

The Impact of Digital Inequities on Esophageal Cancer Disparities in the US

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Population Definitions
2.3. Statistical Methods
3. Results
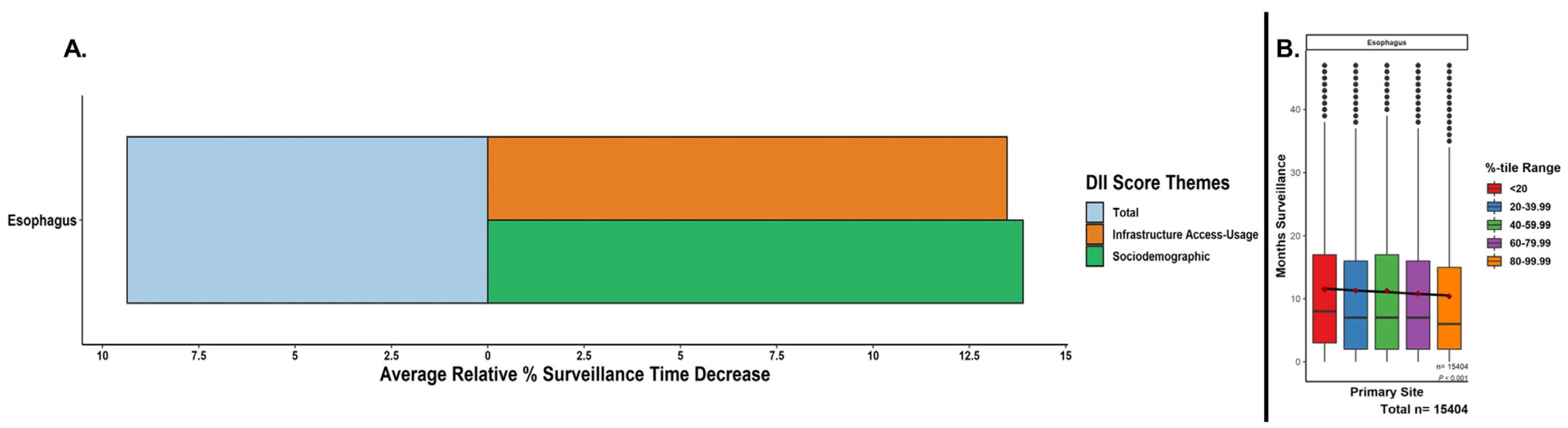
3.1. Trends in Months under Surveillance and Survival by Relative DII Percentile
3.2. Trends in Staging and Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Koulaouzidis, A.; Marlicz, W.; Lok, V.; Chu, C.; Ngai, C.H.; Zhang, L.; Chen, P.; Wang, S.; Yuan, J.; et al. Global Burden, Risk Factors, and Trends of Esophageal Cancer: An Analysis of Cancer Registries from 48 Countries. Cancers 2021, 13, 141. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Benipal, B. Incidence of Esophageal Cancer in the United States from 2001-2015: A United States Cancer Statistics Analysis of 50 States. Cureus 2018, 10, e3709. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.-H.; Lagergren, J. Social group disparities in the incidence and prognosis of oesophageal cancer. United Eur. Gastroenterol. J. 2018, 6, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Chen, I.-C.; Chen, Y.-H.; Chen, C.-C.; Chuang, C.-Y.; Lin, C.-H. The Influence of Socioeconomic Status on Esophageal Cancer in Taiwan: A Population-Based Study. J. Pers. Med. 2022, 12, 595. [Google Scholar] [CrossRef]
- Sridhar, P.; Bhatt, M.; Qureshi, M.M.; Asokan, S.; Truong, M.T.; Suzuki, K.; Mak, K.S.; Litle, V.R. Esophageal Cancer Presentation, Treatment, and Outcomes Vary with Hospital Safety-Net Burden. Ann. Thorac. Surg. 2019, 107, 1472–1479. [Google Scholar] [CrossRef]
- Adler, K.G. Screening for Social Determinants of Health: An Opportunity or Unreasonable Burden? Fam. Pract. Manag. 2018, 25, 3. [Google Scholar]
- Becker, D.; Grapendorf, J.; Greving, H.; Sassenberg, K. Perceived Threat and Internet Use Predict Intentions to Get Bowel Cancer Screening (Colonoscopy): Longitudinal Questionnaire Study. J. Med. Internet Res. 2018, 20, e46. [Google Scholar] [CrossRef] [PubMed]
- Killeen, S.; Hennessey, A.; El Hassan, Y.; Killeen, K.; Clarke, N.; Murray, K.; Waldron, B. Gastric cancer–related information on the Internet: Incomplete, poorly accessible, and overly commercial. Am. J. Surg. 2011, 201, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.Y.; Willicombe, A.; Reid, T.D.; Beaton, C.; Arnold, D.; Ward, J.; Davies, I.L.; Lewis, W.G. Relative Quality of Internet-Derived Gastrointestinal Cancer Information. J. Cancer Educ. 2012, 27, 676–679. [Google Scholar] [CrossRef]
- Connect2HealthFCC-Mapping Broadband Health in America. 2017. Available online: https://www.fcc.gov/reports-research/maps/connect2health/#ll=39.325799,-90.612488&z=6&t=insights&inb=in_bb_access&inh=in_diabetes_rate&dmf=none&inc=none&slb=90,100&slh=10,22 (accessed on 11 February 2023).
- Skevofilakas, M.; Mougiakakou, S.G.; Zarkogianni, K.; Aslanoglou, E.; Pavlopoulos, S.A.; Vazeou, A.; Bartsocas, C.S.; Nikita, K.S. A communication and information technology infrastructure for real time monitoring and management of type 1 diabetes patients. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; Volume 2007, pp. 3685–3688. [Google Scholar] [CrossRef]
- Connect2HealthFCC. Federal Communications Commission. 2015. Available online: https://www.fcc.gov/about-fcc/fcc-initiatives/connect2healthfcc (accessed on 11 February 2023).
- Digital Inclusion|Digital Divide Index. Available online: https://pcrd.purdue.edu/ruralindianastats/broadband/ddi.php?variable=ddi-map&county=Adams (accessed on 11 February 2023).
- Ellison, P.M.; Vanderpool, R.C. Preface: Experiencing Cancer in Appalachian Kentucky. J. Appalach. Health 2020, 2, 71. [Google Scholar] [CrossRef]
- Hesse, B.W.; Ahern, D.; Ellison, M.; Aronoff-Spencer, E.; Vanderpool, R.C.; Onyeije, K.; Gibbons, M.C.; Mullett, T.W.; Chih, M.-Y.; Attencio, V.; et al. Barn-Raising on the Digital Frontier: The L.A.U.N.C.H. Collaborative. J. Appalach. Health 2020, 2, 8. [Google Scholar] [CrossRef]
- Chih, M.-Y.; McCowan, A.; Whittaker, S.; Krakow, M.; Ahern, D.K.; Aronoff-Spencer, E.; Hesse, B.W.; Mullett, T.W.; Vanderpool, R.C. The Landscape of Connected Cancer Symptom Management in Rural America: A Narrative Review of Opportunities for Launching Connected Health Interventions. J. Appalach. Health 2020, 2, 66. [Google Scholar] [CrossRef]
- Fei-Zhang, D.J.; Chelius, D.C.; Patel, U.A.; Smith, S.S.; Sheyn, A.M.; Rastatter, J.C. Assessment of Social Vulnerability in Pediatric Head and Neck Cancer Care and Prognosis in the United States. JAMA Netw. Open 2023, 6, e230016. [Google Scholar] [CrossRef]
- Kawakatsu, Y.; Koyanagi, Y.N.; Oze, I.; Kasugai, Y.; Morioka, H.; Yamaguchi, R.; Ito, H.; Matsuo, K. Association between Socioeconomic Status and Digestive Tract Cancers: A Case-Control Study. Cancers 2020, 12, 3258. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.-X.; Yuan, W.-J.; Huang, C.-H.; Xiao, L.; Xiao, R.-S.; Zeng, P.-W.; Chen, L.; Chen, Z.-H. Socioeconomic deprivation and survival outcomes in patients with colorectal cancer. Am. J. Cancer Res. 2022, 12, 829–838. [Google Scholar]
- Cheng, E.; Soulos, P.R.; Irwin, M.L.; Feliciano, E.M.C.; Presley, C.J.; Fuchs, C.S.; Meyerhardt, J.A.; Gross, C.P. Neighborhood and Individual Socioeconomic Disadvantage and Survival Among Patients with Nonmetastatic Common Cancers. JAMA Netw. Open 2021, 4, e2139593. [Google Scholar] [CrossRef] [PubMed]
- Holowatyj, A.N.; Langston, M.E.; Han, Y.; Viskochil, R.; Perea, J.; Cao, Y.; Rogers, C.R.; Lieu, C.H.; Moore, J.X. Community Health Behaviors and Geographic Variation in Early-Onset Colorectal Cancer Survival Among Women. Clin. Transl. Gastroenterol. 2020, 11, e00266. [Google Scholar] [CrossRef]
- Edwards, E.R.; Fei-Zhang, D.J.; Stein, A.P.; Lott, D.G.; Chelius, D.C.; Sheyn, A.; Rastatter, J. The impact of digital inequities on laryngeal cancer disparities in the US. Am. J. Otolaryngol. 2024, 45, 104066. [Google Scholar] [CrossRef]
- McCampbell, L.; Fei-Zhang, D.J.; Chelius, D.; Rastatter, J.; Sheyn, A. Analyzing County-Level Social Vulnerabilities of Head and Neck Melanomas in the United States. Laryngoscope 2023. [Google Scholar] [CrossRef]
- Lutfallah, S.; Fei-Zhang, D.; Chelius, D.; D’Souza, J.; Paludo, J.; Ruff, M.W.; Rastatter, J.; Sheyn, A. Evaluating social vulnerability impact on care and prognosis of head & neck-nervous system cancers in the US. J. Clin. Oncol. 2023, 41, 6526. [Google Scholar] [CrossRef]
- Stanisic, A.V.; Wu, E.; Fei-Zhang, D.J.; Lewis-Thames, M.; Badawy, S.M. The Influence of Social Vulnerability on the Prognosis of Chronic Myeloid Leukemia in Adults across the United States. Blood 2022, 140, 8129–8130. [Google Scholar] [CrossRef]
- Wu, E.; Stanisic, A.V.; Fei-Zhang, D.J.; Lewis-Thames, M.; Badawy, S.M. The Effects of Social Vulnerability on the Prognosis and Outcomes of Hodgkin’s Lymphoma in Adults across the United States. Blood 2022, 140, 10974–10975. [Google Scholar] [CrossRef]
- Fei-Zhang, D.J.; Chelius, D.C.; Sheyn, A.M.; Rastatter, J.C. Large-data contextualizations of social determinant associations in pediatric head and neck cancers. Curr. Opin. Otolaryngol. Head Neck Surg. 2023, 31, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Azap, L.; Azap, R.; Hyer, M.; Diaz, A.; Pawlik, T.M. The association of upward economic mobility with textbook outcomes among patients undergoing general and cardiovascular surgery. Am. J. Surg. 2023, 225, 494–498. [Google Scholar] [CrossRef]
- Lima, H.A.; Woldesenbet, S.; Moazzam, Z.; Endo, Y.; Munir, M.M.; Shaikh, C.; Rueda, B.O.; Alaimo, L.; Resende, V.; Pawlik, T.M. Association of Minority-Serving Hospital Status with Post-Discharge Care Utilization and Expenditures in Gastrointestinal Cancer. Ann. Surg. Oncol. 2023, 30, 7217–7225. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Li, M.; Kang, R.; Liu, X.; Wang, N.; Zhu, Q.; Cao, J.; Cong, M. The effectiveness of telephone and internet-based supportive care for patients with esophageal cancer on enhanced recovery after surgery in China: A randomized controlled trial. Asia-Pacific J. Oncol. Nurs. 2022, 9, 217–228. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Total Digital Inequity Index Category | ||||||
|---|---|---|---|---|---|---|
| Characteristic | n | Lowest Total DII, n = 11,032 (70%) | Lower Total DII, n = 2328 (15%) | Middle Total DII, n = 1195 (7.6%) | Higher Total DII, n = 558 (3.6%) | Highest Total DII, n = 543 (3.5%) |
| Age | 15,656 | |||||
| 20–44 Years | 255 (2.3%) | 42 (1.8%) | 27 (2.3%) | 15 (2.7%) | 10 (1.8%) | |
| 45–64 Years | 3842 (35%) | 870 (37%) | 477 (40%) | 254 (46%) | 242 (45%) | |
| 65–84 Years | 5882 (53%) | 1237 (53%) | 624 (52%) | 255 (46%) | 270 (50%) | |
| 85+ Years | 1053 (9.5%) | 179 (7.7%) | 67 (5.6%) | 34 (6.1%) | 21 (3.9%) | |
| Sex | 15,656 | |||||
| Male | 8481 (77%) | 1790 (77%) | 959 (80%) | 465 (83%) | 447 (82%) | |
| Female | 2551 (23%) | 538 (23%) | 236 (20%) | 93 (17%) | 96 (18%) | |
| Race | 15,656 | |||||
| White | 8300 (75%) | 1834 (79%) | 959 (80%) | 434 (78%) | 396 (73%) | |
| Black | 867 (7.9%) | 324 (14%) | 161 (13%) | 87 (16%) | 121 (22%) | |
| Hispanic | 1047 (9.5%) | 121 (5.2%) | 54 (4.5%) | 10 (1.8%) | 18 (3.3%) | |
| Asian or Pacific Islander | 709 (6.4%) | 34 (1.5%) | 11 (0.9%) | 23 (4.1%) | 0 (0%) | |
| Native American | 59 (0.5%) | 11 (0.5%) | 7 (0.6%) | 1 (0.2%) | 5 (0.9%) | |
| Unknown | 50 (0.5%) | 4 (0.2%) | 3 (0.3%) | 3 (0.5%) | 3 (0.6%) | |
| Region | 15,656 | |||||
| Midwest | 823 (7.5%) | 700 (30%) | 231 (19%) | 56 (10%) | 6 (1.1%) | |
| Northeast | 2018 (18%) | 531 (23%) | 85 (7.1%) | 0 (0%) | 0 (0%) | |
| South | 1669 (15%) | 573 (25%) | 647 (54%) | 440 (79%) | 480 (88%) | |
| West | 6522 (59%) | 524 (23%) | 232 (19%) | 62 (11%) | 57 (10%) | |
| ICD-O-3 Histopathology | 15,656 | |||||
| Adenocarcinomas | 6696 (61%) | 1392 (60%) | 734 (61%) | 333 (60%) | 290 (53%) | |
| Squamous Cell Neoplasms | 3455 (31%) | 708 (30%) | 374 (31%) | 178 (32%) | 202 (37%) | |
| Epithelial Neoplasms, NOS | 442 (4.0%) | 110 (4.7%) | 35 (2.9%) | 22 (3.9%) | 25 (4.6%) | |
| Unspecified Neoplasms | 338 (3.1%) | 92 (4.0%) | 44 (3.7%) | 22 (3.9%) | 23 (4.2%) | |
| Complex Epithelial Neoplasms | 101 (0.9%) | 26 (1.1%) | 8 (0.7%) | 3 (0.5%) | 3 (0.6%) | |
| TNM Combined Staging | 13,818 | |||||
| Stage I–III | 5678 (58%) | 1186 (58%) | 595 (56%) | 254 (53%) | 283 (60%) | |
| Stage IV & Above | 4089 (42%) | 859 (42%) | 466 (44%) | 221 (47%) | 187 (40%) | |
| No. of Primary Tumors by Dx | 15,060 | |||||
| 1 | 8144 (77%) | 1746 (78%) | 898 (78%) | 446 (82%) | 414 (79%) | |
| 2 or More | 2446 (23%) | 503 (22%) | 253 (22%) | 97 (18%) | 113 (21%) | |
| Primary Surgery Performed | 15,027 | |||||
| No Surgery | 8114 (76%) | 1676 (75%) | 884 (78%) | 404 (79%) | 409 (81%) | |
| Surgery | 2537 (24%) | 547 (25%) | 252 (22%) | 107 (21%) | 97 (19%) | |
| Radiation Therapy Performed | 15,656 | |||||
| No Therapy | 5073 (46%) | 1068 (46%) | 555 (46%) | 247 (44%) | 251 (46%) | |
| Therapy | 5959 (54%) | 1260 (54%) | 640 (54%) | 311 (56%) | 292 (54%) | |
| Chemotherapy Performed | 15,656 | |||||
| No Therapy | 4349 (39%) | 969 (42%) | 501 (42%) | 228 (41%) | 223 (41%) | |
| Therapy | 6683 (61%) | 1359 (58%) | 694 (58%) | 330 (59%) | 320 (59%) | |
| Vital Status on Last Follow-up | 15,656 | |||||
| Alive | 4478 (41%) | 875 (38%) | 449 (38%) | 185 (33%) | 172 (32%) | |
| Dead | 6554 (59%) | 1453 (62%) | 746 (62%) | 373 (67%) | 371 (68%) | |
| Outcome | DII Characteristic | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Advanced Staging | Total | 1.02 | 1.00, 1.05 | 0.042 |
| Infrastructure Access & Usage | 1.04 | 1.01, 1.06 | 0.003 | |
| Sociodemographic | 1.06 | 1.03, 1.08 | 0.000 | |
| Chemotherapy | Total | 0.97 | 0.95, 0.99 | 0.028 |
| Infrastructure Access & Usage | 0.96 | 0.94, 0.99 | 0.001 | |
| Sociodemographic | 0.97 | 0.95, 1.00 | 0.023 | |
| Radiation | Total | 0.98 | 0.96, 1.00 | 0.105 |
| Infrastructure Access & Usage | 0.98 | 0.95, 1.00 | 0.038 | |
| Sociodemographic | 1.00 | 0.98, 1.03 | 0.733 | |
| Surgical Resection | Total | 0.97 | 0.95, 0.99 | 0.048 |
| Infrastructure Access & Usage | 0.95 | 0.93, 0.98 | 0.000 | |
| Sociodemographic | 0.96 | 0.94, 0.99 | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fei-Zhang, D.J.; Edwards, E.R.; Asthana, S.; Chelius, D.C.; Sheyn, A.M.; Rastatter, J.C. The Impact of Digital Inequities on Esophageal Cancer Disparities in the US. Cancers 2023, 15, 5522. https://doi.org/10.3390/cancers15235522
Fei-Zhang DJ, Edwards ER, Asthana S, Chelius DC, Sheyn AM, Rastatter JC. The Impact of Digital Inequities on Esophageal Cancer Disparities in the US. Cancers. 2023; 15(23):5522. https://doi.org/10.3390/cancers15235522
Chicago/Turabian StyleFei-Zhang, David J., Evan R. Edwards, Shravan Asthana, Daniel C. Chelius, Anthony M. Sheyn, and Jeffrey C. Rastatter. 2023. "The Impact of Digital Inequities on Esophageal Cancer Disparities in the US" Cancers 15, no. 23: 5522. https://doi.org/10.3390/cancers15235522
APA StyleFei-Zhang, D. J., Edwards, E. R., Asthana, S., Chelius, D. C., Sheyn, A. M., & Rastatter, J. C. (2023). The Impact of Digital Inequities on Esophageal Cancer Disparities in the US. Cancers, 15(23), 5522. https://doi.org/10.3390/cancers15235522