
Treatment Outcomes of Proton Beam Therapy for Esophageal Squamous Cell Carcinoma at a Single Institute

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PBT Planning and Delivery
2.3. Chemotherapy
2.4. Clinical Assessment
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
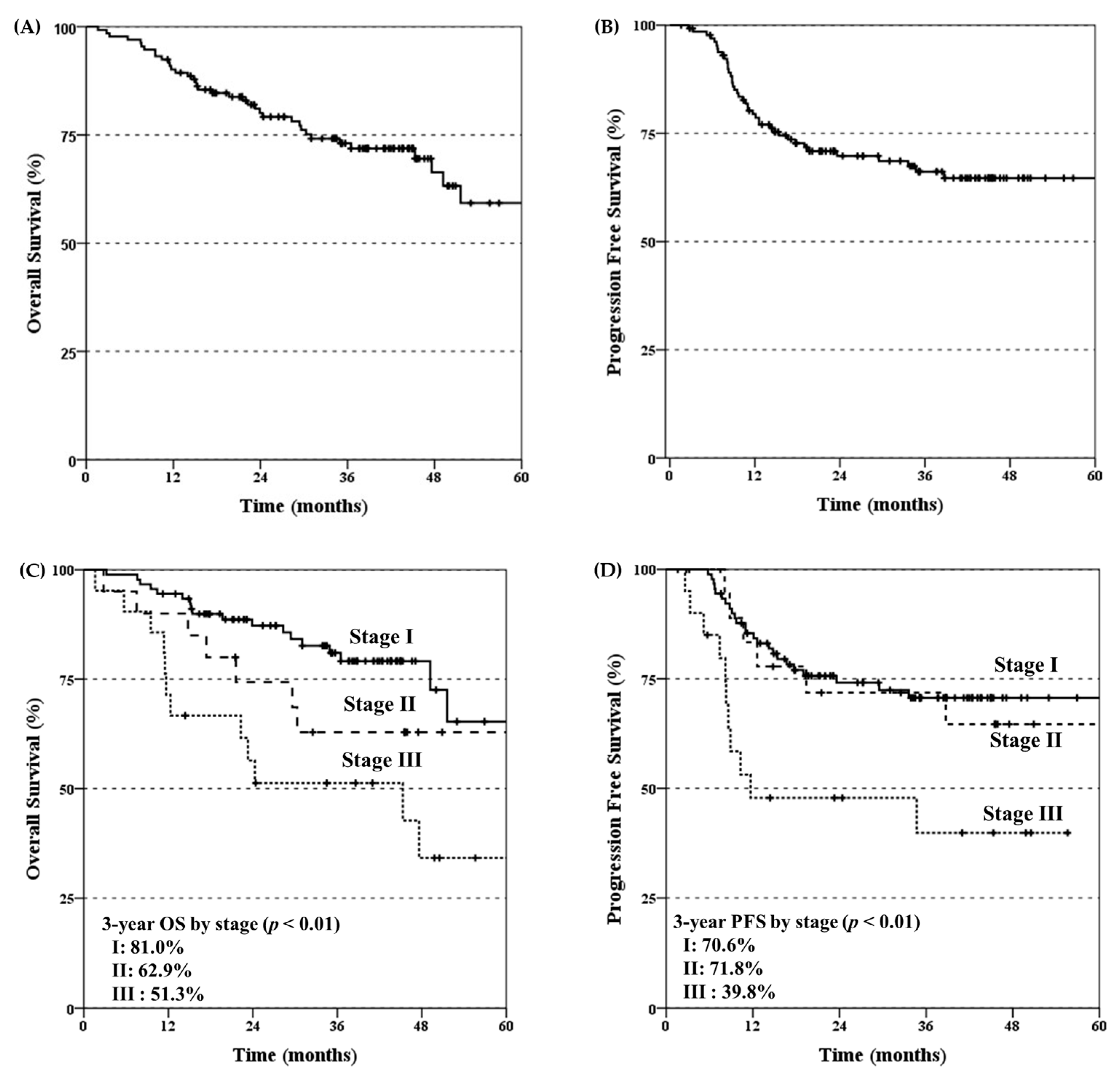
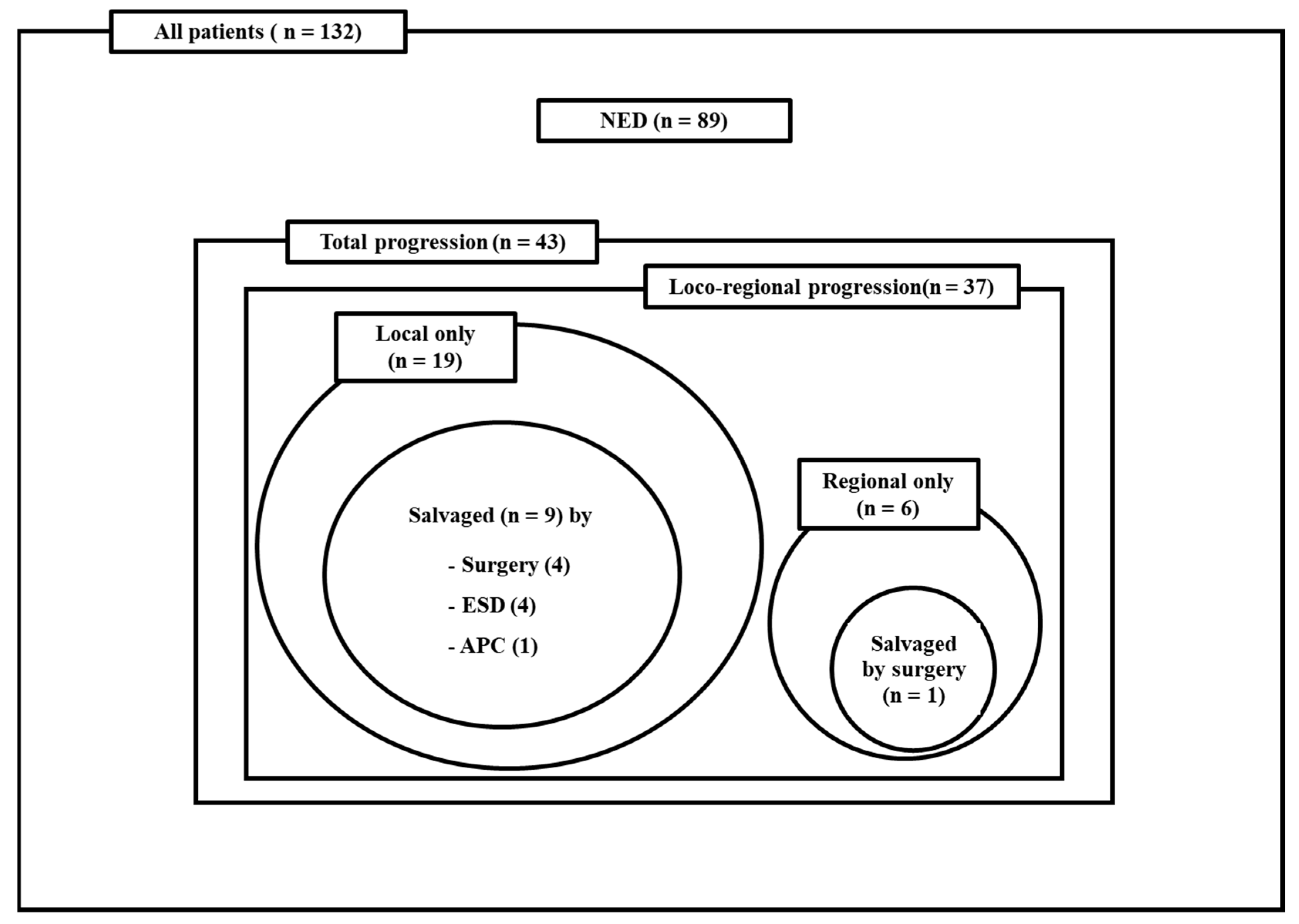
3.2. Survival Outcomes and Patterns of Disease Progression
3.3. Prognostic Factor Analysis
3.4. Treatment-Related Toxicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Noordman, B.J.; Spaander, M.C.W.; Valkema, R.; Wijnhoven, B.P.L.; van Berge Henegouwen, M.I.; Shapiro, J.; Biermann, K.; van der Gaast, A.; van Hillegersberg, R.; Hulshof, M.; et al. Detection of residual disease after neoadjuvant chemoradiotherapy for oesophageal cancer (preSANO): A prospective multicentre, diagnostic cohort study. Lancet Oncol. 2018, 19, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lievre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef] [PubMed]
- Eyck, B.M.; van Lanschot, J.J.B.; Hulshof, M.; van der Wilk, B.J.; Shapiro, J.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; et al. Ten-Year Outcome of Neoadjuvant Chemoradiotherapy Plus Surgery for Esophageal Cancer: The Randomized Controlled CROSS Trial. J. Clin. Oncol. 2021, 39, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Nakajima, T.E.; Ito, Y.; Katada, C.; Ishiyama, H.; Tokunaga, S.Y.; Tanaka, M.; Hironaka, S.; Hashimoto, T.; Ura, T.; et al. Phase II study of concurrent chemoradiotherapy at the dose of 50.4 Gy with elective nodal irradiation for Stage II-III esophageal carcinoma. Jpn. J. Clin. Oncol. 2013, 43, 608–615. [Google Scholar] [CrossRef]
- Lin, S.H.; Merrell, K.W.; Shen, J.; Verma, V.; Correa, A.M.; Wang, L.; Thall, P.F.; Bhooshan, N.; James, S.E.; Haddock, M.G.; et al. Multi-institutional analysis of radiation modality use and postoperative outcomes of neoadjuvant chemoradiation for esophageal cancer. Radiother. Oncol. 2017, 123, 376–381. [Google Scholar] [CrossRef]
- Wang, J.; Wei, C.; Tucker, S.L.; Myles, B.; Palmer, M.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Cox, J.D.; Komaki, R.; et al. Predictors of postoperative complications after trimodality therapy for esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 885–891. [Google Scholar] [CrossRef]
- Shiraishi, Y.; Xu, C.; Yang, J.; Komaki, R.; Lin, S.H. Dosimetric comparison to the heart and cardiac substructure in a large cohort of esophageal cancer patients treated with proton beam therapy or Intensity-modulated radiation therapy. Radiother. Oncol. 2017, 125, 48–54. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, J.M.; Kim, M.S.; Lee, Y.; Suh, Y.G.; Lee, S.U.; Lee, D.Y.; Oh, E.S.; Kim, T.H.; Moon, S.H. A Comparative Analysis of Photon versus Proton Beam Therapy in Neoadjuvant Concurrent Chemoradiotherapy for Intrathoracic Squamous Cell Carcinoma of the Esophagus at a Single Institute. Cancers 2022, 14, 2033. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.G.; Bayasgalan, U.; Kim, H.T.; Lee, J.M.; Kim, M.S.; Lee, Y.; Lee, D.Y.; Lee, S.U.; Kim, T.H.; Moon, S.H. Photon Versus Proton Beam Therapy for T1-3 Squamous Cell Carcinoma of the Thoracic Esophagus Without Lymph Node Metastasis. Front. Oncol. 2021, 11, 699172. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Hobbs, B.P.; Verma, V.; Tidwell, R.S.; Smith, G.L.; Lei, X.; Corsini, E.M.; Mok, I.; Wei, X.; Yao, L.; et al. Randomized Phase IIB Trial of Proton Beam Therapy Versus Intensity-Modulated Radiation Therapy for Locally Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Xi, M.; Xu, C.; Liao, Z.; Chang, J.Y.; Gomez, D.R.; Jeter, M.; Cox, J.D.; Komaki, R.; Mehran, R.; Blum, M.A.; et al. Comparative Outcomes After Definitive Chemoradiotherapy Using Proton Beam Therapy Versus Intensity Modulated Radiation Therapy for Esophageal Cancer: A Retrospective, Single-Institutional Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 667–676. [Google Scholar] [CrossRef]
- Wang, X.; Hobbs, B.; Gandhi, S.J.; Muijs, C.T.; Langendijk, J.A.; Lin, S.H. Current status and application of proton therapy for esophageal cancer. Radiother. Oncol. 2021, 164, 27–36. [Google Scholar] [CrossRef]
- Ono, T.; Wada, H.; Ishikawa, H.; Tamamura, H.; Tokumaru, S. Clinical Results of Proton Beam Therapy for Esophageal Cancer: Multicenter Retrospective Study in Japan. Cancers 2019, 11, 993. [Google Scholar] [CrossRef]
- Motoori, M.; Yano, M.; Ishihara, R.; Yamamoto, S.; Kawaguchi, Y.; Tanaka, K.; Kishi, K.; Miyashiro, I.; Fujiwara, Y.; Shingai, T.; et al. Comparison between radical esophagectomy and definitive chemoradiotherapy in patients with clinical T1bN0M0 esophageal cancer. Ann. Surg. Oncol. 2012, 19, 2135–2141. [Google Scholar] [CrossRef]
- Koide, Y.; Kodaira, T.; Tachibana, H.; Tomita, N.; Makita, C.; Itoh, M.; Abe, T.; Muro, K.; Tajika, M.; Niwa, Y.; et al. Clinical outcome of definitive radiation therapy for superficial esophageal cancer. Jpn. J. Clin. Oncol. 2017, 47, 393–400. [Google Scholar] [CrossRef]
- Kato, H.; Sato, A.; Fukuda, H.; Kagami, Y.; Udagawa, H.; Togo, A.; Ando, N.; Tanaka, O.; Shinoda, M.; Yamana, H.; et al. A phase II trial of chemoradiotherapy for stage I esophageal squamous cell carcinoma: Japan Clinical Oncology Group Study (JCOG9708). Jpn. J. Clin. Oncol. 2009, 39, 638–643. [Google Scholar] [CrossRef]
- Wang, A.; Lu, L.; Fan, J.; Wang, S.; Chen, X. Lymph node metastatic patterns and its clinical significance for thoracic superficial esophageal squamous cell carcinoma. J. Cardiothorac. Surg. 2020, 15, 262. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Yin, W.; Yao, H.; Gu, W. Salvage treatment for lymph node recurrence after radical resection of esophageal squamous cell carcinoma. Radiat. Oncol. 2019, 14, 169. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Moon, S.H.; Cho, K.H.; Kim, T.H.; Kim, M.S.; Lee, J.Y.; Suh, Y.G. Treatment outcomes of extended-field radiation therapy for thoracic superficial esophageal cancer. Radiat. Oncol. J. 2017, 35, 241–248. [Google Scholar] [CrossRef]
- Kato, K.; Muro, K.; Minashi, K.; Ohtsu, A.; Ishikura, S.; Boku, N.; Takiuchi, H.; Komatsu, Y.; Miyata, Y.; Fukuda, H.; et al. Phase II study of chemoradiotherapy with 5-fluorouracil and cisplatin for Stage II-III esophageal squamous cell carcinoma: JCOG trial (JCOG 9906). Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 684–690. [Google Scholar] [CrossRef]
- Nishimura, Y.; Mitsumori, M.; Hiraoka, M.; Koike, R.; Nakamatsu, K.; Kawamura, M.; Negoro, Y.; Fujiwara, K.; Sakurai, H.; Mitsuhashi, N. A randomized phase II study of cisplatin/5-FU concurrent chemoradiotherapy for esophageal cancer: Short-term infusion versus protracted infusion chemotherapy (KROSG0101/JROSG021). Radiother. Oncol. 2009, 92, 260–265. [Google Scholar] [CrossRef]
- Tang, C.; Liao, Z.; Gomez, D.; Levy, L.; Zhuang, Y.; Gebremichael, R.A.; Hong, D.S.; Komaki, R.; Welsh, J.W. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Ye, X.; Ellsworth, S.G.; Smith, J.A.; Narang, A.K.; Garg, T.; Campian, J.; Laheru, D.A.; Zheng, L.; Wolfgang, C.L.; et al. The Association Between Chemoradiation-related Lymphopenia and Clinical Outcomes in Patients With Locally Advanced Pancreatic Adenocarcinoma. Am. J. Clin. Oncol. 2015, 38, 259–265. [Google Scholar] [CrossRef]
- Davuluri, R.; Jiang, W.; Fang, P.; Xu, C.; Komaki, R.; Gomez, D.R.; Welsh, J.; Cox, J.D.; Crane, C.H.; Hsu, C.C.; et al. Lymphocyte Nadir and Esophageal Cancer Survival Outcomes After Chemoradiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 128–135. [Google Scholar] [CrossRef]
- Liu, M.; Li, X.; Cheng, H.; Wang, Y.; Tian, Y. The Impact of Lymphopenia and Dosimetric Parameters on Overall Survival of Esophageal Cancer Patients Treated with Definitive Radiotherapy. Cancer Manag. Res. 2021, 13, 2917–2924. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Total, N (%) | |
|---|---|---|
| Sex | Male | 121 (91.7) |
| Female | 11 (8.3) | |
| Age (year) | Median (range) | 70 (40–89) |
| ECOG PS | 0 | 62 (47.0) |
| 1 | 65 (49.2) | |
| 2 | 5 (3.8) | |
| Histology | Squamous cell carcinoma | 132 (100) |
| Tumor location | Upper thoracic | 16 (12.1) |
| Middle thoracic | 53 (40.2) | |
| Lower thoracic | 59 (44.7) | |
| EG Junction | 4 (3.0) | |
| cT classification | T1a | 16 (12.1) |
| T1b | 75 (56.8) | |
| T2 | 18 (13.6) | |
| T3 | 23 (17.4) | |
| cN classification | N0 | 95 (72.0) |
| N1 | 29 (22.0) | |
| N2 | 8 (6.0) | |
| AJCC stage | I | 91 (68.9) |
| II | 20 (15.1) | |
| III | 21 (16.0) | |
| RT total dose (cGy) | Median (range) | 6600 (4500–7020) |
| RT fraction size (cGy) | Median (range) | 200 (180–210) |
| RT fraction number (fx) | Median (range) | 33 (24–39) |
| Concurrent | No | 81 (61.4) |
| chemotherapy | Xeloda + Cisplatin | 10 (7.6) |
| regimen | Carboplatin + Paclitaxel | 27 (20.4) |
| Capecitabine/Xeloda only | 10 (7.6) | |
| Others | 4 (3.0) | |
| Concurrent | No | 81 (61.4) |
| chemotherapy | q 3 weeks | 17 (12.9) |
| schedule | weekly | 33 (25.0) |
| others | 1 (0.7) | |
| Neoadjuvant chemotherapy | No | 132 (100) |
| No. of Patients, (%) | |||||
|---|---|---|---|---|---|
| Grade | 0 | 1–2 | 3 | 4 | 5 |
| Acute toxicity | |||||
| Esophagitis | 35 (26.5) | 94 (71.2) | 3 (2.3) | 0 (0) | 0 (0) |
| Pneumonitis | 125 (94.7) | 7 (3.0) | 0 (0) | 0 (0) | 0 (0) |
| Dermatitis | 106 (80.3) | 26 (19.7) | 0 (0) | 0 (0) | 0 (0) |
| Anemia | 122 (92.5) | 8 (6.0) | 2 (1.5) | 0 (0) | 0 (0) |
| Neutropenia | 117 (88.7) | 7 (5.3) | 6 (4.5) | 2 (1.5) | 0 (0) |
| Lymphopenia | 65 (49.3) | 38 (28.7) | 29 (22.0) | 0 (0) | 0 (0) |
| Thrombocytopenia | 128 (97.0) | 4 (3.0) | 0 (0) | 0 (0) | 0 (0) |
| Late toxicity | |||||
| Pleural effusion | 96 (72.7) | 34 (25.8) | 2 (1.5) | 0 (0) | 0 (0) |
| Pericardial effusion | 115 (87.1) | 15 (11.5) | 1 (0.7) | 1 (0.7) | 0 (0) |
| Esophageal fistula | 126 (95.4) | 3(2.3) | 2 (1.5) | 1 (0.7) | 0 (0) |
| Esophageal stenosis | 109 (82.6) | 17 (12.9) | 6 (4.5) | 0 (0) | 0 (0) |
| Pneumonitis | 132 (100.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, E.S.; Moon, S.H.; Lee, Y.; Ahn, B.-C.; Lee, J.Y.; Suh, Y.-G.; Chung, J.-H.; Kim, M.S.; Lee, J.M.; Choi, J.-H.; et al. Treatment Outcomes of Proton Beam Therapy for Esophageal Squamous Cell Carcinoma at a Single Institute. Cancers 2023, 15, 5524. https://doi.org/10.3390/cancers15235524
Oh ES, Moon SH, Lee Y, Ahn B-C, Lee JY, Suh Y-G, Chung J-H, Kim MS, Lee JM, Choi J-H, et al. Treatment Outcomes of Proton Beam Therapy for Esophageal Squamous Cell Carcinoma at a Single Institute. Cancers. 2023; 15(23):5524. https://doi.org/10.3390/cancers15235524
Chicago/Turabian StyleOh, Eun Sang, Sung Ho Moon, Youngjoo Lee, Beung-Chul Ahn, Jong Yeul Lee, Yang-Gun Suh, Joo-Hyun Chung, Moon Soo Kim, Jong Mog Lee, Jin-Ho Choi, and et al. 2023. "Treatment Outcomes of Proton Beam Therapy for Esophageal Squamous Cell Carcinoma at a Single Institute" Cancers 15, no. 23: 5524. https://doi.org/10.3390/cancers15235524
APA StyleOh, E. S., Moon, S. H., Lee, Y., Ahn, B.-C., Lee, J. Y., Suh, Y.-G., Chung, J.-H., Kim, M. S., Lee, J. M., Choi, J.-H., & Kim, T. H. (2023). Treatment Outcomes of Proton Beam Therapy for Esophageal Squamous Cell Carcinoma at a Single Institute. Cancers, 15(23), 5524. https://doi.org/10.3390/cancers15235524