen Activator-Induced Cerebral Hemorrhage Following Experimental Stroke. Transl. Stroke Res. 2016, 7, 209–219. [Google Scholar] [CrossRef]
- Qu, K.; Chen, C.P.L.; Halliwell, B.; Moore, P.K.; Wong, P.T.H. Hydrogen sulfide is a mediator of cerebral ischemic damage. Stroke 2006, 37, 889–893. [Google Scholar] [CrossRef]
- Zhang, J.; Shan, H.; Tao, L.; Zhang, M. Biological Effects of Hydrogen Sulfide and Its Protective Role in Intracerebral Hemorrhage. J. Mol. Neurosci. 2020, 70, 2020–2030. [Google Scholar] [CrossRef]
- Biermann, J.; Lagrèze, W.A.; Schallner, N.; Schwer, C.I.; Goebel, U. Inhalative preconditioning with hydrogen sulfide attenuated apoptosis after retinal ischemia/reperfusion injury. Mol. Vis. 2011, 17, 1275–1286. [Google Scholar] [PubMed]
- Scheid, S.; Goeller, M.; Baar, W.; Wollborn, J.; Buerkle, H.; Schlunck, G.; Lagrèze, W.; Goebel, U.; Ulbrich, F. Hydrogen Sulfide Reduces Ischemia and Reperfusion Injury in Neuronal Cells in a Dose- and Time-Dependent Manner. Int. J. Mol. Sci. 2021, 22, 10099. [Google Scholar] [CrossRef] [PubMed]
- Scheid, S.; Goeller, M.; Baar, W.; Wollborn, J.; Buerkle, H.; Schlunck, G.; Lagrèze, W.; Goebel, U.; Ulbrich, F. Inhalative as well as Intravenous Administration of H2S Provides Neuroprotection after Ischemia and Reperfusion Injury in the Rats’ Retina. Int. J. Mol. Sci. 2022, 23, 5519. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Wang, L.; Liu, G.; Wang, S.; Wang, Y.; Wu, Y.; Wang, J.; Sun, X. Role of hydrogen sulfide in subarachnoid hemorrhage. CNS Neurosci. Ther. 2022, 28, 805–817. [Google Scholar] [CrossRef]
- Otterbein, L.E.; Bach, F.H.; Alam, J.; Soares, M.; Lu, H.T.; Wysk, M.; Davis, R.J.; Flavell, R.A.; Choi, A.M. Carbon monoxide has anti-inflammatory effects involving the mitogen-activated protein kinase pathway. Nat. Med. 2000, 6, 422–428. [Google Scholar] [CrossRef]
- Brouard, S.; Otterbein, L.E.; Anrather, J.; Tobiasch, E.; Bach, F.H.; Choi, A.M.; Soares, M.P. Carbon Monoxide Generated by Heme Oxygenase 1 Suppresses Endothelial Cell Apoptosis. J. Exp. Med. 2000, 192, 1015–1026. [Google Scholar] [CrossRef]
- Ryter, S.W.; Otterbein, L.E. Carbon monoxide in biology and medicine. BioEssays 2004, 26, 270–280. [Google Scholar] [CrossRef]
- Dore, S.; Sampei, K.; Goto, S.; Alkayed, N.J.; Guastella, D.; Blackshaw, S.; Gallagher, M.; Traystman, R.J.; Hurn, P.D.; Koehler, R.C.; et al. Heme oxygenase-2 is neuroprotective in cerebral ischemia. Mol. Med. 1999, 5, 656–663. [Google Scholar] [CrossRef]
- Imuta, N.; Hori, O.; Kitao, Y.; Tabata, Y.; Yoshimoto, T.; Matsuyama, T.; Ogawa, S.; Choi, Y.K.; Kim, J.-H.; Lee, D.-K.; et al. Hypoxia-Mediated Induction of Heme Oxygenase Type I and Carbon Monoxide Release from Astrocytes Protects Nearby Cerebral Neurons from Hypoxia-Mediated Apoptosis. Antioxid. Redox Signal. 2007, 9, 543–552. [Google Scholar] [CrossRef]
- Zeynalov, E.; Doré, S. Low Doses of Carbon Monoxide Protect Against Experimental Focal Brain Ischemia. Neurotox. Res. 2009, 15, 133–137. [Google Scholar] [CrossRef]
- Schallner, N.; Pandit, R.; LeBlanc, R.; Thomas, A.J.; Ogilvy, C.S.; Zuckerbraun, B.S.; Gallo, D.; Otterbein, L.E.; Hanafy, K.A. Microglia regulate blood clearance in subarachnoid hemorrhage by heme oxygenase-1. J. Clin. Investig. 2015, 125, 2609–2625. [Google Scholar] [CrossRef] [PubMed]
- Queiroga, C.S.F.; Vercelli, A.; Vieira, H.L.A. Carbon monoxide and the CNS: Challenges and achievements. Br. J. Pharmacol. 2015, 172, 1533–1545. [Google Scholar] [CrossRef] [PubMed]
- Motterlini, R.; Otterbein, L.E. The therapeutic potential of carbon monoxide. Nat. Rev. Drug Discov. 2010, 9, 728–743. [Google Scholar] [CrossRef] [PubMed]
- Schatzschneider, U. Novel lead structures and activation mechanisms for CO-releasing molecules (CORMs). Br. J. Pharmacol. 2015, 172, 1638–1650. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, D.; Fu, X.; Yu, L.; Lu, Z.; Gao, Y.; Liu, X.; Man, J.; Li, S.; Li, N.; et al. Carbon monoxide-releasing molecule-3 protects against ischemic stroke by suppressing neuroinflammation and alleviating blood-brain barrier disruption. J. Neuroinflammation 2018, 15, 188. [Google Scholar] [CrossRef]
- Schallner, N.; Romão, C.C.; Biermann, J.; Lagrèze, W.A.; Otterbein, L.E.; Buerkle, H.; Loop, T.; Goebel, U. Carbon monoxide abrogates ischemic insult to neuronal cells via the soluble guanylate cyclase-cGMP pathway. PLoS ONE 2013, 8, e60672. [Google Scholar] [CrossRef]
- Ulbrich, F.; Hagmann, C.; Buerkle, H.; Romao, C.C.; Schallner, N.; Goebel, U.; Biermann, J. The Carbon monoxide releasing molecule ALF-186 mediates anti-inflammatory and neuroprotective effects via the soluble guanylate cyclase ss1 in rats’ retinal ganglion cells after ischemia and reperfusion injury. J. Neuroinflammation 2017, 14, 130. [Google Scholar] [CrossRef]
- Ulbrich, F.; Kaufmann, K.B.; Meske, A.; Lagrèze, W.A.; Augustynik, M.; Buerkle, H.; Ramao, C.C.; Biermann, J.; Goebel, U. The CORM ALF-186 Mediates Anti-Apoptotic Signaling via an Activation of the p38 MAPK after Ischemia and Reperfusion Injury in Retinal Ganglion Cells. PLoS ONE 2016, 11, e0165182. [Google Scholar] [CrossRef]
- Wollborn, J.; Steiger, C.D.R.N.; Doostkam, S.; Schallner, N.; Schroeter, N.; Kari, F.A.; Meinel, L.D.R.N.; Buerkle, H.; Schick, M.A.; Goebel, U. Carbon Monoxide Exerts Functional Neuroprotection After Cardiac Arrest Using Extracorporeal Resuscitation in Pigs. Crit. Care Med. 2020, 48, e299–e307. [Google Scholar] [CrossRef]
- Goebel, U.; Wollborn, J. Carbon monoxide in intensive care medicine-time to start the therapeutic application?! Intensive Care Med. Exp. 2020, 8, 2. [Google Scholar] [CrossRef]
- Mayr, F.B.; Spiel, A.; Leitner, J.; Marsik, C.; Germann, P.; Ullrich, R.; Wagner, O.; Jilma, B. Effects of Carbon Monoxide Inhalation during Experimental Endotoxemia in Humans. Am. J. Respir. Crit. Care Med. 2005, 171, 354–360. [Google Scholar] [CrossRef]
- Bathoorn, E.; Slebos, D.-J.; Postma, D.S.; Koeter, G.H.; van Oosterhout, A.J.M.; van der Toorn, M.; Boezen, H.M.; Kerstjens, H.A.M. Anti-inflammatory effects of inhaled carbon monoxide in patients with COPD: A pilot study. Eur. Respir. J. 2007, 30, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xue, F.; Liu, G.; Shi, X.; Liu, Y.; Liu, W.; Luo, X.; Sun, X.; Kang, Z. Helium preconditioning attenuates hypoxia/ischemia-induced injury in the developing brain. Brain Res. 2011, 1376, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, K.; Kang, Z.M.; Sun, X.J.; Liu, W.W.; Mao, Y.F. Helium preconditioning protects against neonatal hypoxia-ischemia via nitric oxide mediated up-regulation of antioxidases in a rat model. Behav. Brain Res. 2016, 300, 31–37. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, P.; Liu, Y.; Liu, W.; Yin, N. Helium preconditioning protects the brain against hypoxia/ischemia injury via improving the neurovascular niche in a neonatal rat model. Behav. Brain Res. 2016, 314, 165–172. [Google Scholar] [CrossRef]
- Heurteaux, C.; Guy, N.; Laigle, C.; Blondeau, N.; Duprat, F.; Mazzuca, M.; Lang-Lazdunski, L.; Widmann, C.; Zanzouri, M.; Romey, G.; et al. TREK-1, a K+ channel involved in neuroprotection and general anesthesia. EMBO J. 2004, 23, 2684–2695. [Google Scholar] [CrossRef]
- Ma, D.; Hossain, M.; Chow, A.; Arshad, M.; Battson, R.M.; Sanders, R.D.; Mehmet, H.; Edwards, A.D.; Franks, N.P.; Maze, M. Xenon and hypothermia combine to provide neuroprotection from neonatal asphyxia. Ann. Neurol. 2005, 58, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, R.; Peterson, B.K.; Banks, P.; Simillis, C.; Martin, J.C.S.; Valenzuela, C.A.; Maze, M.; Franks, N.P. Competitive inhibition at the glycine site of the N-methyl-D-aspartate receptor by the anesthetics xenon and isoflurane: Evidence from molecular modeling and electrophysiology. Anesthesiology 2007, 107, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Bantel, C.; Maze, M.; Trapp, S. Noble gas xenon is a novel adenosine triphosphate-sensitive potassium channel opener. Anesthesiology 2010, 112, 623–630. [Google Scholar] [CrossRef]
- Limatola, V.; Ward, P.; Cattano, D.; Gu, J.; Giunta, F.; Maze, M.; Ma, D. Xenon preconditioning confers neuroprotection regardless of gender in a mouse model of transient middle cerebral artery occlusion. Neuroscience 2010, 165, 874–881. [Google Scholar] [CrossRef]
- Ulbrich, F.; Schallner, N.; Coburn, M.; Loop, T.; Lagrèze, W.A.; Biermann, J.; Goebel, U. Argon Inhalation Attenuates Retinal Apoptosis after Ischemia/Reperfusion Injury in a Time- and Dose-Dependent Manner in Rats. PLoS ONE 2014, 9, e115984. [Google Scholar] [CrossRef] [PubMed]
- Ulbrich, F.; Kaufmann, K.B.; Coburn, M.; Lagrèze, W.A.; Roesslein, M.; Biermann, J.; Buerkle, H.; Loop, T.; Goebel, U. Neuroprotective effects of Argon are mediated via an ERK-1/2 dependent regulation of heme-oxygenase-1 in retinal ganglion cells. J. Neurochem. 2015, 134, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Ulbrich, F.; Kaufmann, K.; Roesslein, M.; Wellner, F.; Auwärter, V.; Kempf, J.; Loop, T.; Buerkle, H.; Goebel, U. Argon Mediates Anti-Apoptotic Signaling and Neuroprotection via Inhibition of Toll-Like Receptor 2 and 4. PLoS ONE 2015, 10, e0143887. [Google Scholar] [CrossRef]
- Zhao, H.; Mitchell, S.; Koumpa, S.; Cui, Y.T.; Lian, Q.; Hagberg, H.; Johnson, M.R.; Takata, M.; Ma, D. Heme Oxygenase-1 Mediates Neuroprotection Conferred by Argon in Combination with Hypothermia in Neonatal Hypoxia–Ischemia Brain Injury. Anesthesiology 2016, 125, 180–192. [Google Scholar] [CrossRef]
- Ulbrich, F.; Lerach, T.; Biermann, J.; Kaufmann, K.B.; Lagreze, W.A.; Buerkle, H.; Loop, T.; Goebel, U. Argon mediates protection by interleukin-8 suppression via a TLR2/TLR4/STAT3/NF-κB pathway in a model of apoptosis in neuroblastoma cells in vitro and following ischemia-reperfusion injury in rat retina in vivo. J. Neurochem. 2016, 138, 859–873. [Google Scholar] [CrossRef]
- Goebel, U.; Scheid, S.; Spassov, S.; Schallner, N.; Wollborn, J.; Buerkle, H.; Ulbrich, F. Argon reduces microglial activation and inflammatory cytokine expression in retinal ischemia/reperfusion injury. Neural Regen. Res. 2021, 16, 192–198. [Google Scholar]
- Pagel, P.S.; Krolikowski, J.G.; Shim, Y.H.; Venkatapuram, S.; Kersten, J.R.; Weihrauch, D.; Warltier, D.C.; Pratt, P.F., Jr. Noble gases without anesthetic properties protect myocardium against infarction by activating prosurvival signaling kinases and inhibiting mitochondrial permeability transition in vivo. Anesth. Analg. 2007, 105, 562–569. [Google Scholar] [CrossRef]
- Harris, K.; Armstrong, S.P.; Campos-Pires, R.; Kiru, L.; Franks, N.P.; Dickinson, R. Neuroprotection against traumatic brain injury by xenon, but not argon, is mediated by inhibition at the N-methyl-D-aspartate receptor glycine site. Anesthesiology 2013, 119, 1137–1148. [Google Scholar] [CrossRef]
- Jawad, N.; Rizvi, M.; Gu, J.; Adeyi, O.; Tao, G.; Maze, M.; Ma, D. Neuroprotection (and lack of neuroprotection) afforded by a series of noble gases in an in vitro model of neuronal injury. Neurosci. Lett. 2009, 460, 232–236. [Google Scholar] [CrossRef]
- Koziakova, M.; Harris, K.; Edge, C.J.; Franks, N.P.; White, I.L.; Dickinson, R. Noble gas neuroprotection: Xenon and argon protect against hypoxic–ischaemic injury in rat hippocampus in vitro via distinct mechanisms. Br. J. Anaesth. 2019, 123, 601–609. [Google Scholar] [CrossRef]
- Wu, X.; Shao, C.; Zhang, L.; Tu, J.; Xu, H.; Lin, Z.; Xu, S.; Yu, B.; Tang, Y.; Li, S. The effect of helium-oxygen-assisted mechanical ventilation on chronic obstructive pulmonary disease exacerbation: A systemic review and meta-analysis. Clin. Respir. J. 2018, 12, 1219–1227. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.; Chen, Z.; Zhao, H.; Huang, H.; Liu, W. Noble gas and neuroprotection: From bench to bedside. Front. Pharmacol. 2022, 13, 1028688. [Google Scholar] [CrossRef]
- Aehling, C.; Weber, N.C.; Zuurbier, C.J.; Preckel, B.; Galmbacher, R.; Stefan, K.; Hollmann, M.W.; Popp, E.; Knapp, J. Effects of combined helium pre/post-conditioning on the brain and heart in a rat resuscitation model. Acta Anaesthesiol. Scand. 2018, 62, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Zhang, H.; VanDeripe, D.R.; Cruz-Flores, S.; Panneton, W.M. Heliox and oxygen reduce infarct volume in a rat model of focal ischemia. Exp. Neurol. 2007, 205, 587–590. [Google Scholar] [CrossRef]
- Zuercher, P.; Springe, D.; Grandgirard, D.; Leib, S.L.; Grossholz, M.; Jakob, S.; Takala, J.; Haenggi, M. A randomized trial of the effects of the noble gases helium and argon on neuroprotection in a rodent cardiac arrest model. BMC Neurol. 2016, 16, 43. [Google Scholar] [CrossRef]
- Banks, P.; Franks, N.P.; Dickinson, R. Competitive Inhibition at the Glycine Site of the N -Methyl-d-Aspartate Receptor Mediates Xenon Neuroprotection against Hypoxia–Ischemia. Anesthesiology 2010, 112, 614–622. [Google Scholar] [CrossRef]
- Coburn, M.; Baumert, J.-H.; Roertgen, D.; Thiel, V.; Fries, M.; Hein, M.; Kunitz, O.; Fimm, B.; Rossaint, R. Emergence and early cognitive function in the elderly after xenon or desflurane anaesthesia: A double-blinded randomized controlled trial. Br. J. Anaesth. 2007, 98, 756–762. [Google Scholar] [CrossRef]
- Schäfer, P.; Fahlenkamp, A.; Rossaint, R.; Coburn, M.; Kowark, A. Better haemodynamic stability under xenon anaesthesia than under isoflurane anaesthesia during partial nephrectomy—A secondary analysis of a randomised controlled trial. BMC Anesthesiol. 2019, 19, 125. [Google Scholar] [CrossRef]
- Chakkarapani, E.; Dingley, J.; Liu, X.; Hoque, N.; Aquilina, K.; Porter, H.; Thoresen, M. Xenon enhances hypothermic neuroprotection in asphyxiated newborn pigs. Ann. Neurol. 2010, 68, 330–341. [Google Scholar] [CrossRef]
- Fries, M.; Brücken, A.; Çizen, A.; Westerkamp, M.; Löwer, C.; Deike-Glindemann, J.; Schnorrenberger, N.K.; Rex, S.; Coburn, M.; Nolte, K.W.; et al. Combining xenon and mild therapeutic hypothermia preserves neurological function after prolonged cardiac arrest in pigs. Crit. Care Med. 2012, 40, 1297–1303. [Google Scholar] [CrossRef]
- Arola, O.J.; Laitio, R.M.; Roine, R.O.; Grönlund, J.; Saraste, A.; Pietilä, M.; Airaksinen, J.; Perttilä, J.; Scheinin, H.; Olkkola, K.T.; et al. Feasibility and Cardiac Safety of Inhaled Xenon in Combination With Therapeutic Hypothermia Following Out-of-Hospital Cardiac Arrest. Crit. Care Med. 2013, 41, 2116–2124. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, D.; Robertson, N.J.; Bainbridge, A.; Cady, E.; Charles-Edwards, G.; Deierl, A.; Fagiolo, G.; Franks, N.P.; Griffiths, J.; Hajnal, J.; et al. Moderate hypothermia within 6 h of birth plus inhaled xenon versus moderate hypothermia alone after birth asphyxia (TOBY-Xe): A proof-of-concept, open-label, randomised controlled trial. Lancet Neurol. 2016, 15, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Koskensalo, K.; Virtanen, S.; Saunavaara, J.; Parkkola, R.; Laitio, R.; Arola, O.; Hynninen, M.; Silvasti, P.; Nukarinen, E.; Martola, J.; et al. Comparison of the prognostic value of early-phase proton magnetic resonance spectroscopy and diffusion tensor imaging with serum neuron-specific enolase at 72 h in comatose survivors of out-of-hospital cardiac arrest—A substudy of the XeHypotheca trial. Neuroradiology 2023, 65, 349–360. [Google Scholar] [CrossRef]
- Law, L.S.; Lo, E.A.; Gan, T.J. Xenon Anesthesia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Anesth. Analg. 2016, 122, 678–697. [Google Scholar] [CrossRef]
- Suzuki, T.; Koyama, H.; Sugimoto, M.; Uchida, I.; Mashimo, T. The Diverse Actions of Volatile and Gaseous Anesthetics on Human-cloned 5-Hydroxytryptamine3Receptors Expressed in Xenopus Oocytes. Anesthesiology 2002, 96, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Campos-Pires, R.; Armstrong, S.P.; Sebastiani, A.; Luh, C.; Gruss, M.; Radyushkin, K.; Hirnet, T.; Werner, C.; Engelhard, K.; Franks, N.P.; et al. Xenon Improves Neurologic Outcome and Reduces Secondary Injury Following Trauma in an In Vivo Model of Traumatic Brain Injury. Crit. Care Med. 2015, 43, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Chu, D.; Li, L.; Creed, J.A.; Ryang, Y.-M.; Sheng, H.; Yang, W.; Warner, D.S.; Turner, D.A.; Hoffmann, U. Argon Inhalation for 24 Hours After Onset of Permanent Focal Cerebral Ischemia in Rats Provides Neuroprotection and Improves Neurologic Outcome. Crit. Care Med. 2019, 47, e693–e699. [Google Scholar] [CrossRef]
- Fumagalli, F.; Olivari, D.; Boccardo, A.; De Giorgio, D.; Affatato, R.; Ceriani, S.; Bariselli, S.; Sala, G.; Cucino, A.; Zani, D.; et al. Ventilation With Argon Improves Survival With Good Neurological Recovery After Prolonged Untreated Cardiac Arrest in Pigs. J. Am. Hear. Assoc. 2020, 9, e016494. [Google Scholar] [CrossRef]
- Ulbrich, F.; Goebel, U. Argon: A novel therapeutic option to treat neuronal ischemia and reperfusion injuries? Neural Regen. Res. 2015, 10, 1043–1044. [Google Scholar]
- Ulbrich, F.; Goebel, U. The Molecular Pathway of Argon-Mediated Neuroprotection. Int. J. Mol. Sci. 2016, 17, 1816. [Google Scholar] [CrossRef]
- Zhao, H.; Mitchell, S.; Ciechanowicz, S.; Savage, S.; Wang, T.; Ji, X.; Ma, D. Argon protects against hypoxic-ischemic brain injury in neonatal rats through activation of nuclear factor (erythroid-derived 2)-like 2. Oncotarget 2016, 7, 25640–25641. [Google Scholar] [CrossRef]
- Scheid, S.; Lejarre, A.; Wollborn, J.; Buerkle, H.; Goebel, U.; Ulbrich, F. Argon preconditioning protects neuronal cells with a Toll-like receptor-mediated effect. Neural Regen. Res. 2023, 18, 1371–1377. [Google Scholar] [PubMed]
- Kiss, A.; Shu, H.; Hamza, O.; Santer, D.; Tretter, E.V.; Yao, S.; Markstaller, K.; Hallström, S.; Podesser, B.K.; Klein, K.U. Argon preconditioning enhances postischaemic cardiac functional recovery following cardioplegic arrest and global cold ischaemia. Eur. J. Cardio-Thorac. Surg. 2018, 54, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Alderliesten, T.; Favie, L.M.A.; Neijzen, R.W.; Auwärter, V.; Nijboer, C.H.A.; Marges, R.E.J.; Rademaker, C.M.A.; Kempf, J.; van Bel, F.; Groenendaal, F. Neuroprotection by Argon Ventilation after Perinatal Asphyxia: A Safety Study in Newborn Piglets. PLoS ONE 2014, 9, e113575. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, D.M.; Saunders, C.J.; Ho, H.S.; Wolfe, B.M. Hemodynamic effects of argon pneumoperitoneum. Surg. Endosc. 1994, 8, 315–320, discussion 320–321. [Google Scholar] [CrossRef]
- Junghans, T.; Böhm, B.; Gründel, K.; Schwenk, W. Effects of pneumoperitoneum with carbon dioxide, argon, or helium on hemodynamic and respiratory function. Arch. Surg. 1997, 132, 272–278. [Google Scholar] [CrossRef]
- Shulagin, I.A.; D’iachenko, A.I.; Pavlov, B.N. Effect of argon on oxygen consumption during physical load under hypoxic conditions in humans. Fiziol. Cheloveka 2001, 27, 95–101. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheid, S.; Goebel, U.; Ulbrich, F. Neuroprotection Is in the Air—Inhaled Gases on Their Way to the Neurons. Cells 2023, 12, 2480. https://doi.org/10.3390/cells12202480
Scheid S, Goebel U, Ulbrich F. Neuroprotection Is in the Air—Inhaled Gases on Their Way to the Neurons. Cells. 2023; 12(20):2480. https://doi.org/10.3390/cells12202480
Chicago/Turabian StyleScheid, Stefanie, Ulrich Goebel, and Felix Ulbrich. 2023. "Neuroprotection Is in the Air—Inhaled Gases on Their Way to the Neurons" Cells 12, no. 20: 2480. https://doi.org/10.3390/cells12202480
APA StyleScheid, S., Goebel, U., & Ulbrich, F. (2023). Neuroprotection Is in the Air—Inhaled Gases on Their Way to the Neurons. Cells, 12(20), 2480. https://doi.org/10.3390/cells12202480