
Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators

 , ,
, ,  , ,
, ,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
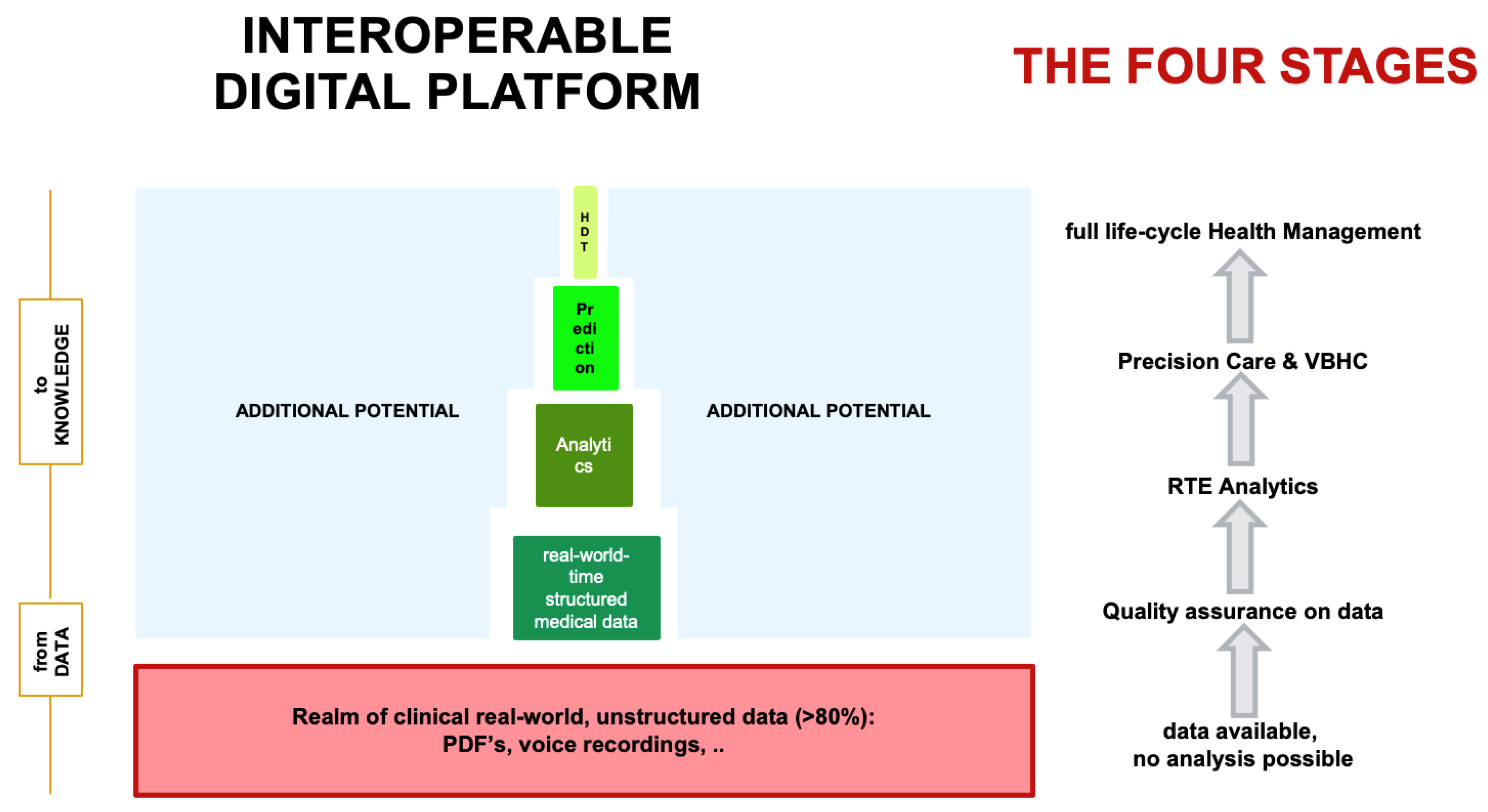
2.1. Description of the Interoperable Digital Platform
2.2. QI and Tools
2.3. Objectives
3. Results
3.1. Definition of Quality Indicators of Sarcoma Care
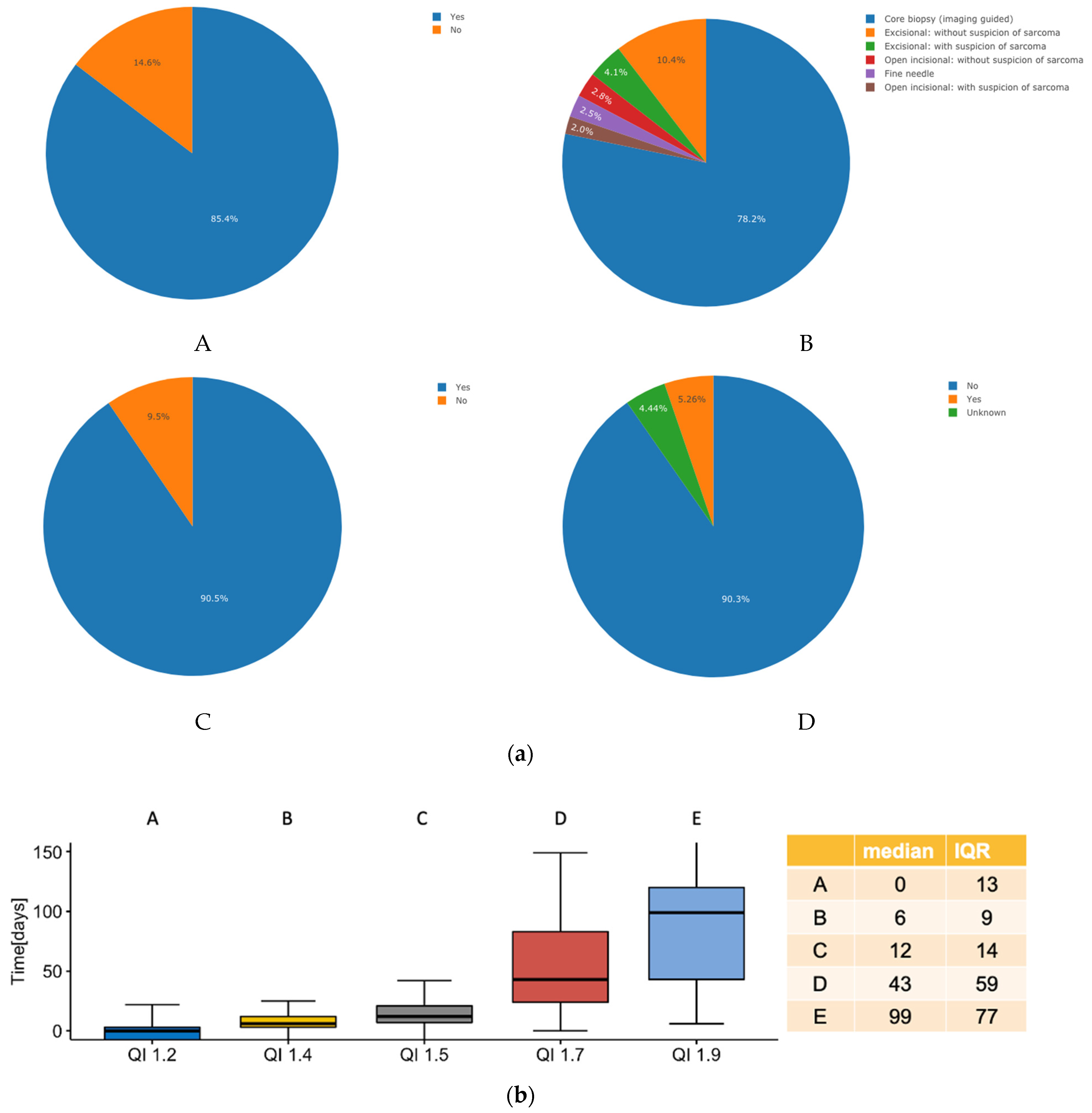
3.2. Quality Indicators of Sarcoma Work-Up
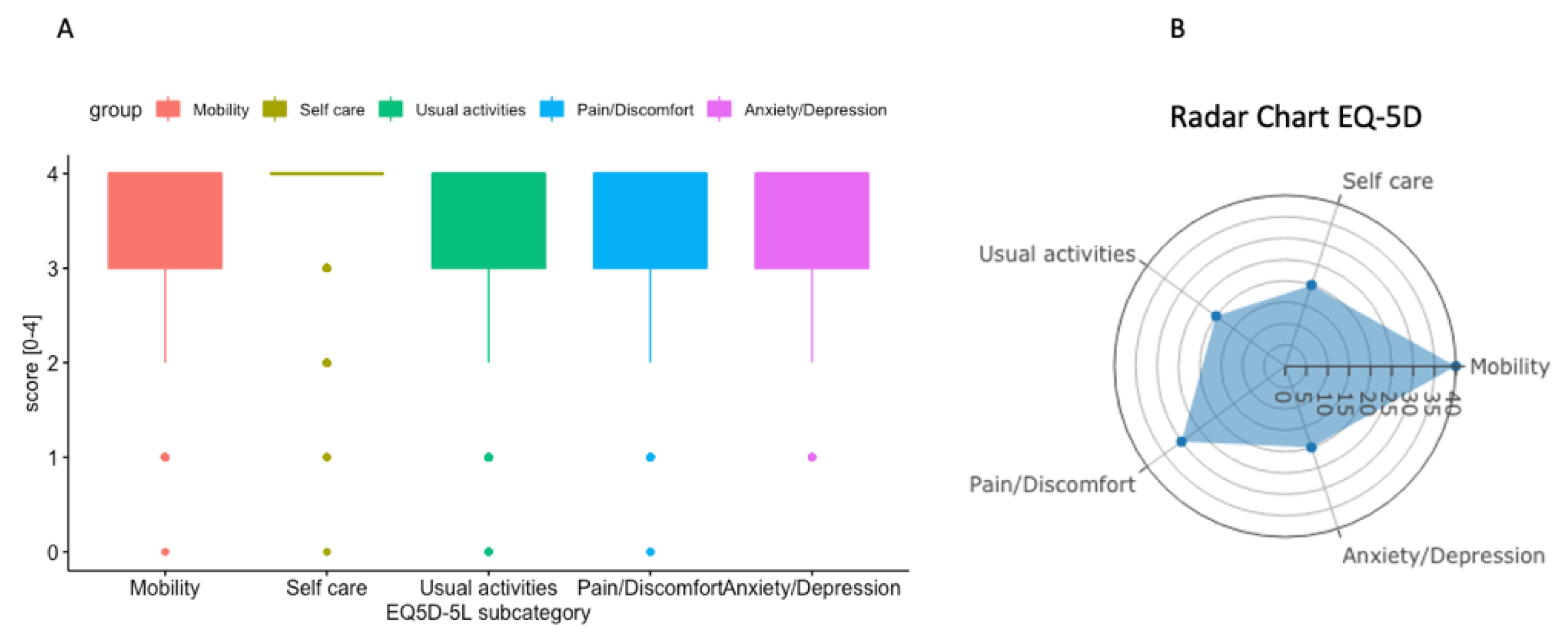
3.3. HRQOL-EQ-5D
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blank, A.T.; Larson, B.M.; Shaw, S.; Wakefield, C.J.; King, T.; Jones, K.B.; Randall, R.L. National Comprehensive Cancer Network guidelines compliance of a sarcoma service: A retrospective review. World J. Clin. Oncol. 2020, 11, 389–396. [Google Scholar] [CrossRef]
- Bagaria, S.P.; Ashman, J.B.; Daugherty, L.C.; Gray, R.J.; Wasif, N. Compliance with National Comprehensive Cancer Network guidelines in the use of radiation therapy for extremity and superficial trunk soft tissue sarcoma in the United States. J. Surg. Oncol. 2014, 109, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, P.H.; Schaapveld, M.; Otter, R.; Hoekstra, H.J. Soft tissue sarcoma—compliance with guidelines. Cancer 2001, 91, 2186–2195. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Hillner, B.E. Ensuring quality cancer care by the use of clinical practice guidelines and critical pathways. J. Clin. Oncol. 2001, 19, 2886–2897. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Thiesse, P.; Ranchere-Vince, D.; Chauvin, F.; Bobin, J.Y.; Sunyach, M.P.; Carret, J.P.; Mongodin, B.; Marec-Berard, P.; Philip, T.; et al. Conformity to clinical practice guidelines, multidisciplinary management and outcome of treatment for soft tissue sarcomas. Ann. Oncol. 2004, 15, 307–315. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Penel, N.; Gouin, F.; Le Cesne, A.; Toulmonde, M. Improving at a nationwide level the management of patients with sarcomas with an expert network. Ann. Oncol. 2022, 33, 659–661. [Google Scholar] [CrossRef]
- Fayet, Y.; Tetreau, R.; Honore, C.; Le Nail, L.R.; Dalban, C.; Gouin, F.; Causeret, S.; Piperno-Neumann, S.; Mathoulin-Pelissier, S.; Karanian, M.; et al. Determinants of the access to remote specialised services provided by national sarcoma reference centres. BMC Cancer 2021, 21, 631. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Casali, P.; Bouvier, C.; Dehais, C.; Galloway, I.; Gietema, J.; Halámková, J.; Hindi, N.; Idbaih, A.; Kinloch, E.; et al. European Reference Network for rare adult solid cancers, statement and integration to health care systems of member states: A position paper of the ERN EURACAN. ESMO Open Cancer Horiz. 2021, 6, 100174. [Google Scholar] [CrossRef]
- Blay, J.Y.; Soibinet, P.; Penel, N.; Bompas, E.; Duffaud, F.; Stoeckle, E.; Mir, O.; Adam, J.; Chevreau, C.; Bonvalot, S.; et al. Improved survival using specialized multidisciplinary board in sarcoma patients. Ann. Oncol. 2017, 28, 2852–2859. [Google Scholar] [CrossRef]
- Porter, M.E.; Lee, T.H.; Murray, A.C.A. The Value-Based Geography Model of Care. NEJM Catal. 2020, 1. [Google Scholar] [CrossRef]
- Blay, J.Y.; Honore, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in reference centers improves survival of sarcoma patients: A nationwide study. Ann. Oncol. 2019, 30, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.Y.; Bonvalot, S.; Gouin, F.; Le Cesne, A.; Penel, N. Criteria for reference centers for sarcomas: Volume but also long-term multidisciplinary organisation. Ann. Oncol. 2019, 30, 2008–2009. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, P.H.; Lausten, G.S.; Pedersen, A.B. The Danish Sarcoma Database. Clin. Epidemiol. 2016, 8, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H. Integrated Practice Units: A Playbook for Health Care Leaders. NEJM Catal. 2021, 2. [Google Scholar] [CrossRef]
- Porter, M.E.; Teisberg, E.O. Redefining competition in health care. Harv. Bus. Rev. 2004, 82, 64–76+136. [Google Scholar]
- Porter, M.E. Value-based health care delivery. Ann. Surg. 2008, 248, 503–509. [Google Scholar] [CrossRef]
- Porter, M.E. A strategy for health care reform—toward a value-based system. N. Engl. J. Med. 2009, 361, 109–112. [Google Scholar] [CrossRef]
- Di Maio, M.; Basch, E.; Denis, F.; Fallowfield, L.J.; Ganz, P.A.; Howell, D.; Kowalski, C.; Perrone, F.; Stover, A.M.; Sundaresan, P.; et al. The role of patient-reported outcome measures in the continuum of cancer clinical care: ESMO Clinical Practice Guideline. Ann. Oncol. 2022, 33, 878–892. [Google Scholar] [CrossRef]
- Porter, M.E.; Larsson, S.; Lee, T.H. Standardizing Patient Outcomes Measurement. N. Engl. J. Med. 2016, 374, 504–506. [Google Scholar] [CrossRef]
- Lyu, H.G.; Haider, A.H.; Landman, A.B.; Raut, C.P. The opportunities and shortcomings of using big data and national databases for sarcoma research. Cancer 2019, 125, 2926–2934. [Google Scholar] [CrossRef]
- Boehm, K.M.; Khosravi, P.; Vanguri, R.; Gao, J.; Shah, S.P. Harnessing multimodal data integration to advance precision oncology. Nat. Rev. Cancer 2022, 22, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, B.; Heesen, P. Real-time interaktive Analyse der Behandlungs-Qualität von Sarkom-Patienten. info@onco-suisse 2022, 1, 13–30. [Google Scholar]
- Concato, J.; Corrigan-Curay, J. Real-World Evidence—Where Are We Now? New Engl. J. Med. 2022, 386, 1680–1682. [Google Scholar] [CrossRef]
- Cheng, L.J.; Tan, R.L.; Luo, N. Measurement Properties of the EQ VAS Around the Globe: A Systematic Review and Meta-Regression Analysis. Value Health 2021, 24, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Reichardt, P.; Leahy, M.; Garcia Del Muro, X.; Ferrari, S.; Martin, J.; Gelderblom, H.; Wang, J.; Krishna, A.; Eriksson, J.; Staddon, A.; et al. Quality of Life and Utility in Patients with Metastatic Soft Tissue and Bone Sarcoma: The Sarcoma Treatment and Burden of Illness in North America and Europe (SABINE) Study. Sarcoma 2012, 2012, 740279. [Google Scholar] [CrossRef] [PubMed]
- Davidson, D.; Barr, R.D.; Riad, S.; Griffin, A.M.; Chung, P.W.; Catton, C.N.; O’Sullivan, B.; Ferguson, P.C.; Davis, A.M.; Wunder, J.S. Health-related quality of life following treatment for extremity soft tissue sarcoma. J. Surg. Oncol. 2016, 114, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H. From Volume to Value in Health Care: The Work Begins. JAMA 2016, 316, 1047–1048. [Google Scholar] [CrossRef]
- Kaplan, R.S.; Porter, M.E. How to solve the cost crisis in health care. Harv. Bus. Rev. 2011, 89, 46–52. [Google Scholar]
- Porter, M.E.; Pabo, E.A.; Lee, T.H. Redesigning primary care: A strategic vision to improve value by organizing around patients’ needs. Health Aff. 2013, 32, 516–525. [Google Scholar] [CrossRef]
- Simmons, D.R.; Robert Carey, A.T.; Carmouche, D.; Roccella, E.J. QualityImpact: A data-driven quality improvement model that imprves clinical care and reduces cost. NEJM Catal. 2021, 2. [Google Scholar] [CrossRef]
- Kann, B.H.; Hosny, A.; Aerts, H. Artificial intelligence for clinical oncology. Cancer Cell 2021, 39, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Callegaro, D.; Miceli, R.; Bonvalot, S.; Ferguson, P.; Strauss, D.C.; Levy, A.; Griffin, A.; Hayes, A.J.; Stacchiotti, S.; Pechoux, C.L.; et al. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: A retrospective analysis. Lancet Oncol. 2016, 17, 671–680. [Google Scholar] [CrossRef] [PubMed]
- van Praag, V.M.; Rueten-Budde, A.J.; Jeys, L.M.; Laitinen, M.K.; Pollock, R.; Aston, W.; van der Hage, J.A.; Dijkstra, P.D.S.; Ferguson, P.C.; Griffin, A.M.; et al. A prediction model for treatment decisions in high-grade extremity soft-tissue sarcomas: Personalised sarcoma care (PERSARC). Eur. J. Cancer 2017, 83, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Irmisch, A.; Bonilla, X.; Chevrier, S.; Lehmann, K.-V.; Singer, F.; Toussaint, N.C.; Esposito, C.; Mena, J.; Milani, E.S.; Casanova, R.; et al. The Tumor Profiler Study: Integrated, multi-omic, functional tumor profiling for clinical decision support. Cancer Cell 2021, 39, 288–293. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| QI FOR MULTIDISCIPLINARY TEAMS (MDT) |
|---|
| 1. Sarcoma work-up of patients |
| 2. MDT/SB management |
| 3. Therapy (incl. surgery, radiation-, chemotherapy) |
| 4. Complexity of sarcoma therapy |
| 5. Clinical metrics outcome (physician based) |
| 6. PROMS/PREMS (patient based) |
| QUALITY INDICATORS: SARCOMA WORK-UP |
|---|
| • was imaging performed before biopsy |
| • time from first patient contact to biopsy |
| • which type of biopsy was performed |
| • time from biopsy to MDT/SB presentation |
| • time from biopsy to SB presentation |
| • was biopsy performed before initiation of treatment? separated according to type of treatment |
| • was there metastasis at presentation |
| • time from MDT/SB presentation to initiation of treatment (incl. analysis depending on type of therapy |
| QUALITY INDICATORS: MDT/SB MANAGEMENT |
|---|
| • how many patients were presented per month/per year |
| • how many presentations took place per month/per year |
| • how many first presentations |
| • how many follow-up presentations |
| • how many bone lesions—superficial/deep soft tissue lesions were presented |
| • how many malignant—intermediate—benign lesions were discussed |
| • how many decisions on: - surgery - radiation therapy - combination radiation therapy–surgery - combination chemotherapy–surgery - combination surgery–radiation therapy–chemotherapy |
| • how many decisions were realized/executed? - Overall - surgery - radiation oncology - chemotherapy |
| • how many patients were presented over entire cycle of care |
| QUALITY INDICATORS: THERAPY |
|---|
| • % margin status (R0, R1, R2) at definitive surgery • surgical, pathological, consens |
| • % amputations |
| • % preoperative radiation therapy (yes/no) |
| • % postoperative radiation therapy (yes/no) |
| • % neoadjuvant chemotherapy (yes/no) |
| • % adjuvant chemotherapy (yes/no) |
| QUALITY INDICATORS: COMPLEXITY OF THERAPY | |
|---|---|
| • surgical complexity STS | Cancers March 2022 |
| • surgical complexity bone sarcoma | Age, grading/type of lesion, prior RT, chemo/whoops, size of lesion, location, resected structures, reconstructed structures, involved disciplines |
| • surgical complexity visceral sarcoma | Age, grading/type of lesion, prior RT, chemo/whoops, size of lesion, location, resected structures, reconstructed structures, involved disciplines |
| • radiation oncology complexity treatment | Aim of RT (curative, locally curative, palliative, definitive, unknown); RT technique (IMRT, VMAT, SRT, 3DCRT, 2DCRT, unknown; RT type (photons, protons, electrons, brachytherapy (transient, permanent), conventional, other, unknown); total dose/number of fractions; GTV/PTV; Grade III/IV toxicities; |
| • systemic treatment complexity | Aim of systemic therapy (curative intent pre/postop, additive, maintenance, palliative); number of curative/palliative cycles planned/executed; time to next treatment (TTT); reasons for discontinuation (completed, discontinued (toxicity, PD, planned, patient‘s wish, death); Grade III/IV toxicities |
| QUALITY INDICATORS: OUTCOME |
|---|
| • local recurrence within 1st year after tumor resection |
| • local recurrence overall |
| • systemic recurrence with 1st year of treatment initiation |
| • systemic recurrence overall |
| • latest follow-up: NED, AWD, DOD, DOR, no assessment possible; lost to followup, unknown) |
| • in case of RT: % vascular disorders (lymphedema, ROM, fibrosis); skin disorders (hyper-,hypopigmentation); bone disorders (osteonecrosis) |
| • in case of chemotherapy: % therapy during last 3 months of life. |
| SARCOMA QUALITY INDICATORS | PROMS/PREMS |
|---|---|
| • work-up/regular f-up | -WHO-ECOG -EQ-5D -EQ-VAS -work ability index |
| • biopsy | -biopsy |
| • surgery | -MSTS upper/lower extremity -TESS upper/lower extremity -visceral |
| • radiation oncology | -local effects of RT |
| • chemotherapy | -EORTC-QLQ-C30 -MDASI |
| • therapy focused | -cancer therapy satisfaction -satisfaction with RT -control preferences |
| • Physican related | -CARE |
| • Institution focused | -satisfaction with institution |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heesen, P.; Studer, G.; Bode, B.; Windegger, H.; Staeheli, B.; Aliu, P.; Martin-Broto, J.; Gronchi, A.; Blay, J.-Y.; Le Cesne, A.; et al. Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators. Cancers 2023, 15, 47. https://doi.org/10.3390/cancers15010047
Heesen P, Studer G, Bode B, Windegger H, Staeheli B, Aliu P, Martin-Broto J, Gronchi A, Blay J-Y, Le Cesne A, et al. Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators. Cancers. 2023; 15(1):47. https://doi.org/10.3390/cancers15010047
Chicago/Turabian StyleHeesen, Philip, Gabriela Studer, Beata Bode, Hubi Windegger, Benjamin Staeheli, Paul Aliu, Javier Martin-Broto, Alessandro Gronchi, Jean-Yves Blay, Axel Le Cesne, and et al. 2023. "Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators" Cancers 15, no. 1: 47. https://doi.org/10.3390/cancers15010047
APA StyleHeesen, P., Studer, G., Bode, B., Windegger, H., Staeheli, B., Aliu, P., Martin-Broto, J., Gronchi, A., Blay, J.-Y., Le Cesne, A., & Fuchs, B. (2023). Quality of Sarcoma Care: Longitudinal Real-Time Assessment and Evidence Analytics of Quality Indicators. Cancers, 15(1), 47. https://doi.org/10.3390/cancers15010047