


Clinical Characteristics, Response to Platinum-Based Chemotherapy and Poly (Adenosine Phosphate-Ribose) Polymerase Inhibitors in Advanced Lung Cancer Patients Harboring BRCA Mutations

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farmer, H.; McCabe, N.; Lord, C.; Tutt, A.; Nature, D.J. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005, 434, 917–921. [Google Scholar] [CrossRef]
- Leongamornlert, D.; Mahmud, N.; Tymrakiewicz, M.; Saunders, E.; Dadaev, T.; Castro, E.; Goh, C.; Govindasami, K.; Guy, M.; O’Brien, L.; et al. Germline BRCA1 mutations increase prostate cancer risk. Br. J. Cancer 2012, 106, 1697–1701. [Google Scholar] [CrossRef]
- Li, S.; Silvestri, V.; Leslie, G.; Rebbeck, T.R.; Neuhausen, S.L.; Hopper, J.L.; Nielsen, H.R.; Lee, A.; Yang, X.; McGuffog, L.; et al. Cancer Risks Associated With BRCA1 and BRCA2 Pathogenic Variants. J. Clin. Oncol. 2022, 40, 1529–1541. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutations. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- Mylavarapu, S.; Das, A.; Roy, M. Role of BRCA Mutations in the Modulation of Response to Platinum Therapy. Front. Oncol. 2018, 8, 16. [Google Scholar] [CrossRef]
- Lung and Bronchus Cancer—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 6 December 2022).
- Remon, J.; Besse, B.; Leary, A.; Bièche, I.; Job, B.; Lacroix, L.; Auguste, A.; Mauduit, M.; Audigier-Valette, C.; Raimbourg, J.; et al. Somatic and Germline BRCA 1 and 2 Mutations in Advanced NSCLC From the SAFIR02-Lung Trial. JTO Clin. Res. Rep. 2020, 1, 100068. [Google Scholar] [CrossRef]
- Sokol, E.S.; Pavlick, D.; Khiabanian, H.; Frampton, G.M.; Ross, J.S.; Gregg, J.P.; Lara, P.N.; Oesterreich, S.; Agarwal, N.; Necchi, A.; et al. Pan-Cancer Analysis of BRCA1 and BRCA2 Genomic Alterations and Their Association With Genomic Instability as Measured by Genome-Wide Loss of Heterozygosity. JCO Precis Oncol. 2020, 4, 442–465. [Google Scholar] [CrossRef]
- Jordan, E.J.; Kim, H.R.; Arcila, M.E.; Barron, D.; Chakravarty, D.; Gao, J.; Chang, M.T.; Ni, A.; Kundra, R.; Jonsson, P.; et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017, 7, 596–609. [Google Scholar] [CrossRef]
- Streff, H.; Profato, J.; Ye, Y.; Nebgen, D.; Peterson, S.K.; Singletary, C.; Arun, B.K.; Litton, J.K. Cancer Incidence in First- and Second-Degree Relatives of BRCA1 and BRCA2 Mutation Carriers. Oncologist 2016, 21, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Parry, E.M.; Gable, D.L.; Stanley, S.E.; Khalil, S.E.; Antonescu, V.; Florea, L.; Armanios, M. Germline Mutations in DNA Repair Genes in Lung Adenocarcinoma. J. Thorac. Oncol. 2017, 12, 1673–1678. [Google Scholar] [CrossRef] [PubMed]
- Riess, J.W.; Redman, M.W.; Wheatley-Price, P.; Faller, B.A.; Villaruz, L.C.; Corum, L.R.; Gowda, A.C.; Srkalovic, G.; Osarogiagbon, R.U.; Baumgart, M.A.; et al. A phase II study of rucaparib in patients with high genomic LOH and/or BRCA 1/2 mutated stage IV non-small cell lung cancer (Lung-MAP Sub-Study, S1900A). J. Clin. Oncol. 2021, 39 (Suppl. S15), 9024. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Thara, E.; Awad, M.M.; Dowlati, A.; Haque, B.; Stinchcombe, T.E.; Dy, G.K.; Spigel, D.R.; Lu, S.; Singh, N.I.; et al. JASPER: Phase 2 trial of first-line niraparib plus pembrolizumab in patients with advanced non-small cell lung cancer. Cancer 2022, 128, 65–74. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Redman, M.W.; Byers, L.A.; Hirsch, F.R.; Mack, P.C.; Schwartz, L.H.; Bradley, J.D.; Stinchcombe, T.E.; Leighl, N.B.; Al Baghdadi, T.; et al. Phase 2 Study of Talazoparib in Patients With Homologous Recombination Repair-Deficient Squamous Cell Lung Cancer: Lung-MAP Substudy S1400G. Clin. Lung Cancer 2021, 22, 187–194.e1. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Blais, N.; Mazieres, J.; Reck, M.; Jones, C.M.; Juhasz, E.; Urban, L.; Orlov, S.; Barlesi, F.; Kio, E.; et al. Randomized, placebo-controlled, phase II study of veliparib in combination with carboplatin and paclitaxel for advanced/metastatic non-small cell lung cancer. Clin. Cancer Res. 2017, 23, 1937–1944. [Google Scholar] [CrossRef]
- Kadouri, L.; Rottenberg, Y.; Zick, A.; Hamburger, T.; Lipson, D.; Peretz, T.; Nechushtan, H. Homologous recombination in lung cancer, germline and somatic mutations, clinical and phenotype characterization. Lung Cancer 2019, 137, 48–51. [Google Scholar] [CrossRef]
- VarSome The Human Genomics Community. Available online: https://varsome.com/ (accessed on 12 July 2023).
- ClinVar. Available online: https://www.ncbi.nlm.nih.gov/clinvar/ (accessed on 12 July 2023).
- cBioPortal for Cancer Genomics. Available online: https://www.cbioportal.org/ (accessed on 27 July 2023).
- Warner, E.; Foulkes, W.; Goodwin, P.; Meschino, W.; Blondal, J.; Paterson, C.; Ozcelik, H.; Goss, P.; Allingham-Hawkins, D.; Hamel, N.; et al. Prevalence and penetrance of BRCA1 and BRCA2 gene mutations in unselected Ashkenazi Jewish women with breast cancer. J. Natl. Cancer Inst. 1999, 91, 1241–1247. [Google Scholar] [CrossRef]
- Tschernichovsky, R.; Averbuch, I.; Goldstein, D.A.; Mutai, R.; Dudnik, E.; Rotem, O.; Laufer-Geva, S.; Peled, N.; Goldberg, Y.; Zer, A. BRCA mutations detected by tumour next-generation sequencing in non-small cell lung cancer: Impact on response to therapy and disease course. Transl. Lung Cancer Res. 2023, 12, 1011–1022. [Google Scholar] [CrossRef]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. 2019, 19, 495–509. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomized, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Fennell, D.A.; Porter, C.; Lester, J.; Danson, S.; Blackhall, F.; Nicolson, M.; Nixon, L.; Gardner, G.; White, A.; Griffiths, G.; et al. Olaparib maintenance versus placebo monotherapy in patients with advanced non-small cell lung cancer (PIN): A multicenter, randomized, controlled, phase 2 trial. eClinicalMedicine 2022, 52, 101595. [Google Scholar] [CrossRef]
- Gulhan, D.C.; Lee, J.J.K.; Melloni, G.E.M.; Cortés-Ciriano, I.; Park, P.J. Detecting the mutational signature of homologous recombination deficiency in clinical samples. Nat. Genet. 2019, 51, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, P.; Bandlamudi, C.; Cheng, M.L.; Srinivasan, P.; Chavan, S.S.; Friedman, N.D.; Rosen, E.Y.; Richards, A.L.; Bouvier, N.; Selcuklu, S.D.; et al. Tumor lineage shapes BRCA-mediated phenotypes. Nature 2019, 571, 7766. [Google Scholar] [CrossRef] [PubMed]
- Wineland, D.; Le, A.N.; Hausler, R.; Kelly, G.; Barrett, E.; Desai, H.; Wubbenhorst, B.; Pluta, J.; Bastian, P.; Symecko, H.; et al. Biallelic BRCA Loss and Homologous Recombination Deficiency in Nonbreast/Ovarian Tumors in Germline BRCA1/2 Carriers. JCO Precis Oncol. 2023, 7, e2300036. [Google Scholar] [CrossRef] [PubMed]
- Murciano-Goroff, Y.R.; Schram, A.M.; Rosen, E.Y.; Won, H.; Gong, Y.; Noronha, A.M.; Janjigian, Y.Y.; Stadler, Z.K.; Chang, J.C.; Yang, S.-R.; et al. Reversion mutations in germline BRCA1/2-mutant tumors reveal a BRCA-mediated phenotype in non-canonical histologies. Nat. Commun. 2022, 13, 7182. [Google Scholar] [CrossRef] [PubMed]
- Elias, K.; Smyczynska, U.; Stawiski, K.; Nowicka, Z.; Webber, J.; Kaplan, J.; Landen, C.; Lubinski, J.; Mukhopadhyay, A.; Chakraborty, D.; et al. Identification of BRCA1/2 mutation female carriers using circulating microRNA profiles. Nat. Commun. 2023, 14, 3350. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | p-BRCA Group (n = 26) | wt-BRCA Control (n = 26) | p-Value |
|---|---|---|---|
| Age at Diagnosis—Median (range) | 67.0 (40–78) | 68.5 (40–79) | 0.61 |
Gender—No. (%)
|
|
| 1.0 |
Ethnic Origin—No. (%)
|
|
| 0.25 |
Smoking status—No. (%)
|
|
| 1.0 |
Personal history of malignancy—No. (%)
|
|
| 0.048 |
Stage at diagnosis—No. (%)
|
|
| 0.71 |
Tumor histology—No. (%)
|
|
| 0.65 |
BRCA Mutation—No. (%)
|
|
| n/a |
Confirmed BRCA germline carrier—No. (%)
|
|
| n/a |
Somatic driver mutations—No. (%)
|
|
| 1.0 |
PDL-1 status group—No. (%)
|
|
| 0.94 |
First-line Treatment
|
|
| 0.96 |
| Treatment Type | p-BRCA Group (n = 18) | wt-BRCA Control (n = 19) | p-Value |
|---|---|---|---|
| Age at Diagnosis—Median (range) | 67.0 (40–75) | 67.0 (40–78) | 0.98 |
Gender—No. (%)
|
|
| 0.40 |
Smoking status—No. (%)
|
|
| 0.38 |
Stage at diagnosis—No. (%)
|
|
| 0.77 |
Tumor histology—No. (%)
|
|
| 0.97 |
PDL-1 status group—No. (%)
|
|
| 0.79 |
First-line Treatment—No. (%)
|
|
| 0.77 |
Best tumor response to first-line PBC—No. (%)
|
|
| 0.12 |
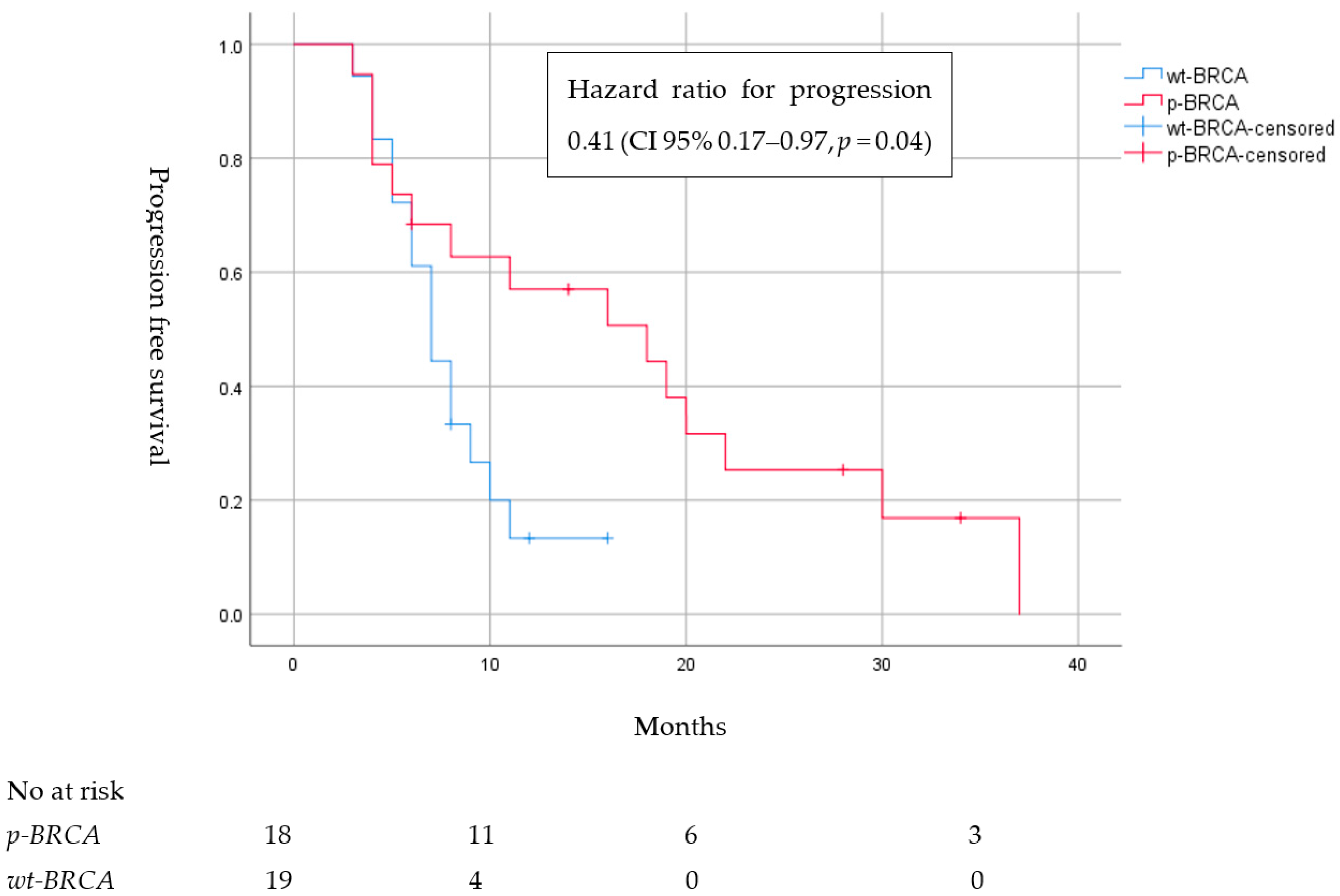
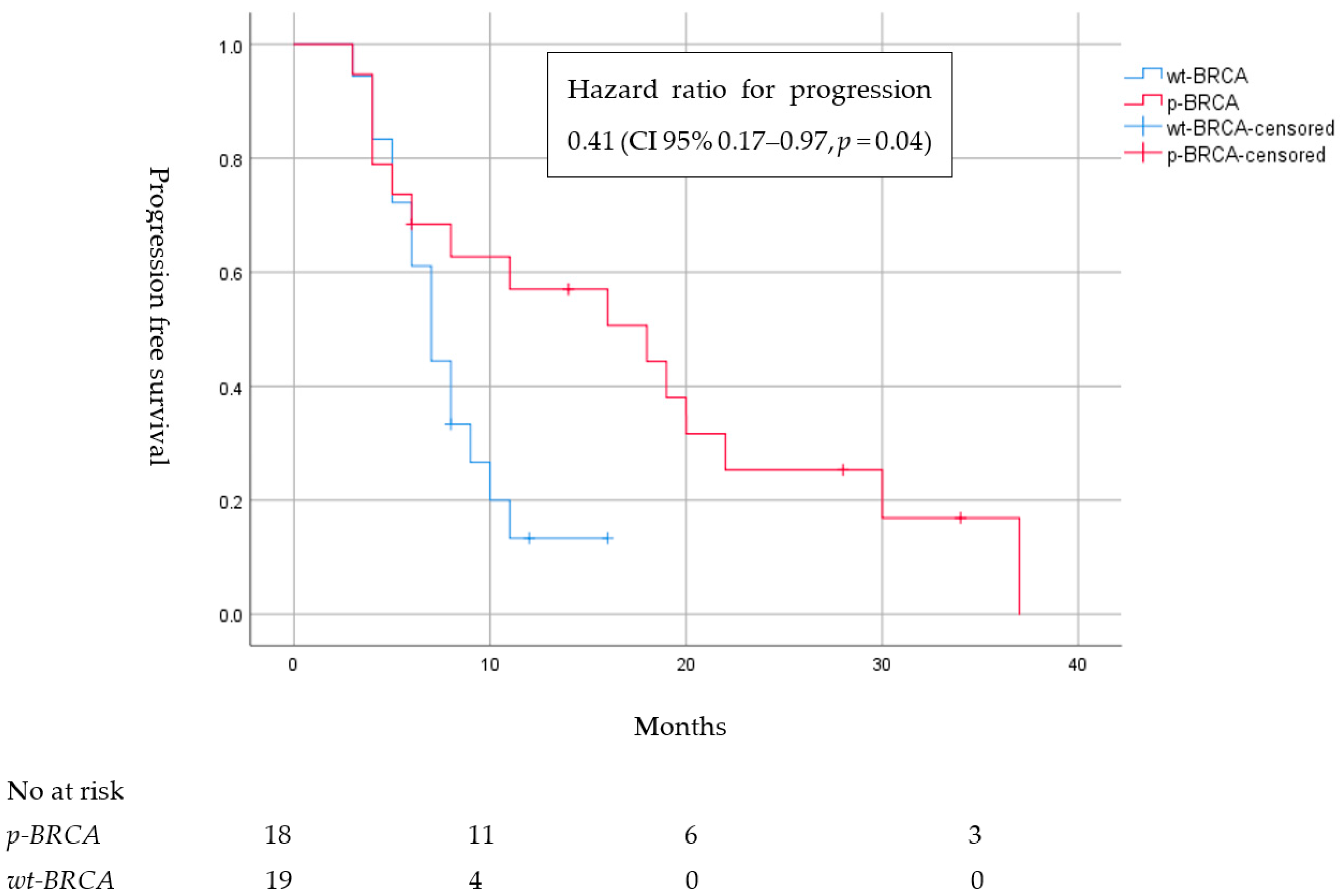
| Median progression-free survival to first-line PBC—months (CI 95%) |
|
| 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnon, J.; Tabi, M.; Rottenberg, Y.; Zick, A.; Blumenfeld, P.; Hamburger, T.; Pikarsky, E.; Avraham, E.; Levine, L.; Popovtzer, A.; et al. Clinical Characteristics, Response to Platinum-Based Chemotherapy and Poly (Adenosine Phosphate-Ribose) Polymerase Inhibitors in Advanced Lung Cancer Patients Harboring BRCA Mutations. Cancers 2023, 15, 4733. https://doi.org/10.3390/cancers15194733
Arnon J, Tabi M, Rottenberg Y, Zick A, Blumenfeld P, Hamburger T, Pikarsky E, Avraham E, Levine L, Popovtzer A, et al. Clinical Characteristics, Response to Platinum-Based Chemotherapy and Poly (Adenosine Phosphate-Ribose) Polymerase Inhibitors in Advanced Lung Cancer Patients Harboring BRCA Mutations. Cancers. 2023; 15(19):4733. https://doi.org/10.3390/cancers15194733
Chicago/Turabian StyleArnon, Johnathan, Michael Tabi, Yakir Rottenberg, Aviad Zick, Philip Blumenfeld, Tamar Hamburger, Eli Pikarsky, Eti Avraham, Leeby Levine, Aron Popovtzer, and et al. 2023. "Clinical Characteristics, Response to Platinum-Based Chemotherapy and Poly (Adenosine Phosphate-Ribose) Polymerase Inhibitors in Advanced Lung Cancer Patients Harboring BRCA Mutations" Cancers 15, no. 19: 4733. https://doi.org/10.3390/cancers15194733
APA StyleArnon, J., Tabi, M., Rottenberg, Y., Zick, A., Blumenfeld, P., Hamburger, T., Pikarsky, E., Avraham, E., Levine, L., Popovtzer, A., Yablonski-Peretz, T., Kadouri, L., & Nechushtan, H. (2023). Clinical Characteristics, Response to Platinum-Based Chemotherapy and Poly (Adenosine Phosphate-Ribose) Polymerase Inhibitors in Advanced Lung Cancer Patients Harboring BRCA Mutations. Cancers, 15(19), 4733. https://doi.org/10.3390/cancers15194733