



Toxicity of Asciminib in Real Clinical Practice: Analysis of Side Effects and Cross-Toxicity with Tyrosine Kinase Inhibitors

 , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
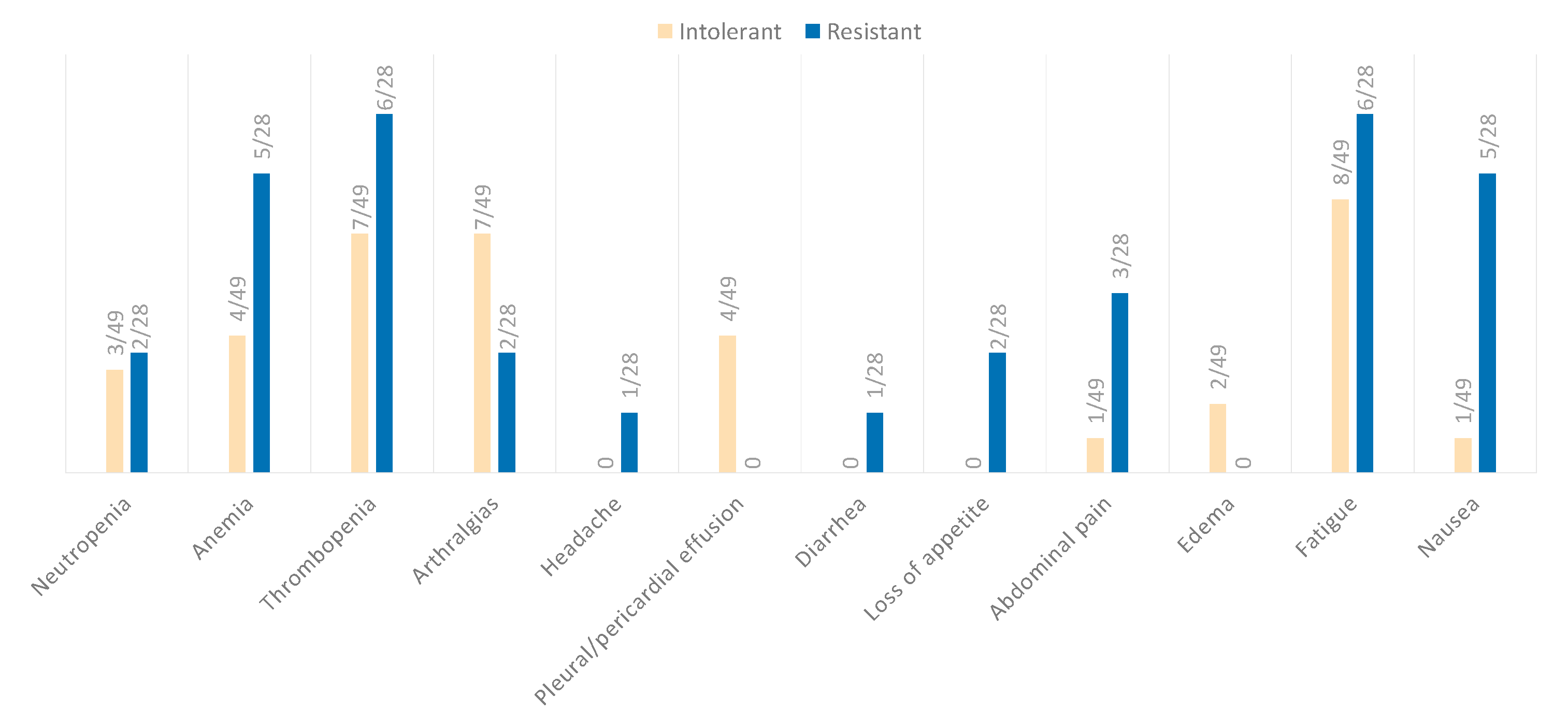
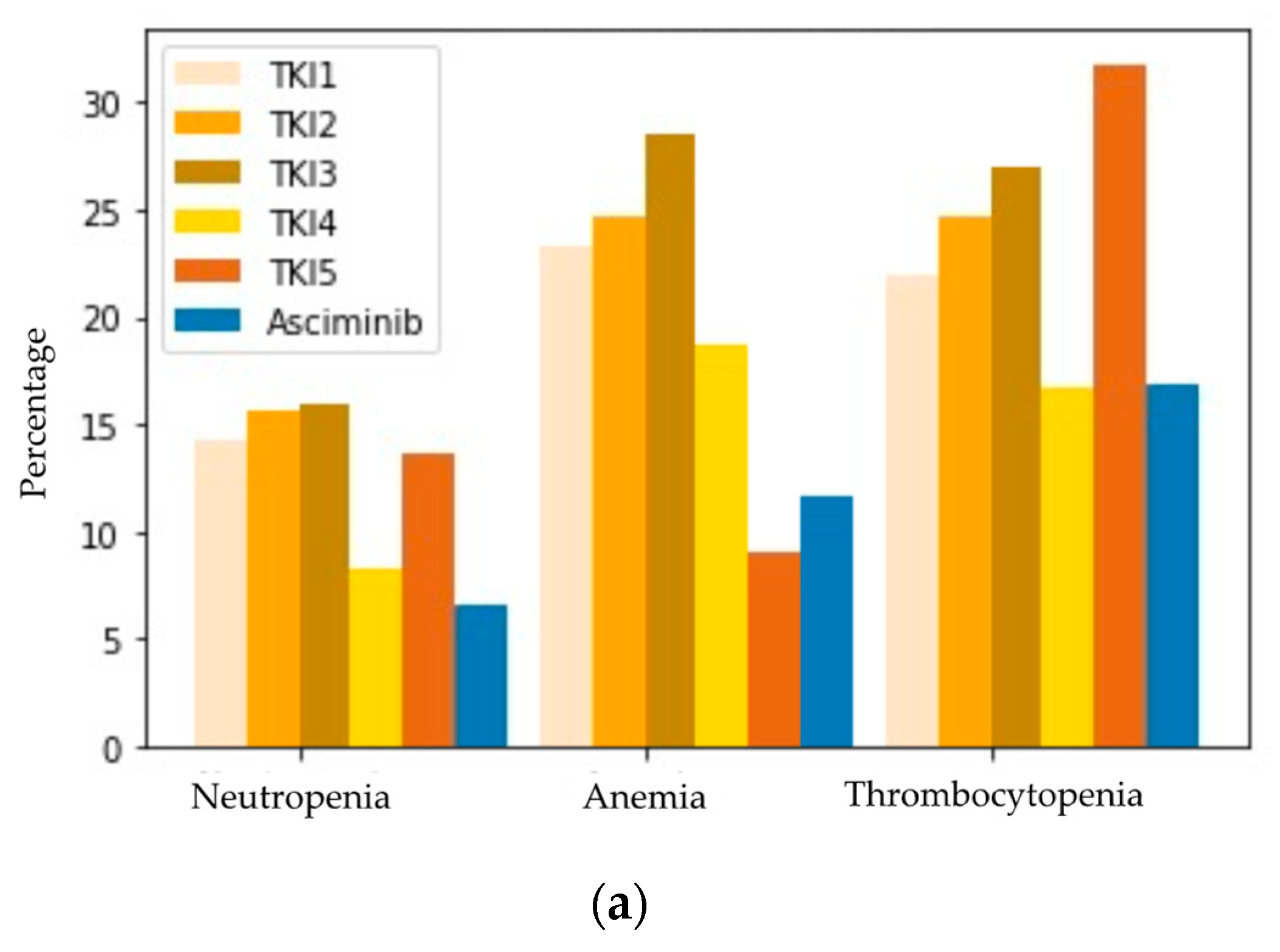
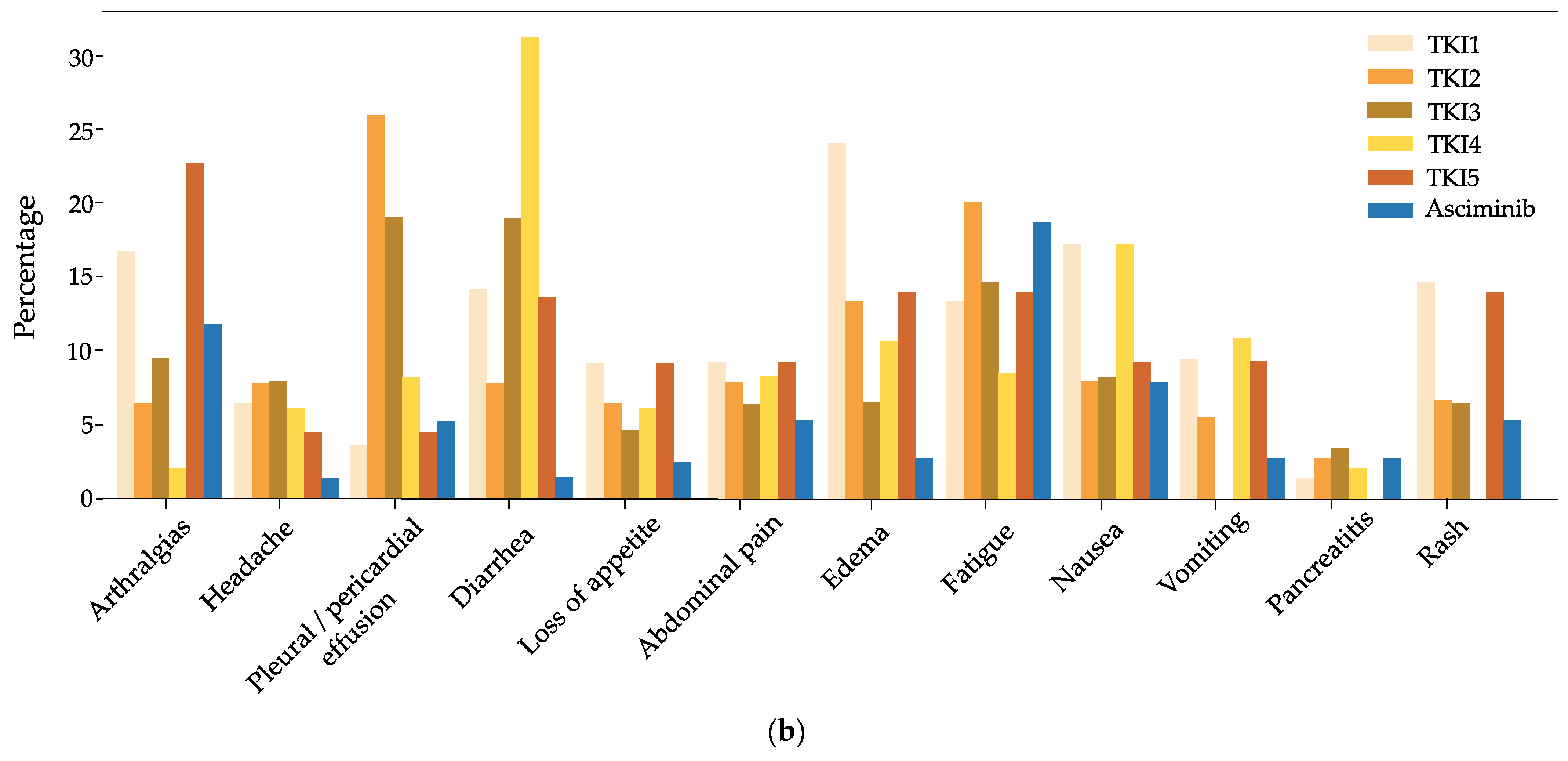
3.1. Safety
3.2. Cross-Toxicity and Cross Intolerance
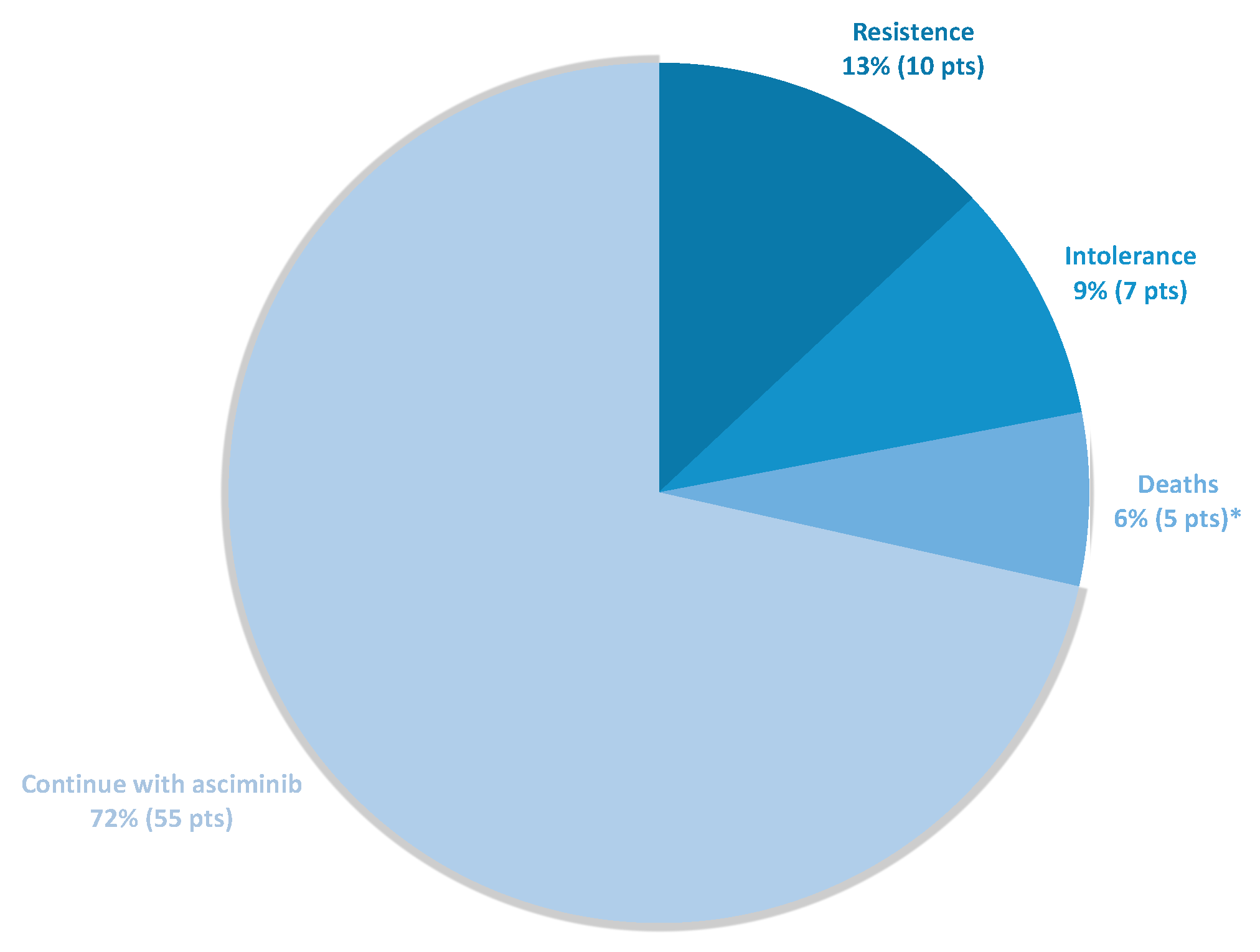
3.3. Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Madhusudan, S.; Ganesan, T.S. Tyrosine kinase inhibitors in cancer therapy. Clin. Biochem. 2004, 37, 618–635. [Google Scholar] [CrossRef]
- Breccia, M.; Colafigli, G.; Scalzulli, E.; Martelli, M. Asciminib: An investigational agent for the treatment of chronic myeloid leukemia. Expert Opin. Investig. Drugs 2021, 30, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef]
- Réa, D.; Hughes, T.P. Development of asciminib, a novel allosteric inhibitor of BCR-ABL1. Crit. Rev. Oncol./Hematol. 2022, 171, 103580. [Google Scholar] [CrossRef] [PubMed]
- Manley, P.W.; Barys, L.; Cowan-Jacob, S.W. The specificity of asciminib, a potential treatment for chronic myeloid leukemia, as a myristate-pocket binding ABL inhibitor and analysis of its interactions with mutant forms of BCR-ABL1 kinase. Leuk. Res. 2020, 98, 106458. [Google Scholar] [CrossRef] [PubMed]
- Lipton, J.H.; Brümmendorf, T.H.; Gambacorti-Passerini, C.; Garcia-Gutiérrez, V.; Deininger, M.W.; Cortes, J.E. Long-term safety review of tyrosine kinase inhibitors in chronic myeloid leukemia—What to look for when treatment-free remission is not an option. Blood Rev. 2022, 56, 100968. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Saglio, G.; Hughes, T.P.; Larson, R.A.; Kim, D.W.; Issaragrisil, S.; Le Coutre, P.D.; Etienne, G.; Dorlhiac-Llacer, P.E.; Clark, R.E.; et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia 2016, 30, 1044–1054. [Google Scholar] [CrossRef]
- Cortes, J.E.; Kim, D.W.; Pinilla-Ibarz, J.; le Coutre, P.D.; Paquette, R.; Chuah, C.; Nicolini, F.E.; Apperley, J.F.; Khoury, H.J.; Talpaz, M.; et al. Ponatinib efficacy and safety in Philadelphia chromosome–positive leukemia: Final 5-year results of the phase 2 PACE trial. Blood 2018, 132, 393–404. [Google Scholar] [CrossRef]
- Brümmendorf, T.H.; Cortes, J.E.; de Souza, C.A.; Guilhot, F.; Duvillié, L.; Pavlov, D.; Gogat, K.; Countouriotis, A.M.; Gambacorti-Passerini, C. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukaemia: Results from the 24-month follow-up of the BELA trial. Br. J. Haematol. 2015, 168, 69–81. [Google Scholar] [CrossRef]
- Cortes, J.E.; Saglio, G.; Kantarjian, H.M.; Baccarani, M.; Mayer, J.; Boqué, C.; Shah, N.P.; Chuah, C.; Casanova, L.; Bradley-Garelik, B.; et al. Final 5-year study results of DASISION: The dasatinib versus imatinib study in treatment-Naïve chronic myeloid leukemia patients trial. J. Clin. Oncol. 2016, 34, 2333–2340. [Google Scholar] [CrossRef]
- García-Gutiérrez, V.; Hernández-Boluda, J.C. Tyrosine Kinase Inhibitors Available for Chronic Myeloid Leukemia: Efficacy and Safety. Front. Oncol. 2019, 9, 603. [Google Scholar] [CrossRef] [PubMed]
- García-Gutiérrez, V.; Breccia, M.; Jabbour, E.; Mauro, M.; Cortes, J.E. A clinician perspective on the treatment of chronic myeloid leukemia in the chronic phase. J. Hematol. Oncol. 2022, 15, 90. [Google Scholar] [CrossRef]
- Rea, D.; Mauro, M.J.; Boquimpani, C.; Minami, Y.; Lomaia, E.; Voloshin, S.; Turkina, A.; Kim, D.W.; Apperley, J.F.; Abdo, A.; et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood 2021, 138, 2031–2041. [Google Scholar] [CrossRef] [PubMed]
- Eglen, R.; Reisine, T. Drug discovery and the human kinome: Recent trends. Pharmacol. Ther. 2011, 130, 144–156. [Google Scholar] [CrossRef]
- Hughes, T.P.; Shanmuganathan, N. Management of TKI-resistant chronic phase CML. Hematology 2022, 2022, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Apperley, J.F. Chronic myeloid leukaemia. Lancet 2015, 385, 1447–1459. [Google Scholar] [CrossRef]
- Eide, C.A.; Zabriskie, M.S.; Stevens, S.L.S.; Antelope, O.; Vellore, N.A.; Than, H.; Schultz, A.R.; Clair, P.; Bowler, A.D.; Pomicter, A.D.; et al. Combining the Allosteric Inhibitor Asciminib with Ponatinib Suppresses Emergence of and Restores Efficacy against Highly Resistant BCR-ABL1 Mutants. Cancer Cell 2019, 36, 431–443.e5. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Kantarjian, H. Chronic myeloid leukemia: 2022 update on diagnosis, therapy, and monitoring. Am. J. Hematol. 2022, 97, 1236–1256. [Google Scholar] [CrossRef]
- Hughes, T.P.; Mauro, M.J.; Cortes, J.E.; Minami, H.; Rea, D.; DeAngelo, D.J.; Breccia, M.; Goh, Y.T.; Talpaz, M.; Hochhaus, A.; et al. Asciminib in Chronic Myeloid Leukemia after ABL Kinase Inhibitor Failure. N. Engl. J. Med. 2019, 381, 2315–2326. [Google Scholar] [CrossRef]
- Garcia-Gutiérrez, V.; Luna, A.; Alonso-Dominguez, J.M.; Estrada, N.; Boque, C.; Xicoy, B.; Giraldo, P.; Angona, A.; Alvarez-Larrán, A.; Sanchez-Guijo, F.; et al. Safety and efficacy of asciminib treatment in chronic myeloid leukemia patients in real-life clinical practice. Blood Cancer J. 2021, 11, 16. [Google Scholar] [CrossRef]
- Luna, A.; Pérez-Lamas, L.; Boque, C.; Giraldo, P.; Xicoy, B.; Ruiz Nuño, C.; Vega, M.M.; Alvarez-Larrán, A.; Salamanca, A.; García-Noblejas, A.; et al. Real-life analysis on safety and efficacy of asciminib for ponatinib pretreated patients with chronic myeloid leukemia. Ann. Hematol. 2022, 101, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Kockerols, C.C.; Janssen, J.J.; Blijlevens, N.M.; Klein, S.K.; van Hussen-Daenen, L.G.; Van Gorkom, G.G.; Smit, W.M.; Van Balen, P.; Biemond, B.J.; Cruijsen, M.J.; et al. Treatment patterns and clinical outcomes of asciminib in a real-world multi-resistant chronic myeloid leukemia patient population. Haematologica 2023, 108, 240–244. [Google Scholar] [CrossRef]
- García-Gutiérrez, V.; Hernandez-Boluda, J.C. An evaluation of asciminib for patients with chronic myeloid leukemia previously treated with ≥2 tyrosine kinase inhibitors. Expert Rev. Hematol. 2022, 15, 477–484. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef]
- Steegmann, J.L.; Baccarani, M.; Breccia, M.; Casado, L.F.; García-Gutiérrez, V.; Hochhaus, A.; Kim, D.W.; Kim, T.D.; Khoury, H.J.; Le Coutre, P.; et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia 2016, 30, 1648–1671. [Google Scholar] [CrossRef] [PubMed]
- Loscocco, F.; Visani, G.; Galimberti, S.; Curti, A.; Isidori, A. BCR-ABL independent mechanisms of resistance in chronic myeloid leukemia. Front. Oncol. 2019, 9, 939. [Google Scholar] [CrossRef]
- Javidi-Sharifi, N.; Hobbs, G. Future Directions in Chronic Phase CML Treatment. Curr. Hematol. Malig. Rep. 2021, 16, 500–508. [Google Scholar] [CrossRef]
- Ernst, T. Frontline Asciminib Combination in Chronic Phase CML. NCT03906292. Available online: https://clinicaltrials.gov/ct2/show/NCT03906292 (accessed on 18 December 2022).
- Issa, G.C. Phase II Study of Dual Targeting of BCR-ABL1 by Adding the Allosteric Inhibitor ABL001 in Patients with Chronic Myeloid Leukemia (CML) and Minimal Residual Disease (MRD) While on Therapy with Tyrosine Kinase Inhibitors. Available online: https://clinicaltrials.gov/ct2/show/NCT04216563 (accessed on 18 December 2022).
- Gleixner, K.V.; Filik, Y.; Berger, D.; Schewzik, C.; Stefanzl, G.; Sadovnik, I.; Degenfeld-Schonburg, L.; Eisenwort, G.; Schneeweiss-Gleixner, M.; Byrgazov, K.; et al. Asciminib and ponatinib exert synergistic anti-neoplastic effects on CML cells expressing BCR-ABL1 T315I-compound mutations. Am. J. Cancer Res. 2021, 11, 4470. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n = 77) | |
|---|---|
| Median age at data collection, y (range) | 66 (37–92) |
| Median age at diagnosis, y (range) | 52 (20–87) |
| Female sex, n (%) | 38 (49) |
| Median time on previous TKIs, y (range) | 6.9 (0.5–29) |
| Disease stage before asciminib, n (%) | |
| Chronic phase | 76 (99) |
| Accelerated phase | 1 (1) |
| Blast phase | 0 |
| Sokal risk, n (%) | |
| Low | 35 (45) |
| Intermediate | 19 (24) |
| High | 13 (17) |
| Unknown | 10 (12) |
| Switch to asciminib due to intolerance, n (%) | 49 (64) |
| Switch to asciminib due to resistance, n (%) | 28 (36) |
| TKI at diagnosis, n (%) | |
| Imatinib | 59 (77) |
| Dasatinib | 8 (10) |
| Nilotinib | 9 (12) |
| Bosutinib | 1 (1) |
| ≥3 prior TKI lines, n (%) | 63 (82) |
| Prior use of ponatinib, n (%) | 26 (34) |
| BCR::ABL1 mutations, n (%) | 19 (25) |
| T315I, n (%) | 4 (5) |
| Thombocytopenia | Anemia | Neutropenia | Cardio-Vascular Events | Arthralgias | Headache | Pleural/Pericardial Effusion | Diarrhea | Loss of Appetite | Abdominal Pain | Edema | Fatigue | Nausea | Vomiting | Pancreatitis | Skin Rash | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ITK1 |
17/77 (22%) | 18/77 (23.4%) | 11/77 (14.3%) | 1/77 (1.3%) | 13/77 (16.8%) | 5/77 (6.4%) | 3/77 (3.8%) | 11/77 (14.2%) | 7/77 (9.1%) | 7/77 (9.1%) | 18/77 (23.4%) | 10/77 (13%) | 13/77 (16.8%) | 7/77 (9.1%) | 1/77 (1.3%) | 11/77 (14.3%) |
| ITK2 |
19/77 (24.7%) | 19/77 (24.7%) | 12/77 (15.6%) | 4/77 (5.1%) | 5/77 (6.5%) | 6/77 (7.8%) | 20/77 (26%) | 6/77 (7.8%) | 5/77 (6.5%) | 6/77 (7.8%) | 10/77 (13%) | 15/77 (19.5%) | 6/77 (7.8%) | 4/77 (5.2%) | 2/77 (2.6%) | 5/77 (6.5%) |
| ITK3 |
17/63 (27%) | 18/63 (28.6%) | 10/63 (15.9%) | 9/63 (14%) | 6/63 (9.5%) | 5/63 (7.9%) | 12/63 (19%) | 12/63 (19%) | 3/63 (4.7%) | 4/63 (6.3%) | 4/63 (6.3%) | 9/63 (14.3%) | 5/63 (7.9%) | 0/63 (0%) | 2/63 (3.2%) | 4/63 (6.3%) |
| ITK4 |
8/48 (16.7%) |
9/48 (18.7%) |
4/48 (8.3%) | 0/48 (0%) | 1/48 (2.1%) | 3/48 (6.2%) | 4/48 (8.3%) | 15/48 (31.2%) | 3/48 (6.2%) | 4/48 (8.3%) | 5/48 (10.4%) | 4/48 (8.3%) | 8/48 (16.7%) | 5/48 (10.4%) | 1/48 (2.1%) | 0/48 (0%) |
| ITK5 |
7/22 (31.8%) |
2/22 (9.1%) | 3/22 (13.6%) | 2/22 (9%) | 5/22 (22.7%) | 1/22 (4.5%) | 1/22 (4.5%) | 3/22 (13.6%) | 2/22 (9.1%) | 2/22 (9.1%) | 3/22 (13.6%) | 3/22 (13.6%) | 2/22 (9.1%) | 2/22 (9.1%) | 0/22 (0%) | 3/22 (13.6%) |
| Asciminib | 13/77 (16.9%) | 9/77 (11.7%) | 5/77 (6.5%) | 0 (0%) | 9/77 (11.7%) | 1/77 (1.3%) | 4/77 (5.2%) | 1/77 (1.3%) | 2/77 (2.6%) | 4/77 (5.2%) | 2/77 (2.6%) | 14/77 (18.2%) | 6/77 (7.8%) | 2/77 (2.6%) | 2/77 (2.6%) | 4/77 (5.2%) |
| Risk of developing toxicity with asciminib in patients WITH that prior EEAA. | 12/28 (43%) | 7/32 (22%) | 4/19 (21%) | 0/15 (0%) | 5/22 (23%) | 0/14 (0%) | 3/29 (10%) | 1/38 (2.6%) | 1/12 (8%) | 1/17 (5.8%) | 1/26 (3.8%) | 7/20 (35%) | 3/22 (13.6%) | 2/12 (16.6%) | 2/6 (33%) | 1/17 (5.8%) |
| Risk of developing toxicity with asciminib in patients WITHOUT that prior EEAA. | 1/49 (2%) | 2/44 (4.6%) | 1/58 (1.7%) | 0/62 (0%) | 4/55 (7%) | 1/63 (1.6%) | 1/48 (2%) | 0/39 (0%) | 1/65 (1.5%) | 3/60 (5%) | 1/51 (2%) | 7/57 (12%) | 3/55 (5.4%) | 0/65 (0%) | 0/71 (0%) | 3/60 (5%) |
| p-value | 0.000 | 0.029 | 0.012 | 1.000 | 0.109 | 1.000 | 0.147 | 0.494 | 0.289 | 1.000 | 1.000 | 0.040 | 0.345 | 0.023 | 0.005 | 1.000 |
| Response to Asciminib | Resistant (n = 27) | Intolerant (n = 47) | Total (n = 74) |
|---|---|---|---|
| CCR a | 12/27 (44%) | 42/47 (89%) | 54/74 (73%) |
| MMR a | 7/27 (26%) | 38/47 (80%) | 45/74 (60%) |
| MR4.5 a | 4/27 (15%) | 19/47 (40%) | 23/74 (31%) |
| Patients without response at baseline | |||
| CCR b | 5/20 (25%) | 13/16 (81%) | 18/36 (50%) |
| MMR b | 5/25 (20%) | 22/30 (73%) | 27/55 (49%) |
| MR4.5 b | 4/27 (15%) | 16/44 (32%) | 20/71 (28%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Lamas, L.; Luna, A.; Boque, C.; Xicoy, B.; Giraldo, P.; Pérez López, R.; Ruiz Nuño, C.; De las Heras, N.; Mora Casterá, E.; López Marín, J.; et al. Toxicity of Asciminib in Real Clinical Practice: Analysis of Side Effects and Cross-Toxicity with Tyrosine Kinase Inhibitors. Cancers 2023, 15, 1045. https://doi.org/10.3390/cancers15041045
Pérez-Lamas L, Luna A, Boque C, Xicoy B, Giraldo P, Pérez López R, Ruiz Nuño C, De las Heras N, Mora Casterá E, López Marín J, et al. Toxicity of Asciminib in Real Clinical Practice: Analysis of Side Effects and Cross-Toxicity with Tyrosine Kinase Inhibitors. Cancers. 2023; 15(4):1045. https://doi.org/10.3390/cancers15041045
Chicago/Turabian StylePérez-Lamas, Lucía, Alejandro Luna, Concepción Boque, Blanca Xicoy, Pilar Giraldo, Raúl Pérez López, Concepción Ruiz Nuño, Natalia De las Heras, Elvira Mora Casterá, Javier López Marín, and et al. 2023. "Toxicity of Asciminib in Real Clinical Practice: Analysis of Side Effects and Cross-Toxicity with Tyrosine Kinase Inhibitors" Cancers 15, no. 4: 1045. https://doi.org/10.3390/cancers15041045
APA StylePérez-Lamas, L., Luna, A., Boque, C., Xicoy, B., Giraldo, P., Pérez López, R., Ruiz Nuño, C., De las Heras, N., Mora Casterá, E., López Marín, J., Segura Díaz, A., Gómez, V., Vélez Tenza, P., Sierra Pacho, M., Vera Goñi, J. A., Moreno Vega, M., Alvarez-Larrán, A., Cortés, M., Pérez Encinas, M., ... García-Gutiérrez, V. (2023). Toxicity of Asciminib in Real Clinical Practice: Analysis of Side Effects and Cross-Toxicity with Tyrosine Kinase Inhibitors. Cancers, 15(4), 1045. https://doi.org/10.3390/cancers15041045