
Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics–Clinicopathological Nomogram


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
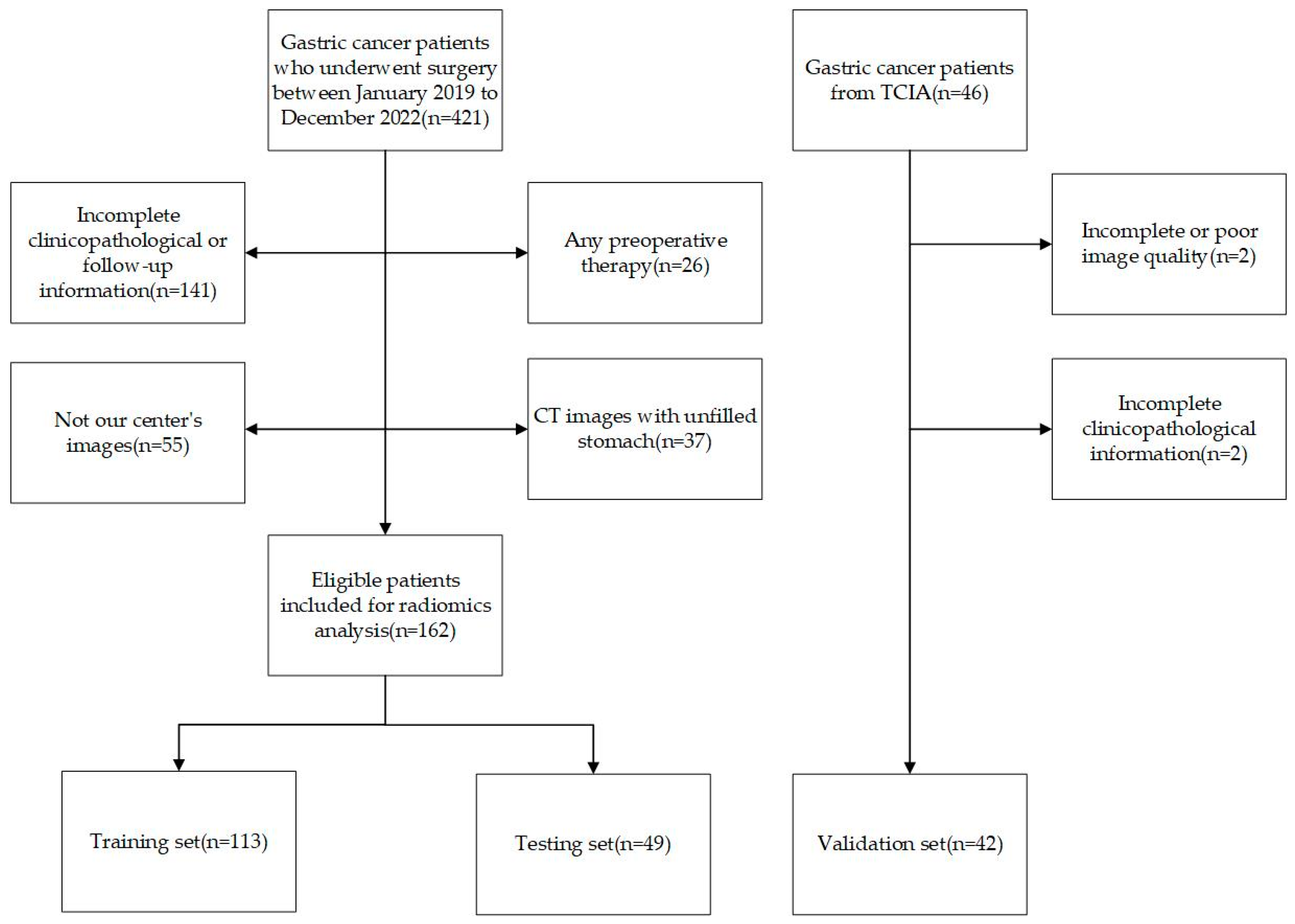
2.1. Patients
2.2. CT Image Acquisition
2.3. Regions of Interest and Extraction of Radiomics Features
2.4. Feature Selection and Calculation of Radscores
2.5. Model Construction and Evaluation
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
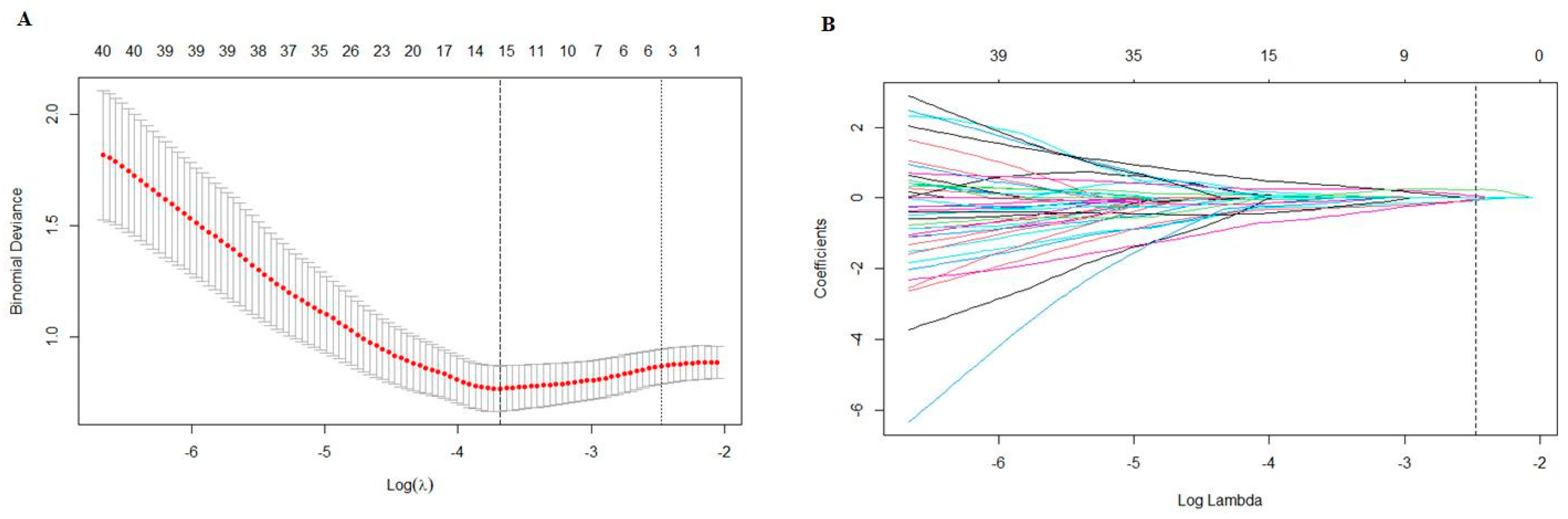
3.2. Radiomics Features Selection and Model Construction
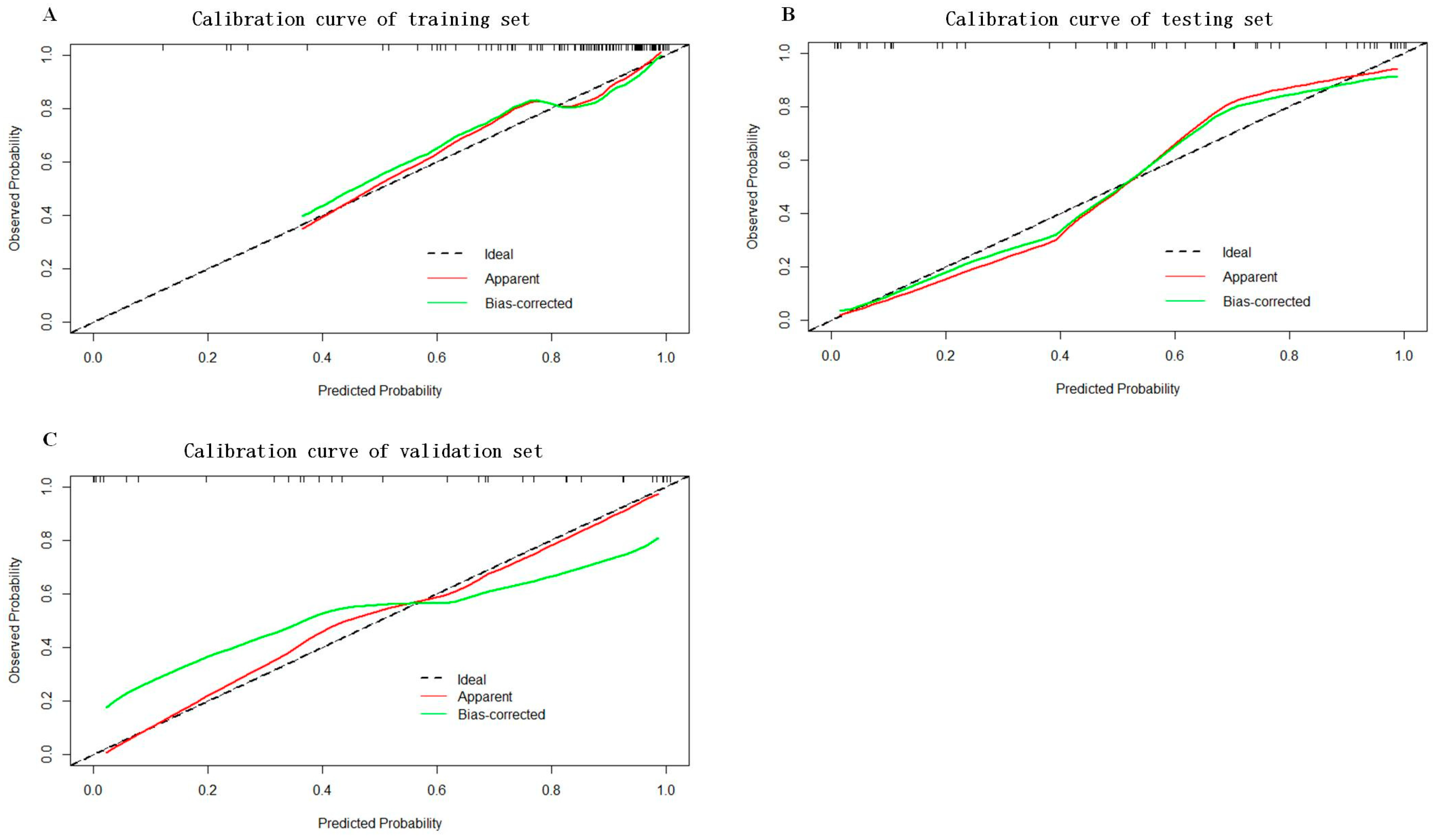
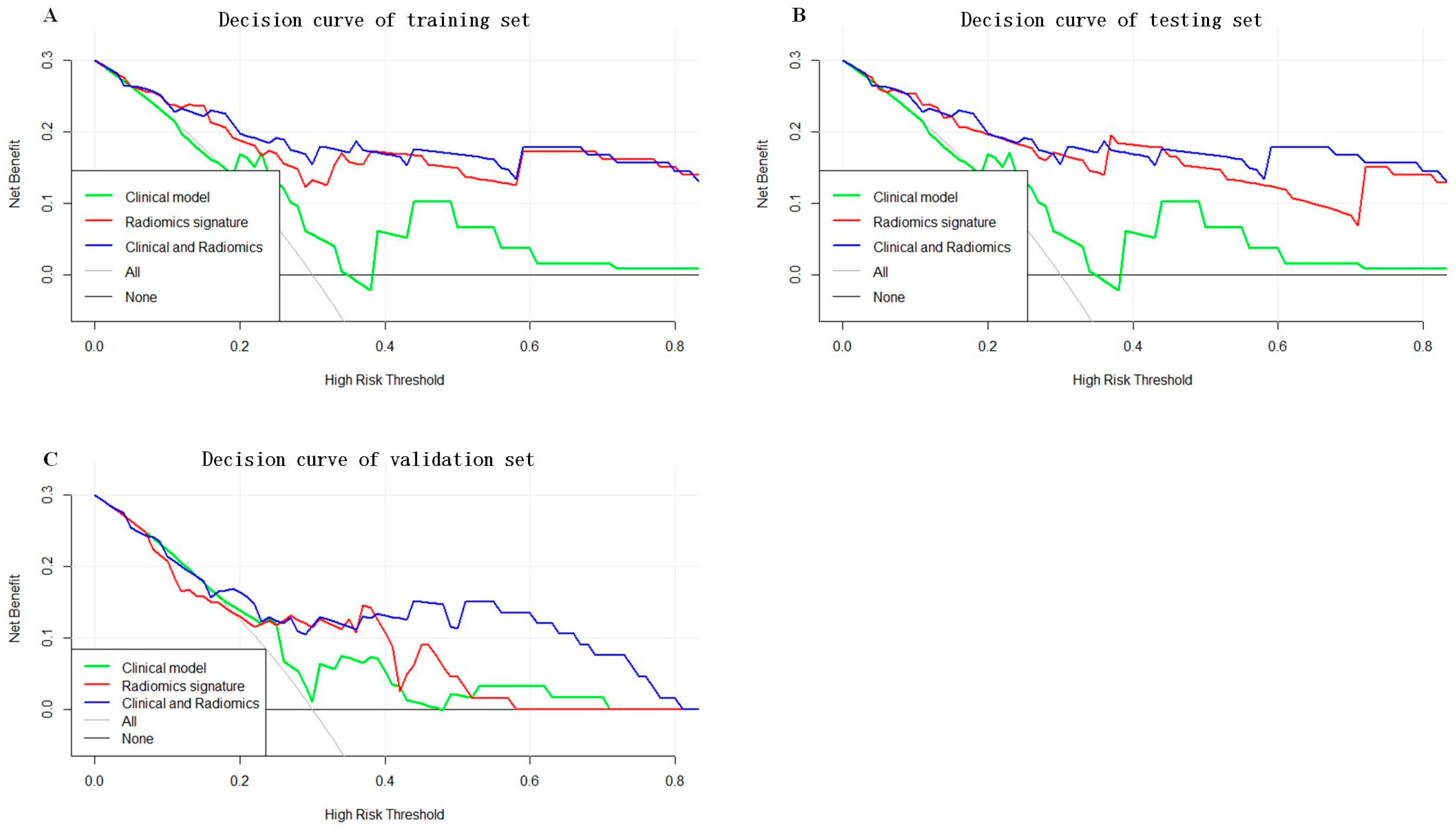
3.3. Construction and Evaluation of Combined Radiomics–Clinicopathological Model
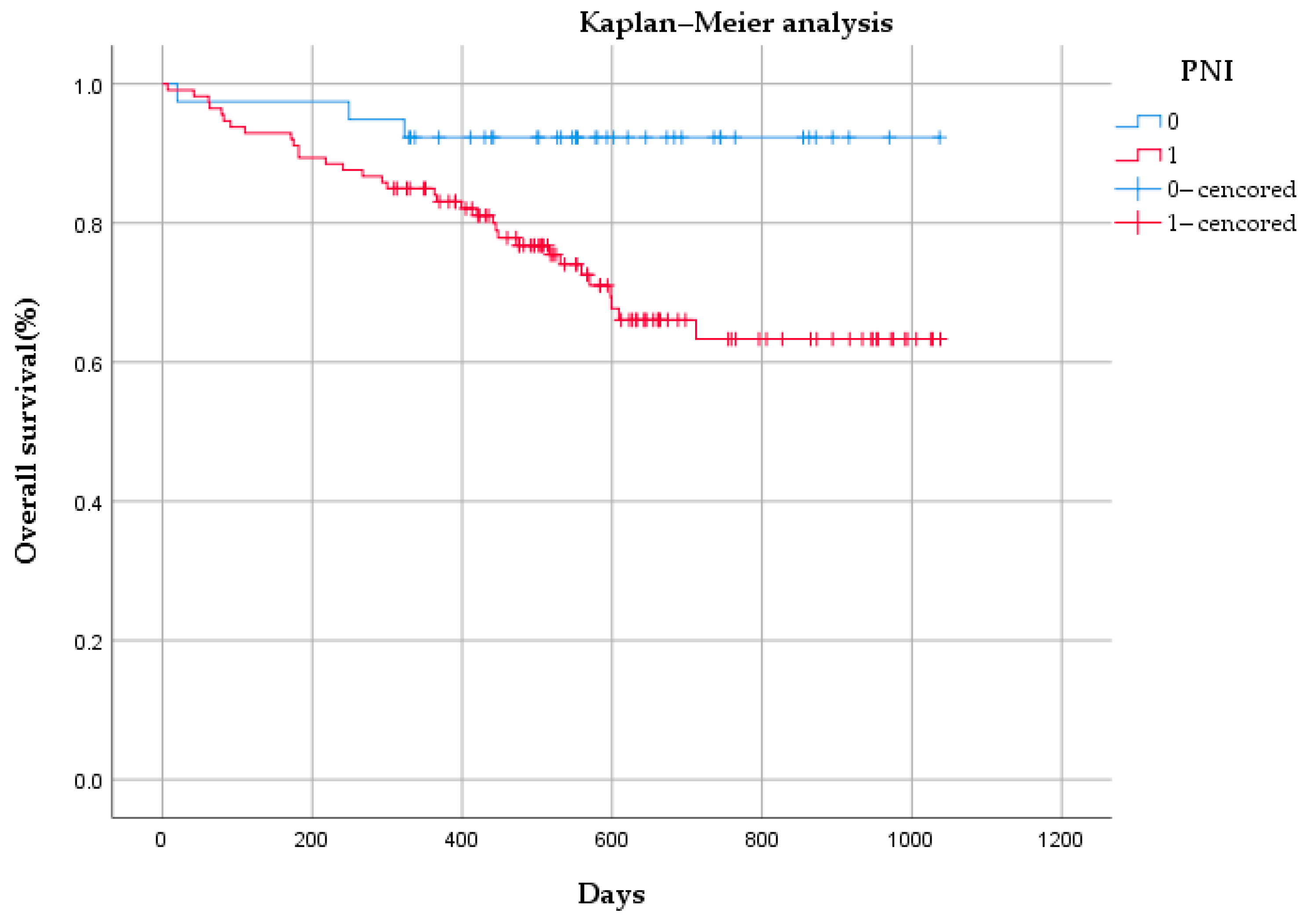
3.4. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ning, F.L.; Zhang, N.N.; Zhao, Z.M.; Du, W.Y.; Zeng, Y.J.; Abe, M.; Pei, J.P.; Zhang, C.D. Global, Regional, and National Burdens with Temporal Trends of Early-, Intermediate-, and Later-Onset Gastric Cancer from 1990 to 2019 and Predictions up to 2035. Cancers 2022, 14, 5417. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef] [PubMed]
- Riihimäki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. Metastatic spread in patients with gastric cancer. Oncotarget 2016, 7, 52307–52316. [Google Scholar] [CrossRef]
- Yu, X.; Hu, F.; Li, C.; Yao, Q.; Zhang, H.; Xue, Y. Clinicopathologic characteristics and prognosis of proximal and distal gastric cancer. OncoTargets Ther. 2018, 11, 1037–1044. [Google Scholar] [CrossRef]
- Liu, L.; Wang, Z.W.; Ji, J.; Zhang, J.N.; Yan, M.; Zhang, J.; Liu, B.Y.; Zhu, Z.G.; Yu, Y.Y. A cohort study and meta-analysis between histopathological classification and prognosis of gastric carcinoma. Anti-Cancer Agents Med. Chem. 2013, 13, 227–234. [Google Scholar] [CrossRef]
- Wang, W.; Yang, Q.; Huang, Q.; Zhang, H.; Zhang, Z.; Gao, J.; Ren, W.; Hu, Y.; Lin, Y.; Dang, Y.; et al. The rs2839698 Single Nucleotide Polymorphism of lncRNA H19 is Associated with Post-Operative Prognosis in T3 Gastric Adenocarcinoma. Clin. Lab. 2018, 64, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Dan, Y.Q.; Choi, Y.Y.; Zhou, Z.G.; Hyung, W.J.; Hu, J.K.; Noh, S.H. The Impact of Nerve Involvement on the Prognosis of Gastric Cancer Patients with Curative Gastrectomy: An International Multicenter Analysis. Dis. Markers 2021, 2021, 8870562. [Google Scholar] [CrossRef]
- Liu, Q.; Ma, Z.; Cao, Q.; Zhao, H.; Guo, Y.; Liu, T.; Li, J. Perineural invasion-associated biomarkers for tumor development. Biomed. Pharmacother. 2022, 155, 113691. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: A review of the literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Zhao, B.; Lv, W.; Mei, D.; Luo, R.; Bao, S.; Huang, B.; Lin, J. Perineural invasion as a predictive factor for survival outcome in gastric cancer patients: A systematic review and meta-analysis. J. Clin. Pathol. 2020, 73, 544–551. [Google Scholar] [CrossRef]
- Li, C.; Wang, M.; Cheng, X.; Jiang, Y.; Xiao, H. Nerve invasion as an independent predictor of poor prognosis in gastric cancer after curative resection. Medicine 2022, 101, e30084. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; Zeng, Y.; Chen, D.; Zhan, W.; Zhan, Y. Application of radiomics in precision prediction of diagnosis and treatment of gastric cancer. Jpn. J. Radiol. 2023, 41, 245–257. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, C.; Xie, J.; Wang, W.; Zha, X.; Lv, W.; Chen, H.; Hu, Y.; Li, T.; Yu, J.; et al. Radiomics signature of computed tomography imaging for prediction of survival and chemotherapeutic benefits in gastric cancer. EBioMedicine 2018, 36, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; He, J.; Liu, S.; Ji, C.; Guan, W.; Chen, L.; Guan, Y.; Yang, X.; Zhou, Z. Radiomics analysis using contrast-enhanced CT for preoperative prediction of occult peritoneal metastasis in advanced gastric cancer. Eur. Radiol. 2020, 30, 239–246. [Google Scholar] [CrossRef]
- Zheng, H.; Zheng, Q.; Jiang, M.; Han, C.; Yi, J.; Ai, Y.; Xie, C.; Jin, X. Contrast-enhanced CT based radiomics in the preoperative prediction of perineural invasion for patients with gastric cancer. Eur. J. Radiol. 2022, 154, 110393. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef]
- Liu, S.; Liu, S.; Ji, C.; Zheng, H.; Pan, X.; Zhang, Y.; Guan, W.; Chen, L.; Guan, Y.; Li, W.; et al. Application of CT texture analysis in predicting histopathological characteristics of gastric cancers. Eur. Radiol. 2017, 27, 4951–4959. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Orman, S.; Cayci, H.M. Gastric cancer: Factors affecting survival. Acta Chir. Belg. 2019, 119, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Chen, H.; Luo, D.; Xiong, Z.; Li, X.; Yin, S.; Jin, L.; Chen, S.; Peng, J.; Lian, L. Lymphovascular or perineural invasion is associated with lymph node metastasis and survival outcomes in patients with gastric cancer. Cancer Med. 2023, 12, 9401–9408. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.F.; Wang, S.Y.; Le, P.H.; Chen, T.H.; Kuo, C.J.; Lin, C.J.; Chou, W.C.; Yeh, T.S.; Hsu, J.T. Prognostic Significance of Perineural Invasion in Patients with Stage II/III Gastric Cancer Undergoing Radical Surgery. J. Pers. Med. 2022, 12, 962. [Google Scholar] [CrossRef] [PubMed]
- Uzun, O.; Gülmez, S.; Senger, A.S.; Ömeroğlu, S.; Polat, E.; Duman, M. Prognostic effect of perineural invasion in successive years in patients with locally advanced gastric cancer. Indian J. Pathol. Microbiol. 2021, 64, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.; Wang, L.; Xia, Y.; Dang, S.; Zhang, X.; He, Z.; Xu, J.; Shang, M.; Xu, Z. Netrin-1 promotes cell neural invasion in gastric cancer via its receptor neogenin. J. Cancer 2019, 10, 3197–3207. [Google Scholar] [CrossRef]
- Jia, X.; Lu, M.; Rui, C.; Xiao, Y. Consensus-Expressed CXCL8 and MMP9 Identified by Meta-Analyzed Perineural Invasion Gene Signature in Gastric Cancer Microarray Data. Front. Genet. 2019, 10, 851. [Google Scholar] [CrossRef]
- Yardimci, A.H.; Kocak, B.; Bektas, C.T.; Sel, I.; Yarikkaya, E.; Dursun, N.; Bektas, H.; Afsarriz, C.U.; Gursu, R.U.; Kilickesmez, O. Tubular gastric adenocarcinoma: Machine learning-based CT texture analysis for predicting lymphovascular and perineural invasion. Diagn. Interv. Radiol. 2020, 26, 515–522. [Google Scholar] [CrossRef]
- Liu, J.; Huang, X.; Chen, S.; Wu, G.; Xie, W.; Franco, J.P.C.; Zhang, C.; Huang, L.; Tian, C.; Tang, W. Nomogram based on clinical characteristics for preoperative prediction of perineural invasion in gastric cancer. J. Int. Med. Res. 2020, 48, 300060519895131. [Google Scholar] [CrossRef]
- Deng, J.; You, Q.; Gao, Y.; Yu, Q.; Zhao, P.; Zheng, Y.; Fang, W.; Xu, N.; Teng, L. Prognostic value of perineural invasion in gastric cancer: A systematic review and meta-analysis. PLoS ONE 2014, 9, e88907. [Google Scholar] [CrossRef]
- Demircioğlu, A. The effect of preprocessing filters on predictive performance in radiomics. Eur. Radiol. Exp. 2022, 6, 40. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set | p | Testing Set | p | ||||
|---|---|---|---|---|---|---|---|
| PNI (+) | PNI (−) | PNI (+) | PNI (−) | ||||
| N = 95 | N = 18 | N = 33 | N = 16 | ||||
| Age (mean ± SD 1) | 66.11 ± 10.85 | 65.72 ± 8.85 | 0.194 | 62.91 ± 11.38 | 67.8 ± 3.42 | 0.494 | |
| Gender, No. (%) | 0.350 | 0.218 | |||||
| Male | 70 (73.7%) | 10 (55.6%) | 26 (78.8%) | 5 (31.3%) | |||
| Female | 25 (26.3%) | 8 (44.4%) | 7 (21.2%) | 11 (68.7%) | |||
| Size, No. (%) | 0.191 | 0.189 | |||||
| <5 cm | 45 (47.4%) | 12 (66.7%) | 18 (54.5%) | 13 (81.2%) | |||
| ≥5 cm | 50 (52.6%) | 6 (33.3%) | 15 (45.5%) | 3 (18.8%) | |||
| Location, No. (%) | 0.315 | 0.205 | |||||
| Antrum | 37 (38.9%) | 9 (50%) | 7 (21.2%) | 4 (25.0%) | |||
| Body | 27 (28.4%) | 2 (11.1%) | 5 (15.2%) | 5 (31.3%) | |||
| Fundus | 31 (32.6%) | 7 (38.9%) | 21 (63.6%) | 7 (43.8%) | |||
| Tissue differentiation, No. (%) | 0.119 | 0.075 | |||||
| High | 51 (53.7%) | 5 (27.8%) | 18 (54.5%) | 9 (56.3%) | |||
| Middle | 28 (29.5%) | 9 (50%) | 10 (30.3%) | 6 (37.5%) | |||
| Low | 16 (16.8%) | 4 (22.2%) | 5 (15.2%) | 1 (6.3%) | |||
| Lauren type, No. (%) | >0.9 | 0.051 | |||||
| Intestinal | 20 (21.5%) | 9 (50.0%) | 5 (15.2%) | 2 (12.5%) | |||
| Diffuse | 35 (37.6%) | 3 (16.7%) | 11 (33.3%) | 1 (6.3%) | |||
| Mixed | 38 (40.9%) | 6 (33.3%) | 17 (51.5%) | 13 (81.3%) | |||
| T stage, No. (%) | <0.001 | 0.008 | |||||
| 1 | 11 (11.6%) | 5 (27.8%) | 8 (24.2%) | 12 (75.0%) | |||
| 2 | 7 (7.37%) | 7 (38.9%) | 2 (6.1%) | 3 (18.8%) | |||
| 3 | 43 (45.3%) | 2 (11.1%) | 13 (39.4%) | 1 (6.3%) | |||
| 4 | 34 (35.8%) | 4 (22.2%) | 10 (30.3%) | 0 | |||
| N stage, No. (%) | <0.001 | 0.003 | |||||
| 0 | 7 (7.37%) | 10 (55.6%) | 5 (15.2%) | 3 (18.8%) | |||
| 1 | 24 (25.3%) | 1 (5.56%) | 3 (9.1%) | 12 (75%) | |||
| 2 | 18 (18.9%) | 5 (27.8%) | 9 (27.3%) | 1 (6.3%) | |||
| 3 | 46 (48.4%) | 2 (11.1%) | 16 (48.5%) | 0 | |||
| LVI 2, No. (%) | 0.014 | 0.001 | |||||
| Yes | 58 (61.1%) | 8 (44.4%) | 25 (75.8%) | 12 (75%) | |||
| No | 37 (38.9%) | 10 (55.6%) | 8 (24.2%) | 4 (25%) | |||
| HER-2 3, No. (%) | 0.847 | 0.881 | |||||
| (0–1+) | 54 (74.0%) | 11 (61.1%) | 19 (57.6%) | 5 (31.3%) | |||
| (++–+++) | 19 (26.0%) | 7 (38.9%) | 14 (42.4%) | 11 (68.7%) | |||
| Neutrophils, median (IQR) | 4.09 (2.79, 4.69) | 3.56 (2.73, 4.27) | 0.417 | 3.63 (3.03, 4.74) | 3.19 (2.83, 5.35) | 0.706 | |
| Lymphocytes, median (IQR) | 1.46 (1.14, 1.80) | 1.33 (1.19, 1.87) | 0.812 | 1.51 (1.03, 1.96) | 1.39 (1.22, 1.82) | 1.000 | |
| Albumin, median (IQR) | 39.80 (36.75, 41.60) | 42.00 (35.85, 44.35) | 0.460 | 41.5 (35.9, 45.5) | 38.1 (36.45, 40.4) | 0.448 | |
| CEA 4, No. (%) | 0.374 | 0.545 | |||||
| ≤10 | 90(95.2%) | 16(88.9%) | 27 (81.9%) | 14 (87.5%) | |||
| >10 | 5(4.8%) | 2(11.1%) | 6 (18.2%) | 2 (12.5%) | |||
| CA125 5, No. (%) | 0.133 | 0.628 | |||||
| ≤35 | 83 (87.3%) | 16 (88.9%) | 19 (57.6%) | 10 (62.5%) | |||
| >35 | 8 (12.7%) | 2 (11.1%) | 14 (42.4%) | 6 (37.5%) | |||
| CA199 6, No. (%) | 0.096 | 0.545 | |||||
| ≤37.0 U/mL | 71 (74.6%) | 15 (83.3%) | 27 (81.8%) | 10 (62.5%) | |||
| >37.0 U/mL | 24 (25.4%) | 3 (16.7%) | 6 (18.2%) | 6 (37.5%) | |||
| Smoking history, No. (%) | 0.983 | 0.245 | |||||
| Yes | 8 (12.7%) | 2 (11.1%) | 29 (87.9%) | 4 (25.0%) | |||
| No | 83 (87.3%) | 16 (88.9%) | 4 (12.1%) | 12 (75.0%) | |||
| Drinking history, No. (%) | 0.876 | 0.262 | |||||
| Yes | 11 (11.6%) | 4 (22.2%) | 30 (90.9%) | 1 (6.3%) | |||
| No | 84 (88.4%) | 14 (77.8%) | 3 (9.1%) | 15 (93.7%) | |||
| Radscore, median (IQR) | 1.74 (1.58, 1.99) | 1.43 (1.14, 1.60) | <0.001 | 1.90 (1.69, 2.07) | 1.50 (1.33, 1.64) | <0.001 | |
| Features | Coefficients |
|---|---|
| wavelet.HLL_glcm_InverseVariance | 0.17618597 |
| original_firstorder_90Percentile | 0.06464257 |
| wavelet.HHH_firstorder_Minimum | −2.96234129 |
| wavelet.LLL_firstorder_Median | 0.84062825 |
| gradient_gldm_DependenceNonUniformityNormalized | 1.20886446 |
| Predicted Factors | OR 1 | 95%CI 2 | p-Value |
|---|---|---|---|
| Age | 1.008 | 0.961–1.057 | 0.754 |
| Gender | 0.786 | 0.272–2.270 | 0.656 |
| Size | 1.031 | 0.846–1.258 | 0.760 |
| Location | 1.086 | 0.638–1.847 | 0.762 |
| Tissue differentiation | 0.646 | 0.352–1.185 | 0.158 |
| Lauren type | 1.261 | 0.693–2.296 | 0.447 |
| T stage | 8.013 | 2.604–24.660 | 0.001 |
| N stage | 2.882 | 1.266–6.564 | 0.012 |
| LVI 3 | 1.344 | 0.162–11.130 | 0.784 |
| HER-2 4 | 0.831 | 0.302–2.286 | 0.720 |
| Neutrophils | 0.981 | 0.840–1.146 | 0.981 |
| Lymphocytes | 1.028 | 0.432–2.448 | 0.950 |
| Albumin | 1.007 | 0.923–1.100 | 0.870 |
| CEA 5 | 1.091 | 0.925–1.288 | 0.300 |
| CA-125 6 | 1.046 | 0.980–1.116 | 0.181 |
| CA-199 7 | 1.027 | 0.990–1.065 | 0.154 |
| Smoking history | 0.432 | 0.074–2.531 | 0.352 |
| Drinking history | 2.169 | 0.260–18.120 | 0.475 |
| Radscore | 3.040 | 1.250–7.397 | 0.014 |
| Training Set (n = 113) | Testing Set (n = 49) | Validation Set (n = 42) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AUC (95%CI) | ACC | SEN | SPE | AUC (95%CI) | ACC | SEN | SPE | AUC (95%CI) | ACC | SEN | SPE | |
| Model1 | 0.820 (0.695–0.944) | 0.832 | 0.851 | 0.400 | 0.768 (0.596–0.941) | 0.837 | 0.851 | 0.500 | 0.669 (0.497–0.842) | 0.619 | 0.600 | 0.667 |
| Model2 | 0.829 (0.738–0.921) | 0.876 | 0.879 | 0.833 | 0.816 (0.683–0.950) | 0.836 | 0.851 | 0.772 | 0.779 (0.625–0.933) | 0.718 | 0.737 | 0.700 |
| Model3 | 0.851 (0.769–0.933) | 0.929 | 0.886 | 0.750 | 0.842 (0.713–0.970) | 0.837 | 0.851 | 0.818 | 0.813 (0.672–0.954) | 0.744 | 0.750 | 0.737 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, H.; Li, R.; Liu, Y.; Zhan, T.; Li, Y.; Zhang, J. Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics–Clinicopathological Nomogram. Cancers 2024, 16, 614. https://doi.org/10.3390/cancers16030614
Jia H, Li R, Liu Y, Zhan T, Li Y, Zhang J. Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics–Clinicopathological Nomogram. Cancers. 2024; 16(3):614. https://doi.org/10.3390/cancers16030614
Chicago/Turabian StyleJia, Heng, Ruzhi Li, Yawei Liu, Tian Zhan, Yuan Li, and Jianping Zhang. 2024. "Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics–Clinicopathological Nomogram" Cancers 16, no. 3: 614. https://doi.org/10.3390/cancers16030614
APA StyleJia, H., Li, R., Liu, Y., Zhan, T., Li, Y., & Zhang, J. (2024). Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics–Clinicopathological Nomogram. Cancers, 16(3), 614. https://doi.org/10.3390/cancers16030614