
Safety, Feasibility and Efficacy of Lokomat® and Armeo®Spring Training in Deconditioned Paediatric, Adolescent and Young Adult Cancer Patients
 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Outcomes
2.4. Safety
2.5. Feasibility
2.6. Preliminary Efficacy
- Cardiopulmonary fitness was assessed using cardiopulmonary fitness tests on a cycle-ergometer and conducted according to standardised procedures (American Thoracic Society/American College of Chest Physicians) [33].
- Walking endurance was assessed using the six-minute walk test [34].
- Gait efficiency was assessed using the ten-metre walk test (comfortable pace and fast pace) [35].
- Trunk flexibility was measured using a sit and reach box (Flex-Tester Sit and Reach Flexibility Test Box, Novel Products Inc., Rockton, IL, USA) [38].
- Unilateral gross manual dexterity was assessed using the box and block test [39].
- Shoulder flexibility was assessed using the back scratch test [39].
- Maximal grip strength was assessed using a hydraulic hand grip dynamometer (Saehan, SH5001, Masan, Republic of Korea) [40].
- Muscular endurance was assessed using the 30-s arm curl test (5lb and 8lb) [41].
- In addition, all participants completed the following self-reported questionnaires at baseline and 6 weeks:
- Quality of life was assessed using the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) [42].
- Fatigue was assessed by the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) [43].
- Leisure time physical activity was assessed using the Godin-Shephard Leisure Time Physical Activity Questionnaire (GSLTPAQ) [44].
- Activities of daily living were assessed using the Canadian Occupational Performance Measure (COPM) [45].
2.7. Sample Size
2.8. Statistical Analysis
3. Results
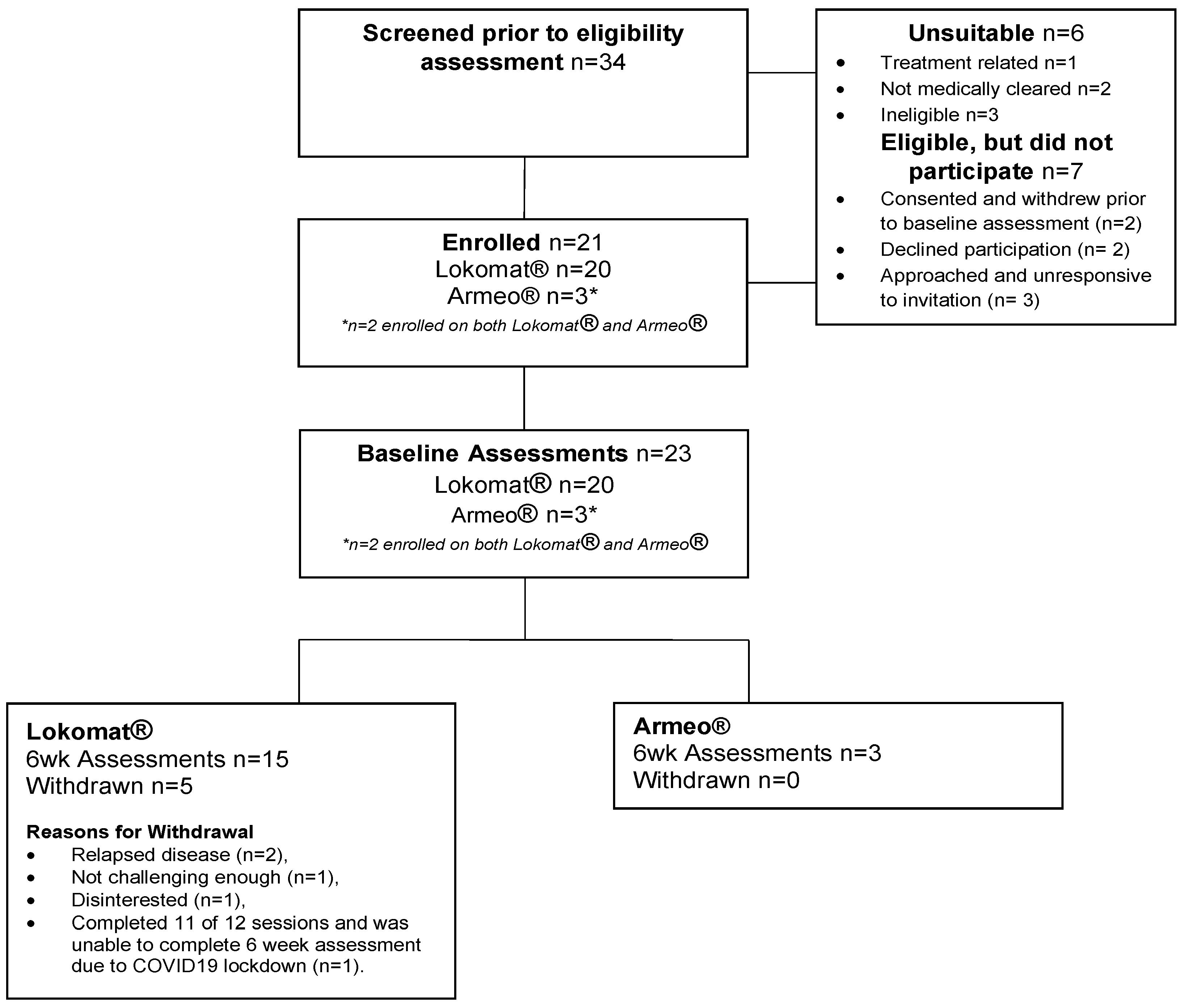
3.1. Recruitment and Retention
3.2. Participant Characteristics
3.3. Safety
3.4. Feasibility
3.4.1. Demand
3.4.2. Adherence
3.4.3. Frequency of Needing to Interrupt or Cease Sessions
3.4.4. Patient-Reported Outcomes
3.4.5. Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atkinson, M.; Murnane, A.; Goddard, T.; Pendergrast, C.; Rogers, P.; Manudhane, R.; Osborn, M. A randomized controlled trial of a structured exercise intervention after the completion of acute cancer treatment in adolescents and young adults. Pediatr. Blood Cancer 2020, 68, e28751. [Google Scholar] [CrossRef] [PubMed]
- Ness, K.K.; Plana, J.C.; Joshi, V.M.; Luepker, R.V.; Durand, J.B.; Green, D.M.; Partin, R.E.; Santucci, A.K.; Howell, R.M.; Srivastava, D.K.; et al. Exercise intolerance, mortality, and organ system impairment in adult survivors of childhood cancer. J. Clin. Oncol. 2020, 38, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.M.; Repka, C.P.; Lalonde, T.L.; Dallow, K.T.; Barlow, C.E.; Hayward, R. Demonstration of the need for cardiovascular and pulmonary normative data for cancer survivors. Int. J. Sport. Med. 2014, 35, 1134–1137. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.L.; Lucia, A.; et al. American College of Sports Medicine round table on exercise guidelines for cancer patients. Med. Sci. Sport. Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Koelwyn, G.J.; Khouri, M.; Mackey, J.R.; Douglas, P.S.; Jones, L.W. Running on empty: Cardiovascular reserve capacity and late effects of the therapy in cancer survivorship. J. Clin. Oncol. 2012, 30, 4458–4461. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.; Xu, L.; Bhatia, S.; Cooper, R.; Brar, S.; Wong, F.L.; Armenian, S.H. Cardiovascular disease risk profiles in survivors of adolescent and young adult (AYA) cancer: The Kaiser Permanente AYA cancer survivors study. J. Clin. Oncol. 2016, 34, 1626–1633. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Zopf, E.M.; Zhang, X.; Schmitz, K.H. The impact of exercise on cancer mortality, recurrence and treatment-related adverse effects. Epidemiol. Rev. 2017, 39, 71–92. [Google Scholar] [CrossRef]
- Jones, L.W.; Eves, N.D.; Haykowsky, M.; Freedland, S.J.; Mackey, J.R. Exercise intolerance in cancer and the role of exercise therapy to reverse dysfunction. Lancet Oncol. 2009, 10, 598–605. [Google Scholar] [CrossRef]
- Lakoski, S.G.; Eves, N.D.; Douglas, P.S.; Jones, L.W. Exercise rehabilitation in patients with cancer. Nat. Rev. Clin. Oncol. 2013, 9, 288–296. [Google Scholar] [CrossRef]
- Jones, L.W.; Liang, Y.; Pituskin, E.N.; Battaglini, C.L.; Scott, J.M.; Hornsby, W.E.; Haykowsky, M. Effect of Exercise Training on Peak Oxygen Consumption in Patients with Cancer: A Meta-Analysis. Oncologist 2011, 16, 112–120. [Google Scholar] [CrossRef]
- Christensen, J.F.; Jones, L.W.; Andersen, J.L.; Daugaard, G.; Rorth, M.; Hojman, P. Muscle dysfunction in cancer patients. Ann. Oncol. 2014, 25, 947–958. [Google Scholar] [CrossRef]
- Wurz, A.; Brunet, J. The effects of physical activity on health and QOL in adolescent cancer survivors: A systematic review. JMIR Cancer 2016, 24, e5431. [Google Scholar] [CrossRef]
- Fong, D.Y.T.; Ho, J.W.C.; Hui, B.P.H.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.K.; Cerin, E.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Physical activity for cancer survivors: Meta-analysis of randomized controlled trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef]
- Shi, Q.; Zheng, J.; Liu, K. Supervised Exercise Interventions in Childhood Cancer Survivors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Children 2022, 9, 824. [Google Scholar] [CrossRef]
- Morales, J.S.; Valenzuela, P.L.; Velázquez-Díaz, D.; Castillo-García, A.; Jiménez-Pavón, D.; Lucia, A.; Fiuza-Luces, C. Exercise and Childhood Cancer—A Historical Review. Cancers 2021, 14, 82. [Google Scholar] [CrossRef]
- Murnane, A.; Gough, K.; Thompson, K.; Holland, L.; Conyers, R. Adolescents and young adult cancer survivors: Exercise habits, QOL and physical activity preferences. Support Care Cancer 2015, 23, 501–510. [Google Scholar] [CrossRef]
- Gonzalez, A.; Garcia, L.; Kilby, J.; McNair, P. Robotic devices for paediatric rehabilitation: A review of design features. Biomed. Eng. Online 2021, 20, 89. [Google Scholar] [CrossRef]
- Baronchelli, F.; Zucchella, C.; Serrao, M.; Intiso, D.; Bartolo, M. The Effect of Robotic Assisted Gait Training with Lokomat® on Balance Control After Stroke: Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 661815. [Google Scholar] [CrossRef]
- Olczak, A.; Truszczyńska-Baszak, A.; Stępień, A. The Use of Armeo®Spring Device to Assess the Effect of Trunk Stabilization Exercises on the Functional Capabilities of the Upper Limb—An Observational Study of Patients after Stroke. Sensors 2022, 22, 4336. [Google Scholar] [CrossRef]
- Mirelman, A.; Patritti, B.L.; Bonato, P.; Deutsch, J.E. Effects of robot-virtual reality compared with robot alone training on gait kinetics of individuals post stroke. In Proceedings of the 2007 Virtual Rehabilitation, Venice, Italy, 27–29 September 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 65–69. [Google Scholar]
- Aurich-Schuler, T.; Grob, F.; van Hedel, H.J.A.; Labruyere, R. Can Lokomat therapy with children and adolescents be improved? An adaptive clinical pilot trial comparing Guidance force, Path control, and FreeD. J. Neuroeng. Rehabil. 2017, 14, 76. [Google Scholar] [CrossRef]
- Colomer, C.; Baldoví, A.; Torromé, S.; Navarro, M.D.; Moliner, B.; Ferri, J.; Noé, E. Efficacy of Armeo®Spring during the chronic phase of stroke. Study in mild to moderate cases of hemiparesis. Neurología 2013, 28, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Lefmann, S.; Russo, R.; Hillier, S. The effectiveness of robotic-assisted gait training for paediatric gait disorders: Systematic review. J. Neuroeng. Rehabil. 2017, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Conner, B.C.; Remec, N.M.; Lerner, Z.F. Is robotic gait training effective for individuals with cerebral palsy? A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2022, 36, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; Colombo, V.; et al. What does evidence tell us about the use of gait robotic devices in patients with multiple sclerosis? A comprehensive systematic review on functional outcomes and clinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 841–849. [Google Scholar] [CrossRef]
- Bessler, J.; Prange-Lasonder, G.B.; Schulte, R.V.; Schaake, L.; Prinsen, E.C.; Buurke, J.H. Occurrence and Type of Adverse Events During the Use of Stationary Gait Robots—A Systematic Literature Review. Front. Robot. AI 2020, 7, 557606. [Google Scholar] [CrossRef]
- van Dellen, F.; Labruyère, R. Settings matter: A scoping review on parameters in robot-assisted gait therapy identifies the importance of reporting standards. J. Neuroeng. Rehabil. 2022, 19, 40. [Google Scholar] [CrossRef]
- Ness, K.K.; Hudson, M.M.; Ginsberg, J.P.; Nagarajan, R.; Kaste, S.C.; Marina, N.; Whitton, J.; Robison, L.L.; Gurney, J.G. Physical Performance Limitations in the Childhood Cancer Survivor Study Cohort. J. Clin. Oncol. 2009, 27, 2382–2389. [Google Scholar] [CrossRef]
- Thabane, L.; Hopewell, S.; Lancaster, G.; Bond, C.M.; Coleman, C.L.; Campbell, M.J.; Eldridge, S. Methods and processes for development of a CONSORT extension for reporting pilot randomized controlled trials. Pilot Feasibility Stud. 2016, 2, 25. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef]
- National Cancer Institute. Cancer Therapy Evaluation Program. Common Terminology Criteria for Adverse Events. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 24 August 2022).
- Weisman, I.M. ATS/ACCP statement on the cardiopulmonary exercise testing. Am. J. Respir. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; Macintyre, N.R.; Mckay, R.T.; Johnson, D.; Wanger, J.S.; Zeballos, J.; Bittner, V. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respire Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Karpman, C.; LeBrasseur, N.; DePew, Z.S.; Novotny, P.J.; Benzo, R.P. Measuring Gait Speed in the Out-Patient Clinic: Methodology and Feasibility. Respir. Care 2013, 59, 531–537. [Google Scholar] [CrossRef]
- Marlow, N.; Hastings, K.; Hansson, J. Exercise and Sports Science Australia’s Outcome Measures for Exercise Physiologists: Ensuring Evidence-Based Practice; Exercise and Sports Science Australia: Brisbane, Australia, 2014. [Google Scholar]
- Coldwells, A.; Atkinson, G.; Reilly, T. Sources of variation in back and leg dynamometry. Ergonomics 1994, 37, 79–86. [Google Scholar] [CrossRef]
- Reese, N.B.; Brandy, W.D. Joint Range of Motion and Muscle Length Testing, 2nd ed.; Saunders Elsevier: Philadelphia, PA, USA, 2010; pp. 47–79. [Google Scholar]
- Kontson, K.; Marcus, I.; Myklebust, B.; Civillico, E. Targeted box and blocks test: Normative data and comparison to standard tests. PLoS ONE 2017, 12, e0177965. [Google Scholar] [CrossRef]
- Wind, A.E.; Takken, T.; Helders, P.J.; Engelbert, R.H.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediatr. 2010, 169, 281–287. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2001. [Google Scholar]
- Giesinger, J.M.; Kuijpers, W.; Young, T.; Tomaszewski, K.A.; Friend, E.; Zabernigg, A.; Holzner, B.; Aaronson, N.K. Health and Quality of Life Outcomes: Thresholds for clinical importance for four key domains of the EORTC QLQ-C30: Physical functioning, emotional functioning, fatigue and pain. Health Qual. Life Outcomes 2016, 14, 2–8. [Google Scholar] [CrossRef]
- Storic, L.; Linder, J.; Kane, L.; Foster, C.; Gugliotti, M. Does exercise provide a positive therapeutic effect for patients with cancer related fatigue? A systematic review. Rehabil. Oncol. 2013, 31, 14–22. [Google Scholar] [CrossRef]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. The use of the Godin-Shephard leisure-time physical activity questionnaire in oncology research: A systematic review. BMC Med. Res. Methodol. 2015, 15, 60. [Google Scholar] [CrossRef]
- Ohno, K.; Tomori, K.; Sawada, T.; Seike, Y.; Yaguchi, A.; Kobayashi, R. Measurement Properties of the Canadian Occupational Performance Measure: A Systematic Review. Am. J. Occup. Ther. 2021, 75, 7506205100. [Google Scholar] [CrossRef]
- Tomczak, M.; Tomczak, E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trends Sport. Sci. 2014, 1, 19–25. [Google Scholar]
- Munsie, C.; Ebert, J.; Joske, D.; Ackland, T. The benefit of physical activity in adolescentand young adult cancer patients during and after treatment:a systematic review. J. Adolesc. Young-Adult Oncol. 2019, 8, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Braam, K.I.; van der Torre, P.; Takken, T.; Veening, M.A.; van Dulmen-den Broeder, E.; Kaspers, G.J.L. Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst. Rev. 2016, 3, CD008796. [Google Scholar] [CrossRef] [PubMed]
- Carty, C.P.; Dickinson, I.C.; Watts, M.C.; Crawford, R.W.; Steadman, P. Impairment and disability following limb salvage procedures for bone sarcoma. Knee 2009, 16, 405–408. [Google Scholar] [CrossRef]
- Hobbie, W.L.; Ogle, S.; Reilly, M.; Barakat, L.; Lucas, M.S.; Ginsberg, J.P.; Fisher, M.J.; Volpe, E.M.; Deatrick, J.A. Adolescent and young adult survivors of childhood brain tumors: Life after treatment in their own words. Cancer Nurs. 2016, 39, 134–143. [Google Scholar] [CrossRef]
- Yeha, S.W.; Linc, L.W.; Tamg, K.W.; Tsaik, C.P.; Hong, C.H.; Kuan, Y.C. Efficacy of robot-assisted gait training in multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 41, 102034. [Google Scholar] [CrossRef]
- Jones, L.W.; Dolinsky, V.; Haykowsky, M.; Patterson, I.; Allen, J.; Scott, J.M.; Rogan, K.; Khouri, M.; Hornsby, W.; Young, M.; et al. Effects of aerobic training to improve cardiovascular function and prevent cardiac remodeling after cytotoxic therapy in early breast cancer [abstract]. In Proceedings of the American Association for Cancer Research 102nd Annual Meeting, Orlando, FL, USA, 2–6 April 2011; p. a5024. [Google Scholar]


{kind=link}
| Baseline Characteristics of Participants (n = 21) | |||
|---|---|---|---|
| Variable | No. | % | |
| Age mean ± Standard Deviation (SD), year (y) | 16 ± 5 | ||
| Female% | 12 | 57 | |
| Weight, mean ± SD, kg | 54 ± 22 | ||
| Body Mass Index (BMI), mean ± SD, kg/m2 | 21 ± 8 | ||
| Diagnosis | |||
| Sarcoma | 19 | ||
| Ewing Sarcoma | 3 | ||
| Osteosarcoma | 1 | ||
| Leukaemia | 14 | ||
| * Therapy-related Acute Myeloid Leukaemia | 1 | ||
| Pre-B Acute Lymphoblastic Leukaemia | 2 | ||
| Lymphoma | 19 | ||
| Classical Hodgkin Lymphoma | 3 | ||
| * Burkitts Lymphoma | 1 | ||
| Germ Cell | |||
| Central Nervous System Germ Cell Tumour | 1 | 4 | |
| Other | |||
| Medulloblastoma | 5 | 23 | |
| Pilocytic Astrocytoma | 3 | 14 | |
| Sacral meningioma-papillary variant, G3 | 1 | 4 | |
| Myxopapillary Ependymoma | 1 | 4 | |
| Treatment Intensity | |||
| Level 1 Least Intensive | 1 | 5 | |
| Level 2 Moderately Intensive | 3 | 14 | |
| Level 3 Very Intensive | 14 | 67 | |
| Level 4 Most Intensive | 3 | 14 | |
| Causality | ||||
|---|---|---|---|---|
| Unlikely to be Related | Possibly/Probably Related | Certainly Related | ||
| Grade | 1—mild, intervention not indicated | 16 | 27 | 2 |
| 2—moderate, minimal intervention | 0 | 1 | 2 | |
| 3—severe or medically significant | 1 | 0 | 0 | |
| 4—life threatening consequences | 0 | 0 | 0 | |
| 5—death related to adverse event | 0 | 0 | 0 | |
| Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | |
|---|---|---|---|---|---|
| Sessions were fun | 8 | 7 | 1 | 0 | 0 |
| I was comfortable | 8 | 6 | 2 | 0 | 0 |
| I liked coming | 8 | 5 | 3 | 0 | 0 |
| I saw improvement | 11 | 4 | 1 | 0 | 0 |
| Continue if available | 6 | 6 | 4 | 0 | 0 |
| Freq appropriate | 6 | 9 | 1 | 0 | 0 |
| Duration appropriate | 6 | 10 | 0 | 0 | 0 |
| Lokomat | |||||
|---|---|---|---|---|---|
| Outcome Measure | Baseline All Participants Mean SD n | Baseline Completers Mean SD n | 6 Weeks Mean SD n | Effect Size | p Value |
| VO2Peak (mL·kg−1·min−1) | 22.63 (9.1) n = 10 | 21.8 (6.0) n = 7 | 23.3 (6.8) n = 7 | 0.63 | 0.018 |
| 10 MWT Comfortable (s) | 9.7 (1.7) n = 19 | 9.9 (1.6) n = 14 | 7.7 (2.0) n = 14 | 0.51 | 0.004 |
| 10 MWT Maximal (s) | 7.0 (1.7) n = 19 | 7.5 (1.3) n = 14 | 5.3 (3.4) n = 14 | 0.60 | 0.001 |
| 6 MWT(m) | 416.0 (174.3) n = 19 | 419.1 (145.0) n = 14 | 487.29 (158.9) n = 14 | 0.60 | 0.002 |
| Max Back and Leg Strength | 44.4 (46.2) n = 8 | 28.0 (16.7) n = 5 | 40.8 (16.0) n = 5 | 0.71 | 0.043 |
| Trunk Flexibility | 12.25 (10.9) n = 20 | 15.1 (6.6) n = 10 | 19.2 (3.6) n = 10 | 0.60 | 0.059 |
| EORTC QLQC30 * | 63.8 (15.1) n = 20 | 63.3 (13.3) n = 15 | 73.3 (19.7) n = 15 | 0.61 | 0.018 |
| FACIT fatigue ** | 32.8 (10.4) n = 20 | 31.6 (9.5) n = 13 | 37.5 (10.6) n = 15 | 0.53 | 0.039 |
| GLTPAQ–LSI *** | 27.8 (31.0) n = 20 | 25.3 (22.4) n = 15 | 36.0 (30.6) n = 15 | 0.30 | 0.249 |
| COPM Performance **** | 3.9 (1.1) n = 19 | 3.7 (1.0) n = 15 | 6.3 (1.9) n = 15 | 0.83 | 0.001 |
| COPM Satisfaction | 3.3 (1.4) n = 19 | 3.3 (0.9) n = 15 | 6.6 (1.7) n = 15 | 0.88 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atkinson, M.; Tully, A.; Maher, C.A.; Innes-Wong, C.; Russo, R.N.; Osborn, M.P. Safety, Feasibility and Efficacy of Lokomat® and Armeo®Spring Training in Deconditioned Paediatric, Adolescent and Young Adult Cancer Patients. Cancers 2023, 15, 1250. https://doi.org/10.3390/cancers15041250
Atkinson M, Tully A, Maher CA, Innes-Wong C, Russo RN, Osborn MP. Safety, Feasibility and Efficacy of Lokomat® and Armeo®Spring Training in Deconditioned Paediatric, Adolescent and Young Adult Cancer Patients. Cancers. 2023; 15(4):1250. https://doi.org/10.3390/cancers15041250
Chicago/Turabian StyleAtkinson, Morgan, Angela Tully, Carol A. Maher, Christopher Innes-Wong, Ray N. Russo, and Michael P. Osborn. 2023. "Safety, Feasibility and Efficacy of Lokomat® and Armeo®Spring Training in Deconditioned Paediatric, Adolescent and Young Adult Cancer Patients" Cancers 15, no. 4: 1250. https://doi.org/10.3390/cancers15041250
APA StyleAtkinson, M., Tully, A., Maher, C. A., Innes-Wong, C., Russo, R. N., & Osborn, M. P. (2023). Safety, Feasibility and Efficacy of Lokomat® and Armeo®Spring Training in Deconditioned Paediatric, Adolescent and Young Adult Cancer Patients. Cancers, 15(4), 1250. https://doi.org/10.3390/cancers15041250