

A Review of Margetuximab-Based Therapies in Patients with HER2-Positive Metastatic Breast Cancer

Abstract
Simple Summary
Abstract
1. Introduction
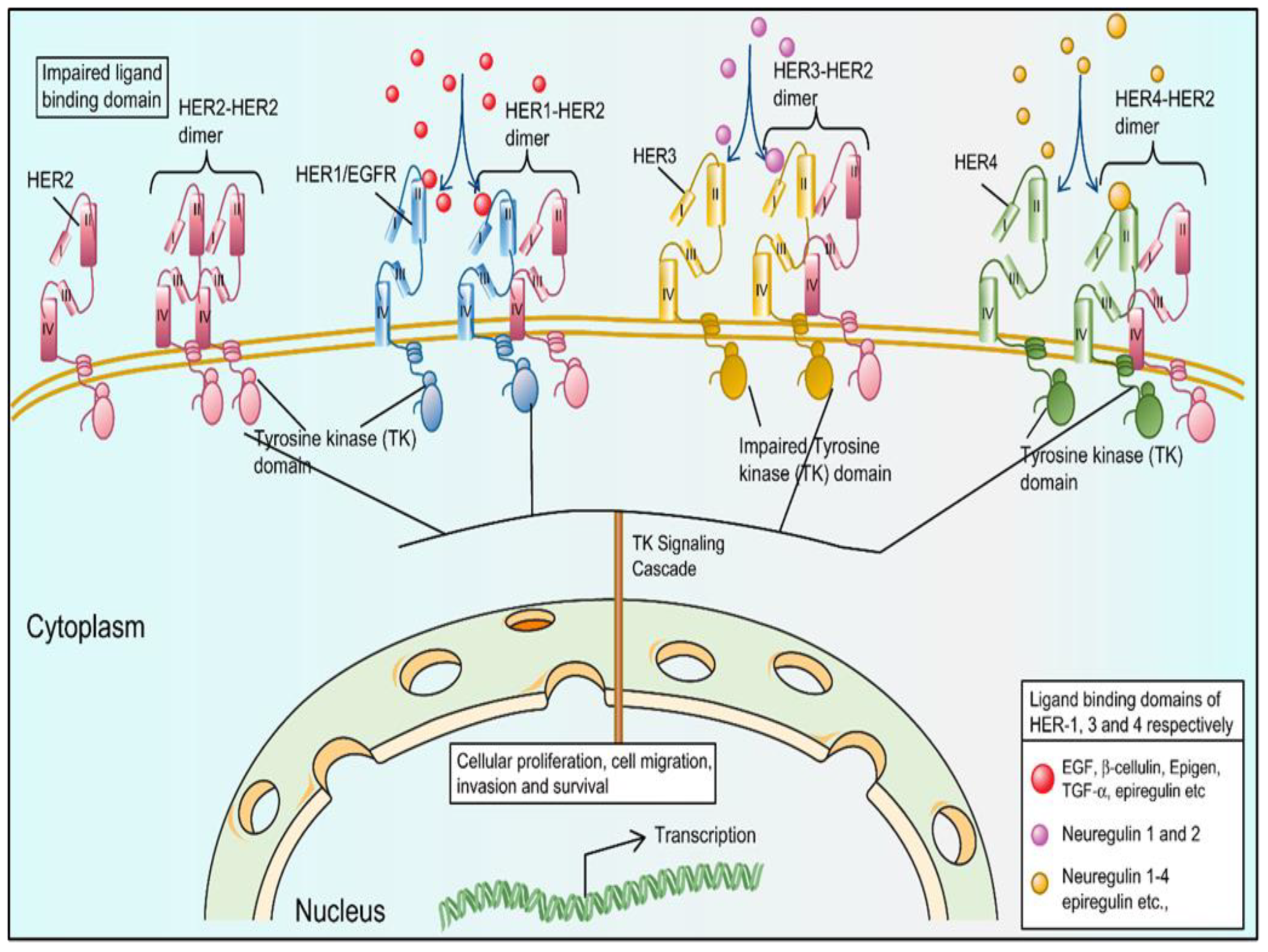
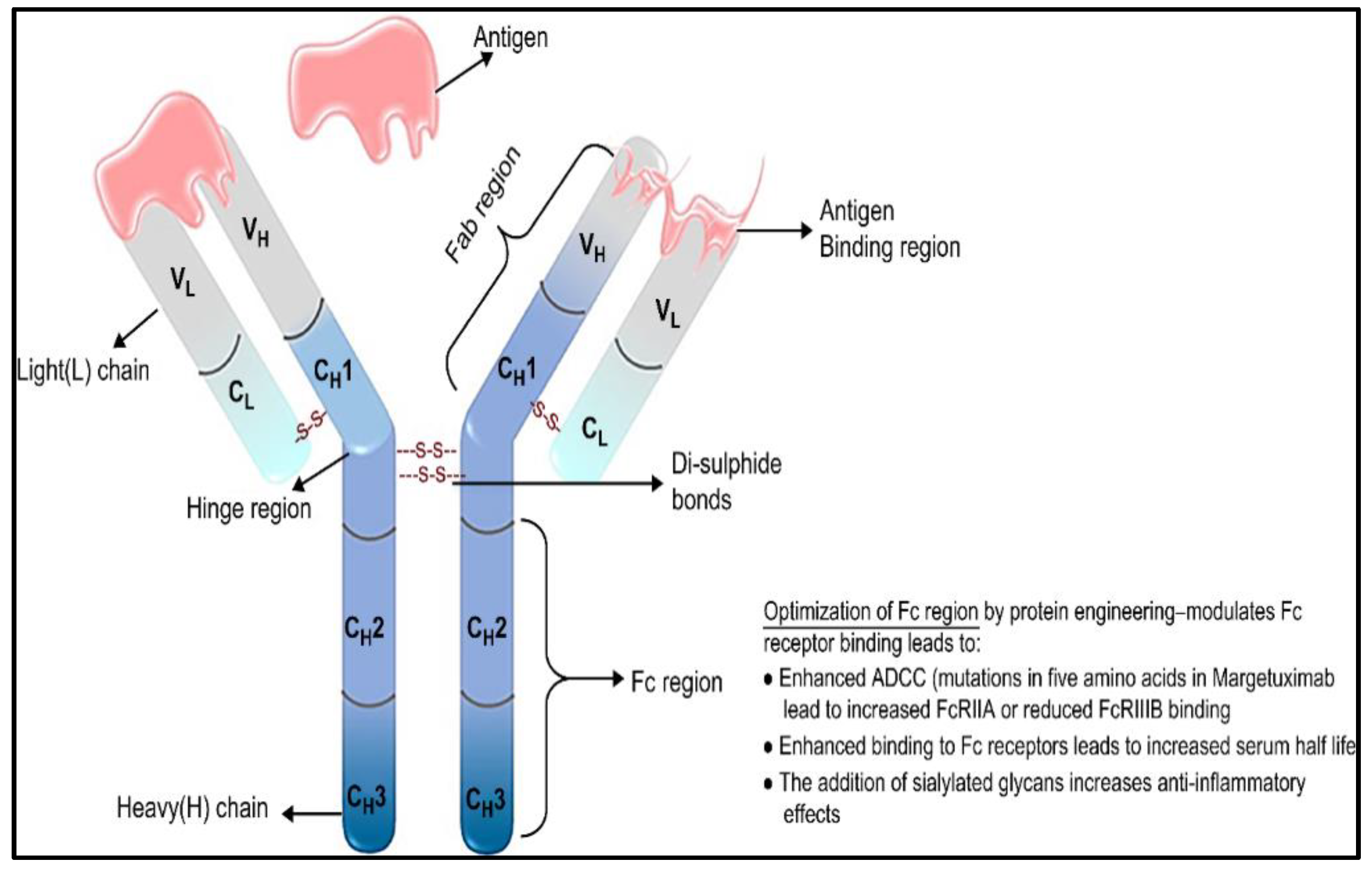
2. Structural Biology of HER-Family Receptors
3. Unique Characteristics of HER2 Promote Tumor Progression in BC
4. Existing Anti-HER2 Therapies for HER2 + BC
5. Current Insights on Margetuximab, a Novel Anti-HER2 Drug for Treatment of Positive Metastatic Breast Cancer
6. Pharmacology of Margetuximab
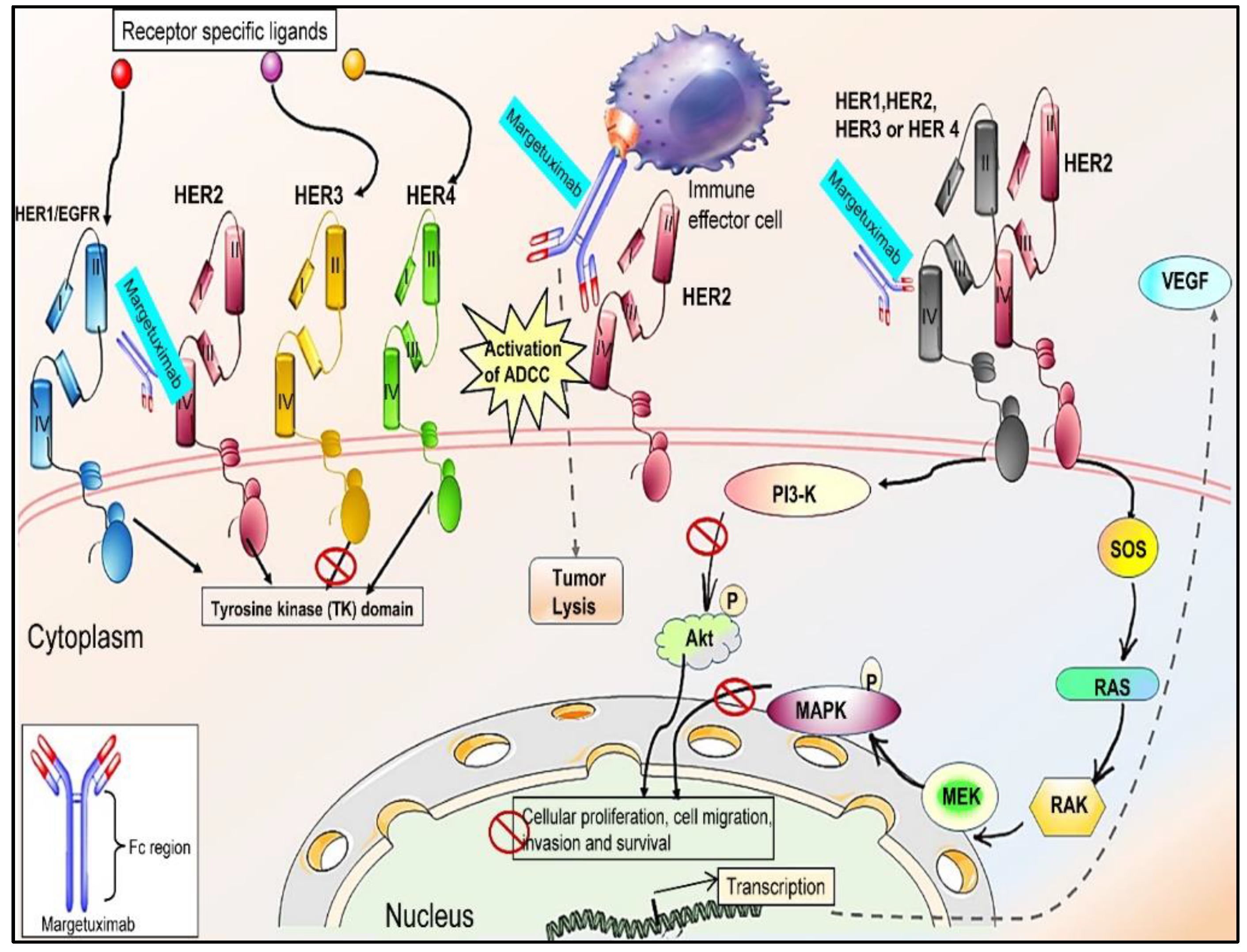
6.1. Mechanism of Action
6.2. Pharmacokinetic Properties
6.3. Indications/Therapeutic Use
6.4. Tolerability and Toxicity
6.5. Dosage and Administration
6.6. Clinical Trials of Margetuximab in BC
7. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Turashvili, G.; Brogi, E. Tumor heterogeneity in breast cancer. Front. Med. 2017, 4, 227. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, B. Targeted therapeutic options and future perspectives for HER2-positive breast cancer. Signal Transduct. Target. Ther. 2019, 4, 34. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.W.S.; Wu, M.; Cho, W.C.S.; To, K.K.W. Recent Advances in the Treatment of Breast Cancer. Front. Oncol. 2018, 8, 227. [Google Scholar] [CrossRef]
- Pashayan, N.; Antoniou, A.C.; Ivanus, U.; Esserman, L.J.; Easton, D.F.; French, D.; Sroczynski, G.; Hall, P.; Cuzick, J.; Evans, D.G.; et al. Personalized early detection and prevention of breast cancer: ENVISION consensus statement. Nat. Rev. Clin. Oncol. 2020, 17, 687–705. [Google Scholar] [CrossRef]
- Schettini, F.; Pascual, T.; Conte, B.; Chic, N.; Brasó-Maristany, F.; Galván, P.; Martínez, O.; Adamo, B.; Vidal, M.; Muñoz, M.; et al. HER2-enriched subtype and pathological complete response in HER2-positive breast cancer: A systematic review and meta-analysis. Cancer Treat. Rev. 2020, 84, 101965. [Google Scholar] [CrossRef]
- English, D.P.; Roque, D.M.; Santin, A.D. HER2 Expression Beyond Breast Cancer: Therapeutic Implications for Gynecologic Malignancies. Mol. Diagn. Ther. 2013, 17, 85–99. [Google Scholar] [CrossRef]
- Wahdan-Alaswad, R.; Liu, B.; Thor, A.D. Targeted lapatinib anti-HER2/ErbB2 therapy resistance in breast cancer: Opportunities to overcome a difficult problem. Cancer Drug Resist 2020, 3, 179–198. [Google Scholar] [CrossRef]
- Zielińska, M.; Zarankiewicz, N.; Kosz, K.; Kuchnicka, A.; Ciseł, B. HER2-positive breast cancer—Available anti-HER2 therapies and new agents under investigation. J. Pre-Clin. Clin. Res. 2020, 14, 44–48. [Google Scholar] [CrossRef]
- Peyvandi, S.; Lan, Q.; Lorusso, G. Chemotherapy-induced immunological breast cancer dormancy: A new function for old drugs? J. Cancer Metastasis Treat. 2019, 5, 44. [Google Scholar] [CrossRef][Green Version]
- Griguolo, G.; Pascual, T.; Dieci, M.V.; Guarneri, V.; Prat, A. Interaction of host immunity with HER2-targeted treatment and tumor heterogeneity in HER2-positive breast cancer. J. Immunother. Cancer 2019, 7, 90. [Google Scholar] [CrossRef] [PubMed]
- Gote, V.; Nookala, A.; Bolla, P.; Pal, D. Drug Resistance in Metastatic Breast Cancer: Tumor Targeted Nanomedicine to the Rescue. Int. J. Mol. Sci. 2021, 22, 4673. [Google Scholar] [CrossRef] [PubMed]
- Mezni, E.; Vicier, C.; Guerin, M.; Sabatier, R.; Bertucci, F.; Gonçalves, A. New Therapeutics in HER2-Positive Advanced Breast Cancer: Towards a Change in Clinical Practices? Cancers 2020, 12, 1573. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; De Gregorio, N.; Widschwendter, P.; Fink, V.; Huober, J. Targeted Therapies in HER2-Positive Breast Cancer—A Systematic Review. Breast Care 2015, 10, 173–178. [Google Scholar] [CrossRef]
- Li, S.G.; Li, L. Targeted therapy in HER2-positive breast cancer. Biomed. Rep. 2013, 1, 499–505. [Google Scholar] [CrossRef]
- Iqbal, N.; Iqbal, N. Human epidermal growth factor receptor 2 (HER2) in cancers: Overexpression and therapeutic implications. Mol. Biol. Int. 2014, 2014, 852748. [Google Scholar] [CrossRef]
- Marchini, C.; Lucia, P.; Cristina, K.; Chiara, G.; Federico, G.; Elena, Q.; Manuela, I.; Serenella, M.P.; Elda, T.; Augusto, A. Her2-driven carcinogenesis: New mouse models for novel immunotherapies. In Oncogene and Cancer-From Bench to Clinic; IntechOpen: London, UK, 2013. [Google Scholar]
- Ferreira, P.M.P.; Pessoa, C. Molecular biology of human epidermal receptors, signaling pathways and targeted therapy against cancers: New evidences and old challenges. Braz. J. Pharm. Sci. 2017, 53, e16076. [Google Scholar] [CrossRef]
- Kiyatkin, A.; Rosenburgh, I.K.V.A.V.; Klein, D.E.; Lemmon, M.A. Kinetics of receptor tyrosine kinase activation define ERK signaling dynamics. Sci. Signal. 2020, 13, 1. [Google Scholar] [CrossRef]
- Maruyama, I.N. Mechanisms of Activation of Receptor Tyrosine Kinases: Monomers or Dimers. Cells 2014, 3, 304–330. [Google Scholar] [CrossRef]
- Ross, J.S.; Fletcher, J.A.; Linette, G.P.; Stec, J.; Clark, E.; Ayers, M.; Bloom, K.J. The Her-2/neu gene and protein in breast cancer 2003: Biomarker and target of therapy. Oncologist 2003, 8, 307–325. [Google Scholar] [CrossRef]
- Fichter, C.D.; Przypadlo, C.M.; Buck, A.; Herbener, N.; Riedel, B.; Schäfer, L.; Nakagawa, H.; Walch, A.; Reinheckel, T.; Werner, M.; et al. A new model system identifies epidermal growth factor receptor-human epidermal growth factor receptor 2 (HER2) and HER2-human epidermal growth factor receptor 3 heterodimers as potent inducers of oesophageal epithelial cell invasion. J. Pathol. 2017, 243, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Wee, P.; Wang, Z. Epidermal Growth Factor Receptor Cell Proliferation Signaling Pathways. Cancers 2017, 9, 52. [Google Scholar] [CrossRef] [PubMed]
- Roskoski, R., Jr. The ErbB/HER family of protein-tyrosine kinases and cancer. Pharmacol. Res. 2014, 79, 34–74. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z. ErbB Receptors and Cancer. In ErbB Receptor Signaling; Humana Press: New York, NY, USA, 2017; Volume 1652, pp. 3–35. [Google Scholar] [CrossRef]
- Brandão, M.; Aftimos, P.; Azim, H.A.; Sotiriou, C. Molecular biology of breast cancer. In Essential Concepts in Molecular Pathology, 2nd ed.; Tsongalis, G.J., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 449–461. [Google Scholar]
- Inoue, K.; Fry, E.A. Aberrant Splicing of Estrogen Receptor, HER2, and CD44 Genes in Breast Cancer. Genet. Epigenetics 2015, 7, 19–32. [Google Scholar] [CrossRef]
- Ruiz, I.R.; Vicario, R.; Morancho, B.; Morales, C.B.; Arenas, E.J.; Herter, S.; Freimoser-Grundschober, A.; Somandin, J.; Sam, J.; Ast, O.; et al. p95HER2–T cell bispecific antibody for breast cancer treatment. Sci. Transl. Med. 2018, 10, eaat1445. [Google Scholar] [CrossRef]
- Arribas, J.; Baselga, J.; Pedersen, K.; Parra-Palau, J.L. p95HER2 and Breast Cancer: Figure 1. Cancer Res. 2011, 71, 1515–1519. [Google Scholar] [CrossRef]
- Gutierrez, C.; Schiff, R. HER2: Biology, Detection, and Clinical Implications. Arch. Pathol. Lab. Med. 2011, 135, 55–62. [Google Scholar] [CrossRef]
- Hudis, C.A. Trastuzumab–Mechanism of Action and Use in Clinical Practice. N. Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef]
- Zardavas, D.; Pugliano, L.; Ades, F.; Bozovic-Spasojevic, I.; Capelan, M.; de Azambuja, E. Targeted treatments of HER2-positive metastatic breast cancer: Trastuzumab and beyond. Breast Cancer Manag. 2012, 1, 217–233. [Google Scholar] [CrossRef]
- Burris, H.A.; Hurwitz, H.I.; Dees, E.C.; Dowlati, A.; Blackwell, K.L.; O’Neil, B.; Marcom, P.K.; Ellis, M.J.; Overmoyer, B.; Jones, S.F.; et al. Phase I Safety, Pharmacokinetics, and Clinical Activity Study of Lapatinib (GW572016), a Reversible Dual Inhibitor of Epidermal Growth Factor Receptor Tyrosine Kinases, in Heavily Pretreated Patients with Metastatic Carcinomas. J. Clin. Oncol. 2005, 23, 5305–5313. [Google Scholar] [CrossRef]
- Dai, C.; Ma, S.; Wang, F.; Zhao, H.; Wu, X.; Huang, Z.; Chen, Z.-S.; To, K.; Fu, L. Lapatinib promotes the incidence of hepatotoxicity by increasing chemotherapeutic agent accumulation in hepatocytes. Oncotarget 2015, 6, 17738–17752. [Google Scholar] [CrossRef]
- Moon, J.Y.; Han, J.M.; Seo, I.; Gwak, H.S. Risk factors associated with the incidence and time to onset of lapatinib-induced hepatotoxicity. Breast Cancer Res. Treat. 2019, 178, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Bates, J.S. Pertuzumab in Metastatic Breast Cancer. J. Adv. Pract. Oncol. 2012, 3, 391. [Google Scholar] [CrossRef] [PubMed]
- Royce, M.; Herold, K. New Agents for the Management of Advanced HER2-Positive Breast Cancer. J. Adv. Pract. Oncol. 2016, 7, 295–298. [Google Scholar] [PubMed]
- Krop, I.; Winer, E.P. Trastuzumab Emtansine: A Novel Antibody–Drug Conjugate for HER2-Positive Breast Cancer. Clin. Cancer Res. 2014, 20, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, S. Trastuzumab Emtansine: A Review of Its Use in Patients with HER2-Positive Advanced Breast Cancer Previously Treated with Trastuzumab-Based Therapy. Drugs 2014, 74, 675–686. [Google Scholar] [CrossRef]
- Gharwan, H.; Groninger, H. Kinase inhibitors and monoclonal antibodies in oncology: Clinical implications. Nat. Rev. Clin. Oncol. 2015, 13, 209–227. [Google Scholar] [CrossRef]
- Ho, G.-F.; Chai, C.-S.; Alip, A.; Wahid, M.I.A.; Abdullah, M.M.; Foo, Y.-C.; How, S.-H.; Zaatar, A.; Lam, K.-S.; Leong, K.-W.; et al. Real-world experience of first-line afatinib in patients with EGFR-mutant advanced NSCLC: A multicenter observational study. BMC Cancer 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Burstein, H.J.; Sun, Y.; Dirix, L.Y.; Jiang, Z.; Paridaens, R.; Tan, A.R.; Awada, A.; Ranade, A.; Jiao, S.; Schwartz, G.; et al. Neratinib, an Irreversible ErbB Receptor Tyrosine Kinase Inhibitor, in Patients with Advanced ErbB2-Positive Breast Cancer. J. Clin. Oncol. 2010, 28, 1301–1307. [Google Scholar] [CrossRef]
- Martin, M.; Holmes, F.A.; Ejlertsen, B.; Delaloge, S.; Moy, B.; Iwata, H.; von Minckwitz, G.; Chia, S.K.L.; Mansi, J.; Barrios, C.H.; et al. Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET): 5-year analysis of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1688–1700. [Google Scholar] [CrossRef]
- Paranjpe, R.; Basatneh, D.; Tao, G.; De Angelis, C.; Noormohammed, S.; Ekinci, E.; Abughosh, S.; Ghose, R.; Trivedi, M.V. Neratinib in HER2-Positive Breast Cancer Patients. Ann. Pharmacother. 2019, 53, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Puma Biotechnology, Inc. NERLYNX (Neratinib) [Package Insert]. U.S. Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/208051s000lbl.pdf (accessed on 4 September 2021).
- Daiichi Sankyo, Inc. ENHERTU (Fam-Trastuzumab Deruxtecan-Nxki) [Package Insert]. U.S. Food and Drug Administration. Revised July 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761139s011lbl.pdf (accessed on 20 October 2022).
- Bešlija, S.; Gojković, Z.; Cerić, T.; Abazović, A.M.; Marijanović, I.; Vranić, S.; Mustedanagić–Mujanović, J.; Skenderi, F.; Rakita, I.; Guzijan, A.; et al. 2020 consensus guideline for optimal approach to the diagnosis and treatment of HER2-positive breast cancer in Bosnia and Herzegovina. Bosn. J. Basic Med Sci. 2020, 21, 120–135. [Google Scholar] [CrossRef] [PubMed]
- Mestres, J.A.; Imolins, A.B.; Martínez, L.C.; López-Muñiz, J.I.C.; Gil, E.C.; Ferré, A.D.J.; Berrón, S.D.B.; Pérez, Y.F.; Mata, J.G.; Palomo, A.G.; et al. Defining the optimal sequence for the systemic treatment of metastatic breast cancer. Clin. Transl. Oncol. 2017, 19, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Van Der Horst, H.J.; Nijhof, I.S.; Mutis, T.; Chamuleau, M.E.D. Fc-Engineered Antibodies with Enhanced Fc-Effector Function for the Treatment of B-Cell Malignancies. Cancers 2020, 12, 3041. [Google Scholar] [CrossRef]
- Liu, H.; Saxena, A.; Sidhu, S.S.; Wu, D. Fc Engineering for Developing Therapeutic Bispecific Antibodies and Novel Scaffolds. Front. Immunol. 2017, 8, 38. [Google Scholar] [CrossRef]
- Kang, T.H.; Jung, S.T. Boosting therapeutic potency of antibodies by taming Fc domain functions. Exp. Mol. Med. 2019, 51, 1–9. [Google Scholar] [CrossRef]
- Ilieva, K.M.; Fazekas-Singer, J.; Achkova, D.Y.; Dodev, T.S.; Mele, S.; Crescioli, S.; Bax, H.J.; Cheung, A.; Karagiannis, P.; Correa, I.; et al. Functionally Active Fc Mutant Antibodies Recognizing Cancer Antigens Generated Rapidly at High Yields. Front. Immunol. 2017, 8, 1112. [Google Scholar] [CrossRef]
- Costa, R.L.B.; Czerniecki, B.J. Clinical development of immunotherapies for HER2+ breast cancer: A review of HER2-directed monoclonal antibodies and beyond. npj Breast Cancer 2020, 6, 10. [Google Scholar] [CrossRef]
- Pento, J.T. Monoclonal Antibodies for the Treatment of Cancer. Anticancer Res. 2017, 37, 5935–5939. [Google Scholar] [CrossRef]
- Church, D.N.; Price, C.G. A Review of Trastuzumab-Based Therapy in Patients with HER2-positive Metastatic Breast Cancer. Clin. Med. Ther. 2009, 1, CMT-S35. [Google Scholar] [CrossRef]
- Fan, X.; Brezski, R.; Deng, H.; Dhupkar, P.M.; Shi, Y.; Gonzalez, A.; Zhang, S.; Rycyzyn, M.; Strohl, W.; Jordan, R.E.; et al. A Novel Therapeutic Strategy to Rescue the Immune Effector Function of Proteolytically Inactivated Cancer Therapeutic Antibodies. Mol. Cancer Ther. 2015, 14, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.Y.; Overmoyer, B. Prolonged Survival in Patients with Metastatic HER2-Positive Inflammatory Breast Cancer: A Case Report and Review of the Literature. Case Rep. Oncol. 2021, 14, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.H. Therapeutic Monoclonal Antibodies Approved by FDA in 2020. Clin. Res. Immunol. 2021, 4, 1–2. [Google Scholar]
- Brezski, R.J. Novel Generation of Antibody-Based Therapeutics. In Novel Approaches and Strategies for Biologics, Vaccines and Cancer Therapies; Elsevier: Amsterdam, The Netherlands, 2015; pp. 125–146. [Google Scholar]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S.; Li, H.; Ciccarone, V.; Zhang, T.; Stavenhagen, J.; et al. Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. [Google Scholar] [CrossRef]
- MacroGenics. MARGENZA (Margetuximab-Cmkb): Highlights of Prescribing Information. 2020. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/761150s000lbl.pd (accessed on 27 August 2021).
- Ochoa, M.C.; Minute, L.; Rodriguez, I.; Garasa, S.; Ruiz, E.P.; Inogés, S.; Melero, I.; Berraondo, P. Antibody-dependent cell cytotoxicity: Immunotherapy strategies enhancing effector NK cells. Immunol. Cell Biol. 2017, 95, 347–355. [Google Scholar] [CrossRef]
- Kohrt, H.; Rajasekaran, N.; Chester, C.; Yonezawa, A.; Zhao, X. Enhancement of antibody-dependent cell mediated cytotoxicity: A new era in cancer treatment. ImmunoTargets Ther. 2015, 4, 91–100. [Google Scholar] [CrossRef]
- Blázquez-Moreno, A.; Park, S.; Im, W.; Call, M.J.; Call, M.E.; Reyburn, H.T. Transmembrane features governing Fc receptor CD16A assembly with CD16A signaling adaptor molecules. Proc. Natl. Acad. Sci. USA 2017, 114, E5645–E5654. [Google Scholar] [CrossRef]
- Patel, K.R.; Benavente, M.C.R.; Lorenz, W.W.; Mace, E.M.; Barb, A.W. Fc γ receptor IIIa/CD16a processing correlates with the expression of glycan-related genes in human natural killer cells. J. Biol. Chem. 2021, 296, 100183. [Google Scholar] [CrossRef]
- Jing, Y.; Ni, Z.; Wu, J.; Higgins, L.; Markowski, T.W.; Kaufman, D.; Walcheck, B. Identification of an ADAM17 Cleavage Region in Human CD16 (FcγRIII) and the Engineering of a Non-Cleavable Version of the Receptor in NK Cells. PLoS ONE 2015, 10, e0121788. [Google Scholar] [CrossRef]
- Mahaweni, N.M.; Olieslagers, T.I.; Rivas, I.O.; Molenbroeck, S.J.J.; Groeneweg, M.; Bos, G.M.J.; Tilanus, M.G.J.; Voorter, C.E.M.; Wieten, L. A comprehensive overview of FCGR3A gene variability by full-length gene sequencing including the identification of V158F polymorphism. Sci. Rep. 2018, 8, 15983. [Google Scholar] [CrossRef]
- Larionov, A.A. Current Therapies for Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer Patients. Front. Oncol. 2018, 8, 89. [Google Scholar] [CrossRef] [PubMed]
- Kellner, C.; Otte, A.; Cappuzzello, E.; Klausz, K.; Peipp, M. Modulating Cytotoxic Effector Functions by Fc Engineering to Improve Cancer Therapy. Transfus. Med. Hemotherapy 2017, 44, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Mathieu, M.; Brezski, R.J. IgG Fc engineering to modulate antibody effector functions. Protein Cell 2018, 9, 63–73. [Google Scholar] [CrossRef]
- Kaplon, H.; Muralidharan, M.; Schneider, Z.; Reichert, J.M. Antibodies to watch in 2020. mAbs 2020, 12, 1703531. [Google Scholar] [CrossRef]
- Chen, D.; Zhao, Y.; Li, M.; Shang, H.; Li, N.; Li, F.; Wang, W.; Wang, Y.; Jin, R.; Liu, S.; et al. A general Fc engineering platform for the next generation of antibody therapeutics. Theranostics 2021, 11, 1901–1917. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Giaccone, G.; Im, S.A.; Oh, D.Y.; Bauer, T.M.; Nordstrom, J.L.; Li, H.; Chichili, G.R.; Moore, P.A.; Hong, S.; et al. First-in-human phase 1 study of margetuximab (MGAH22), an Fc-modified chimeric monoclonal antibody, in patients with HER2-positive advanced solid tumors. Ann. Oncol. 2017, 28, 855–861. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. 2021; PubChem Substance Record for SID 172232539, Margetuximab (USAN), Source: KEGG. Available online: https://pubchem.ncbi.nlm.nih.gov/substance/172232539 (accessed on 2 September 2021).
- Margetuximab. Available online: https://go.drugbank.com/drugs/DB14967 (accessed on 4 September 2021).
- Tarantino, P.; Morganti, S.; Uliano, J.; Giugliano, F.; Crimini, E.; Curigliano, G. Margetuximab for the treatment of HER2-positive metastatic breast cancer. Expert Opin. Biol. Ther. 2020, 21, 127–133. [Google Scholar] [CrossRef]
- Pegram, M.D.; Tan-Chiu, E.; Miller, K.; Rugo, H.S.; Yardley, D.A.; Liv, S.; Stewart, S.J.; Erban, J.K. A single-arm, open-label, phase 2 study of MGAH22 (margetuximab) [fc-optimized chimeric anti-HER2 monoclonal antibody (mAb)] in patients with relapsed or refractory advanced breast cancer whose tumors express HER2 at the 2+ level by immunohistochemistry and lack evidence of HER2 gene amplification by FISH. J. Clin. Oncol. 2014, 32, TPS671. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.-A.; Cardoso, F.; Cortés, J.; Curigliano, G.; Musolino, A.; Pegram, M.D.; Wright, G.S.; Saura, C.; Escrivá-De-Romaní, S.; et al. Efficacy of Margetuximab vs Trastuzumab in Patients with Pretreated ERBB2-Positive Advanced Breast Cancer. A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 573–584. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.A.; Cardoso, F.; Cortes, J.; Curigliano, G.; Musolino, A.; Pegram, M.D.; Bachelot, T.; Wright, G.S.; Saura, C.; et al. Margetuximab Versus Trastuzumab in Patients with Previously Treated HER2-Positive Advanced Breast Cancer (SOPHIA): Final Overall Survival Results From a Randomized Phase 3 Trial. J. Clin. Oncol. 2022. [Google Scholar] [CrossRef]
- Catenacci, D.V.T.; Kang, Y.-K.; Park, H.; Uronis, H.E.; Lee, K.-W.; Ng, M.C.H.; Enzinger, P.C.; Park, S.H.; Gold, P.J.; Lacy, J.; et al. Margetuximab plus pembrolizumab in patients with previously treated, HER2-positive gastro-oesophageal adenocarcinoma (CP-MGAH22–05): A single-arm, phase 1b–2 trial. Lancet Oncol. 2020, 21, 1066–1076. [Google Scholar] [CrossRef] [PubMed]
- Catenacci, D.V.; Rosales, M.; Chung, H.C.; Yoon, H.H.; Shen, L.; Moehler, M.; Kang, Y.-K. MAHOGANY: Margetuximab combination in HER2+ unresectable/metastatic gastric/gastroesophageal junction adenocarcinoma. Future Oncol. 2021, 17, 1155–1164. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Agent | Year of FDA Approval | Mechanism of Action | Indication | Dosage | Major Adverse Effects | Box Warning |
|---|---|---|---|---|---|---|
| Trastuzumab [31,32] | 1998 | A humanized monoclonal IgG1 antibody that targets the extracellular domain (domain IV) of human HER2/neu, preventing dimerization and inducing ADCC | Treatment of HER2/neu overexpressing breast cancer/HER2 + MBC (first-line setting in therapy); used as adjuvant/neo adjuvant therapy alongside chemotherapy for ≤ 1 year. | Initial loading dose of 4 mg/kg IV followed by 2 mg/kg weekly or a loading dose of 8 mg/kg IV followed by 6 mg/kg every 3 weeks | Fever, infusion related reactions, diarrhea, headache, increased cough, rash, anemia, neutropenia, and myalgia | Cardiotoxicity, decline in left ventricular function; pulmonary toxicity (rare); infusion-related reactions |
| Lapatinib [33,34,35] | 2007 | Reversible tyrosine kinase inhibitor of HER1 and HER2 phosphorylation, resulting in an inhibition of signal transduction | Used in combination with capecitabine | 1250 mg/kg orally for 1–21 days along with 1000 mg/m2 capecitabine for 1–14 days, repeated every 3 weeks | Nausea, diarrhea, fatigue, and rash (acne, dermatitis acneiform) | Idiosyncratic hepatotoxicity |
| Pertuzumab [36,37] | 2012 | A humanized monoclonal IgG1 antibody that targets the ECD II of HER2/neu, preventing heterodimerization of HER2 with other HER family members | Used as adjuvant/neo adjuvant therapy; given for 1 year for node positive disease; used in conjunction with trastuzumab and taxane for MBC as a first-line therapy | Initial loading dose of 840 mg/kg followed by 420 mg/kg every 3 weeks | Nausea, diarrhea, neutropenia, alopecia, rash, and peripheral neuropathy | Cardiotoxicity, decline in LVF, IRR hypersensitivity reactions/anaphylaxis, cardiomyopathy, and embryo-fetal toxicity |
| Ado-trastuzumab Emtansine (T-DM1) [38,39] | 2013 | An antibody drug conjugate comprising trastuzumab linked to a potent anti-microtubule agent DM1 (derivative of maytansine); causes cell-cycle arrest, leads to apoptosis, induces ADCC, and disrupts downstream HER2 signaling | Used to treat patients with HER2 + MBC who previously received trastuzumab and a taxane; adjuvant treatment of patients with HER2+ early BC | 3.6 mg/kg IV every 3 weeks | Fatigue, nausea, headache, thrombocytopenia, and constipation | Hepatotoxicity, left ventricular dysfunction, pulmonary toxicity, IRR hypersensitivity reactions, thrombocytopenia, and neurotoxicity |
| Afatinib [40,41] | 2013 | Irreversible HER1 and HER2 tyrosine kinase inhibitor; induces phosphorylation leading to subsequent inhibition of signal transduction | Used as first-line therapy for advanced NSCLC patients with mutant-HER1 | Afatinib, 40 mg or 30 mg once daily | Diarrhea, paronychia, acneiform skin rash, stomatitis, and a loss of appetite | Left ventricular dysfunction, diarrhea, hepatotoxicity, hand-foot skin reaction, and interstitial lung disease |
| Neratinib [42,43,44,45] | 2017 | Irreversible HER1 and HER2 tyrosine kinase inhibitor; causes phosphorylation leading to subsequent inhibition of signal transduction | Extended adjuvant therapy administered after trastuzumab and chemotherapy | 240 mg orally with food continued for 1 year along with prophylactic loperamide | Diarrhea, nausea, vomiting, anorexia, abdominal pain fatigue, and decreased appetite | Diarrhea (grade ≥ 3), hepatotoxicity, and embryo-fetal toxicity |
| Trastuzumab-deruxtecan [46] | 2019 | An antibody-drug conjugate comprising trastuzumab linked to topoisomerase I inhibitor (deruxtecan); induces ADCC, disrupts downstream HER2 signaling leads to apoptosis and cell-cycle arrest | Used for patients with metastatic or unresectable HER2+ breast cancer who have had one or more prior anti-HER2-based regimens | 5.4 mg/kg IV every 3 weeks | Nausea, diarrhea, vomiting, musculoskeletal pain, and myelosuppression | Interstitial lung disease, left ventricular dysfunction, neutropenia, embryo-fetal toxicity |
| NCT Identifier | Year of Clinical Study | Study Title | Phase and Study Design | Study Participant | Study Type | Subject Number | Status | Study Arm |
|---|---|---|---|---|---|---|---|---|
| NCT01148849 [73] | 2010 | Safety study of Margetuximab in HER2+ carcinomas | I-Single Group Assignment, open label, treatment purpose | ≥18 years (adults, older adults), with confirmed HER2 + MBC | IV | 66 | Completed | Margetuximab |
| NCT01828021 [60] | 2013 | Phase 2 study of Margetuximab in patients with relapsed or refractory advanced BC | II-Single Group Assignment, open label, treatment purpose | Age ≥ 18 years (adults, older adults), with confirmed invasive BC | IV | 25 | Completed | Margetuximab |
| NCT02492711 [76] | 2015 | Margetuximab plus chemotherapy vs. Trastuzumab plus chemotherapy in the treatment of HER2 + MBC (SOPHIA) | III-Randomized, parallel assignment, open label, treatment purpose | Age ≥ 18 years (adults, older adults), with confirmed HER2 + MBC | IV | 624 | Completed | Margetuximab and the chosen chemotherapy (Capecitabine/Vinorelbine/Eribulin/Gemcitabine) vs. Trastuzumab and the chosen chemotherapy |
| NCT03133988 | 2017 | Margetuximab Expanded Access Program | not available | Children, adults, older adults | EA | Case -by-case basis | Approved for marketing | Margetuximab |
| NCT04262804 | 2020 | A study to evaluate the efficacy and safety of Margetuximab plus chemotherapy in the treatment of Chinese patients with HER2 + MBC | II-Randomized, parallel assignment, open label, treatment purpose | Male or female, age ≥ 18 years, with confirmed HER2 + MBC; have received at least 2 prior lines of anti-HER2 directed therapy in the metastatic setting | IV | 120 | Recruiting | Margetuximab and the chosen chemotherapy (Capecitabine/Vinorelbine/Gemcitabine) vs. Trastuzumab and the chosen chemotherapy |
| NCT04398108 | 2020 | A study to evaluate the pharmacokinetics of Margetuximab in Chinese patients with HER2 + MBC | I-Single group assignment, open label, treatment purpose | Male or female, age ≥ 18 years, with confirmed HER2 + MBC; have received at least 2 prior lines of anti-HER2 directed therapy in the metastatic setting | IV | 16 | Completed | Margetuximab and the chosen chemotherapy (Capecitabine/Vinorelbine/Gemcitabine) |
| NCT04425018 | 2020 | MARGetuximab or trastuzumab (MARGOT) (MARGOT) | II-Randomized, parallel assignment, open label, treatment purpose | Male or female, age ≥ 18 years, with confirmed Stage II or III invasive BC | IV | 171 | Recruiting | Arm (a): Paclitaxel, Pertzumab, and Margetuximab; arm (b): Paclitaxel, Pertzumab, and Trastuzumab |
| NCT Identifier | Study Title | Phase and Study Design | Study Participant | Study Type | Subjects, n | Status | Study Arm | Indications |
|---|---|---|---|---|---|---|---|---|
| NCT02689284 [80] | Combination of margetuximab and pembrolizumab for advanced, metastatic HER2+ gastric or gastroesophageal junction cancer | Ib/2 Single group assignment, open label, treatment purpose | Age ≥ 18 years’ old; with confirmed HER2 + MGEJ or gastric cancer; Have received trastuzumab or at least 1/>lines of cytotoxic CT in the metastatic setting | Interventional | 95 | Completed | Margetuximab plus pembrolizumab | Gastric, stomach, and esophageal cancer |
| NCT04082364 [81] | Combination of margetuximab, INCMGA00012, MGD013, and chemotherapy Phase 2/3 trial in HER2+ gastric/GEJ cancer (MAHOGANY) | II/III Randomized, parallel assignment, open label, treatment purpose | Age ≥ 18 years (Adult, Older Adult), with confirmed HER2 + M (GEJ) or gastric cancer | Interventional | 860 | Recruiting | Cohort A: single-arm cohort. (safety efficacy evaluation); Cohort B Part 1: randomized, 4-arm segment; Cohort B Part 2: randomized, 2-arm segment | Gastric cancer, gastroesophageal junction cancer, and HER2+ gastric cancer |
| NCT03219268 [76] | A study of MGD013 in patients with unresectable or metastatic neoplasms | I Non-randomized, single group assignment, open label, treatment purpose | Age ≥18 years (Adult, Older Adult), with confirmed advanced unresectable or metastatic solid tumors; cohort expansion only | Interventional | 353 | Active, not recruiting | Dose escalation followed by Cohort Expansion Phase at the MTD. MGD013; MGD013 + margetuximab | Advanced solid tumors, hematologic neoplasms, ovarian cancer, HER2 + BC, NSCLC, cervical cancer, TNBC etc. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alasmari, M.M. A Review of Margetuximab-Based Therapies in Patients with HER2-Positive Metastatic Breast Cancer. Cancers 2023, 15, 38. https://doi.org/10.3390/cancers15010038
Alasmari MM. A Review of Margetuximab-Based Therapies in Patients with HER2-Positive Metastatic Breast Cancer. Cancers. 2023; 15(1):38. https://doi.org/10.3390/cancers15010038
Chicago/Turabian StyleAlasmari, Moudi M. 2023. "A Review of Margetuximab-Based Therapies in Patients with HER2-Positive Metastatic Breast Cancer" Cancers 15, no. 1: 38. https://doi.org/10.3390/cancers15010038
APA StyleAlasmari, M. M. (2023). A Review of Margetuximab-Based Therapies in Patients with HER2-Positive Metastatic Breast Cancer. Cancers, 15(1), 38. https://doi.org/10.3390/cancers15010038