
How Is the Spectrum of Sarcoma Surgery Assessed?

 ,
,  ,
,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
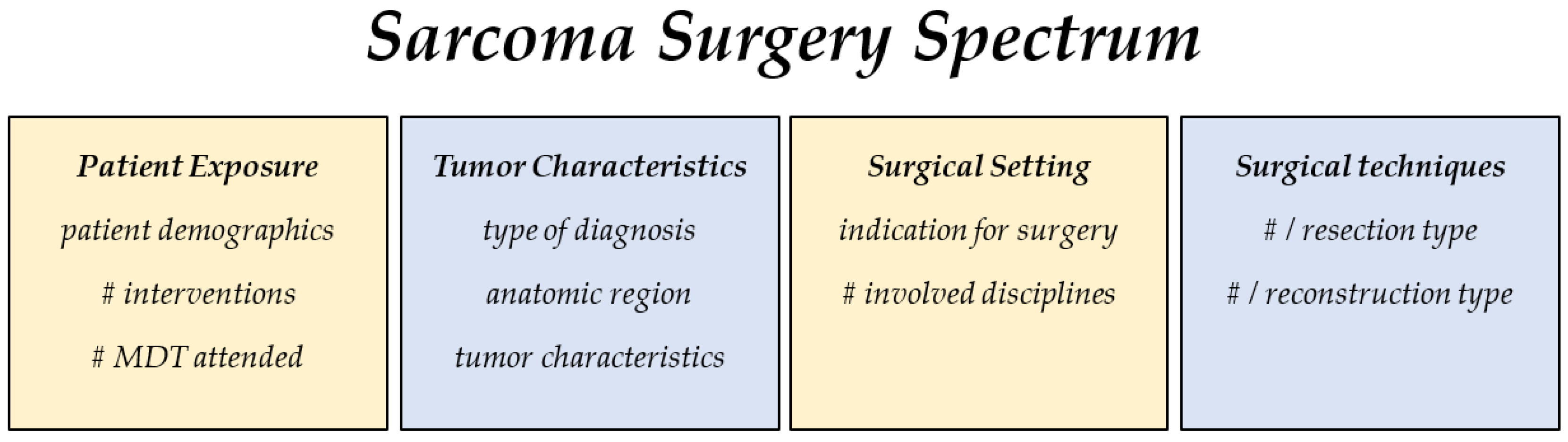
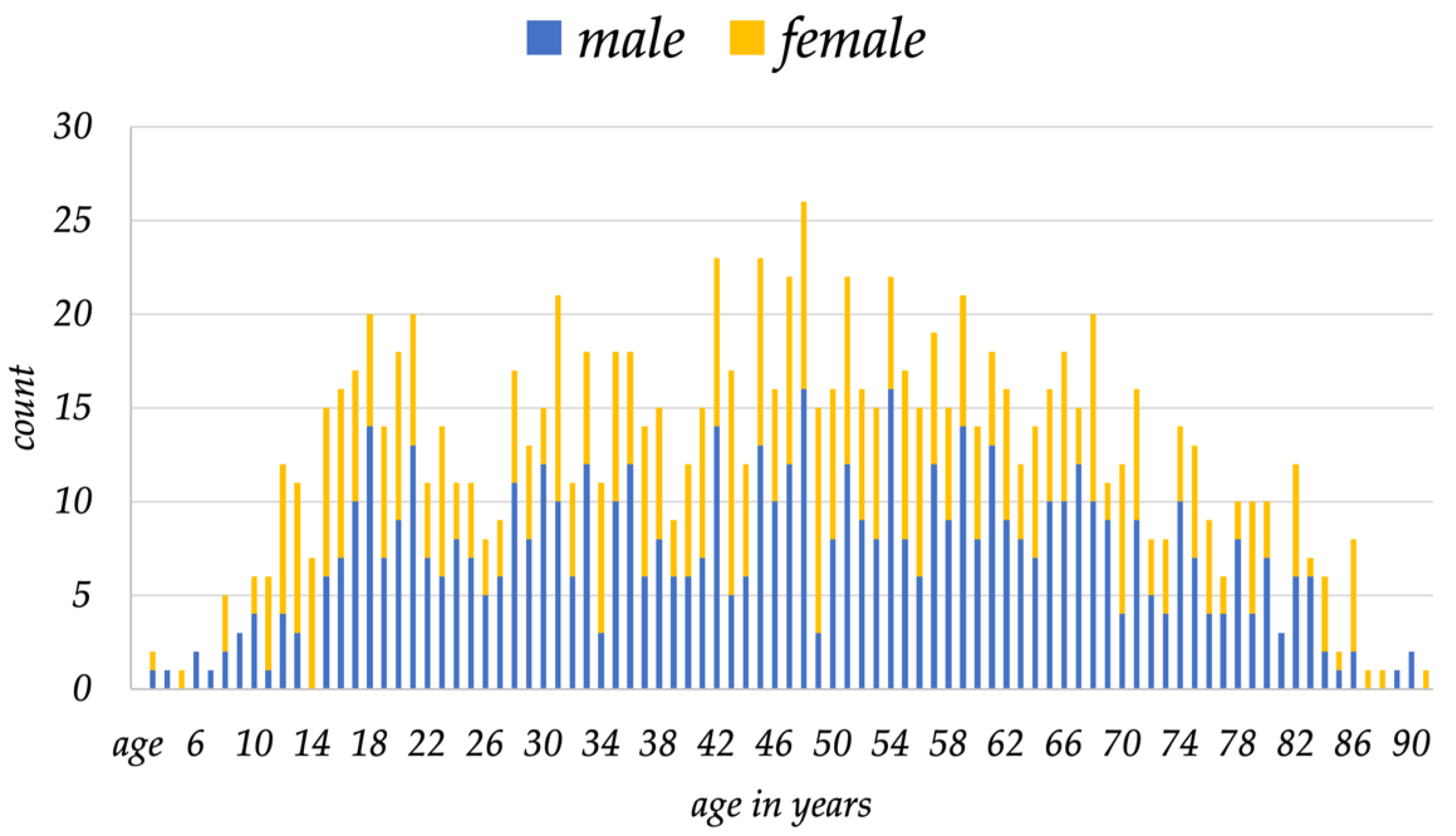
3.1. Patient Exposure
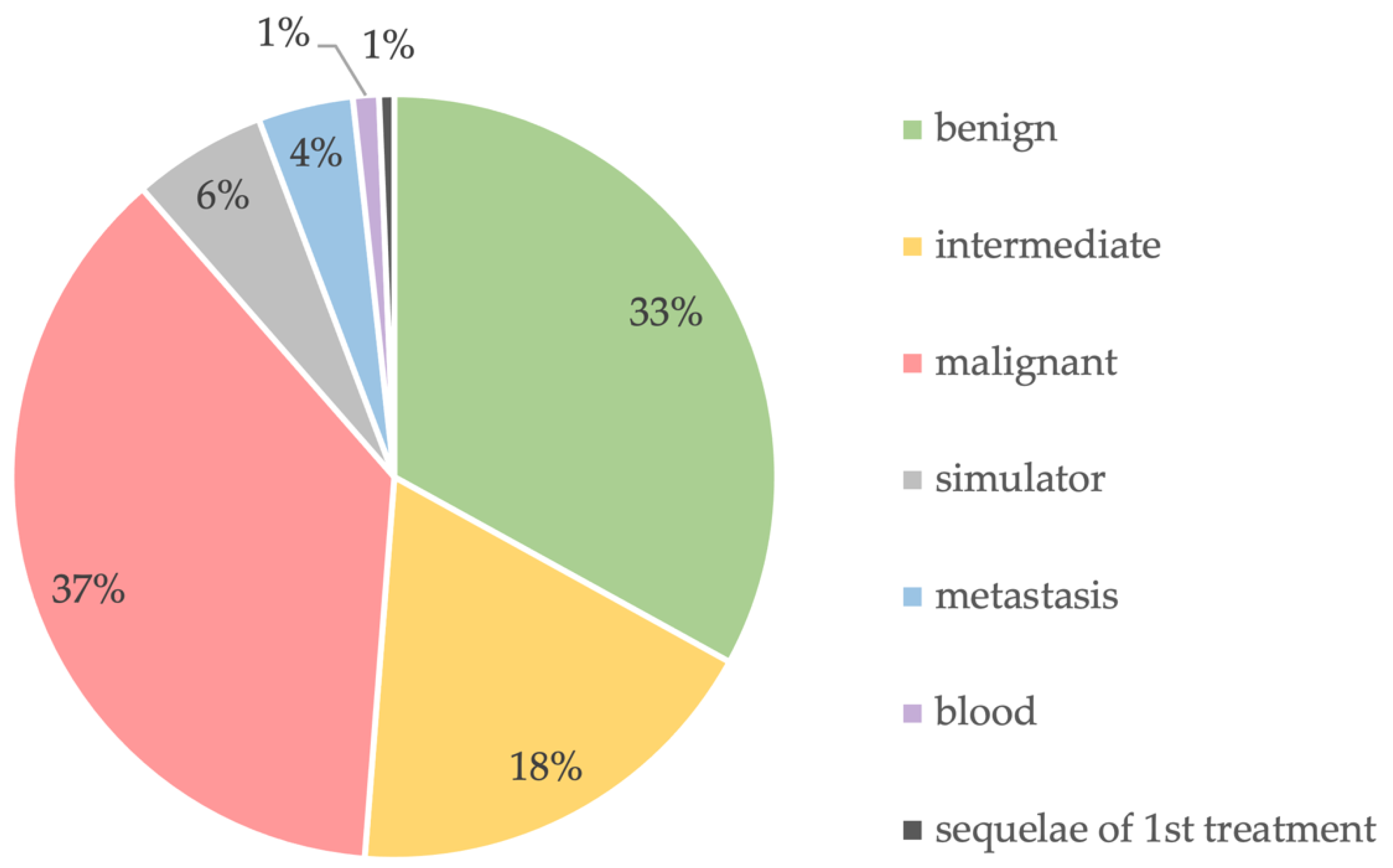
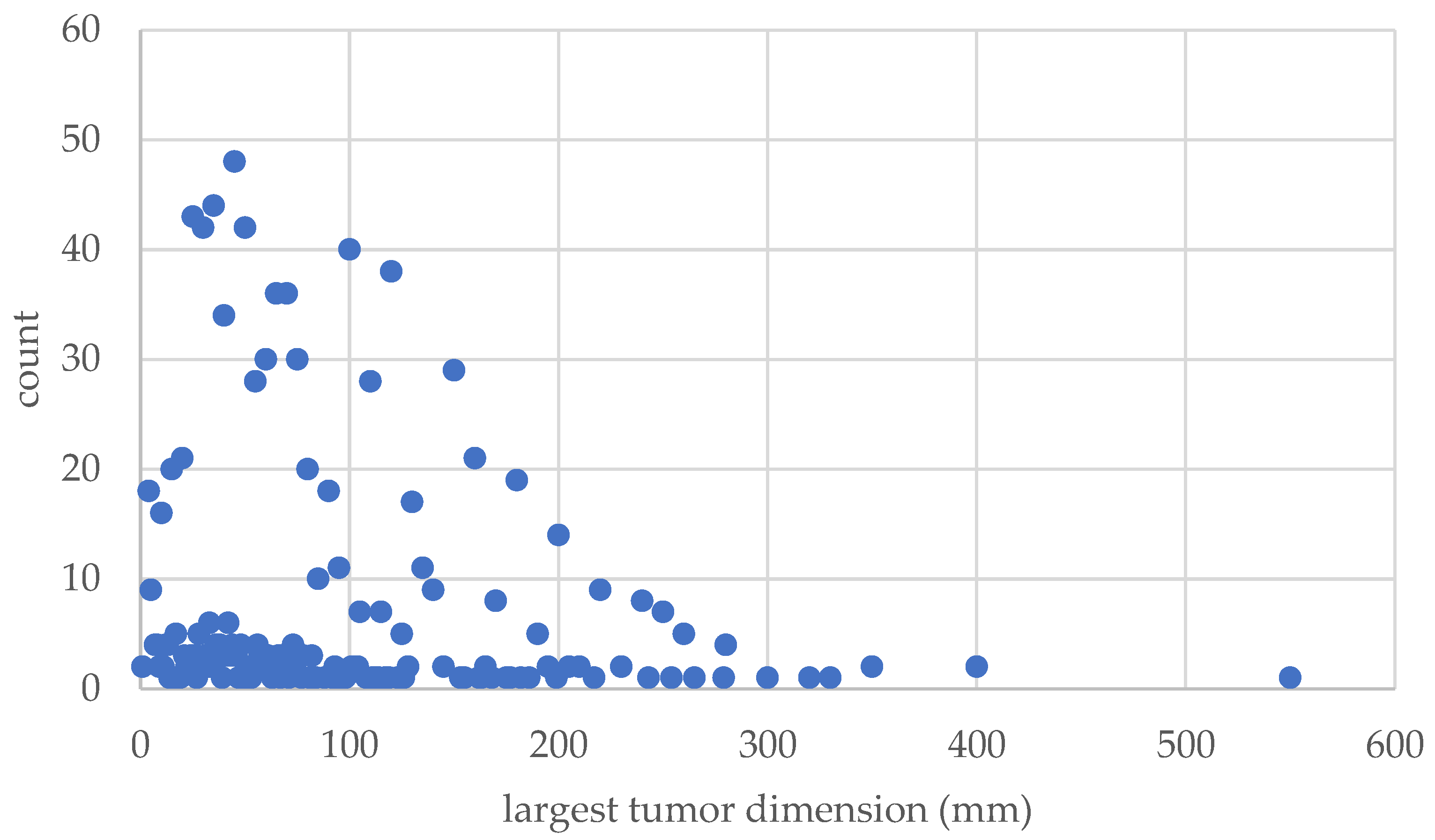
3.2. Tumor Characteristics
3.3. Surgical Settings
3.4. Surgical Techniques
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blay, J.Y.; Soibinet, P.; Penel, N.; Bompas, E.; Duffaud, F.; Stoeckle, E.; Mir, O.; Adam, J.; Chevreau, C.; Bonvalot, S.; et al. Improved Survival Using Specialized Multidisciplinary Board in Sarcoma Patients. Ann. Oncol. 2017, 28, 2852–2859. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.Y.; Bonvalot, S.; Gouin, F.; le Cesne, A.; Penel, N. Criteria for Reference Centers for Sarcomas: Volume but Also Long-Term Multidisciplinary Organisation. Ann. Oncol. 2019, 30, 2008–2009. [Google Scholar] [CrossRef] [PubMed]
- Heiden, B.T.; Kozower, B.D. Keeping a Safe Distance From Surgical Volume Standards. J. Clin. Oncol. 2022, 40, 1033–1035. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H. From Volume to Value in Health Care: The Work Begins. JAMA 2016, 316, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence Improving Outcomes for People with Sarcoma. Available online: https://www.nice.org.uk/guidance/csg9 (accessed on 20 June 2022).
- Heesen, P.; Studer, G.; Bode, B.; Windegger, H.; Staeheli, B.; Aliu, P.; Martin-Broto, J.; Gronchi, A.; Blay, J.Y.; Le Cesne, A.; et al. Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators. Cancers 2022, 15, 47. [Google Scholar] [CrossRef] [PubMed]
- Biau, D.J.; Ferguson, P.C.; Chung, P.; Griffin, A.M.; Catton, C.N.; O’Sullivan, B.; Wunder, J.S. Local Recurrence of Localized Soft Tissue Sarcoma: A New Look at Old Predictors. Cancer 2012, 118, 5867–5877. [Google Scholar] [CrossRef]
- Henshaw, R.M. The Role of Surgery in the Multidisciplinary Care of Sarcoma. In Sarcoma: A Multidisciplinary Approach to Treatment; Henshaw, R.M., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 69–116. ISBN 978-3-319-43121-5. [Google Scholar]
- Balch, C. What Is a Surgical Oncologist? Ann. Surg. Oncol. 2018, 1, 7–9. [Google Scholar] [CrossRef]
- Are, C.; McMasters, K.M.; Giuliano, A.; Balch, C.; Anderson, B.O.; Berman, R.; Audisio, R.; Kovacs, T.; Savant, D.; Toprani, R.; et al. Global Forum of Cancer Surgeons: A Steady Voice for Cancer Surgeons to Improve Surgical Care for Cancer Patients Globally. Ann. Surg. Oncol. 2018, 25, 2114–2116. [Google Scholar] [CrossRef]
- Porter, M.E.; Lee, T.H. Integrated Practice Units: A Playbook for Health Care Leaders. NEJM Catal. 2021, 2. [Google Scholar] [CrossRef]
- Porter, M.E.; Lee, T.H.; Murray, A.C.A. The Value-Based Geography Model of Care. NEJM Catal. 2020, 1. [Google Scholar] [CrossRef]
- Porter, M.E.; School, H.B. Redefining Health Care: Creating Value-Based Competition on Results; Harvard Business School Press: Brighton, MA, USA, 2006. [Google Scholar]
- Fuchs, B.; Studer, G.; Bode, B.; Wellauer, H.; Frei, A.; Theus, C.; Schüpfer, G.; Plock, J.; Windegger, H.; Breitenstein, S. Development of a Value-Based Healthcare Delivery Model for Sarcoma Patients. Swiss Med. Wkly. 2021, 151, w30047. [Google Scholar] [CrossRef] [PubMed]
- Sambri, A.; Caldari, E.; Fiore, M.; Zucchini, R.; Giannini, C.; Pirini, M.G.; Spinnato, P.; Cappelli, A.; Donati, D.M.; de Paolis, M. Margin Assessment in Soft Tissue Sarcomas: Review of the Literature. Cancers 2021, 13, 1687. [Google Scholar] [CrossRef]
- Bonvalot, S.; Gaignard, E.; Stoeckle, E.; Meeus, P.; Decanter, G.; Carrere, S.; Honore, C.; Delhorme, J.B.; Fau, M.; Tzanis, D.; et al. Survival Benefit of the Surgical Management of Retroperitoneal Sarcoma in a Reference Center: A Nationwide Study of the French Sarcoma Group from the NetSarc Database. Ann. Surg. Oncol. 2019, 26, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Boussard, T.; Macklin, P.; Greenspan, E.J.; Gryshuk, A.L.; Stahlberg, E.; Syeda-Mahmood, T.; Shmulevich, I. Digital Twins for Predictive Oncology Will Be a Paradigm Shift for Precision Cancer Care. Nat. Med. 2021, 27, 2065–2066. [Google Scholar] [CrossRef] [PubMed]
- Frei, A.; Scaglioni, M.F.; Giovanoli, P.; Breitenstein, S.; Heesen, P.; Fuchs, B. Definition of the Surgical Case Complexity in the Treatment of Soft Tissue Tumors of the Extremities and Trunk. Cancers 2022, 14, 1559. [Google Scholar] [CrossRef] [PubMed]
- Shamout, F.; Zhu, T.; Clifton, D.A. Machine Learning for Clinical Outcome Prediction. IEEE Rev. Biomed. Eng. 2021, 14, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, N.; Ahmed, A.R.; Matsumoto, S.; Manabe, J.; Matsushita, Y. The Concept of Curative Margin in Surgery for Bone and Soft Tissue Sarcoma. Clin. Orthop. Relat. Res. 2004, 419, 165–172. [Google Scholar] [CrossRef]
- Harati, K.; Goertz, O.; Pieper, A.; Daigeler, A.; Joneidi-Jafari, H.; Niggemann, H.; Stricker, I.; Lehnhardt, M. Soft Tissue Sarcomas of the Extremities: Surgical Margins Can Be Close as Long as the Resected Tumor Has No Ink on It. Oncologist 2017, 22, 1400–1410. [Google Scholar] [CrossRef]
- Fuchs, B.; Bode, B.; Studer, G.; Breitenstein, S. Wie Entwickelt Sich Die Sarkomchirurgie? Available online: https://www.universimed.com/ch/article/onkologie/wie-sarkomchirurgie-38855 (accessed on 20 June 2022).
- Blay, J.Y.; Honoré, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in Reference Centers Improves Survival of Sarcoma Patients: A Nationwide Study. Ann. Oncol. 2019, 30, 1143–1153. [Google Scholar] [CrossRef]
- Hohenberger, P.; Linder, L. FAQ’s Zum Erhebungsbogen Für Sarkomzentren Modul Im Onkologischen Zentrum. Available online: https://www.onkozert.de/wordpress/wp-content/uploads/2022/01/eb_msar-D_faq_211117.pdf?v=56457126 (accessed on 20 June 2022).
- White, J.; Toy, P.; Gibbs, P.; Enneking, W.; Scarborough, M. The Current Practice of Orthopaedic Oncology in North America. Clin. Orthop. Relat. Res. 2010, 468, 2840–2853. [Google Scholar] [CrossRef]
- Baum, P.; Lenzi, J.; Diers, J.; Rust, C.; Eichhorn, M.E.; Taber, S.; Germer, C.-T.; Winter, H.; Wiegering, A. Risk-Adjusted Mortality Rates as a Quality Proxy Outperform Volume in Surgical Oncology—A New Perspective on Hospital Centralization Using National Population-Based Data. J. Clin. Oncol. 2022, 40, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pujade Lauraine, E.; le Cesne, A.; Pautier, P.; Vacher Lavenue, M.C.; Trama, A.; Casali, P.; Coindre, J.M.; Blay, J.Y. Improving Treatment Results with Reference Centres for Rare Cancers: Where Do We Stand? Eur. J. Cancer 2017, 77, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Lazarides, A.L.; Kerr, D.L.; Nussbaum, D.P.; Kreulen, R.T.; Somarelli, J.A.; Blazer, D.G.; Brigman, B.E.; Eward, W.C. Soft Tissue Sarcoma of the Extremities: What Is the Value of Treating at High-Volume Centers? Clin. Orthop. Relat. Res. 2019, 477, 718–727. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Soft Tissue | 628 | Bone | 339 |
|---|---|---|---|
| Adipocytic | 258 | Chondrogenic | 141 |
| Fibroblastic/myofibroblastic | 97 | Osteogenic | 90 |
| Undifferentiated/unclassified sarcoma | 82 | Tumors of undefined neoplastic nature | 45 |
| Tumors of uncertain differentiation | 71 | Osteoclastic giant cell rich | 24 |
| Nerve sheath tumors | 49 | Ewing | 18 |
| Fibro-histiocytic tumors | 21 | Notochordal tumors | 7 |
| Vascular tumors of soft tumors | 14 | Undifferentiated high-grade pleomorphic sarcoma | 4 |
| Smooth muscle tumors | 19 | Fibrohistiocytic | 3 |
| Chondro-osseous tumors | 10 | Fibrogenic | 2 |
| Pericytic tumors | 4 | Myogenic, lipogenic, epithelial tumors | 2 |
| Skeletal muscle tumors | 4 | Tumor syndromes | 2 |
| Vascular tumors | 1 | ||
| Non-neoplastic/simulator | 62 | ||
| Metastasis | 44 | ||
| Lymphoma myeloma leukemia | 12 | ||
| Sequelae of prior therapy | 8 | ||
| Resection | Count | Reconstruction | Count |
|---|---|---|---|
| Bone | 489 | Bone | 319 |
| simple curettage | 107 | cementation | 18 |
| rotationplasty (lower extremity) | 2 | ORIF (incl. bone ankers; removal of OS material) | 61 |
| hemi-cortex resection | 20 | autograft | 11 |
| complete bone resection: extra-articular | 108 | vascularized fibula autograft (based on fibular artery) | 10 |
| complete bone resection: transarticular | 92 | non-vascularized fibula autograft | 1 |
| with 3D patient-specific cutting guides | 23 | allograft chips | 45 |
| radiofrequency ablation (RFA); cryotherapy, MR-HIFU | 41 | bulk allograft | 32 |
| tendon resection | 2 | conventional prosthesis | 9 |
| ligament resection | 1 | modular tumor prosthesis | 79 |
| forced epiphyseolysis OT (Canadell technique) | 1 | custom-made prosthesis | 2 |
| extra-articular scapulo-humeral resection (Tikhoff–Linberg) | 1 | growing prosthesis | 4 |
| biopsy/gain of diagnostic tissue | 12 | pedicle screws/rods/cages | 18 |
| removal of cement | 1 | other bone reconstruction | 11 |
| resection–replantation (upper extremity) | 1 | distraction osteogenesis | 1 |
| Internal hemipelvectomy | 38 | artificial bone substitute (Ca-sulfate, etc.) | 7 |
| Type I—ilium | 15 | cement spacer/pseudarthrosis/flail joint | 2 |
| Type II—Acetabular | 13 | arthrodesis | 4 |
| Type III—Pubic | 4 | vascularized epiphyseal transfer (based on tibial anterior artery) | 2 |
| Type IV—Sacral | 6 | Gore-Tex mesh, Trevira, etc. | 2 |
| Amputation | 39 | Soft Tissues | 159 |
| Forequarter | 5 | skin-/mesh-graft | 41 |
| External hemipelvectomy | 5 | pedicled tissue transfer | 96 |
| Upper extremity | 5 | rectus abdominis | 3 |
| Lower extremity | 24 | rectus abdominis (with skin) | 7 |
| Soft Tissues | 1800 | gastrocnemius | 10 |
| simple | 694 | latissimus dorsi | 12 |
| tendon resection | 23 | latissimus dorsi (with skin) | 3 |
| ligament resection | 5 | gracilis | 3 |
| resection of funiculus, scrotum, genitals | 3 | soleus | 3 |
| other STS resection | 11 | ALT | 8 |
| muscle resection | 419 | other muscle flap | 47 |
| vessel dissection | 225 | free tissue transfer | 22 |
| nerve dissection | 270 | latissimus dorsi | 8 |
| periosteum resection | 41 | gracilis | 2 |
| bone resection | 20 | ALT | 8 |
| vessel resection | 38 | other perforator flap | 3 |
| nerve resection | 50 | other free tissue transfer | 1 |
| MR-HIFU | 1 | Chest wall | 11 |
| Chest/Thoracic | 11 | Abdomen | 14 |
| chest wall resection | 7 | abdominal wall | 4 |
| other chest/lung resection | 2 | colon anastomosis | 3 |
| wedge resection | 2 | bladder | 2 |
| Abdomen | 19 | ureter | 2 |
| abdominal wall resection | 1 | other intraabdominal reconstruction | 5 |
| kidney | 2 | Sequelae of First Treatment | 29 |
| suprarenal glands | 1 | cement spaces implantation | 4 |
| ureter | 3 | partial implantation/replacement | 22 |
| bladder | 3 | complete compartment implantation/replacement | 3 |
| colon/rectum | 4 | Neurovascular | 70 |
| bowel | 2 | vascular | 56 |
| uterus/ovaries | 1 | artery complete | 14 |
| other abdominal resection | 2 | vein complete | 13 |
| Sequelae of 1st treatment | 106 | lympho-venous | 21 |
| debridement | 27 | other vessel reconstruction | 8 |
| inlay change | 5 | neural | 14 |
| partial removal of prosthesis | 26 | nerve reconstruction | 8 |
| complete removal of prosthesis | 3 | neurotization/local transfer | 2 |
| infection | 7 | autologous | 4 |
| wound healing breakdown | 11 | Tendon/Ligament | 38 |
| osteosynthesis breakdown | 2 | autologous tendon transfer | 18 |
| fracture | 1 | allograft tendon reconstruction | 2 |
| other | 24 | local tendon reconstruction | 18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theus-Steinmann, C.; Schelling, G.; Heesen, P.; Breitenstein, S.; Scaglioni, M.F.; Fuchs, B. How Is the Spectrum of Sarcoma Surgery Assessed? Cancers 2023, 15, 1305. https://doi.org/10.3390/cancers15041305
Theus-Steinmann C, Schelling G, Heesen P, Breitenstein S, Scaglioni MF, Fuchs B. How Is the Spectrum of Sarcoma Surgery Assessed? Cancers. 2023; 15(4):1305. https://doi.org/10.3390/cancers15041305
Chicago/Turabian StyleTheus-Steinmann, Carlo, Georg Schelling, Philip Heesen, Stefan Breitenstein, Mario F. Scaglioni, and Bruno Fuchs. 2023. "How Is the Spectrum of Sarcoma Surgery Assessed?" Cancers 15, no. 4: 1305. https://doi.org/10.3390/cancers15041305
APA StyleTheus-Steinmann, C., Schelling, G., Heesen, P., Breitenstein, S., Scaglioni, M. F., & Fuchs, B. (2023). How Is the Spectrum of Sarcoma Surgery Assessed? Cancers, 15(4), 1305. https://doi.org/10.3390/cancers15041305