
Current Status of Radiolabeled Monoclonal Antibodies Targeting PSMA for Imaging and Therapy

Abstract
:Simple Summary
Abstract
1. Introduction
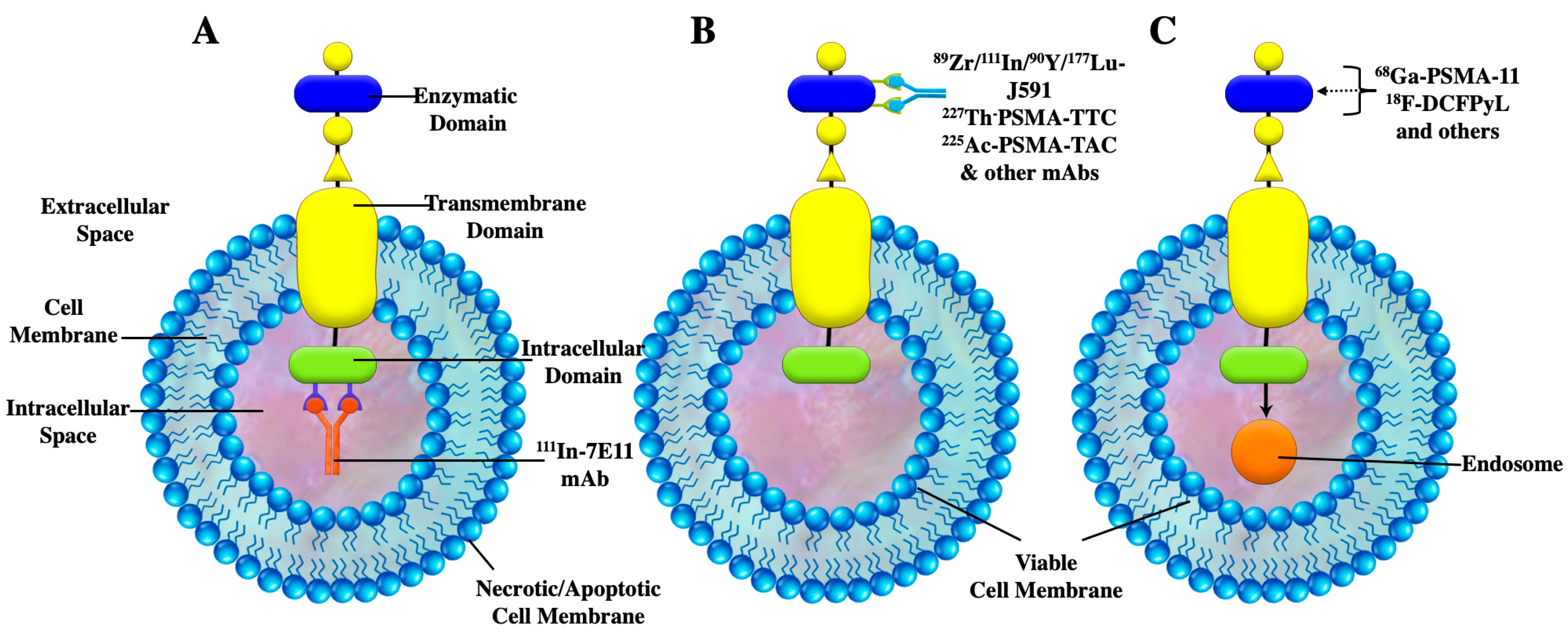
2. Radiolabeled Monoclonal Antibodies Targeting PSMA
2.1. 111In-7E11-C5
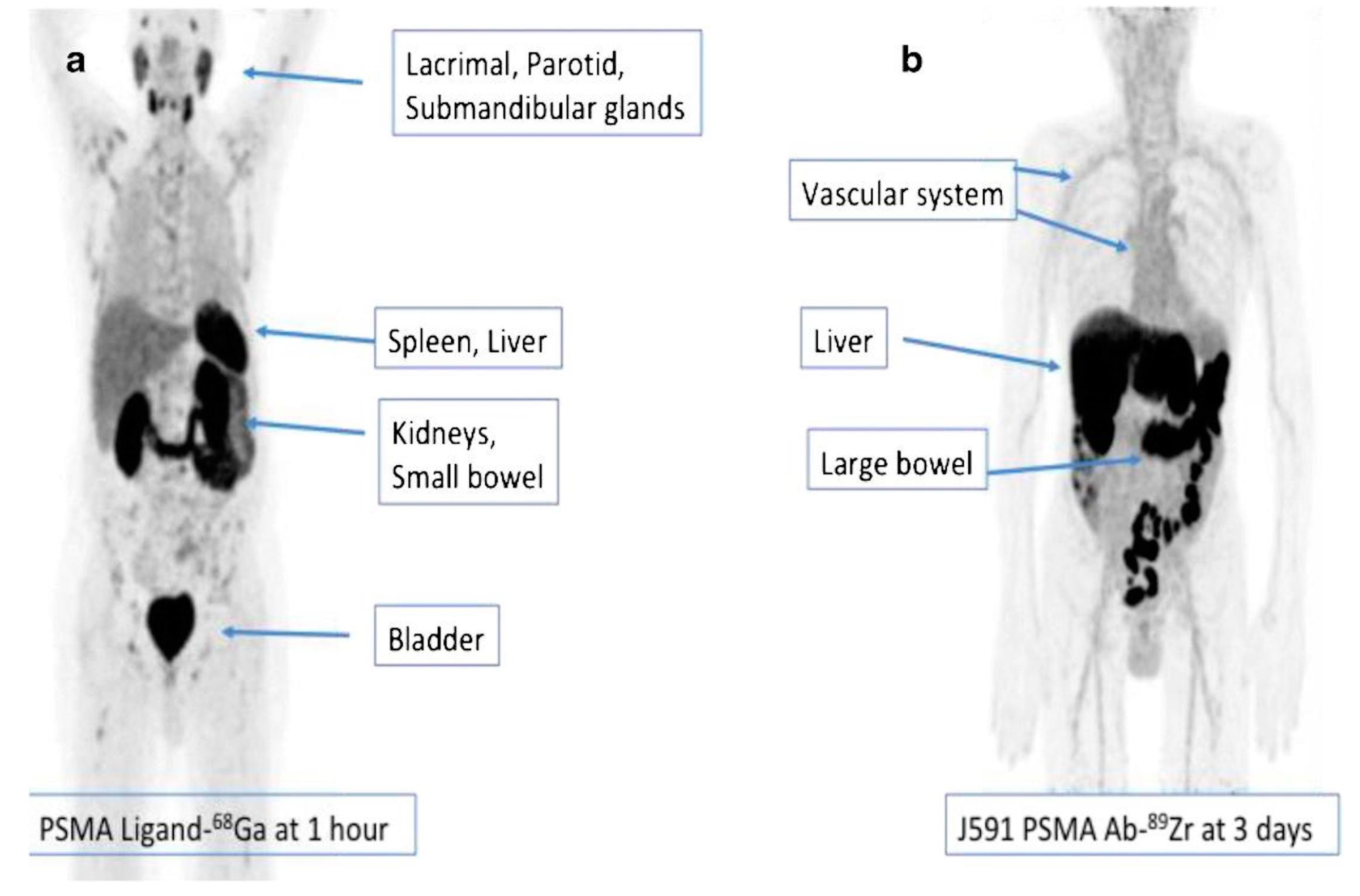
2.2. 89Zr-J591
2.3. 177Lu-J591
2.4. 117Lu-DOTA-TLX591
2.5. 64Cu-TLX592
2.6. 225Ac-J591
2.7. Comparison of Biodistribution of 177Lu-PSMA-617, 177Lu-J591, and 225Ac-J591
2.8. 227Th-PSMA-TTC
2.9. 225Ac-PSMA-TAC
3. Preclinical Studies and Future Directions
4. PSMA-Based mAbs vs. Small Molecular Ligands
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Allen, T.M. Ligand-targeted therapeutics in anticancer therapy. Nat. Rev. Cancer 2002, 2, 750–763. [Google Scholar] [CrossRef] [PubMed]
- Oriuchi, N.; Higuchi, T.; Hanaoka, H.; Iida, Y.; Endo, K. Current status of cancer therapy with radiolabeled monoclonal antibody. Ann. Nucl. Med. 2005, 19, 355–365. [Google Scholar] [CrossRef]
- Attarwala, H. Role of antibodies in cancer targeting. J. Nat. Sci. Biol. Med. 2010, 1, 53–56. [Google Scholar] [CrossRef]
- Yokota, T.; Milenic, D.E.; Whitlow, M.; Schlom, J. Rapid tumor penetration of a single-chain Fv and comparison with other immunoglobulin forms. Cancer Res. 1992, 52, 3402–3408. [Google Scholar] [PubMed]
- Saha, G.B. Diagnostic Uses of Radiopharmaceuticals in Nuclear Medicine. In Fundamentals of Nuclear Pharmacy; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Warram, J.M.; de Boer, E. Antibody-based imaging strategies for cancer. Cancer Metastasis Rev. 2014, 33, 809–822. [Google Scholar] [CrossRef] [PubMed]
- Pillai, M.R.A.; Nanabala, R.; Joy, A.; Sasikumar, A.; Knapp, F.F. Radiolabeled enzyme inhibitors and binding agents targeting PSMA: Effective theranostic tools for imaging and therapy of prostate cancer. Nucl. Med. Biol. 2016, 43, 692–720. [Google Scholar] [CrossRef]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Davis, M.I.; Bennett, M.J. Crystal structure of prostate-specific membrane antigen, a tumor marker and peptidase. Proc. Natl. Acad. Sci. USA 2005, 102, 5981–5986. [Google Scholar] [CrossRef]
- Ghosh, A.; Wang, X.; Klein, E.; Heston, W.D. Novel Role of Prostate-Specific Membrane Antigen in Suppressing Prostate Cancer Invasiveness. Cancer Res. 2005, 65, 727–731. [Google Scholar] [CrossRef]
- Luthi-Carter, R.; Barczak, A.K.; Speno, H.; Coyle, J.T. Molecular characterization of human brain N-acetylated alpha-linked acidic dipeptidase (NAALADase). J. Pharmacol. Exp. Ther. 1998, 286, 1020–1025. [Google Scholar]
- Pinto, J.T.; Suffoletto, B.P.; Berzin, T.; Qiao, C.H.; Lin, S.; Tong, W.P.; May, F.; Mukherjee, B.; Heston, W.D. Prostate-specific membrane antigen: A novel folate hydrolase in human prostatic carcinoma cells. Clin. Cancer Res. 1996, 2, 1445–1451. [Google Scholar] [PubMed]
- Chang, S.S. Overview of Prostate-Specific Membrane Antigen. Rev. Urol. 2004, 6 (Suppl. S10), S13–S18. [Google Scholar]
- Rajasekaran, S.A.; Anilkumar, G.; Oshima, E.; Bowie, J.U.; Liu, H.; Heston, W.; Bander, N.H.; Rajasekaran, A.K. A Novel Cytoplasmic Tail MXXXL Motif Mediates the Internalization of Prostate-specific Membrane Antigen. Mol. Biol. Cell 2003, 14, 4835–4845. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Udovicich, C.; Tran, B.; Zargar, H.; Murphy, D.G.; Hofman, M.S. Expanding the role of small-molecule PSMA ligands beyond PET staging of prostate cancer. Nat. Rev. Urol. 2020, 17, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Fendler, W.P.; Rowe, S.P.; Calais, J.; Hofman, M.S.; Maurer, T.; Schwarzenboeck, S.M.; Kratowchil, C.; Herrmann, K.; Giesel, F.L. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J. Nucl. Med. 2017, 58 (Suppl. S2), 67S–76S. [Google Scholar] [CrossRef]
- Wright, G.L., Jr.; Grob, B.M.; Haley, C.; Grossman, K.; Newhall, K.; Petrylak, D.; Troyer, J.; Konchuba, A.; Schellhammer, P.F.; Moriarty, R. Upregulation of prostate-specific membrane antigen after androgen-deprivation therapy. Urology 1996, 48, 326–334. [Google Scholar] [CrossRef]
- Ceci, F.; Fanti, S. PSMA-PET/CT imaging in prostate cancer: Why and when. Clin. Transl. Imaging 2019, 7, 377–379. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Udovicich, C.; Perera, M.; Hofman, M.S.; Siva, S.; Del Rio, A.; Murphy, D.G.; Lawrentschuk, N. 68 Ga-prostate-specific membrane antigen-positron emission tomography/computed tomography in advanced prostate cancer: Current state and future trends. Prostate Int. 2017, 5, 125–129. [Google Scholar] [CrossRef]
- Jindal, V. Immunotherapy: A glimmer of hope for metastatic prostate cancer. Chin. Clin. Oncol. 2018, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- Lawhn-Heath, C.; Salavati, A.; Behr, S.C.; Rowe, S.P.; Calais, J.; Fendler, W.P.; Eiber, M.; Emmett, L.; Hofman, M.S.; Hope, T.A. Prostate-specific Membrane Antigen PET in Prostate Cancer. Radiology 2021, 299, 248–260. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves 18F-rhPSMA-7.3 to Identify Prostate Cancer in PET Imaging. Available online: https://www.cancernetwork.com/view/fda-approves-18f-rhpsma-7-3-to-identify-prostate-cancer-in-pet-imaging (accessed on 30 May 2023).
- Hennrich, U.; Eder, M. [(177)Lu]Lu-PSMA-617 (Pluvicto(TM)): The First FDA-Approved Radiotherapeutical for Treatment of Prostate Cancer. Pharmaceuticals 2022, 15, 1292. [Google Scholar] [CrossRef]
- Zia, N.A.; Cullinane, C.; Van Zuylekom, J.K.; Waldeck, K.; McInnes, L.E.; Buncic, G.; Haskali, M.B.; Roselt, P.D.; Hicks, R.J.; Donnelly, P.S. A Bivalent Inhibitor of Prostate Specific Membrane Antigen Radiolabeled with Copper-64 with High Tumor Uptake and Retention. Angew. Chem. Int. Ed. 2019, 58, 14991–14994. [Google Scholar] [CrossRef] [PubMed]
- Szabo, Z.; Mena, E. Initial Evaluation of [(18)F]DCFPyL for Prostate-Specific Membrane Antigen (PSMA)-Targeted PET Imaging of Prostate Cancer. Mol. Imaging Biol. 2015, 17, 565–574. [Google Scholar] [CrossRef]
- Cho, S.Y.; Gage, K.L.; Mease, R.C.; Senthamizhchelvan, S.; Holt, D.P.; Jeffrey-Kwanisai, A.; Endres, C.J.; Dannals, R.F.; Sgouros, G.; Lodge, M.; et al. Biodistribution, Tumor Detection, and Radiation Dosimetry of 18F-DCFBC, a Low-Molecular-Weight Inhibitor of Prostate-Specific Membrane Antigen, in Patients with Metastatic Prostate Cancer. J. Nucl. Med. 2012, 53, 1883–1891. [Google Scholar] [CrossRef]
- Oh, S.W.; Wurzer, A. Quantitative and Qualitative Analyses of Biodistribution and PET Image Quality of a Novel Radiohybrid PSMA, (18)F-rhPSMA-7, in Patients with Prostate Cancer. J. Nucl. Med. 2020, 61, 702–709. [Google Scholar] [CrossRef]
- Tolvanen, T.; Kalliokoski, K. Safety, Biodistribution, and Radiation Dosimetry of (18)F-rhPSMA-7.3 in Healthy Adult Volunteers. J. Nucl. Med. 2021, 62, 679–684. [Google Scholar] [CrossRef]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef]
- Weineisen, M.; Schottelius, M.; Simecek, J.; Baum, R.P.; Yildiz, A.; Beykan, S.; Kulkarni, H.R.; Lassmann, M.; Klette, I.; Eiber, M.; et al. 68Ga- and 177Lu-Labeled PSMA I&T: Optimization of a PSMA-Targeted Theranostic Concept and First Proof-of-Concept Human Studies. J. Nucl. Med. 2015, 56, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Kurth, J.; Krause, B.J. External radiation exposure, excretion, and effective half-life in (177)Lu-PSMA-targeted therapies. EJNMMI Res. 2018, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Struthers, H.; Winiger, C.; Zhernosekov, K.; Schibli, R. DOTA Conjugate with an Albumin-Binding Entity Enables the First Folic Acid–Targeted 177Lu-Radionuclide Tumor Therapy in Mice. J. Nucl. Med. 2013, 54, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.S.; Zhang, M.; Meng, Y.G.; Kadkhodayan, M.; Kirchhofer, D.; Combs, D.; Damico, L.A. Albumin Binding as a General Strategy for Improving the Pharmacokinetics of Proteins. J. Biol. Chem. 2002, 277, 35035–35043. [Google Scholar] [CrossRef]
- Zang, J.; Liu, Q.; Sui, H.; Wang, R.; Jacobson, O.; Fan, X.; Zhu, Z.; Chen, X. 177Lu-EB-PSMA Radioligand Therapy with Escalating Doses in Patients with Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2020, 61, 1772–1778. [Google Scholar] [CrossRef]
- Zang, J.; Fan, X.; Wang, H.; Liu, Q.; Wang, J.; Li, H.; Li, F.; Jacobson, O.; Niu, G.; Zhu, Z.; et al. First-in-human study of 177Lu-EB-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. 2019, 46, 148–158. [Google Scholar] [CrossRef]
- Wang, Z.; Tian, R.; Niu, G.; Ma, Y.; Lang, L.; Szajek, L.P.; Kiesewetter, D.O.; Jacobson, O.; Chen, X. Single Low-Dose Injection of Evans Blue Modified PSMA-617 Radioligand Therapy Eliminates Prostate-Specific Membrane Antigen Positive Tumors. Bioconjugate Chem. 2018, 29, 3213–3221. [Google Scholar] [CrossRef]
- Miyahira, A.K.; Pienta, K.J.; Morris, M.J.; Bander, N.H.; Baum, R.P.; Fendler, W.P.; Goeckeler, W.; Gorin, M.A.; Hennekes, H.; Pomper, M.G.; et al. Meeting report from the Prostate Cancer Foundation PSMA-directed radionuclide scientific working group. Prostate 2018, 78, 775–789. [Google Scholar] [CrossRef]
- Lin, M.; Paolillo, V.; Le, D.B.; Macapinlac, H.; Ravizzini, G.C. Monoclonal antibody based radiopharmaceuticals for imaging and therapy. Curr. Probl. Cancer 2021, 45, 100796. [Google Scholar] [CrossRef]
- Kuo, L.J.; Yang, L.-X. Gamma-H2AX—A novel biomarker for DNA double-strand breaks. In Vivo 2008, 22, 305–309. [Google Scholar]
- Manyak, M.J.; Hinkle, G.H.; Olsen, J.O.; Chiaccherini, R.P.; Partin, A.W.; Piantadosi, S.; Burgers, J.K.; Texter, J.H.; Neal, C.E.; Libertino, J.A.; et al. Immunoscintigraphy with indium-111-capromab pendetide: Evaluation before definitive therapy in patients with prostate cancer. Urology 1999, 54, 1058–1063. [Google Scholar] [CrossRef]
- Taneja, S.S. Imaging in the diagnosis and management of prostate cancer. Rev. Urol. 2004, 6, 101–113. [Google Scholar] [PubMed]
- Lamb, H.M.; Faulds, D. Capromab pendetide. A review of its use as an imaging agent in prostate cancer. Drugs Aging 1998, 12, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Elgamal, A.A.; Troychak, M.J. ProstaScint scan may enhance identification of prostate cancer recurrences after prostatectomy, radiation, or hormone therapy: Analysis of 136 scans of 100 patients. Prostate 1998, 37, 261–269. [Google Scholar] [CrossRef]
- Taneja, S.S. ProstaScint(R) Scan: Contemporary Use in Clinical Practice. Rev. Urol. 2004, 6 (Suppl. S10), S19–S28. [Google Scholar]
- Wilkinson, S.; Chodak, G. The Role of 111 Indium-Capromab Pendetide Imaging for Assessing Biochemical Failure after Radical Prostatectomy. J. Urol. 2004, 172, 133–136. [Google Scholar] [CrossRef] [PubMed]
- EUSA Pharma (USA). Inc ProstaScint® Kit (Capromab Pendetide) [Package Insert]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/103608s5043lbl.pdf (accessed on 21 June 2023).
- Jetty, S.; Loftus, J.R. Prostate Cancer-PET Imaging Update. Cancers 2023, 15, 796. [Google Scholar] [CrossRef]
- Bander, N.H.; Trabulsi, E.J. Targeting metastatic prostate cancer with radiolabeled monoclonal antibody J591 to the extra-cellular domain of prostate specific membrane antigen. J. Urol. 2003, 170, 1717–1721. [Google Scholar] [CrossRef]
- Osborne, J.R.; Akhtar, N.H.; Vallabhajosula, S.; Anand, A.; Deh, K.; Tagawa, S.T. Prostate-specific membrane antigen-based imaging. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 144–154. [Google Scholar] [CrossRef]
- Vallabhajosula, S.; Kuji, I. Pharmacokinetics and biodistribution of 111In- and 177Lu-labeled J591 antibody specific for prostate-specific membrane antigen: Prediction of 90Y-J591 radiation dosimetry based on 111In or 177Lu? J. Nucl. Med. 2005, 46, 634–641. [Google Scholar]
- Osborne, J.R.; Green, D.A. A prospective pilot study of (89)Zr-J591/prostate specific membrane antigen positron emission tomography in men with localized prostate cancer undergoing radical prostatectomy. J. Urol. 2014, 191, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Tagawa, S.T.; Milowsky, M.I. Phase II study of Lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 for metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2013, 19, 5182–5191. [Google Scholar] [CrossRef] [PubMed]
- Pandit-Taskar, N.; O’Donoghue, J.A. (8)(9)Zr-huJ591 immuno-PET imaging in patients with advanced metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2093–2105. [Google Scholar] [CrossRef] [PubMed]
- Pandit-Taskar, N.; O’Donoghue, J.A. A Phase I/II Study for Analytic Validation of 89Zr-J591 ImmunoPET as a Molecular Im-aging Agent for Metastatic Prostate Cancer. Clin Cancer Res. 2015, 21, 5277–5285. [Google Scholar] [CrossRef]
- Cornelis, F.H.; Durack, J.C.; Pandit-Taskar, N.; Ulaner, G.A.; Lewis, J.S.; Morris, M.J.; Solomon, S.B. Long–Half-Life 89Zr-Labeled Radiotracers Can Guide Percutaneous Biopsy within the PET/CT Suite without Reinjection of Radiotracer. J. Nucl. Med. 2018, 59, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Pandit-Taskar, N.; O’Donoghue, J.A. First-in-Human Imaging with 89Zr-Df-IAB2M Anti-PSMA Minibody in Patients with Metastatic Prostate Cancer: Pharmacokinetics, Biodistribution, Dosimetry, and Lesion Uptake. J. Nucl. Med. 2016, 57, 1858–1864. [Google Scholar] [CrossRef]
- Donin, N.M.; Reiter, R.E. Why Targeting PSMA Is a Game Changer in the Management of Prostate Cancer. J. Nucl. Med. 2018, 59, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Niaz, M.J.; Tagawa, S.T. Prostate-Specific Membrane Antigen (PSMA)-Targeted Radionuclide Therapies for Prostate Cancer. Curr. Oncol. Rep. 2021, 23, 59. [Google Scholar] [CrossRef]
- Das, T.; Banerjee, S. Theranostic Applications of Lutetium-177 in Radionuclide Therapy. Curr. Radiopharm. 2016, 9, 94–101. [Google Scholar] [CrossRef]
- Bander, N.H.; Milowsky, M.I.; Nanus, D.M.; Kostakoglu, L.; Vallabhajosula, S.; Goldsmith, S.J. Phase I Trial of 177Lutetium-Labeled J591, a Monoclonal Antibody to Prostate-Specific Membrane Antigen, in Patients with Androgen-Independent Prostate Cancer. J. Clin. Oncol. 2005, 23, 4591–4601. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Vallabhajosula, S. Phase 1/2 study of fractionated dose lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 ((177) Lu-J591) for metastatic castration-resistant prostate cancer. Cancer 2019, 125, 2561–2569. [Google Scholar] [CrossRef]
- 177Lu-DOTA-TLX591 Safety, Biodistribution and Dosimetry Study (ProstACTSelect). 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04786847 (accessed on 9 May 2023).
- 177Lu-DOTA-rosopatamab with Best Standard of Care (SoC) for the Second Line of Treatment for Metastatic Castrate-Resistant Prostate Cancer, Which Expresses PSMA (PROSTACT). 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04876651 (accessed on 9 May 2023).
- CUPID. First Patient Dosed in CUPID Study of Telix’s Targeted Alpha Therapy Candidate for Prostate Cancer. 2023. Available online: https://telixpharma.com/news-views/first-patient-dosed-in-cupid-study-of-telixs-targeted-alpha-therapy-candidate-for-prostate-cancer/ (accessed on 9 May 2023).
- Tagawa, S.T.; Sun, M.; Sartor, A.O.; Thomas, C.; Singh, S.; Bissassar, M.; Fernandez, E.; Niaz, M.J.; Ho, B.; Vallabhajosula, S.; et al. Phase I study of 225Ac-J591 for men with metastatic castration-resistant prostate cancer (mCRPC). J. Clin. Oncol. 2021, 39, 5015. [Google Scholar] [CrossRef]
- Nauseef, W.M.; Castellanos, S. Phase I results of a phase I/II trial of pembrolizumab and AR signaling inhibitor (ARSI) +/− 225Ac-J591 for chemo-naïve metastatic castration-resistant prostate cancer (mCRPC). In Proceedings of the Society for Urologic Oncology (SUO) 23rd Annual Meeting, San Diego, CA, USA, 30 November–2 December 2022. Poster 76. [Google Scholar]
- Fractionated and Multiple Dose 225Ac-J591 for Progressive mCRPC. Available online: https://clinicaltrials.gov/ct2/show/NCT04506567 (accessed on 9 May 2023).
- Kratochwil, C.; Bruchertseifer, F. 225Ac-PSMA-617 for PSMA-Targeted alpha-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef]
- Bander, N.H. Bander on Preliminary Data on 225Ac-J591 Plus Pembrolizumab in mCRPC. 2023. Available online: https://www.onclive.com/view/dr-bander-on-preliminary-data-on-225ac-j591-plus-pembrolizumab-in-mcrpc (accessed on 16 May 2023).
- ClinicalTrials. Maximizing Responses to Anti-PD1 Immunotherapy with PSMA-targeted Alpha Therapy in mCRPC. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04946370 (accessed on 16 May 2023).
- AUA 2020: Comparison of Prostate-Specific Membrane Antigen-Targeted Radionuclide Therapy with Lutetium-177 via An-tibody J591 vs. Small Molecule Ligand PSMA-617. Available online: https://www.urotoday.com/conference-highlights/aua-2020/aua-2020-prostate-cancer/122691-aua-2020-comparison-of-prostate-specific-membrane-antigen-targeted-radionuclide-therapy-with-lutetium-177-via-antibody-j591-vs-small-molecule-ligand-psma-617.html (accessed on 20 June 2023).
- Label for PLUVICTOTM (Lutetium Lu 177 Vipivotide Tetraxetan) Injection. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=215833 (accessed on 20 June 2023).
- Sartor, O.; de Bono, J. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Nauseef, W.M.; Sun, M.P. A phase I/II dose-escalation study of fractionated 225Ac-J591 for progressive metastatic castration-resistant prostate cancer (mCRPC) in patients with prior treatment with 177Lu-PSMA. J. Clin. Oncol. 2023, 41, 6. [Google Scholar] [CrossRef]
- Nauseef, W.M.; Sun, M. Abstract CT014: Phase I dose-escalation study of fractionated dose 225Ac J591 for metastatic castration resistant prostate cancer. Cancer Res. 2023, 83 (Suppl. S8). CT014. [Google Scholar] [CrossRef]
- Hammer, S.; Hagemann, U.B.; Zitzmann-Kolbe, S.; Larsen, A.; Ellingsen, C.; Geraudie, S.; Grant, D.; Indrevoll, B.; Smeets, R.; von Ahsen, O.; et al. Preclinical Efficacy of a PSMA-Targeted Thorium-227 Conjugate (PSMA-TTC), a Targeted Alpha Therapy for Prostate Cancer. Clin. Cancer Res. 2020, 26, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Study to Evaluate the Safety, Tolerability, Pharmacokinetics, and Antitumor Activity of a Thorium-227 Labeled Antibody-Chelator Conjugate Alone and in Combination with Darolutamide, in Patients with Metastatic Castration Resistant Prostate Cancer. 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03724747 (accessed on 9 May 2023).
- Schatz, C.; Zitzmann-Kolbe, S. Preclinical efficacy of a PSMA-targeted actinium-225 conjugate (225Ac-pelgifatamab) a targeted alpha therapy for prostate cancer. In Proceedings of the EANM Barcelona, Barcelona, Spain, 15–19 October 2022. [Google Scholar]
- Su, Y.; Liu, Y.; Behrens, C.R.; Bidlingmaier, S.; Lee, N.-K.; Aggarwal, R.; Sherbenou, D.W.; Burlingame, A.L.; Hann, B.C.; Simko, J.P.; et al. Targeting CD46 for both adenocarcinoma and neuroendocrine prostate cancer. J. Clin. Investig. 2018, 3, 4640–4653. [Google Scholar] [CrossRef]
- Sherbenou, D.W.; Aftab, B.T.; Su, Y.; Behrens, C.R.; Wiita, A.; Logan, A.C.; Acosta-Alvear, D.; Hann, B.C.; Walter, P.; Shuman, M.A.; et al. Antibody-drug conjugate targeting CD46 eliminates multiple myeloma cells. J. Clin. Investig. 2016, 126, 4640–4653. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, T.; Hua, J.; Wang, Q.; Su, Y.; Chen, P.; Bidlingmaier, S.; Li, A.; Xie, Z.; Bidkar, A.P.; et al. CD46 targeted 212Pb alpha particle radioimmunotherapy for prostate cancer treatment. J. Exp. Clin. Cancer Res. 2023, 42, 61. [Google Scholar] [CrossRef] [PubMed]
- Bidkar, A.P.; Wang, S.; Bobba, K.N.; Chan, E.; Bidlingmaier, S.; Egusa, E.A.; Peter, R.; Ali, U.; Meher, N.; Wadhwa, A.; et al. Treatment of Prostate Cancer with CD46-targeted 225Ac Alpha Particle Radioimmunotherapy. Clin. Cancer Res. 2023, 29, 1916–1928. [Google Scholar] [CrossRef] [PubMed]
- Mazzocco, C.; Fracasso, G.; Germain-Genevois, C.; Dugot-Senant, N.; Figini, M.; Colombatti, M.; Grenier, N.; Couillaud, F. In vivo imaging of prostate cancer using an anti-PSMA scFv fragment as a probe. Sci. Rep. 2016, 6, 23314. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, B.; Fracasso, G.; Luison, E.; Cingarlini, S.; Mortarino, M.; Coliva, A.; Seregni, E.; Bombardieri, E.; Zuccolotto, G.; Rosato, A.; et al. A single-chain fragment against prostate specific membrane antigen as a tool to build theranostic reagents for prostate cancer. Eur. J. Cancer 2013, 49, 2223–2232. [Google Scholar] [CrossRef] [PubMed]
- Wester, H.-J.; Schottelius, M. PSMA-Targeted Radiopharmaceuticals for Imaging and Therapy. Semin. Nucl. Med. 2019, 49, 302–312. [Google Scholar] [CrossRef]
- Barrett, J.A.; Coleman, R.E.; Goldsmith, S.J.; Vallabhajosula, S.; Petry, N.A.; Cho, S.; Armor, T.; Stubbs, J.B.; Maresca, K.P.; Stabin, M.G.; et al. First-in-Man Evaluation of 2 High-Affinity PSMA-Avid Small Molecules for Imaging Prostate Cancer. J. Nucl. Med. 2013, 54, 380–387. [Google Scholar] [CrossRef]
- Zechmann, C.M.; Afshar-Oromieh, A. Radiation dosimetry and first therapy results with a (124)I/ (131)I-labeled small mol-ecule (MIP-1095) targeting PSMA for prostate cancer therapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1280–1292. [Google Scholar] [CrossRef]
- dos Santos, J.C.; Beijer, B.; Bauder-Wüst, U.; Schäfer, M.; Leotta, K.; Eder, M.; Benešová, M.; Kleist, C.; Giesel, F.; Kratochwil, C.; et al. Development of Novel PSMA Ligands for Imaging and Therapy with Copper Isotopes. J. Nucl. Med. 2020, 61, 70–79. [Google Scholar] [CrossRef]
- McInnes, L.E.; Cullinane, C.; Roselt, P.D.; Jackson, S.; Blyth, B.J.; van Dam, E.M.; Zia, N.A.; Harris, M.J.; Hicks, R.J.; Donnelly, P.S. Therapeutic Efficacy of a Bivalent Inhibitor of Prostate-Specific Membrane Antigen Labeled with 67Cu. J. Nucl. Med. 2021, 62, 829–832. [Google Scholar] [CrossRef]
- Banerjee, S.R.; Pullambhatla, M.; Foss, C.A.; Nimmagadda, S.; Ferdani, R.; Anderson, C.J.; Mease, R.C.; Pomper, M.G. 64Cu-Labeled Inhibitors of Prostate-Specific Membrane Antigen for PET Imaging of Prostate Cancer. J. Med. Chem. 2014, 57, 2657–2669. [Google Scholar] [CrossRef]
- Hicks, R.J.; Jackson, P. (64)Cu-SARTATE PET Imaging of Patients with Neuroendocrine Tumors Demonstrates High Tumor Uptake and Retention, Potentially Allowing Prospective Dosimetry for Peptide Receptor Radionuclide Therapy. J. Nucl. Med. 2019, 60, 777–785. [Google Scholar] [CrossRef]
- Ma, M.T.; Cooper, M.S.; Paul, R.L.; Shaw, K.P.; Karas, J.A.; Scanlon, D.; White, J.M.; Blower, P.J.; Donnelly, P.S. Macrobicyclic Cage Amine Ligands for Copper Radiopharmaceuticals: A Single Bivalent Cage Amine Containing Two Lys3-bombesin Targeting Peptides. Inorg. Chem. 2011, 50, 6701–6710. [Google Scholar] [CrossRef] [PubMed]
- Neels, O.C.; Kopka, K.; Liolios, C.; Afshar-Oromieh, A. Radiolabeled PSMA Inhibitors. Cancers 2021, 13, 6255. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radioligand Radiolabeled mAbs | Half-Life | Emission α Particle | Max β+/− or Energy (MeV) | Max γ Particle Energy (MeV) | Clinical Use | ClinicalTrials.gov Identifier |
|---|---|---|---|---|---|---|
| 64Cu-TLX592 | 12.7 | AE, β+ | 0.653 | 1.346 | Auger therapy, PET | NCT04726033 |
| 64Cu-CuSarbisPSMA | Pre-clinical only | |||||
| 89Zr-Df-IAb2M | 78.4 h | β | 0.909 | PET | NCT02349022 | |
| 89Zr-J591 | NCT01543659 | |||||
| 111In-7E11 | 8 d | AE, γ | 0.171; 0.245 | Auger therapy, SPECT | NCT02349022, NCT00992745 | |
| 177Lu-J591 - | 6.7 d | AE, β−, γ | 0.177; 0.385; 0.5 | 0.208 | Auger therapy, β therapy, SPECT | NCT00195039, NCT00538668 |
| 177Lu-DOTA-TLX591 | NCT04786847, NCT04876651 | |||||
| 212Pb-TCMC-YS5 | 10.6 h | β− | β therapy (daughter α) | NCT05245006 | ||
| 225Ac-J591 | 10.0 d | α | 5.6-5.793 | α therapy (daughter β, SPECT) | NCT03276572, NCT04506567, NCT04946370 | |
| 225Ac-PSMA-TAC | NCT05219500 | |||||
| 225Ac-DOTA-YS5 | Pre-clinical only | |||||
| 227Th-PSMA-TTC | 18.7 d | α | 5.9 | α therapy | NCT03724747 | |
| Probe for fluorescence imaging | ||||||
| X770-scFvD2B | Fluorescent scFv of the anti-PSMA antibody | Pre-clinical only |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abusalem, M.; Martiniova, L.; Soebianto, S.; DePalatis, L.; Ravizzini, G. Current Status of Radiolabeled Monoclonal Antibodies Targeting PSMA for Imaging and Therapy. Cancers 2023, 15, 4537. https://doi.org/10.3390/cancers15184537
Abusalem M, Martiniova L, Soebianto S, DePalatis L, Ravizzini G. Current Status of Radiolabeled Monoclonal Antibodies Targeting PSMA for Imaging and Therapy. Cancers. 2023; 15(18):4537. https://doi.org/10.3390/cancers15184537
Chicago/Turabian StyleAbusalem, Mohammed, Lucia Martiniova, Sarita Soebianto, Louis DePalatis, and Gregory Ravizzini. 2023. "Current Status of Radiolabeled Monoclonal Antibodies Targeting PSMA for Imaging and Therapy" Cancers 15, no. 18: 4537. https://doi.org/10.3390/cancers15184537
APA StyleAbusalem, M., Martiniova, L., Soebianto, S., DePalatis, L., & Ravizzini, G. (2023). Current Status of Radiolabeled Monoclonal Antibodies Targeting PSMA for Imaging and Therapy. Cancers, 15(18), 4537. https://doi.org/10.3390/cancers15184537