
Combining Classic and Novel Neutrophil-Related Biomarkers to Identify Non-Small-Cell Lung Cancer
 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Detection of Novel Neutrophil-Related Biomarkers via Luminex Assays
2.3. Statistical Analysis
3. Results
3.1. Stage 1
3.2. Stage 2
3.3. Stage 3
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Leiter, A.; Veluswamy, R.R.; Wisnivesky, J.P. The global burden of lung cancer: Current status and future trends. Nat. Rev. Clin. Oncol. 2023, 20, 624–639. [Google Scholar] [CrossRef] [PubMed]
- Shaul, M.E.; Fridlender, Z.G. Tumour-associated neutrophils in patients with cancer. Nat. Rev. Clin. Oncol. 2019, 16, 601–620. [Google Scholar] [CrossRef] [PubMed]
- Silvestre-Roig, C.; Braster, Q.; Ortega-Gomez, A.; Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nat. Rev. Cardiol. 2020, 17, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Papayannopoulos, V. Neutrophil extracellular traps in immunity and disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Coffelt, S.B.; Wellenstein, M.D.; de Visser, K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef] [PubMed]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Cassatella, M.A.; Costantini, C.; Jaillon, S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat. Rev. Immunol. 2011, 11, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, C.C.; Malanchi, I. Neutrophils in cancer: Heterogeneous and multifaceted. Nat. Rev. Immunol. 2022, 22, 173–187. [Google Scholar] [CrossRef]
- Wculek, S.K.; Bridgeman, V.L.; Peakman, F.; Malanchi, I. Early Neutrophil Responses to Chemical Carcinogenesis Shape Long-Term Lung Cancer Susceptibility. iScience 2020, 23, 101277. [Google Scholar] [CrossRef]
- Matlung, H.L.; Babes, L.; Zhao, X.W.; van Houdt, M.; Treffers, L.W.; van Rees, D.J.; Franke, K.; Schornagel, K.; Verkuijlen, P.; Janssen, H.; et al. Neutrophils Kill Antibody-Opsonized Cancer Cells by Trogoptosis. Cell Rep. 2018, 23, 3946–3959.e6. [Google Scholar] [CrossRef]
- Faget, J.; Peters, S.; Quantin, X.; Meylan, E.; Bonnefoy, N. Neutrophils in the era of immune checkpoint blockade. J. Immunother. Cancer 2021, 9, e002242. [Google Scholar] [CrossRef] [PubMed]
- Valero, C.; Lee, M.; Hoen, D.; Weiss, K.; Kelly, D.W.; Adusumilli, P.S.; Paik, P.K.; Plitas, G.; Ladanyi, M.; Postow, M.A.; et al. Pretreatment neutrophil-to-lymphocyte ratio and mutational burden as biomarkers of tumor response to immune checkpoint inhibitors. Nat. Commun. 2021, 12, 729. [Google Scholar] [CrossRef] [PubMed]
- Sui, Q.; Zhang, X.; Chen, C.; Tang, J.; Yu, J.; Li, W.; Han, K.; Jiang, W.; Liao, L.; Kong, L.; et al. Inflammation promotes resistance to immune checkpoint inhibitors in high microsatellite instability colorectal cancer. Nat. Commun. 2022, 13, 7316. [Google Scholar] [CrossRef] [PubMed]
- Rebuzzi, S.E.; Prelaj, A.; Friedlaender, A.; Cortellini, A.; Addeo, A.; Genova, C.; Naqash, A.R.; Auclin, E.; Mezquita, L.; Banna, G.L. Prognostic scores including peripheral blood-derived inflammatory indices in patients with advanced non-small-cell lung cancer treated with immune checkpoint inhibitors. Crit. Rev. Oncol. Hematol. 2022, 179, 103806. [Google Scholar] [CrossRef] [PubMed]
- Que, H.; Fu, Q.; Lan, T.; Tian, X.; Wei, X. Tumor-associated neutrophils and neutrophil-targeted cancer therapies. Biochim. Biophys. Acta Rev. Cancer 2022, 1877, 188762. [Google Scholar] [CrossRef] [PubMed]
- Adrover, J.M.; McDowell, S.A.C.; He, X.Y.; Quail, D.F.; Egeblad, M. NETworking with cancer: The bidirectional interplay between cancer and neutrophil extracellular traps. Cancer Cell 2023, 41, 505–526. [Google Scholar] [CrossRef] [PubMed]
- Eruslanov, E.B.; Bhojnagarwala, P.S.; Quatromoni, J.G.; Stephen, T.L.; Ranganathan, A.; Deshpande, C.; Akimova, T.; Vachani, A.; Litzky, L.; Hancock, W.W.; et al. Tumor-associated neutrophils stimulate T cell responses in early-stage human lung cancer. J. Clin. Investig. 2014, 124, 5466–5480. [Google Scholar] [CrossRef]
- Akbay, E.A.; Koyama, S.; Liu, Y.; Dries, R.; Bufe, L.E.; Silkes, M.; Alam, M.M.; Magee, D.M.; Jones, R.; Jinushi, M.; et al. Interleukin-17A Promotes Lung Tumor Progression through Neutrophil Attraction to Tumor Sites and Mediating Resistance to PD-1 Blockade. J. Thorac. Oncol. 2017, 12, 1268–1279. [Google Scholar] [CrossRef]
- Schalper, K.A.; Carleton, M.; Zhou, M.; Chen, T.; Feng, Y.; Huang, S.P.; Walsh, A.M.; Baxi, V.; Pandya, D.; Baradet, T.; et al. Elevated serum interleukin-8 is associated with enhanced intratumor neutrophils and reduced clinical benefit of immune-checkpoint inhibitors. Nat. Med. 2020, 26, 688–692. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Hildesheim, A.; Engels, E.A.; Kemp, T.J.; Park, J.H.; Katki, H.A.; Koshiol, J.; Shelton, G.; Caporaso, N.E.; et al. Circulating inflammation markers and prospective risk for lung cancer. J. Natl. Cancer Inst. 2013, 105, 1871–1880. [Google Scholar] [CrossRef]
- Xie, X.; Shi, Q.; Wu, P.; Zhang, X.; Kambara, H.; Su, J.; Yu, H.; Park, S.Y.; Guo, R.; Ren, Q.; et al. Single-cell transcriptome profiling reveals neutrophil heterogeneity in homeostasis and infection. Nat. Immunol. 2020, 21, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Zhao, W.; Li, Y.; Ying, Z.; Luo, Y.; Wang, Q.; Li, X.; Lu, W.; Dong, X.; Wu, Y.; et al. Prediction of risk and overall survival of pancreatic cancer from blood soluble immune checkpoint-related proteins. Front. Immunol. 2023, 14, 1189161. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; He, Y.; Li, W.; Xu, X.; Hu, Q.; Bian, Z.; Xu, A.; Tu, H.; Wu, M.; Wu, X. Soluble Immune Checkpoint-Related Proteins in Blood Are Associated With Invasion and Progression in Non-Small Cell Lung Cancer. Front. Immunol. 2022, 13, 887916. [Google Scholar] [CrossRef] [PubMed]
- Muri, J.; Cecchinato, V.; Cavalli, A.; Shanbhag, A.A.; Matkovic, M.; Biggiogero, M.; Maida, P.A.; Moritz, J.; Toscano, C.; Ghovehoud, E.; et al. Autoantibodies against chemokines post-SARS-CoV-2 infection correlate with disease course. Nat. Immunol. 2023, 24, 604–611. [Google Scholar] [CrossRef]
- Genchi, A.; Brambilla, E.; Sangalli, F.; Radaelli, M.; Bacigaluppi, M.; Furlan, R.; Andolfo, A.; Drago, D.; Magagnotti, C.; Scotti, G.M.; et al. Neural stem cell transplantation in patients with progressive multiple sclerosis: An open-label, phase 1 study. Nat. Med. 2023, 29, 75–85. [Google Scholar] [CrossRef]
- Zhao, Y.; Rahmy, S.; Liu, Z.; Zhang, C.; Lu, X. Rational targeting of immunosuppressive neutrophils in cancer. Pharmacol. Ther. 2020, 212, 107556. [Google Scholar] [CrossRef]
- Schett, G.; Dayer, J.M.; Manger, B. Interleukin-1 function and role in rheumatic disease. Nat. Rev. Rheumatol. 2016, 12, 14–24. [Google Scholar] [CrossRef]
- Afonina, I.S.; Müller, C.; Martin, S.J.; Beyaert, R. Proteolytic Processing of Interleukin-1 Family Cytokines: Variations on a Common Theme. Immunity 2015, 42, 991–1004. [Google Scholar] [CrossRef]
- Isailovic, N.; Daigo, K.; Mantovani, A.; Selmi, C. Interleukin-17 and innate immunity in infections and chronic inflammation. J. Autoimmun. 2015, 60, 1–11. [Google Scholar] [CrossRef]
- De Filippo, K.; Dudeck, A.; Hasenberg, M.; Nye, E.; van Rooijen, N.; Hartmann, K.; Gunzer, M.; Roers, A.; Hogg, N. Mast cell and macrophage chemokines CXCL1/CXCL2 control the early stage of neutrophil recruitment during tissue inflammation. Blood 2013, 121, 4930–4937. [Google Scholar] [CrossRef]
- Zhou, S.L.; Dai, Z.; Zhou, Z.J.; Wang, X.Y.; Yang, G.H.; Wang, Z.; Huang, X.W.; Fan, J.; Zhou, J. Overexpression of CXCL5 mediates neutrophil infiltration and indicates poor prognosis for hepatocellular carcinoma. Hepatology 2012, 56, 2242–2254. [Google Scholar] [CrossRef] [PubMed]
- Pylaeva, E.; Lang, S.; Jablonska, J. The Essential Role of Type I Interferons in Differentiation and Activation of Tumor-Associated Neutrophils. Front. Immunol. 2016, 7, 629. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Zhu, B.; Chen, D. Type I interferon-mediated tumor immunity and its role in immunotherapy. Cell Mol. Life Sci. 2022, 79, 191. [Google Scholar] [CrossRef] [PubMed]
- The blood proteome of imminent lung cancer diagnosis. Nat. Commun. 2023, 14, 3042. [CrossRef] [PubMed]
- Wang, T.; Du, G.; Wang, D. The S100 protein family in lung cancer. Clin. Chim. Acta 2021, 520, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Ancel, J.; Dormoy, V.; Raby, B.N.; Dalstein, V.; Durlach, A.; Dewolf, M.; Gilles, C.; Polette, M.; Deslée, G. Soluble biomarkers to predict clinical outcomes in non-small cell lung cancer treated by immune checkpoints inhibitors. Front. Immunol. 2023, 14, 1171649. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Raices, M.; Cayol, F.; Corvatta, F.; Caram, L.; Dietrich, A. Is the neutrophil-to-lymphocyte ratio a prognostic factor in non-small cell lung cancer patients who receive adjuvant chemotherapy? Semin. Oncol. 2022, 49, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef]
- Wang, F.; Chen, L.; Wang, Z.; Xu, Q.; Huang, H.; Wang, H.; Li, X.; Yu, M.; Chen, J.; Lin, F.; et al. Prognostic value of the modified systemic inflammation score in non-small-cell lung cancer with brain metastasis. Cancer Cell Int. 2022, 22, 320. [Google Scholar] [CrossRef]
- Liu, W.; Ren, S.; Yang, L.; Xiao, Y.; Zeng, C.; Chen, C.; Wu, F.; Hu, Y. The predictive role of hematologic markers in resectable nsclc patients treated with neoadjuvant chemoimmunotherapy: A retrospective cohort study. Int. J. Surg. 2023, 109, 3519–3526. [Google Scholar] [CrossRef]
- Nøst, T.H.; Alcala, K.; Urbarova, I.; Byrne, K.S.; Guida, F.; Sandanger, T.M.; Johansson, M. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur. J. Epidemiol. 2021, 36, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.C.; Neelapu, S.S.; Giavridis, T.; Sadelain, M. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nat. Rev. Immunol. 2022, 22, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Manzoor, S.; Siddiqui, S.; Mariappan, N.; Zafar, I.; Ahmad, A.; Ahmad, A. Epigenetic underpinnings of inflammation: Connecting the dots between pulmonary diseases, lung cancer and COVID-19. Semin. Cancer Biol. 2022, 83, 384–398. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Karin, M. IL-6 and related cytokines as the critical lynchpins between inflammation and cancer. Semin. Immunol. 2014, 26, 54–74. [Google Scholar] [CrossRef]
- Zhou, B.; Liu, J.; Wang, Z.M.; Xi, T. C-reactive protein, interleukin 6 and lung cancer risk: A meta-analysis. PLoS ONE 2012, 7, e43075. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.C.; Yang, C.C.; Yang, Y.F.; Yan, L.J.; Ding, Z.N.; Liu, H.; Yan, Y.C.; Dong, Z.R.; Wang, D.X.; Li, T. Peripheral cytokine levels as novel predictors of survival in cancer patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Front. Immunol. 2022, 13, 884592. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Yang, L.; Xu, H.; Zheng, S.; Wang, Z.; Wang, S.; Yang, Y.; Zhang, S.; Feng, X.; Sun, N.; et al. Systematic analysis of IL-6 as a predictive biomarker and desensitizer of immunotherapy responses in patients with non-small cell lung cancer. BMC Med. 2022, 20, 187. [Google Scholar] [CrossRef]
- Barrera, L.; Montes-Servín, E.; Barrera, A.; Ramírez-Tirado, L.A.; Salinas-Parra, F.; Bañales-Méndez, J.L.; Sandoval-Ríos, M.; Arrieta, Ó. Cytokine profile determined by data-mining analysis set into clusters of non-small-cell lung cancer patients according to prognosis. Ann. Oncol. 2015, 26, 428–435. [Google Scholar] [CrossRef]
- Chang, C.H.; Hsiao, C.F.; Yeh, Y.M.; Chang, G.C.; Tsai, Y.H.; Chen, Y.M.; Huang, M.S.; Chen, H.L.; Li, Y.J.; Yang, P.C.; et al. Circulating interleukin-6 level is a prognostic marker for survival in advanced nonsmall cell lung cancer patients treated with chemotherapy. Int. J. Cancer 2013, 132, 1977–1985. [Google Scholar] [CrossRef]
- Enewold, L.; Mechanic, L.E.; Bowman, E.D.; Zheng, Y.L.; Yu, Z.; Trivers, G.; Alberg, A.J.; Harris, C.C. Serum concentrations of cytokines and lung cancer survival in African Americans and Caucasians. Cancer Epidemiol. Biomark. Prev. 2009, 18, 215–222. [Google Scholar] [CrossRef]
- Pine, S.R.; Mechanic, L.E.; Enewold, L.; Chaturvedi, A.K.; Katki, H.A.; Zheng, Y.L.; Bowman, E.D.; Engels, E.A.; Caporaso, N.E.; Harris, C.C. Increased levels of circulating interleukin 6, interleukin 8, C-reactive protein, and risk of lung cancer. J. Natl. Cancer Inst. 2011, 103, 1112–1122. [Google Scholar] [CrossRef] [PubMed]
- Ohishi, W.; Cologne, J.B.; Fujiwara, S.; Suzuki, G.; Hayashi, T.; Niwa, Y.; Akahoshi, M.; Ueda, K.; Tsuge, M.; Chayama, K. Serum interleukin-6 associated with hepatocellular carcinoma risk: A nested case-control study. Int. J. Cancer 2014, 134, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Boersma, B.; Jiskoot, W.; Lowe, P.; Bourquin, C. The interleukin-1 cytokine family members: Role in cancer pathogenesis and potential therapeutic applications in cancer immunotherapy. Cytokine Growth Factor. Rev. 2021, 62, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Shao, M.; Chen, Y.; Zhou, J.; Qian, J.; Xu, L.; Ma, H.; Wang, X.; Xu, Y.; Lu, D.; et al. Allele 2 of the interleukin-1 receptor antagonist gene (IL1RN*2) is associated with a decreased risk of primary lung cancer. Cancer Lett. 2006, 236, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, G.; Colafrancesco, S.; Emmi, G.; Imazio, M.; Lopalco, G.; Maggio, M.C.; Sota, J.; Dinarello, C.A. Interleukin 1α: A comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun. Rev. 2021, 20, 102763. [Google Scholar] [CrossRef] [PubMed]
- Palomo, J.; Dietrich, D.; Martin, P.; Palmer, G.; Gabay, C. The interleukin (IL)-1 cytokine family--Balance between agonists and antagonists in inflammatory diseases. Cytokine 2015, 76, 25–37. [Google Scholar] [CrossRef]
- Wu, T.C.; Xu, K.; Martinek, J.; Young, R.R.; Banchereau, R.; George, J.; Turner, J.; Kim, K.I.; Zurawski, S.; Wang, X.; et al. IL1 Receptor Antagonist Controls Transcriptional Signature of Inflammation in Patients with Metastatic Breast Cancer. Cancer Res. 2018, 78, 5243–5258. [Google Scholar] [CrossRef]
- Mantovani, A.; Dinarello, C.A.; Molgora, M.; Garlanda, C. Interleukin-1 and Related Cytokines in the Regulation of Inflammation and Immunity. Immunity 2019, 50, 778–795. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
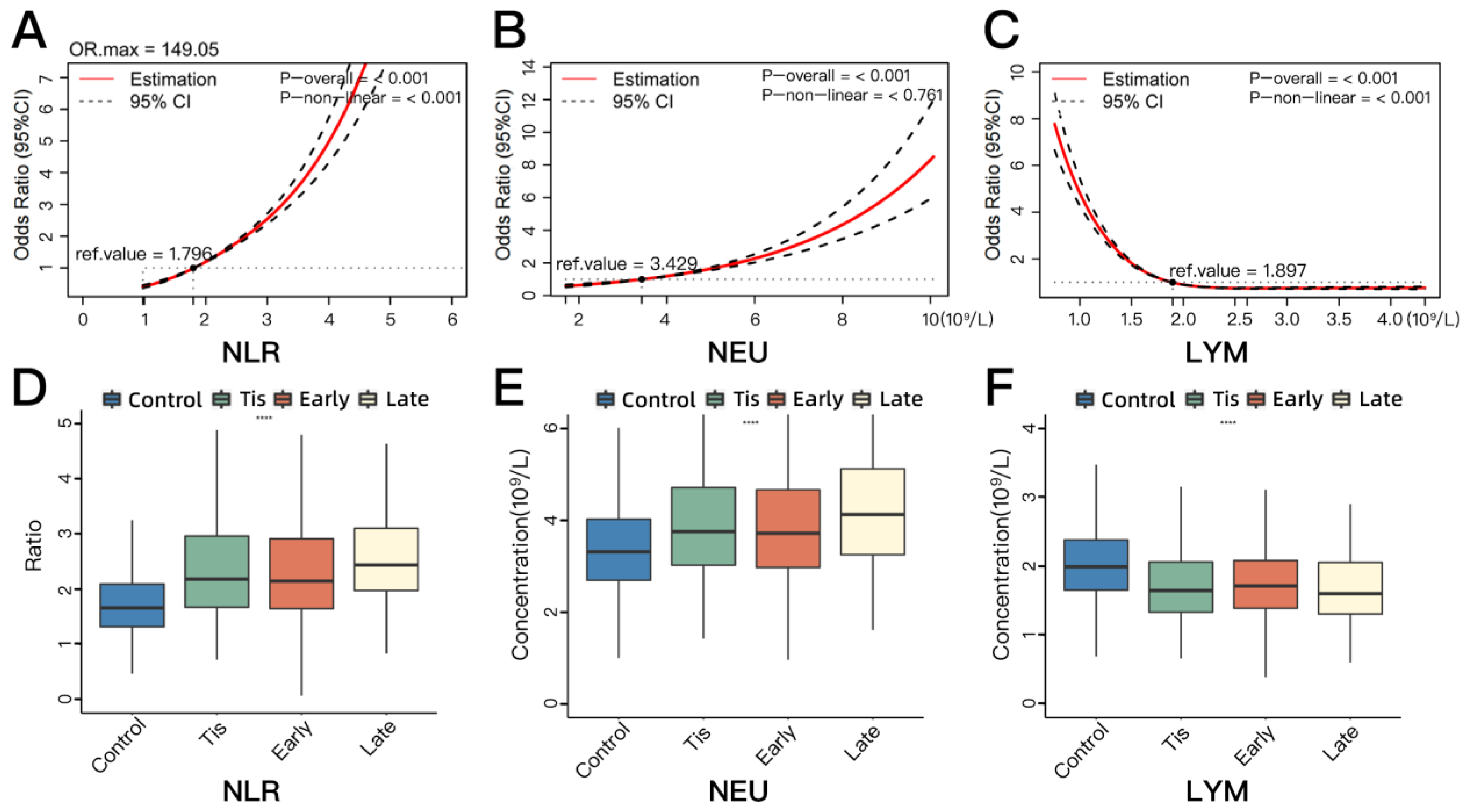
| Markers | Control (n = 6791) Median [Q1–Q3] | NSCLC (n = 3942) Median [Q1–Q3] | * p | ** p | *** p | **** p | ||
|---|---|---|---|---|---|---|---|---|
| Tis (n = 450) | Early (n = 3376) | Late (n = 116) | ||||||
| NLR | 1.657 [1.315–2.090] | 2.179 [1.670–2.962] | 2.142 [1.644–2.911] | 2.436 [1.972–3.102] | <0.001 | <0.001 | 0.332 | <0.001 |
| NEU (109/L) | 3.310 [2.690–4.020] | 3.750 [3.020–4.710] | 3.715 [2.970–4.660] | 4.120 [3.248–5.115] | <0.001 | <0.001 | 0.670 | 0.005 |
| LYM (109/L) | 1.990 [1.650–2.380] | 1.645 [1.333–2.060] | 1.710 [1.388–2.080] | 1.600 [1.305–2.053] | <0.001 | <0.001 | 0.360 | 0.142 |
| Markers | Control (n = 66) | NSCLC (n = 132) | OR (95% CI) * | p Value * | OR (95% CI) **, a | p Value **, a |
|---|---|---|---|---|---|---|
| IL-6 | ||||||
| Low | 34 (51.52) | 15 (11.36) | 1 (ref) | <0.001 | 1 (ref) | <0.001 |
| High | 32 (48.48) | 117 (88.64) | 9.339 (3.882, 22.464) | 10.687 (3.875, 29.473) | ||
| CXCL2 | ||||||
| Low | 33 (50.00) | 52 (39.39) | 1 (ref) | 0.151 | 1 (ref) | 0.196 |
| High | 33 (50.00) | 80 (6.61) | 1.570 (0.848, 2.907) | 1.824 (0.903, 3.683) | ||
| IL-1RA | ||||||
| Low | 33 (50.00) | 17 (12.88) | 1 (ref) | <0.001 | 1 (ref) | <0.001 |
| High | 33 (50.00) | 115 (87.12) | 7.535 (3.293, 17.244) | 8.113 (3.182, 20.689) | ||
| IL-1α | ||||||
| Low | 33 (50.00) | 64 (48.48) | 1 (ref) | 0.849 | 1 (ref) | 0.615 |
| High | 33 (50.00) | 68 (51.52) | 1.056 (0.603, 1.850) | 1.314 (0.700, 2.466) | ||
| CXCL5 | ||||||
| Low | 33 (50.00) | 62 (46.97) | 1 (ref) | 0.703 | 1 (ref) | 0.594 |
| High | 33 (50.00) | 70 (53.3) | 1.116 (0.636, 1.958) | 1.371 (0.719, 2.613) | ||
| S100B | ||||||
| Low | 42 (63.64) | 70 (53.3) | 1 (ref) | 0.184 | 1 (ref) | 0.531 |
| High | 24 (36.36) | 62 (46.97) | 1.481 (0.830, 2.645) | 1.287 (0.663, 2.501) | ||
| GM-CSF | ||||||
| Low | 52 (78.79) | 100 (75.76) | 1 (ref) | 0.633 | 1 (ref) | 0.611 |
| High | 14 (21.21) | 32 (24.24) | 1.191 (0.582, 2.436) | 1.294 (0.563, 2.977) |
| Models | NRI | 95% CI a | * p Value | IDI | 95% CI b | ** p Value |
|---|---|---|---|---|---|---|
| Model 1 vs. Model 2 | 59.85% | 0.331, 0.935 | <0.001 | 0.128 | 0.079, 0.176 | <0.001 |
| Model 2 vs. Model 2 + IL-6 | 75.00% | 0.319, 1.022 | <0.001 | 0.148 | 0.092, 0.203 | <0.001 |
| Model 2 vs. Model 2 + IL-1RA | 61.36% | 0.122, 0.962 | 0.003 | 0.122 | 0.068, 0.176 | <0.001 |
| Model 2 + IL-6 vs. Model 3 | 16.67% | −0.055, 0.779 | 0.423 | 0.050 | 0.012, 0.088 | 0.010 |
| Model 2 + IL-1RA vs. Model 3 | 29.55% | −0.001, 0.866 | 0.227 | 0.076 | 0.033, 0.119 | 0.001 |
| Model 2 vs. Model 3 | 97.73% | 0.667, 1.279 | <0.001 | 0.198 | 0.137, 0.259 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, Y.; Wang, Q.; Xu, C.; Guo, Q.; Dai, R.; Xu, X.; Zhang, Y.; Wu, M.; Wu, X.; Tu, H. Combining Classic and Novel Neutrophil-Related Biomarkers to Identify Non-Small-Cell Lung Cancer. Cancers 2024, 16, 513. https://doi.org/10.3390/cancers16030513
Ren Y, Wang Q, Xu C, Guo Q, Dai R, Xu X, Zhang Y, Wu M, Wu X, Tu H. Combining Classic and Novel Neutrophil-Related Biomarkers to Identify Non-Small-Cell Lung Cancer. Cancers. 2024; 16(3):513. https://doi.org/10.3390/cancers16030513
Chicago/Turabian StyleRen, Yunzhao, Qinchuan Wang, Chenyang Xu, Qian Guo, Ruoqi Dai, Xiaohang Xu, Yuhao Zhang, Ming Wu, Xifeng Wu, and Huakang Tu. 2024. "Combining Classic and Novel Neutrophil-Related Biomarkers to Identify Non-Small-Cell Lung Cancer" Cancers 16, no. 3: 513. https://doi.org/10.3390/cancers16030513
APA StyleRen, Y., Wang, Q., Xu, C., Guo, Q., Dai, R., Xu, X., Zhang, Y., Wu, M., Wu, X., & Tu, H. (2024). Combining Classic and Novel Neutrophil-Related Biomarkers to Identify Non-Small-Cell Lung Cancer. Cancers, 16(3), 513. https://doi.org/10.3390/cancers16030513