Evaluation of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) Samples from Advanced Non-Small Cell Lung Cancer for Whole Genome, Whole Exome and Comprehensive Panel Sequencing

 , , , , , , , , , , , ,
, , , , , , , , , , , ,  , and
, and  add
Show full author list
add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cohort and EBUS-TBNA Specimen Collection
2.2. DNA and RNA Extraction from Research-Based EBUS-TBNA and Blood Specimens
2.3. Single-Nucleotide Polymorphism (SNP) Arrays
2.4. Sequencing
2.5. Mutation Detection
2.6. Clinically Actionable Mutations
2.7. Tumor Mutation Burden (TMB), Microsatellite Instability (MSI), and Other Potential Biomarkers of Immunotherapy
2.8. Mutational Signatures
3. Results
3.1. Cohort
Results of SOC Testing
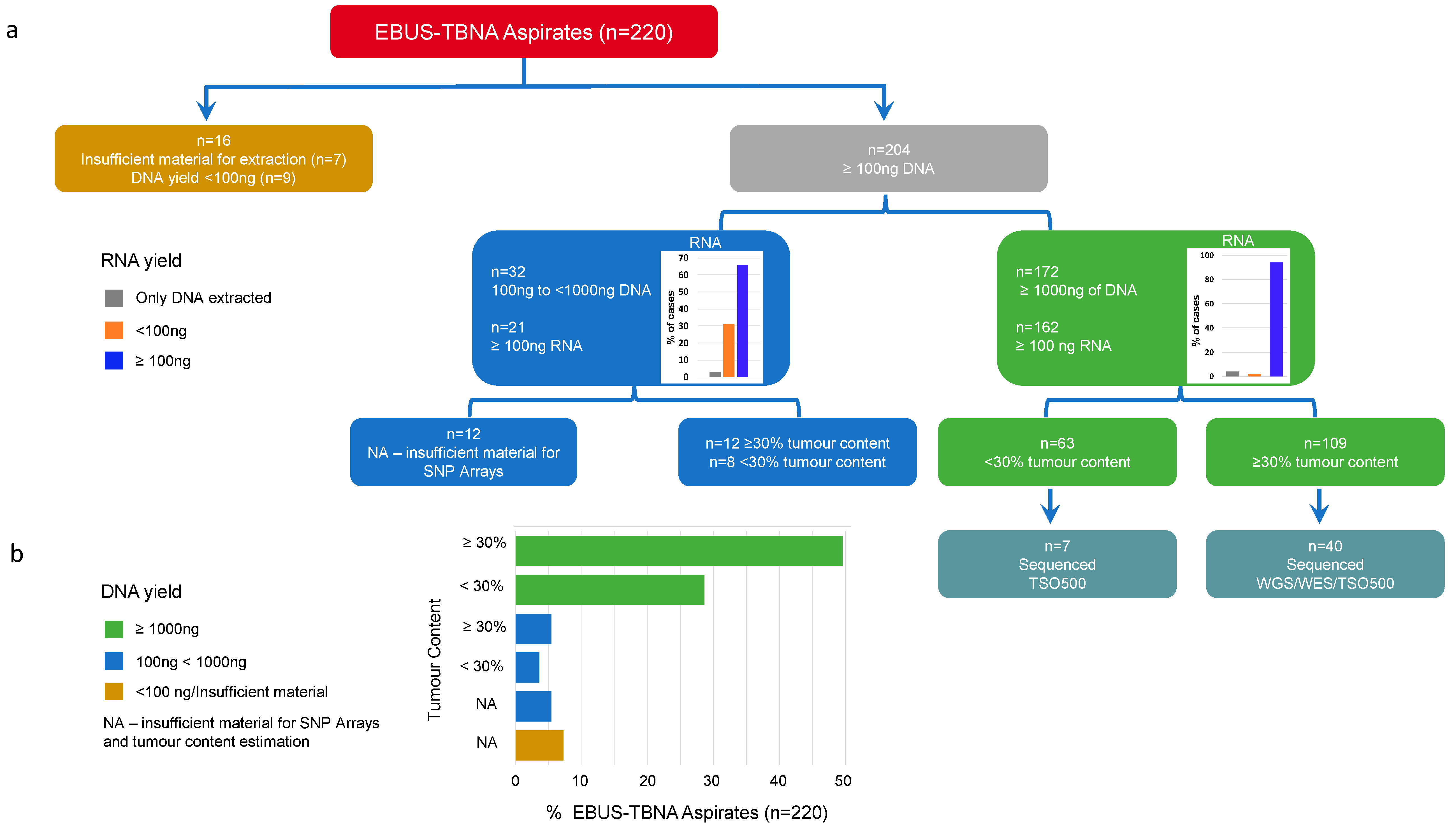
3.2. DNA and RNA Yield from EBUS-TBNA Aspirates from 220 NSCLC Cases
3.3. Comparing TSO500, WES, and WGS Sequencing Platforms
3.4. Discrepancies of Actionable Mutations Detected between Sequencing Platforms
3.5. TSO500 on Low-Tumor-Content Samples
3.6. Detection of Potential Biomarkers of Immunotherapy Response
3.7. Mutational Signatures in EBUS-TBNA Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, M.; Herbst, R.S.; Boshoff, C. Toward personalized treatment approaches for non-small-cell lung cancer. Nat. Med. 2021, 27, 1345–1356. [Google Scholar] [CrossRef]
- Wolff, H.B.; Steeghs, E.M.P.; Mfumbilwa, Z.A.; Groen, H.J.M.; Adang, E.M.; Willems, S.M.; Grunberg, K.; Schuuring, E.; Ligtenberg, M.J.L.; Tops, B.B.J.; et al. Cost-Effectiveness of Parallel Versus Sequential Testing of Genetic Aberrations for Stage IV Non-Small-Cell Lung Cancer in the Netherlands. JCO Precis. Oncol. 2022, 6, e2200201. [Google Scholar] [CrossRef]
- Righi, L.; Franzi, F.; Montarolo, F.; Gatti, G.; Bongiovanni, M.; Sessa, F.; La Rosa, S. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA)-from morphology to molecular testing. J. Thorac. Dis. 2017, 9 (Suppl. S5), S395–S404. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Gondos, A.; Saldana, D.; Thomas, M.; Mascaux, C.; Bubendorf, L.; Barlesi, F. Genomic testing among patients with newly diagnosed advanced non-small cell lung cancer in the United States: A contemporary clinical practice patterns study. Lung Cancer 2022, 167, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, M.E.; Choi, K.; Lanman, R.B.; Licitra, E.J.; Skrzypczak, S.M.; Pe Benito, R.; Wu, T.; Arunajadai, S.; Kaur, S.; Harper, H.; et al. Genomic Profiling of Advanced Non-Small Cell Lung Cancer in Community Settings: Gaps and Opportunities. Clin. Lung Cancer 2017, 18, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, C.; Marmarelis, M.E.; Hwang, W.T.; Scholes, D.G.; McWilliams, T.L.; Singh, A.P.; Sun, L.; Kosteva, J.; Costello, M.R.; Cohen, R.B.; et al. Association Between Availability of Molecular Genotyping Results and Overall Survival in Patients With Advanced Nonsquamous Non-Small-Cell Lung Cancer. JCO Precis. Oncol. 2023, 7, e2300191. [Google Scholar] [CrossRef] [PubMed]
- Mack, P.C.; Klein, M.I.; Ayers, K.L.; Zhou, X.; Guin, S.; Fink, M.; Rossi, M.; Ai-Kateb, H.; O’Connell, T.; Hantash, F.M.; et al. Targeted Next-Generation Sequencing Reveals Exceptionally High Rates of Molecular Driver Mutations in Never-Smokers With Lung Adenocarcinoma. Oncologist 2022, 27, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Sadik, H.; Pritchard, D.; Keeling, D.M.; Policht, F.; Riccelli, P.; Stone, G.; Finkel, K.; Schreier, J.; Munksted, S. Impact of Clinical Practice Gaps on the Implementation of Personalized Medicine in Advanced Non-Small-Cell Lung Cancer. JCO Precis. Oncol. 2022, 6, e2200246. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Tsao, M.S.; Kambartel, K.O.; Isobe, H.; Huang, M.S.; Barrios, C.H.; Khattak, A.; de Marinis, F.; Kothari, S.; Arunachalam, A.; et al. Molecular testing and treatment patterns for patients with advanced non-small cell lung cancer: PIvOTAL observational study. PLoS ONE 2018, 13, e0202865. [Google Scholar] [CrossRef] [PubMed]
- Suehnholz, S.P.; Nissan, M.H.; Zhang, H.; Kundra, R.; Nandakumar, S.; Lu, C.; Carrero, S.; Dhaneshwar, A.; Fernandez, N.; Xu, B.W.; et al. Quantifying the Expanding Landscape of Clinical Actionability for Patients with Cancer. Cancer Discov. 2024, 14, 49–65. [Google Scholar] [CrossRef]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef]
- Lemery, S.; Keegan, P.; Pazdur, R. First FDA Approval Agnostic of Cancer Site—When a Biomarker Defines the Indication. N. Engl. J. Med. 2017, 377, 1409–1412. [Google Scholar] [CrossRef]
- Subbiah, V.; Solit, D.B.; Chan, T.A.; Kurzrock, R. The FDA approval of pembrolizumab for adult and pediatric patients with tumor mutational burden (TMB) >/=10: A decision centered on empowering patients and their physicians. Ann. Oncol. 2020, 31, 1115–1118. [Google Scholar] [CrossRef]
- Kang, Y.J.; O’Haire, S.; Franchini, F.; IJzerman, M.J.; Zalcberg, J.; Macrae, F.; Canfell, K.; Steinberg, J. A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours. Sci. Rep. 2022, 12, 20495. [Google Scholar] [CrossRef]
- Sholl, L.M.; Hirsch, F.R.; Hwang, D.; Botling, J.; Lopez-Rios, F.; Bubendorf, L.; Mino-Kenudson, M.; Roden, A.C.; Beasley, M.B.; Borczuk, A.; et al. The Promises and Challenges of Tumor Mutation Burden as an Immunotherapy Biomarker: A Perspective from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2020, 15, 1409–1424. [Google Scholar] [CrossRef]
- Scalera, S.; Mazzotta, M.; Corleone, G.; Sperati, F.; Terrenato, I.; Krasniqi, E.; Pizzuti, L.; Barba, M.; Vici, P.; Gallo, E.; et al. KEAP1 and TP53 Frame Genomic, Evolutionary, and Immunologic Subtypes of Lung Adenocarcinoma With Different Sensitivity to Immunotherapy. J. Thorac. Oncol. 2021, 16, 2065–2077. [Google Scholar] [CrossRef]
- Ravi, A.; Hellmann, M.D.; Arniella, M.B.; Holton, M.; Freeman, S.S.; Naranbhai, V.; Stewart, C.; Leshchiner, I.; Kim, J.; Akiyama, Y.; et al. Genomic and transcriptomic analysis of checkpoint blockade response in advanced non-small cell lung cancer. Nat. Genet. 2023, 55, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Fielding, D.I.; Dalley, A.J.; Singh, M.; Nandakumar, L.; Lakis, V.; Chittoory, H.; Fairbairn, D.; Patch, A.M.; Kazakoff, S.H.; Ferguson, K.; et al. Evaluating Diff-Quik cytology smears for large-panel mutation testing in lung cancer-Predicting DNA content and success with low-malignant-cellularity samples. Cancer Cytopathol. 2023, 131, 373–382. [Google Scholar] [CrossRef]
- Zhang, C.; Kim, R.Y.; McGrath, C.M.; Andronov, M.; Haas, A.R.; Ma, K.C.; Lanfranco, A.R.; Hutchinson, C.T.; Morrissette, J.J.D.; DiBardino, D.M. The Performance of an Extended Next Generation Sequencing Panel Using Endobronchial Ultrasound-Guided Fine Needle Aspiration Samples in Non-Squamous Non-Small Cell Lung Cancer: A Pragmatic Study. Clin. Lung Cancer 2023, 24, e105–e112. [Google Scholar] [CrossRef] [PubMed]
- Leong, T.L.; Aloe, C.; Aujla, S.; Wang, H.; Gayevskiy, V.; Asselin-Labat, M.L.; Gray, L.A.; Steinfort, D.; Bozinovski, S. Heterogeneity of tumour mutational burden in metastatic NSCLC demonstrated by endobronchial ultrasound sampling. Front. Oncol. 2023, 13, 1150349. [Google Scholar] [CrossRef] [PubMed]
- Fielding, D.; Dalley, A.J.; Singh, M.; Nandakumar, L.; Lakis, V.; Chittoory, H.; Fairbairn, D.; Ferguson, K.; Bashirzadeh, F.; Bint, M.; et al. Whole Genome Sequencing in Advanced Lung Cancer can be Performed Using Diff-Quik Cytology Smears Derived from Endobronchial Ultrasound, Transbronchial Needle Aspiration (EBUS TBNA). Lung 2023, 201, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Pestinger, V.; Smith, M.; Sillo, T.; Findlay, J.M.; Laes, J.F.; Martin, G.; Middleton, G.; Taniere, P.; Beggs, A.D. Use of an Integrated Pan-Cancer Oncology Enrichment Next-Generation Sequencing Assay to Measure Tumour Mutational Burden and Detect Clinically Actionable Variants. Mol. Diagn. Ther. 2020, 24, 339–349. [Google Scholar] [CrossRef]
- Song, S.; Nones, K.; Miller, D.; Harliwong, I.; Kassahn, K.S.; Pinese, M.; Pajic, M.; Gill, A.J.; Johns, A.L.; Anderson, M.; et al. qpure: A tool to estimate tumor cellularity from genome-wide single-nucleotide polymorphism profiles. PLoS ONE 2012, 7, e45835. [Google Scholar] [CrossRef] [PubMed]
- Newell, F.; Kong, Y.; Wilmott, J.S.; Johansson, P.A.; Ferguson, P.M.; Cui, C.; Li, Z.; Kazakoff, S.H.; Burke, H.; Dodds, T.J.; et al. Whole-genome landscape of mucosal melanoma reveals diverse drivers and therapeutic targets. Nat. Commun. 2019, 10, 3163. [Google Scholar] [CrossRef]
- Patch, A.M.; Christie, E.L.; Etemadmoghadam, D.; Garsed, D.W.; George, J.; Fereday, S.; Nones, K.; Cowin, P.; Alsop, K.; Bailey, P.J.; et al. Whole-genome characterization of chemoresistant ovarian cancer. Nature 2015, 521, 489–494. [Google Scholar] [CrossRef]
- Nones, K.; Waddell, N.; Wayte, N.; Patch, A.M.; Bailey, P.; Newell, F.; Holmes, O.; Fink, J.L.; Quinn, M.C.J.; Tang, Y.H.; et al. Genomic catastrophes frequently arise in esophageal adenocarcinoma and drive tumorigenesis. Nat. Commun. 2014, 5, 5224. [Google Scholar] [CrossRef]
- Kassahn, K.S.; Holmes, O.; Nones, K.; Patch, A.M.; Miller, D.K.; Christ, A.N.; Harliwong, I.; Bruxner, T.J.; Xu, Q.; Anderson, M.; et al. Somatic point mutation calling in low cellularity tumors. PLoS ONE 2013, 8, e74380. [Google Scholar] [CrossRef] [PubMed]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef]
- Cingolani, P.; Platts, A.; Wang, L.L.; Coon, M.; Nguyen, T.; Wang, L.; Land, S.J.; Lu, X.; Ruden, D.M. A program for annotating and predicting the effects of single nucleotide polymorphisms, SnpEff: SNPs in the genome of Drosophila melanogaster strain w1118; iso-2; iso-3. Fly 2012, 6, 80–92. [Google Scholar] [CrossRef]
- Raine, K.M.; Van Loo, P.; Wedge, D.C.; Jones, D.; Menzies, A.; Butler, A.P.; Teague, J.W.; Tarpey, P.; Nik-Zainal, S.; Campbell, P.J. ascatNgs: Identifying Somatically Acquired Copy-Number Alterations from Whole-Genome Sequencing Data. Curr. Protoc. Bioinform. 2016, 56, 15.9.1–15.9.17. [Google Scholar] [CrossRef]
- Favero, F.; Joshi, T.; Marquard, A.M.; Birkbak, N.J.; Krzystanek, M.; Li, Q.; Szallasi, Z.; Eklund, A.C. Sequenza: Allele-specific copy number and mutation profiles from tumor sequencing data. Ann. Oncol. 2015, 26, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.T.; Thorvaldsdottir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Paradas, J.; Hernandez-Prieto, S.; Lora, D.; Sanchez, E.; Rosado, A.; Caniego-Casas, T.; Carrizo, N.; Enguita, A.B.; Munoz-Jimenez, M.T.; Rodriguez, B.; et al. Tumor mutational burden assessment in non-small-cell lung cancer samples: Results from the TMB(2) harmonization project comparing three NGS panels. J. Immunother. Cancer 2021, 9, e001904. [Google Scholar] [CrossRef] [PubMed]
- Stenzinger, A.; Allen, J.D.; Maas, J.; Stewart, M.D.; Merino, D.M.; Wempe, M.M.; Dietel, M. Tumor mutational burden standardization initiatives: Recommendations for consistent tumor mutational burden assessment in clinical samples to guide immunotherapy treatment decisions. Genes Chromosomes Cancer 2019, 58, 578–588. [Google Scholar] [CrossRef]
- Niu, B.; Ye, K.; Zhang, Q.; Lu, C.; Xie, M.; McLellan, M.D.; Wendl, M.C.; Ding, L. MSIsensor: Microsatellite instability detection using paired tumor-normal sequence data. Bioinformatics 2014, 30, 1015–1016. [Google Scholar] [CrossRef]
- Fujimoto, A.; Fujita, M.; Hasegawa, T.; Wong, J.H.; Maejima, K.; Oku-Sasaki, A.; Nakano, K.; Shiraishi, Y.; Miyano, S.; Yamamoto, G.; et al. Comprehensive analysis of indels in whole-genome microsatellite regions and microsatellite instability across 21 cancer types. Genome Res. 2020, 30, 334–346. [Google Scholar] [CrossRef]
- Vega, D.M.; Yee, L.M.; McShane, L.M.; Williams, P.M.; Chen, L.; Vilimas, T.; Fabrizio, D.; Funari, V.; Newberg, J.; Bruce, L.K.; et al. Aligning tumor mutational burden (TMB) quantification across diagnostic platforms: Phase II of the Friends of Cancer Research TMB Harmonization Project. Ann. Oncol. 2021, 32, 1626–1636. [Google Scholar] [CrossRef]
- Merino, D.M.; McShane, L.M.; Fabrizio, D.; Funari, V.; Chen, S.J.; White, J.R.; Wenz, P.; Baden, J.; Barrett, J.C.; Chaudhary, R.; et al. Establishing guidelines to harmonize tumor mutational burden (TMB): In silico assessment of variation in TMB quantification across diagnostic platforms: Phase I of the Friends of Cancer Research TMB Harmonization Project. J. Immunother. Cancer 2020, 8, e000147. [Google Scholar] [CrossRef]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients With Non-Small-Cell Lung Cancer Profiled With Targeted Next-Generation Sequencing. J. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef]
- Negrao, M.V.; Skoulidis, F.; Montesion, M.; Schulze, K.; Bara, I.; Shen, V.; Xu, H.; Hu, S.; Sui, D.; Elamin, Y.Y.; et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J. Immunother. Cancer 2021, 9, e002891. [Google Scholar] [CrossRef]
- Alessi, J.V.; Elkrief, A.; Ricciuti, B.; Wang, X.; Cortellini, A.; Vaz, V.R.; Lamberti, G.; Frias, R.L.; Venkatraman, D.; Fulgenzi, C.A.M.; et al. Clinicopathologic and Genomic Factors Impacting Efficacy of First-Line Chemoimmunotherapy in Advanced NSCLC. J. Thorac. Oncol. 2023, 18, 731–743. [Google Scholar] [CrossRef]
- Rossi, E.D.; Wiles, A.; Vecchione, A. Lung cancer and molecular testing in small biopsies versus cytology: The Logics of Worlds. Cancer Cytopathol. 2020, 128, 637–641. [Google Scholar] [CrossRef]
- Arcila, M.E.; Yang, S.R.; Momeni, A.; Mata, D.A.; Salazar, P.; Chan, R.; Elezovic, D.; Benayed, R.; Zehir, A.; Buonocore, D.J.; et al. Ultrarapid EGFR Mutation Screening Followed by Comprehensive Next-Generation Sequencing: A Feasible, Informative Approach for Lung Carcinoma Cytology Specimens With a High Success Rate. JTO Clin. Res. Rep. 2020, 1, 100077. [Google Scholar] [CrossRef]
- D’Ardia, A.; Caputo, A.; Fumo, R.; Ciaparrone, C.; Gaeta, S.; Picariello, C.; Zeppa, P.; D’Antonio, A. Advanced non-small cell lung cancer: Rapid evaluation of EGFR status on fine-needle cytology samples using Idylla. Pathol. Res. Pract. 2021, 224, 153547. [Google Scholar] [CrossRef] [PubMed]
- Steuten, L.; Goulart, B.; Meropol, N.J.; Pritchard, D.; Ramsey, S.D. Cost Effectiveness of Multigene Panel Sequencing for Patients With Advanced Non-Small-Cell Lung Cancer. JCO Clin. Cancer Inf. 2019, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zou, D.; Ye, W.; Hess, L.M.; Bhandari, N.R.; Ale-Ali, A.; Foster, J.; Quon, P.; Harris, M. Diagnostic Value and Cost-Effectiveness of Next-Generation Sequencing-Based Testing for Treatment of Patients with Advanced/Metastatic Non-Squamous Non-Small-Cell Lung Cancer in the United States. J. Mol. Diagn. 2022, 24, 901–914. [Google Scholar] [CrossRef] [PubMed]
- Arriola, E.; Bernabe, R.; Campelo, R.G.; Biscuola, M.; Enguita, A.B.; Lopez-Rios, F.; Martinez, R.; Mezquita, L.; Palanca, S.; Pareja, M.J.; et al. Cost-Effectiveness of Next-Generation Sequencing Versus Single-Gene Testing for the Molecular Diagnosis of Patients With Metastatic Non-Small-Cell Lung Cancer From the Perspective of Spanish Reference Centers. JCO Precis. Oncol. 2023, 7, e2200546. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.H.; Cha, H.; Shim, J.H.; Lee, B.; Chung, J.; Lee, C.; Kim, N.K.D.; Choi, Y.L.; Hwang, S.; Lee, Y.; et al. Clinical advantage of targeted sequencing for unbiased tumor mutational burden estimation in samples with low tumor purity. J. Immunother. Cancer 2020, 8, e001199. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Mayoh, C.; Lau, L.M.S.; Khuong-Quang, D.A.; Pinese, M.; Kumar, A.; Barahona, P.; Wilkie, E.E.; Sullivan, P.; Bowen-James, R.; et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat. Med. 2020, 26, 1742–1753. [Google Scholar] [CrossRef] [PubMed]
- Degasperi, A.; Zou, X.; Amarante, T.D.; Martinez-Martinez, A.; Koh, G.C.C.; Dias, J.M.L.; Heskin, L.; Chmelova, L.; Rinaldi, G.; Wang, V.Y.W.; et al. Substitution mutational signatures in whole-genome-sequenced cancers in the UK population. Science 2022, 376, abl9283. [Google Scholar] [CrossRef] [PubMed]
- Sosinsky, A.; Ambrose, J.; Cross, W.; Turnbull, C.; Henderson, S.; Jones, L.; Hamblin, A.; Arumugam, P.; Chan, G.; Chubb, D.; et al. Insights for precision oncology from the integration of genomic and clinical data of 13,880 tumors from the 100,000 Genomes Cancer Programme. Nat. Med. 2024, 30, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Ren, L.; Chen, Z.; Fang, L.T.; Zhao, Y.; Lack, J.; Guan, M.; Zhu, B.; Jaeger, E.; Kerrigan, L.; et al. Toward best practice in cancer mutation detection with whole-genome and whole-exome sequencing. Nat. Biotechnol. 2021, 39, 1141–1150. [Google Scholar] [CrossRef]
- Punekar, S.R.; Shum, E.; Grello, C.M.; Lau, S.C.; Velcheti, V. Immunotherapy in non-small cell lung cancer: Past, present, and future directions. Front. Oncol. 2022, 12, 877594. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 220) | Number of Patients (%) |
|---|---|
| Age, average (range) | 67.17 (42–88) |
| Sex (n = 220) | |
| Female | 87(40%) |
| Male | 133 (60%) |
| Histology (n = 220) | |
| Adenocarcinoma | 98 (44.5%) |
| Non-small cell lung cancer | 63 (28.6%) |
| Squamous cell carcinoma | 59 (26.8%) |
| Tumor stage (n = 220) | |
| IA | 3 |
| IB | 7 |
| IIB | 9 |
| IIIA | 43 |
| IIIB | 41 |
| IIIC | 17 |
| IVA | 40 |
| IVB | 55 |
| Information not available | 5 |
| Lymph node station/mass * (n = 220) | |
| 2R | 1 |
| 3 | 2 |
| 4R | 45 |
| 4L | 19 |
| 7 | 74 |
| 10 | 9 |
| 11R | 36 |
| 11L | 21 |
| 12 | 3 |
| Tumor mass | 8 |
| Information not available | 2 |
| Smoking status (n = 220) | |
| Current smoker | 67 (30.5%) |
| Ex-smoker | 112 (50.9%) |
| Never smoked | 17 (7.7%) |
| Information not available | 24 (10.9%) |
| Standard of care testing (n = 161 non-squamous NSCLC) | |
| Single-gene test (EGFR) | 46 (28.6%) |
| Small NGS panel | 74 (45.9%) |
| Insufficient tissue for testing | 31 (19.3%) |
| Not tested | 7 (4.3%) |
| Information not available | 3 (1.9%) |
| ALK and ROS1 testing (n = 161 non-squamous NSCLC) | |
| Positive ROS1 | 1 (0.5%) |
| Positive ALK | 1 (0.5%) |
| Equivocal | 2 (1.2%) |
| Negative | 112 (69.6%) |
| Not tested | 14 (8.7%) |
| Insufficient tissue | 26 (16.1%) |
| Information not available | 5 (3.1%) |
| PD-L1 (n = 220) | |
| Tested | 160 (72%) |
| Not tested | 23 (10.5%) |
| Insufficient tissue | 24 (10.9%) |
| Information not available | 13 (5.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fielding, D.; Lakis, V.; Dalley, A.J.; Chittoory, H.; Newell, F.; Koufariotis, L.T.; Patch, A.-M.; Kazakoff, S.; Bashirzadeh, F.; Son, J.H.; et al. Evaluation of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) Samples from Advanced Non-Small Cell Lung Cancer for Whole Genome, Whole Exome and Comprehensive Panel Sequencing. Cancers 2024, 16, 785. https://doi.org/10.3390/cancers16040785
Fielding D, Lakis V, Dalley AJ, Chittoory H, Newell F, Koufariotis LT, Patch A-M, Kazakoff S, Bashirzadeh F, Son JH, et al. Evaluation of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) Samples from Advanced Non-Small Cell Lung Cancer for Whole Genome, Whole Exome and Comprehensive Panel Sequencing. Cancers. 2024; 16(4):785. https://doi.org/10.3390/cancers16040785
Chicago/Turabian StyleFielding, David, Vanessa Lakis, Andrew J. Dalley, Haarika Chittoory, Felicity Newell, Lambros T. Koufariotis, Ann-Marie Patch, Stephen Kazakoff, Farzad Bashirzadeh, Jung Hwa Son, and et al. 2024. "Evaluation of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) Samples from Advanced Non-Small Cell Lung Cancer for Whole Genome, Whole Exome and Comprehensive Panel Sequencing" Cancers 16, no. 4: 785. https://doi.org/10.3390/cancers16040785
APA StyleFielding, D., Lakis, V., Dalley, A. J., Chittoory, H., Newell, F., Koufariotis, L. T., Patch, A.-M., Kazakoff, S., Bashirzadeh, F., Son, J. H., Ryan, K., Steinfort, D., Williamson, J. P., Bint, M., Pahoff, C., Nguyen, P. T., Twaddell, S., Arnold, D., Grainge, C., ... Nones, K. (2024). Evaluation of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) Samples from Advanced Non-Small Cell Lung Cancer for Whole Genome, Whole Exome and Comprehensive Panel Sequencing. Cancers, 16(4), 785. https://doi.org/10.3390/cancers16040785