
The Impact of Physical Activity on the Outcomes of Active Surveillance in Prostate Cancer Patients: A Scoping Review

 ,
,  , , , , , , , ,
, , , , , , , ,  , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Evidence Acquisition
- -
- Population: men of all ages affected by low-risk prostate cancer.
- -
- Intervention: active surveillance.
- -
- Comparison: physical activity levels.
- -
- Outcome: tumor progression/disease reclassification.
- -
- the criteria for inclusion in AS protocols
- -
- the definition of “disease progression”
- -
- the methods used to assess and quantify PA
- -
- interventions conducted by researchers on patients’ PA.
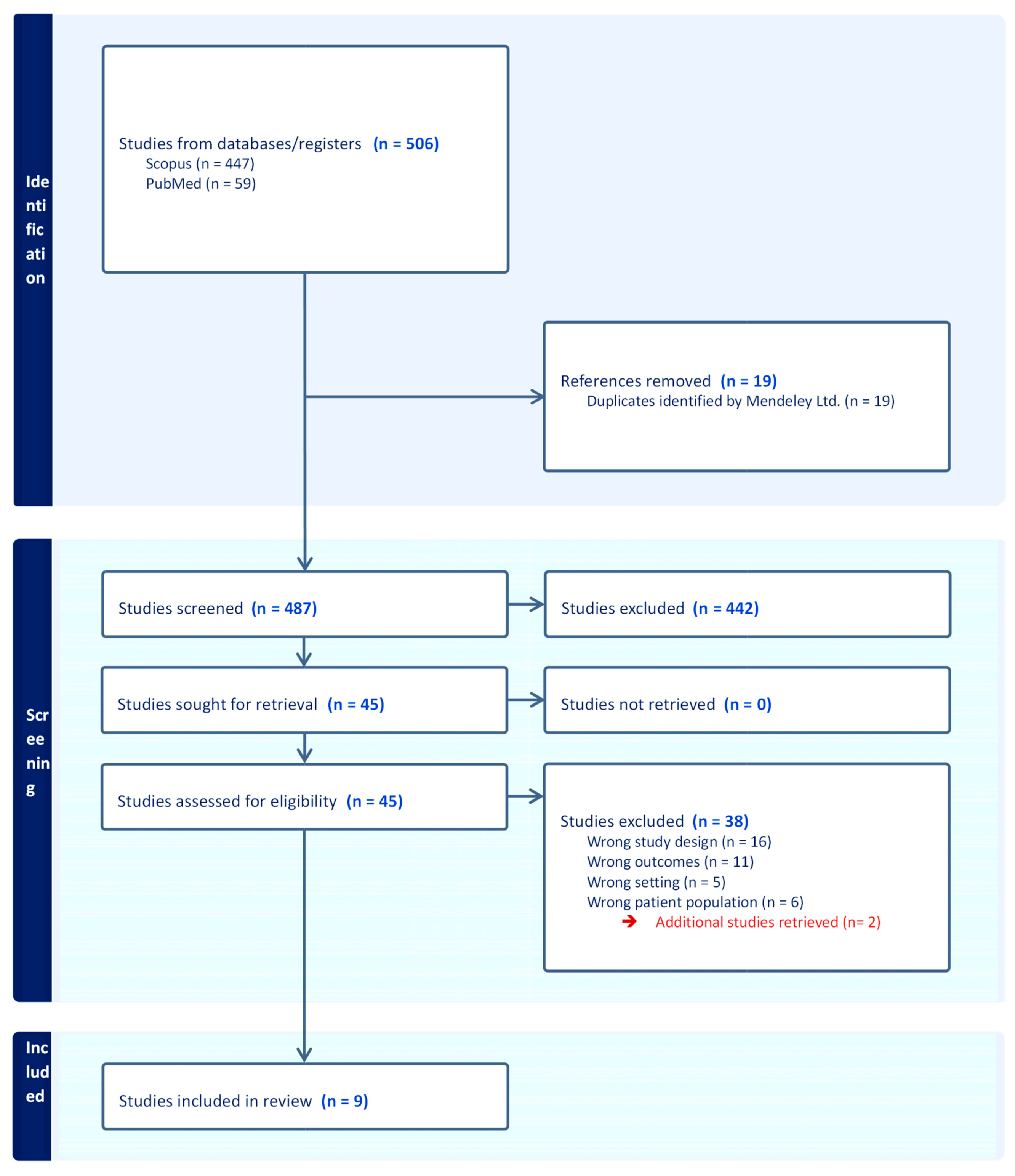
3. Results of the Search
4. Evidence Synthesis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Al Hussein Al Awamlh, B.; Wu, X.; Barocas, D.A.; Moses, K.A.; Hoffman, R.M.; Basourakos, S.P.; Lewicki, P.; Smelser, W.W.; Arenas-Gallo, C.; Shoag, J.E. Intensity of Observation with Active Surveillance or Watchful Waiting in Men with Prostate Cancer in the United States. Prostate Cancer Prostatic Dis. 2023, 26, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Chen, X.; Cole, A.P.; Abdollah, F.; Choueiri, T.K.; Kibel, A.S.; Lipsitz, S.R.; Iyer, H.S.; Trinh, Q.-D. Changes in Prostate-Specific Antigen Screening after the 2018 United States Preventive Services Task Force Recommendations and Through the COVID-19 Pandemic. Eur. Urol. Oncol. 2023, 7, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Bjurlin, M.A.; Nicholson, J.; Tammela, T.L.; Penson, D.F.; Carter, H.B.; Carroll, P.; Etzioni, R. Overdiagnosis and Overtreatment of Prostate Cancer. Eur. Urol. 2014, 65, 1046–1055. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Metcalfe, C.; Davis, M.; Turner, E.L.; Martin, R.M.; Young, G.J.; Walsh, E.I.; Bryant, R.J.; et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N. Engl. J. Med. 2023, 388, 1547–1558. [Google Scholar] [CrossRef]
- Bacon, C.G.; Giovannucci, E.; Testa, M.; Glass, T.A.; Kawachi, I. The Association of Treatment-Related Symptoms with Quality-of-Life Outcomes for Localized Prostate Carcinoma Patients. Cancer 2002, 94, 862–871. [Google Scholar] [CrossRef]
- Cooperberg, M.R. Active Surveillance for Low-Risk Prostate Cancer-An Evolving International Standard of Care. JAMA Oncol. 2017, 3, 1398–1399. [Google Scholar] [CrossRef]
- Kato, T.; Hirama, H.; Mitsuzuka, K.; Maruyama, S.; Sasaki, H.; Saito, T.; Matsumoto, R.; Sakamoto, S.; Sakai, Y.; Fukuhara, H.; et al. Reclassification Prediction of First-Year Protocol Biopsy on Active Surveillance of Prostate Cancer by P2PSA-Related Parameters: From PRIAS-JAPAN. Prostate Cancer Prostatic Dis. 2022, 25, 666–671. [Google Scholar] [CrossRef]
- Klotz, L. Active Surveillance for Low-Risk Prostate Cancer. Curr. Urol. Rep. 2015, 16, 24. [Google Scholar] [CrossRef]
- Chiam, K.; Carle, C.; Hughes, S.; Kench, J.G.; Woo, H.H.; Lord, S.; Smith, D.P. Use of Multiparametric Magnetic Resonance Imaging (MpMRI) in Active Surveillance for Low-Risk Prostate Cancer: A Scoping Review on the Benefits and Harm of MpMRI in Different Biopsy Scenarios. Prostate Cancer Prostatic Dis. 2021, 24, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Fairey, A.S.; Boulé, N.G.; Field, C.J.; Wharton, S.A.; Courneya, K.S. Effects of Exercise on Cardiorespiratory Fitness and Biochemical Progression in Men with Localized Prostate Cancer Under Active Surveillance: The ERASE Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Bourke, L.; Smith, D.; Steed, L.; Hooper, R.; Carter, A.; Catto, J.; Albertsen, P.C.; Tombal, B.; Payne, H.A.; Rosario, D.J. Exercise for Men with Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. 2016, 69, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Wekesa, A.; Harrison, M.; Watson, R.W. Physical Activity and Its Mechanistic Effects on Prostate Cancer. Prostate Cancer Prostatic Dis. 2015, 18, 197–207. [Google Scholar] [CrossRef]
- Nader, S.; Massoud, A.; Al-Obeidat, F.; Mohamed, W.F.; Hafez, W.; Rashid, A.; Yousef, O.A.E.; Gador, M.; Ahmed, S.; Jose, M.; et al. Impact of Aerobic and Resistance Training on Fatigue, Quality of Life, and Physical Activity in Prostate Cancer Patients: A Systematic Review and Meta-Analysis. Int. J. Surg. 2024. [Google Scholar] [CrossRef]
- Mak, S.; Thomas, A. Steps for Conducting a Scoping Review. J. Grad. Med. Educ. 2022, 14, 565–567. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO Framework to Improve Searching PubMed for Clinical Questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ornish, D.; Weidner, G.; Fair, W.R.; Marlin, R.; Pettengill, E.B.; Raisin, C.J.; Dunn-Emke, S.; Crutchfield, L.; Jacobs, F.N.; Barnard, R.J.; et al. Intensive Lifestyle Changes May Affect the Progression of Prostate Cancer. J. Urol. 2005, 174, 1065–1069; discussion 1069–1070. [Google Scholar] [CrossRef] [PubMed]
- Frattaroli, J.; Weidner, G.; Dnistrian, A.M.; Kemp, C.; Daubenmier, J.J.; Marlin, R.O.; Crutchfield, L.; Yglecias, L.; Carroll, P.R.; Ornish, D. Clinical Events in Prostate Cancer Lifestyle Trial: Results from Two Years of Follow-Up. Urology 2008, 72, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Richman, E.L.; Kenfield, S.A.; Stampfer, M.J.; Paciorek, A.; Carroll, P.R.; Chan, J.M. Physical Activity after Diagnosis and Risk of Prostate Cancer Progression: Data from the Cancer of the Prostate Strategic Urologic Research Endeavor. Cancer Res. 2011, 71, 3889–3895. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.; Chan, J.M. Physical Activity and Survival after Prostate Cancer Diagnosis in the Health Professionals Follow-up Study. J. Clin. Oncol. 2011, 29, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, A.K.; Hansen, R.D.; Borre, M.; Larsen, R.G.; Jensen, J.M.; Overgaard, K.; Borre, M.; Kyrø, C.; Landberg, R.; Olsen, A.; et al. A Lifestyle Intervention among Elderly Men on Active Surveillance for Non-Aggressive Prostate Cancer: A Randomised Feasibility Study with Whole-Grain Rye and Exercise. Trials 2017, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Vandersluis, A.D.; Guy, D.E.; Klotz, L.H.; Fleshner, N.E.; Kiss, A.; Parker, C.; Venkateswaran, V. The Role of Lifestyle Characteristics on Prostate Cancer Progression in Two Active Surveillance Cohorts. Prostate Cancer Prostatic Dis. 2016, 19, 305–310. [Google Scholar] [CrossRef]
- Guy, D.E.; Vandersluis, A.; Klotz, L.H.; Fleshner, N.; Kiss, A.; Parker, C.; Venkateswaran, V. Total Energy Expenditure and Vigorous-Intensity Physical Activity Are Associated with Reduced Odds of Reclassification among Men on Active Surveillance. Prostate Cancer Prostatic Dis. 2018, 21, 187–195. [Google Scholar] [CrossRef]
- Papadopoulos, E.; Alibhai, S.M.H.; Tomlinson, G.A.; Matthew, A.G.; Nesbitt, M.; Finelli, A.; Trachtenberg, J.; Santa Mina, D. Influence of Physical Activity on Active Surveillance Discontinuation in Men with Low-Risk Prostate Cancer. Cancer Causes Control 2019, 30, 1009–1012. [Google Scholar] [CrossRef]
- Brassetti, A.; Ferriero, M.; Napodano, G.; Sanseverino, R.; Badenchini, F.; Tuderti, G.; Anceschi, U.; Bove, A.; Misuraca, L.; Mastroianni, R.; et al. Physical Activity Decreases the Risk of Cancer Reclassification in Patients on Active Surveillance: A Multicenter Retrospective Study. Prostate Cancer Prostatic Dis. 2021, 24, 1151–1157. [Google Scholar] [CrossRef]
- Sacks, D.; Baxter, B.; Campbell, B.C.V.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A.; et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke: From the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of Interventional Radiology (SIR), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO). J. Vasc. Interv. Radiol. 2018, 29, 441–453. [Google Scholar] [CrossRef]
- Loeb, S.; Fu, B.C.; Bauer, S.R.; Pernar, C.H.; Chan, J.M.; Van Blarigan, E.L.; Giovannucci, E.L.; Kenfield, S.A.; Mucci, L.A. Association of Plant-Based Diet Index with Prostate Cancer Risk. Am. J. Clin. Nutr. 2022, 115, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Sidhu, M.; Gowin, K. Understanding the Mechanisms of Diet and Outcomes in Colon, Prostate, and Breast Cancer; Malignant Gliomas; and Cancer Patients on Immunotherapy. Nutrients 2020, 12, 2226. [Google Scholar] [CrossRef]
- Goodall, P.P.; Little, J.; Robinson, E.; Trimble, I.; Cole, O.J.; Walton, T.J. Initial Experience of an Algorithm-Based Protocol for the Community Follow-up of Men with Prostate Cancer. BJU Int. 2017, 119, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Saxe, G.A.; Hébert, J.R.; Carmody, J.F.; Kabat-Zinn, J.; Rosenzweig, P.H.; Jarzobski, D.; Reed, G.W.; Blute, R.D. Can Diet in Conjunction with Stress Reduction Affect the Rate of Increase in Prostate Specific Antigen after Biochemical Recurrence of Prostate Cancer? J. Urol. 2001, 166, 2202–2207. [Google Scholar] [CrossRef]
- Tosoian, J.J.; Mamawala, M.; Epstein, J.I.; Landis, P.; Wolf, S.; Trock, B.J.; Carter, H.B. Intermediate and Longer-Term Outcomes from a Prospective Active-Surveillance Program for Favorable-Risk Prostate Cancer. J. Clin. Oncol. 2015, 33, 3379–3385. [Google Scholar] [CrossRef] [PubMed]
- Naha, U.; Freedland, S.J.; Abern, M.R.; Moreira, D.M. The Association of Cancer-Specific Anxiety with Disease Aggressiveness in Men on Active Surveillance of Prostate Cancer. Prostate Cancer Prostatic Dis. 2021, 24, 335–340. [Google Scholar] [CrossRef] [PubMed]
- De Nunzio, C.; Brassetti, A.; Cancrini, F.; Prata, F.; Cindolo, L.; Sountoulides, P.; Toutziaris, C.; Gacci, M.; Lombardo, R.; Cicione, A.; et al. Physical Inactivity, Metabolic Syndrome and Prostate Cancer Diagnosis: Development of a Predicting Nomogram. Metabolites 2023, 13, 111. [Google Scholar] [CrossRef] [PubMed]
- Cicione, A.; Brassetti, A.; Lombardo, R.; Franco, A.; Turchi, B.; D’Annunzio, S.; Nacchia, A.; Tubaro, A.; Simone, G.; De Nunzio, C. Metabolic Syndrome and Physical Inactivity May Be Shared Etiological Agents of Prostate Cancer and Coronary Heart Diseases. Cancers 2022, 14, 936. [Google Scholar] [CrossRef]
- Van Blarigan, E.L.; Gerstenberger, J.P.; Kenfield, S.A.; Giovannucci, E.L.; Stampfer, M.J.; Jones, L.W.; Clinton, S.K.; Chan, J.M.; Mucci, L.A. Physical Activity and Prostate Tumor Vessel Morphology: Data from the Health Professionals Follow-up Study. Cancer Prev. Res. 2015, 8, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jacobs, E.J.; Gapstur, S.M.; Maliniak, M.L.; Gansler, T.; McCullough, M.L.; Stevens, V.L.; Patel, A.V. Recreational Physical Activity in Relation to Prostate Cancer-Specific Mortality among Men with Nonmetastatic Prostate Cancer. Eur. Urol. 2017, 72, 931–939. [Google Scholar] [CrossRef]
- Bonn, S.E.; Sjölander, A.; Lagerros, Y.T.; Wiklund, F.; Stattin, P.; Holmberg, E.; Grönberg, H.; Bälter, K. Physical Activity and Survival among Men Diagnosed with Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2015, 24, 57–64. [Google Scholar] [CrossRef]
- Dovey, Z.; Horowitz, A.; Waingankar, N. The Influence of Lifestyle Changes (Diet, Exercise and Stress Reduction) on Prostate Cancer Tumour Biology and Patient Outcomes: A Systematic Review. BJUI Compass 2023, 4, 385–416. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef]
- Ornish, D.; Lin, J.; Chan, J.M.; Epel, E.; Kemp, C.; Weidner, G.; Marlin, R.; Frenda, S.J.; Magbanua, M.J.M.; Daubenmier, J.; et al. Effect of Comprehensive Lifestyle Changes on Telomerase Activity and Telomere Length in Men with Biopsy-Proven Low-Risk Prostate Cancer: 5-Year Follow-up of a Descriptive Pilot Study. Lancet Oncol. 2013, 14, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Ornish, D.; Magbanua, M.J.M.; Weidner, G.; Weinberg, V.; Kemp, C.; Green, C.; Mattie, M.D.; Marlin, R.; Simko, J.; Shinohara, K.; et al. Changes in Prostate Gene Expression in Men Undergoing an Intensive Nutrition and Lifestyle Intervention. Proc. Natl. Acad. Sci. USA 2008, 105, 8369–8374. [Google Scholar] [CrossRef] [PubMed]
- Magbanua, M.J.M.; Richman, E.L.; Sosa, E.V.; Jones, L.W.; Simko, J.; Shinohara, K.; Haqq, C.M.; Carroll, P.R.; Chan, J.M. Physical Activity and Prostate Gene Expression in Men with Low-Risk Prostate Cancer. Cancer Causes Control 2014, 25, 515–523. [Google Scholar] [CrossRef]
- Rundqvist, H.; Augsten, M.; Strömberg, A.; Rullman, E.; Mijwel, S.; Kharaziha, P.; Panaretakis, T.; Gustafsson, T.; Östman, A. Effect of Acute Exercise on Prostate Cancer Cell Growth. PLoS ONE 2013, 8, e67579. [Google Scholar] [CrossRef]
- Womble, P.R.; Montie, J.E.; Ye, Z.; Linsell, S.M.; Lane, B.R.; Miller, D.C. Contemporary Use of Initial Active Surveillance Among Men in Michigan with Low-Risk Prostate Cancer. Eur. Urol. 2015, 67, 44–50. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Carroll, P.R. Trends in Management for Patients with Localized Prostate Cancer, 1990-2013. JAMA 2015, 314, 80–82. [Google Scholar] [CrossRef]
- Chen, R.C.; Rumble, R.B.; Loblaw, D.A.; Finelli, A.; Ehdaie, B.; Cooperberg, M.R.; Morgan, S.C.; Tyldesley, S.; Haluschak, J.J.; Tan, W.; et al. Active Surveillance for the Management of Localized Prostate Cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J. Clin. Oncol. 2016, 34, 2182–2190. [Google Scholar] [CrossRef]
- Sanghera, S.; Coast, J.; Martin, R.M.; Donovan, J.L.; Mohiuddin, S. Cost-Effectiveness of Prostate Cancer Screening: A Systematic Review of Decision-Analytical Models. BMC Cancer 2018, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Patel, H.D.; Taylor, J.; Borin, J.F.; Jacobsohn, K.; Kenfield, S.A.; Eggener, S.E.; Price, C.; Davuluri, M.; Byrne, N.; et al. Systematic Review of the Impact of a Plant-Based Diet on Prostate Cancer Incidence and Outcomes. Prostate Cancer Prostatic Dis. 2022, 25, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.M.; Mott, S.L.; McDowell, B.D.; Anand, S.T.; Nepple, K.G. Trends and Practices for Managing Low-Risk Prostate Cancer: A SEER-Medicare Study. Prostate Cancer Prostatic Dis. 2022, 25, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, K.B.; Chan, J.M.; Ryan, C.J.; Kenfield, S.A. Diet and Lifestyle Considerations for Patients with Prostate Cancer. Urol. Oncol. 2020, 38, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Vesprini, D.; Sethukavalan, P.; Jethava, V.; Zhang, L.; Jain, S.; Yamamoto, T.; Mamedov, A.; Loblaw, A. Long-Term Follow-up of a Large Active Surveillance Cohort of Patients with Prostate Cancer. J. Clin. Oncol. 2015, 33, 272–277. [Google Scholar] [CrossRef]
- De Nunzio, C.; Brassetti, A.; Simone, G.; Lombardo, R.; Mastroianni, R.; Collura, D.; Muto, G.; Gallucci, M.; Tubaro, A. Metabolic Syndrome Increases the Risk of Upgrading and Upstaging in Patients with Prostate Cancer on Biopsy: A Radical Prostatectomy Multicenter Cohort Study. Prostate Cancer Prostatic Dis. 2018, 21, 438–445. [Google Scholar] [CrossRef]
- De Nunzio, C.; Simone, G.; Brassetti, A.; Mastroianni, R.; Collura, D.; Muto, G.; Gallucci, M.; Tubaro, A. Metabolic Syndrome Is Associated with Advanced Prostate Cancer in Patients Treated with Radical Retropubic Prostatectomy: Results from a Multicentre Prospective Study. BMC Cancer 2016, 16, 407. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Design | Number of Pts | Population Details | Intervention Details | Assessment of Physical Activity | Stratification by Intensity (Score—Scale) | Measured Oncological Outcomes | Association PA and Progression of PCa (Yes/No) | Quantitative Results |
|---|---|---|---|---|---|---|---|---|---|
| Ornish et al., 2005 [20] | Randomized controlled trial | 93 | GS < 7 PSA 4–10 ng/mL T1-T2 stage | Experimental group vs. control group | Self-reporting questionnaire (0: no adherence; 1: adherence) | Not reported | Increased PSA, LNCaP cell growth | yes | (r = −0.23, p < 0.035) |
| Frattaroli et al., 2008 [21] | Randomized controlled trial | 93 | GS < 7 PSA 4–10 ng/mL | Experimental group vs. usual care | Self-reporting questionnaire (0%: no adherence; 100%: adherence) | Not reported | Conventional PCa treatment, increased PSA | yes/no | r = 0.255; CI: (0.053–0.437); p < 0.005/p > 0.05 (PSA) |
| Richman et al., 2011 [22] | Retrospective study (Cross-sectional study) | 1455 | Clinically localized prostate cancer | Individual physical activity | Metabolic equivalent task (MET-hour/week) value | Non vigorous PA: MET < 6 Vigorous PA: MET ≥ 6 | Increased suspicious PSA, secondary treatment | yes | HR 0.43; 95%CI: (0.21–0.91); p = 0.03 |
| Kenfield et al. 2011 [23] | Prospective study | 2705 | GS < 7 T1-T2 stage | Different type of physical activity | Metabolic equivalent task (MET-hour/week) value | Non vigorous PA: MET < 6 Vigorous PA: MET ≥ 6 | Increased suspicious PSA, PCa specific death | yes | HR 0.44; 95% CI: (0.17–1.15) |
| Eriksen et al., 2012 [24] | Randomized controlled trial | 26 | Clinically localized prostate cancer | Experimental group vs. control group | Accelerometers/Gyroscopes | Not reported | Increased suspicious PSA | no | HR 0.2; 95% CI: (−2.1–2.6) |
| Vandersluis et al., 2016 [25] | Retrospective study | 131 | GS ≤ 7 PSA < 10 ng/mL T1c-T2a stage | Individual physical activity | Metabolic equivalent task (MET-hour/week) value | Non vigorous PA: MET < 6 Vigorous PA: MET ≥ 6 | Tumor upgrading at biopsy | no | 95% CI: (0.77–1.16); p = 0.29/ 95% CI: (0.55–1.02); p = 0.066 |
| Guy et al., 2019 [26] | Retrospective study (Cross-sectional study) | 131 | GS ≤ 7 PSA < 10 ng/mL T1c-T2a stage | Recreational and total Physical activity | Global Physical Activity Questionnaire (GPAQ)/ Adjusted MET value for activity = Standard MET value for activity × ([3.5 mL O2/kg·min]/[3.6145 − (0.0367 × BMI) − (0.0038 × age) + (0.1790 × 2)]) | Moderate intensity: small increases in Breathing and heart rate Vigorous intensity: large increases in breathing and heart rate | Tumor Tumor upgrading at biopsy | yes | OR 0.42; 95% CI: (0.20–0.85) (p-trend = 0.027) |
| Papadopoulos et al., 2019 [27] | Retrospective study (Cross-sectional study) | 421 | GS ≤ 6 PSA < 10 ng/mL Stage ≤ T2a | Individual physical activity | Godin Leisure-Time Exercise Questionnaire (GLTEQ)/ Metabolic equivalent task (MET-hour/week) value | Inactive: <210 MET-min/wk) Insufficiently active: 210 < MET-min/wk < 500 Active: 500 < MET-min/wk < 1000 Highly active: > 1000 MET-min/wk | Tumor upgrading at biopsy | no | HR 1.11; 95% CI: (1.03–1.21) |
| Brassetti et al., 2021 [28] | Retrospective study (Cross-sectional study) | 85 | ISUP 1 ≤ 2 positive cores, stage T1c-T2a, PSA ≤ 10 ng/mL, PSA density < 0.2 | Individual physical activity | Physical Activity Scale for the Elderly (PASE) | Sedentary: PASE ≤ 65 Moderately active: 65 < PASE < 125 Active: PASE ≥ 125 | Tumor upgrading at biopsy | yes | HR: 0.987; 95%CI: (0.977–0.998); p = 0.016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brassetti, A.; Cacciatore, L.; Bove, A.M.; Anceschi, U.; Proietti, F.; Misuraca, L.; Tuderti, G.; Flammia, R.S.; Mastroianni, R.; Ferriero, M.C.; et al. The Impact of Physical Activity on the Outcomes of Active Surveillance in Prostate Cancer Patients: A Scoping Review. Cancers 2024, 16, 630. https://doi.org/10.3390/cancers16030630
Brassetti A, Cacciatore L, Bove AM, Anceschi U, Proietti F, Misuraca L, Tuderti G, Flammia RS, Mastroianni R, Ferriero MC, et al. The Impact of Physical Activity on the Outcomes of Active Surveillance in Prostate Cancer Patients: A Scoping Review. Cancers. 2024; 16(3):630. https://doi.org/10.3390/cancers16030630
Chicago/Turabian StyleBrassetti, Aldo, Loris Cacciatore, Alfredo Maria Bove, Umberto Anceschi, Flavia Proietti, Leonardo Misuraca, Gabriele Tuderti, Rocco Simone Flammia, Riccardo Mastroianni, Maria Consiglia Ferriero, and et al. 2024. "The Impact of Physical Activity on the Outcomes of Active Surveillance in Prostate Cancer Patients: A Scoping Review" Cancers 16, no. 3: 630. https://doi.org/10.3390/cancers16030630
APA StyleBrassetti, A., Cacciatore, L., Bove, A. M., Anceschi, U., Proietti, F., Misuraca, L., Tuderti, G., Flammia, R. S., Mastroianni, R., Ferriero, M. C., Chiacchio, G., D’Annunzio, S., Pallares-Mendez, R., Lombardo, R., Leonardo, C., De Nunzio, C., & Simone, G. (2024). The Impact of Physical Activity on the Outcomes of Active Surveillance in Prostate Cancer Patients: A Scoping Review. Cancers, 16(3), 630. https://doi.org/10.3390/cancers16030630