
Somatostatin Receptor 2 Expression Profiles and Their Correlation with the Efficacy of Somatostatin Analogues in Gastrointestinal Neuroendocrine Tumors

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Tissues and Patient Characteristics
2.2. Single Immunohistochemistry
2.3. Double-Immunohistochemistry
2.4. Evaluation of Ki-67 Labeling Index
2.5. Evaluation of Single Immunohistochemistry of SSTR2 Immunoreactivity Using Manual/Eyeball Analysis (Volante Scores and Immunoreactive Scores) and DIA
2.6. Evaluation of Double Immunohistochemical Staining of SSTR2 Immunoreactivity
2.7. Statistical Analyses
3. Results
3.1. The Correlations of SSTR2 Immunoreactivity Evaluated by Three Scoring Systems
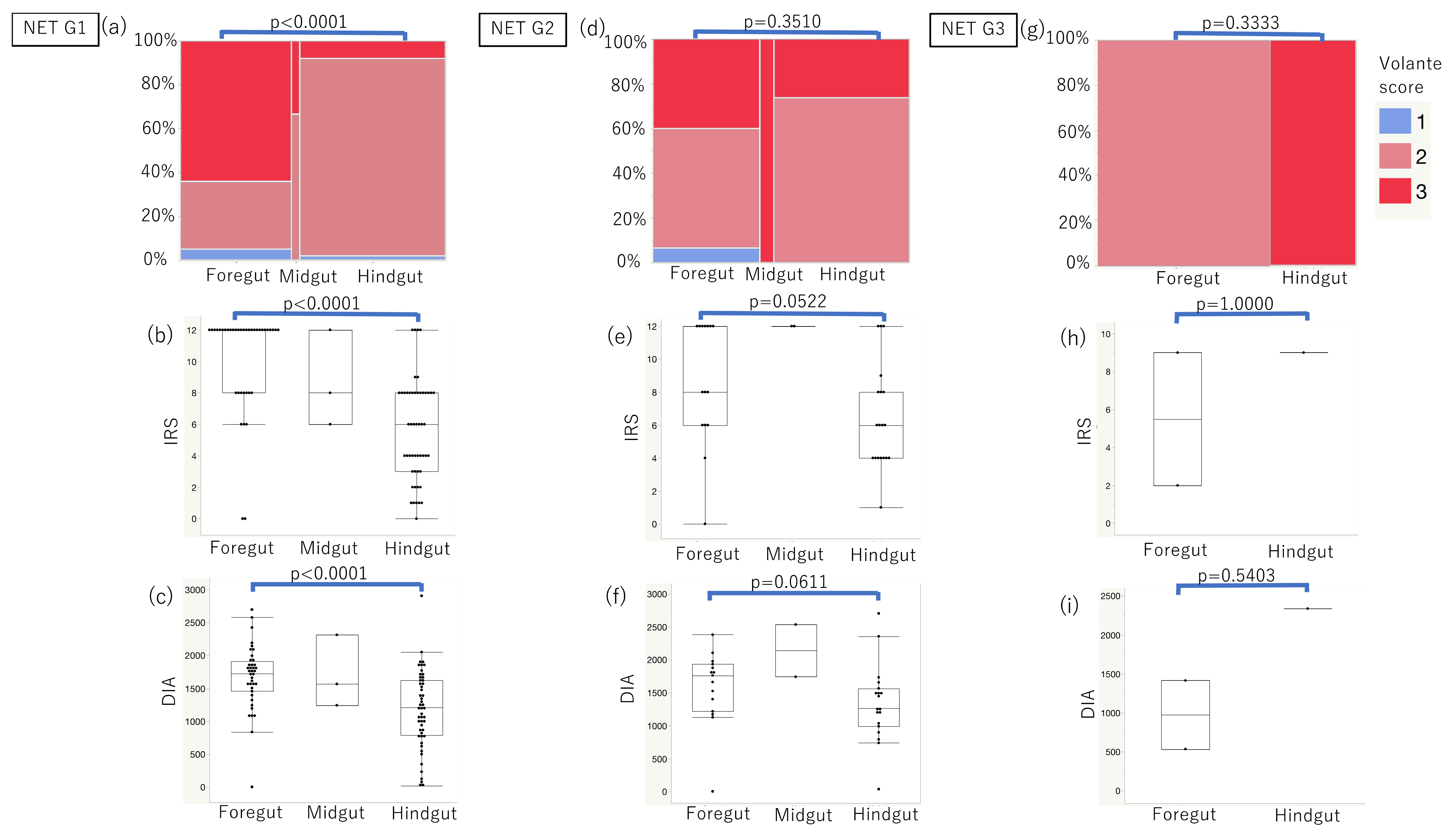
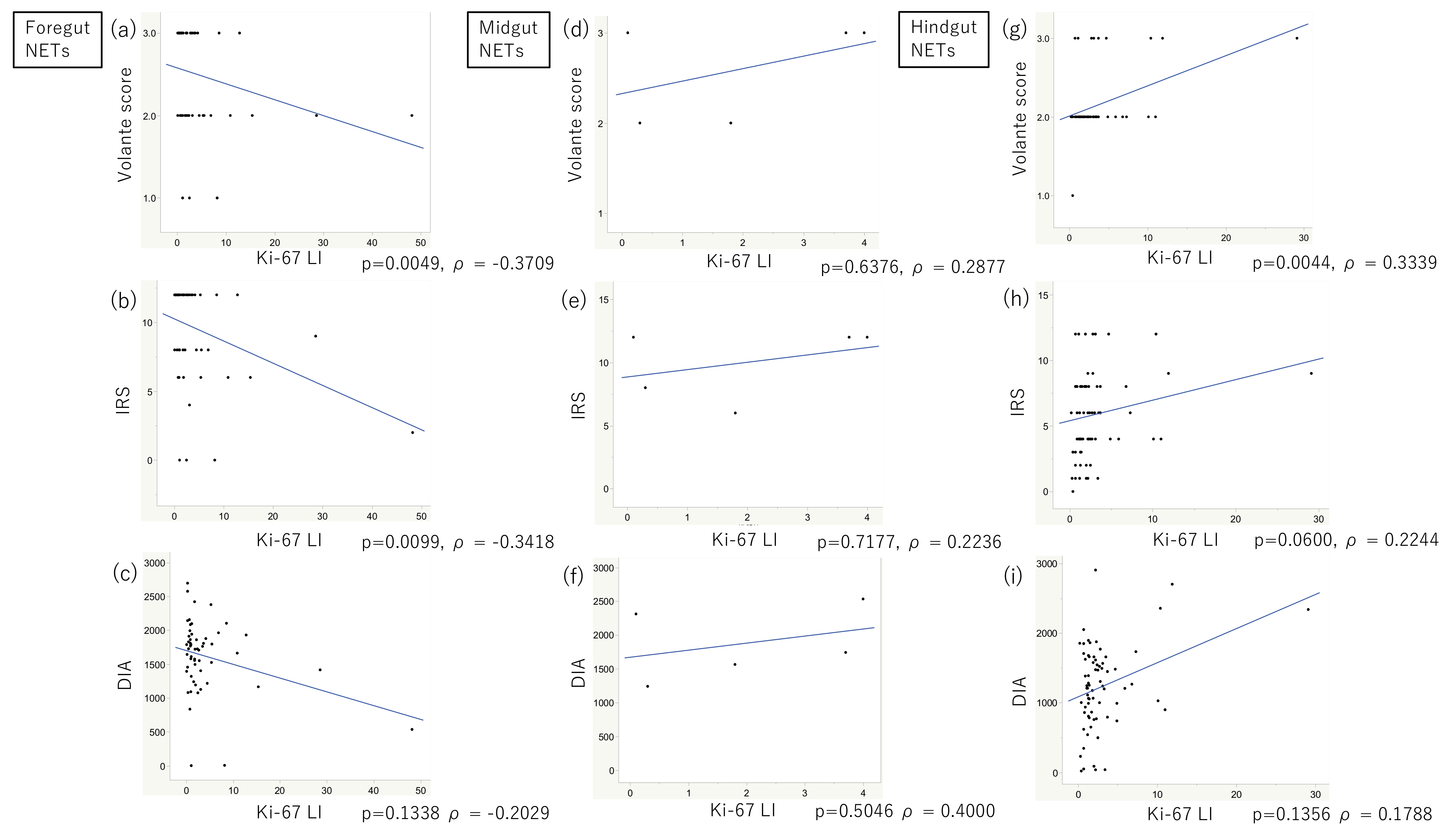
3.2. SSTR2 Immunoreactivity Evaluated by Three Scoring Systems and Their Correlations with Embryological Origins, Ki-67 LI, and Histological Grades in Group 2
3.3. SSTR2 Immunoreactivity and Its Correlation with the Therapeutic Efficacy of Somatostatin Analogues in Group 3 When Evaluated Using Three Scoring Systems
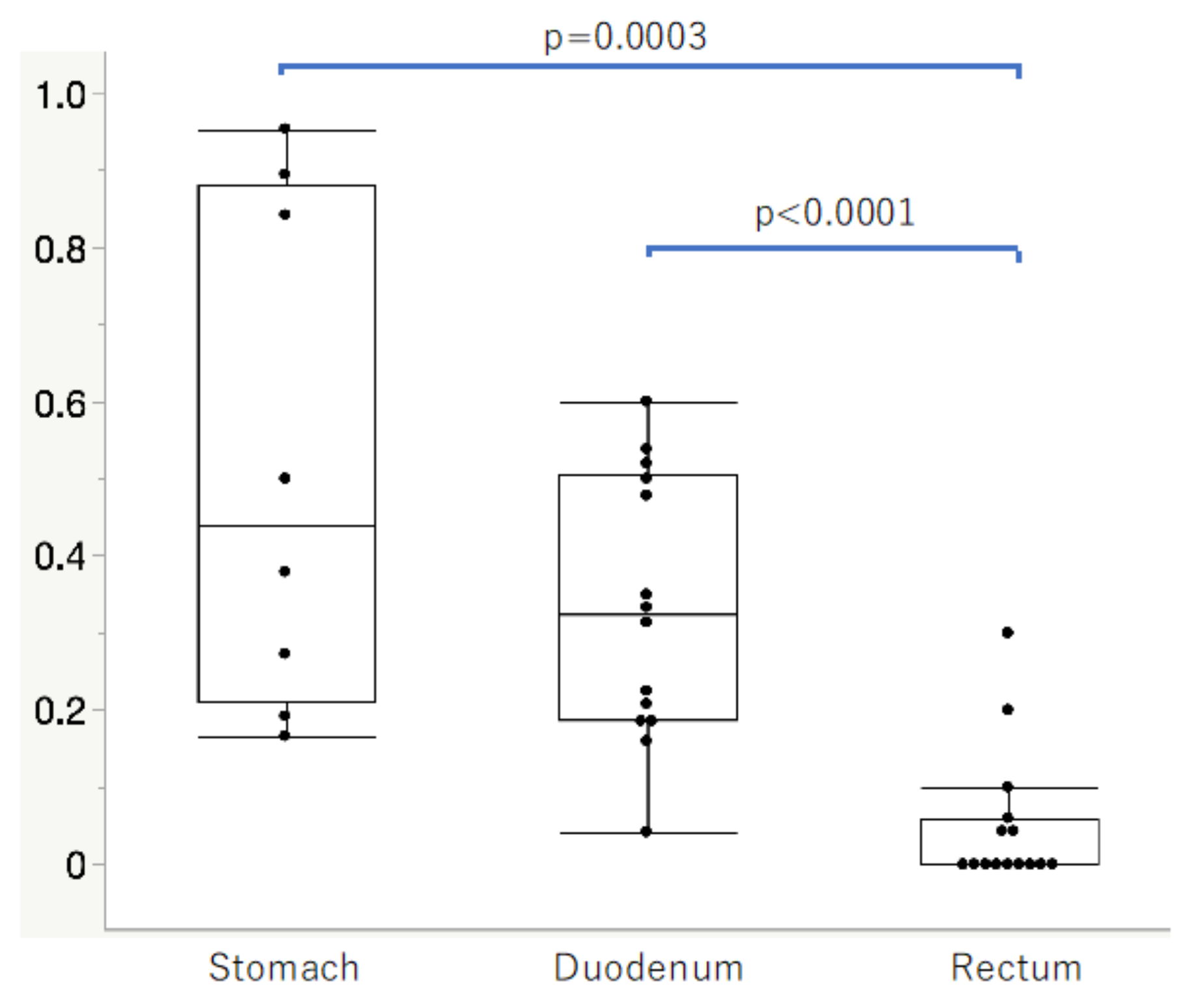
3.4. SSTR2-Positive Rates in Normal Neuroendocrine Cells of the Gastrointestinal Mucosa in Group 4
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taal, B.G.; Visser, O. Epidemiology of neuroendocrine tumours. Neuroendocrinology 2004, 80, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M. Gastrointestinal neuroendocrine tumors in 2020. World J. Gastrointest. Oncol. 2020, 12, 79–807. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.M. Proton Pump Inhibitor Use, Hypergastrinemia, and Gastric Carcinoids-What Is the Relationship? Int. J. Mol. Sci. 2020, 21, 662. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.D.; Sandler, M. The classification of carcinoid tum ours. Lancet 1963, 1, 238–239. [Google Scholar] [CrossRef]
- Watanabe, H.; Yamazaki, Y.; Fujishima, F.; Izumi, K.; Imamura, M.; Hijioka, S.; Toriyama, K.; Yatabe, Y.; Kudo, A.; Motoi, F.; et al. O(6)-methylguanine DNA methyltransferase and glucose transporter 2 in foregut and hindgut gastrointestinal neuroendocrine neoplasms. BMC Cancer 2020, 20, 1195. [Google Scholar] [CrossRef]
- Rindi, G.; Klöppel, G.; Couvelard, A.; Komminoth, P.; Körner, M.; Lopes, J.M.; McNicol, A.-M.; Nilsson, O.; Perren, A.; Scarpa, A.; et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: A consensus proposal including a grading system. Virchows Arch. 2007, 451, 757–762. [Google Scholar] [CrossRef]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef]
- Oberg, K.E.; Reubi, J.C.; Kwekkeboom, D.J.; Krenning, E.P. Role of somatostatins in gastroenteropancreatic neuroendocrine tumor development and therapy. Gastroenterology 2010, 139, 742–753.e1. [Google Scholar] [CrossRef]
- Öberg, K.E. Gastrointestinal neuroendocrine tumors. Ann. Oncol. 2010, 21, vii72–vii80. [Google Scholar] [CrossRef]
- Kim, J.Y.; Hong, S.M. Recent Updates on Neuroendocrine Tumors from the Gastrointestinal and Pancreatobiliary Tracts. Arch. Pathol. Lab. Med. 2016, 140, 437–448. [Google Scholar] [CrossRef]
- Elf, A.K.; Johanson, V.; Marin, I.; Bergström, A.; Nilsson, O.; Svensson, J.; Wangberg, B.; Bernhardt, P.; Elias, E. Evaluation of SSTR2 Expression in SI-NETs and Relation to Overall Survival after PRRT. Cancers 2021, 23, 2035. [Google Scholar] [CrossRef]
- Guillermet-Guibert, J.; Lahlou, H.; Cordelier, P.; Bousquet, C.; Pyronnet, S.; Susini, C. Physiology of somatostatin receptors. J. Endocrinol. Investig. 2005, 28, 5–9. [Google Scholar]
- Dalm, V.A.; van Hagen, P.M.; van Koetsveld, P.M.; Achilefu, S.; Houtsmuller, A.B.; Pols, D.H.; van der Lely, A.-J.; Lamberts, S.W.J.; Hofland, L.J. Expression of somatostatin, cortistatin, and somatostatin receptors in human monocytes, macrophages, and dendritic cells. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E344–E353. [Google Scholar] [CrossRef] [PubMed]
- Ampofo, E.; Nalbach, L.; Menger, M.D.; Laschke, M.W. Regulatory Mechanisms of Somatostatin Expression. Int. J. Mol. Sci. 2020, 21, 4170. [Google Scholar] [CrossRef] [PubMed]
- Martín-Gago, P.; Rol, Á.; Todorovski, T.; Aragón, E.; Martin-Malpartida, P.; Verdaguer, X.; Miret, M.V.; Fernandez-Carneado, J.; Ponsati, B.; Macias, M.J.; et al. Peptide aromatic interactions modulated by fluorinated residues: Synthesis, structure and biological activity of Somatostatin analogs containing 3-(3’,5’difluorophenyl)-alanine. Sci. Rep. 2016, 6, 27285. [Google Scholar] [CrossRef]
- Somvanshi, R.K.; Kumar, U. Pathophysiology of GPCR Homo- and Heterodimerization: Special Emphasis on Somatostatin Receptors. Pharmaceuticals 2012, 5, 417–446. [Google Scholar] [CrossRef] [PubMed]
- Theodoropoulou, M.; Stalla, G.K. Somatostatin receptors: From signaling to clinical practice. Front. Neuroendocrinol. 2013, 34, 228–252. [Google Scholar] [CrossRef]
- Kasajima, A.; Papotti, M.; Ito, W.; Brizzi, M.P.; La Salvia, A.; Rapa, I.; Tachibana, T.; Yazdani, S.; Sasano, H.; Volante, M. High interlaboratory and interobserver agreement of somatostatin receptor immunohistochemical determination and correlation with response to somatostatin analogs. Hum. Pathol. 2018, 72, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Volante, M.; Brizzi, M.P.; Faggiano, A.; La Rosa, S.; Rapa, I.; Ferrero, A.; Mansueto, G.; Righi, L.; Garancini, S.; Capello, C.; et al. Somatostatin receptor type 2A immunohistochemistry in neuroendocrine tumors: A proposal of scoring system correlated with somatostatin receptor scintigraphy. Mod. Pathol. 2007, 20, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Gatto, F.; Feelders, R.A.; van der Pas, R.; Kros, J.M.; Waaijers, M.; Sprij-Mooij, D.; Neggers, S.J.C.M.M.; van der Lelij, A.-J.; Minuto, F.; Lamberts, S.W.J.; et al. Immunoreactivity score using an anti-sst2A receptor monoclonal antibody strongly predicts the biochemical response to adjuvant treatment with somatostatin analogs in acromegaly. J. Clin. Endocrinol. Metab. 2013, 98, E66–E71. [Google Scholar] [CrossRef]
- Cullinane, C.; Waldeck, K.; Kirby, L.; Rogers, B.E.; Eu, P.; Tothill, R.W.; Hicks, R.J. Enhancing the anti-tumour activity of 177Lu-DOTA-octreotate radionuclide therapy in somatostatin receptor-2 expressing tumour models by targeting PARP. Sci. Rep. 2020, 10, 10196. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Parghane, R.V.; Chakrabarty, S. Peptide Receptor Radionuclide Therapy of Neuroendocrine Tumors. Semin. Nucl. Med. 2020, 50, 447–464. [Google Scholar] [CrossRef] [PubMed]
- Marcuzzo, T.; Giudici, F.; Ober, E.; Rizzardi, C.; Bottin, C.; Zanconati, F. Her2 immunohistochemical evaluation by traditional microscopy and by digital analysis, and the consequences for FISH testing. Pathol. Res. Pract. 2016, 212, 911–918. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Watanabe, H.; Ide, R.; Yamazaki, Y.; Fujishima, F.; Kasajima, A.; Yazdani, S.; Tachibana, T.; Motoi, F.; Unno, M.; Sasano, H. Quantitative digital image analysis of somatostatin receptor 2 immunohistochemistry in pancreatic neuroendocrine tumors. Med. Mol. Morphol. 2021, 54, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; de Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef]
- Koelzer, V.H.; Gisler, A.; Hanhart, J.C.; Griss, J.; Wagner, S.N.; Willi, N.; Cathomas, G.; Sachs, M.; Kempf, W.; Thommen, D.S.; et al. Digital image analysis improves precision of PD-L1 scoring in cutaneous melanoma. Histopathology 2018, 73, 397–406. [Google Scholar] [CrossRef]
- Borin, J.F.; Tang, L.H.; Kidd, M.; Miu, K.; Borteçen, K.H.; Sandor, A.; Modlin, I.M. Somatostatin receptor regulation of gastric enterochromaffin-like cell transformation to gastric carcinoid. Surgery 1996, 120, 1026–1032. [Google Scholar] [CrossRef]
- Rindi, G.; Bordi, C.; Rappel, S.; La Rosa, S.; Stolte, M.; Solcia, E. Gastric carcinoids and neuroendocrine carcinomas: Pathogenesis, pathology, and behavior. World J. Surg. 1996, 20, 168–172. [Google Scholar] [CrossRef]
- Klomp, M.J.; Dalm, S.U.; de Jong, M.; Feelders, R.A.; Hofland, J.; Hofland, L.J. Epigenetic regulation of somatostatin and somatostatin receptors in neuroendocrine tumors and other types of cancer. Rev. Endocr. Metab. Disord. 2021, 22, 495–510. [Google Scholar] [CrossRef] [PubMed]
- Butt, S.; Evans, J.; Mauri, F.; Sharma, R. Methylation of somatostatin receptor 2 gene in neuroendocrine tumours as a predictor of tumour response to peptide receptor radionuclide therapy. Clin. Med. 2019, 19, 123. [Google Scholar] [CrossRef]
- Kaemmerer, D.; Peter, L.; Lupp, A.; Schulz, S.; Sänger, J.; Baum, R.P.; Prasad, V.; Hommann, M. Comparing of IRS and Her2 as immunohistochemical scoring schemes in gastroenteropancreatic neuroendocrine tumors. Int. J. Clin. Exp. Pathol. 2012, 5, 187–194. [Google Scholar] [PubMed]
- Koopman, T.; de Bock, G.H.; Buikema, H.J.; Smits, M.M.; Louwen, M.; Hage, M.; Imholz, A.L.T.; van der Vegt, B. Digital image analysis of HER2 immunohistochemistry in gastric- and oesophageal adenocarcinoma: A validation study on biopsies and surgical specimens. Histopathology 2018, 72, 191–200. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Supplier (Catalogue Number) | Host | Antigen Retrieval Treatment | Dilution | Reaction Time of Primary Antibody | Antibody Type | Secondary Antibody | Positive Control |
|---|---|---|---|---|---|---|---|---|
| Ki-67 | Agilent technologies, US (IR626) | Mouse | PT Link (97 ℃, 20 min), Target Retrieval Solution High PH | Ready to use | 20 min, room temperature | MIB-1 | EnVision FLEX | Epithelial cell |
| SSTR2 | Abcam, England (ab134152) | Rabbit | AC (121 ℃, 5 min), pH 6.0 | 1:2000 | 4 ℃, overnight | UMB1 | Histofine Kit | Islet of langerhans |
| Chromogranin A | Agilent technologies, US (A0430) | Rabbit | Microwave (210 W, 15 min), pH 6.0 | 1:1500 | 4 ℃, overnight | polyclonal | Histofine Kit | Islet of langerhans |
| GI-NET | p-Value | ||||
|---|---|---|---|---|---|
| Foregut | Midgut | Hindgut | |||
| Total number | 56 | 5 | 71 | ||
| Age | Median (range) | 60.5 (33–88) | 62 (53–74) | 61 (36–82) | NS |
| Sex | Male | 36 | 3 | 46 | NS |
| Female | 20 | 2 | 25 | ||
| Function | Non-function | 42 | 3 | 70 | <0.0001 |
| Gastrinoma | 13 | 0 | 0 | ||
| Carcinoid syndrome | 0 | 2 | 0 | ||
| Not available | 1 | 0 | 1 | ||
| Hereditary background | Not detected | 45 | 5 | 71 | 0.0002 |
| MEN1 | 11 | 0 | 0 | ||
| Volante score | 0 | 0 | 0 | 0 | <0.0001 |
| 1 | 3 | 0 | 1 | ||
| 2 | 22 | 2 | 60 | ||
| 3 | 31 | 3 | 10 | ||
| IRS | Median (range) | 12 (0–12) | 12 (6–12) | 6 (0–12) | <0.0001 |
| DIA * | Median (range) | 1723 (0–2695) | 1741 (1240–2533) | 1238 (19–2904) | <0.0001 |
| WHO2019 | NET G1 | 38 | 3 | 51 | NS |
| NETG2 | 15 | 2 | 19 | ||
| NET G3 | 2 | 0 | 1 | ||
| Ki-67 LI | Median (range) | 1.7 (0.1–48.2) | 1.8 (0.2–29.1) | 1.9 (0.1–29.1) | NS |
| Case No. | Sex | Age | Primary Location | Tissue Origin | Grade | Preoperative Therapy | SSTR2 Immunoreactivity | Treatment | Response to SSA | SD, CR = Positive PD = Negative | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Volante Score | IRS | DIA * | ||||||||||
| 1 | M | 63 | midgut | primary site | G1 | TS1, Octreotide | 2 | 4 | 769 | Octreotide, UFT | CR | positive |
| 2 | F | 60 | hindgut | primary site | G2 | Not done | 2 | 6 | 1492 | Lanreotide | SD | positive |
| 3 | M | 55 | midgut | primary site | G2 | Not done | 3 | 12 | 1741 | Lanreotide | SD | positive |
| 4 | M | 61 | hindgut | primary site | G2 | Octreotide | 1 | 0 | 163 | Octreotide | SD | positive |
| 5 | F | 45 | hindgut | primary site | G1 | Octreotide, Lanreotide | 2 | 2 | 1075 | Octreotide, Lanreotide | SD | positive |
| 6 | M | 65 | hindgut | primary site | G2 | Not done | 2 | 4 | 898 | Octreotide, Lanreotide | SD | positive |
| 7 | M | 48 | hindgut | metastatic site (liver) | G2 | Octreotide, Lanreotide | 2 | 2 | 830 | Octreotide, Lanreotide | PD | negative |
| 8 | M | 72 | midgut | metastatic site (liver) | G2 | Octreotide, Lanreotide | 2 | 4 | 731 | Octreotide, Lanreotide | PD | negative |
| 9 | M | 61 | foregut | primary site | G2 | Not done | 2 | 12 | 2379 | Octreotide | PD | negative |
| 10 | M | 73 | foregut | metastatic site (liver) | G2 | Not done | 1 | 0 | 215 | Lanreotide | PD | negative |
| 11 | M | 74 | midgut | primary site | G1 | Not done | 2 | 8 | 1240 | Lanreotide | SD | positive |
| 12 | F | 65 | foregut | metastatic site (liver) | G1 | Octreotide | 2 | 8 | 1467 | Octreotide | SD | positive |
| 13 | F | 67 | midgut | primary site | G1 | Octreotide, Everolimus | 2 | 2 | 967 | Octreotide | SD | positive |
| 14 | F | 71 | hindgut | primary site | G2 | Not done | 2 | 4 | 1027 | 5FU, CDDP, Octreotide | SD | positive |
| Case No. | Site | Age | Sex | Positive Rates * | |
|---|---|---|---|---|---|
| 1 | Stomach | Pyloric gland | 64 | Male | 0.953 |
| 2 | Pyloric gland | 81 | Male | 0.842 | |
| 3 | Fundic glands | 55 | Male | 0.5 | |
| 4 | Pyloric gland | 83 | Female | 0.166 | |
| 5 | Cardiac gland | 83 | Male | 0.379 | |
| 6 | Fundic glands | 66 | Male | 0.894 | |
| 7 | Fundic glands | 63 | Male | 0.192 | |
| 8 | Cardiac gland | 58 | Female | 0.272 | |
| 1 | Duodenum | Bulb of duodenum | 64 | Male | 0.52 |
| 2 | Bulb of duodenum | 81 | Male | 0.16 | |
| 4 | Bulb of duodenum | 83 | Female | 0.333 | |
| 5 | Bulb of duodenum | 83 | Male | 0.208 | |
| 8 | Bulb of duodenum | 58 | Female | 0.6 | |
| 9 | Bulb of duodenum | 73 | Male | 0.538 | |
| 10 | Bulb of duodenum | 69 | Female | 0.5 | |
| 11 | Second portion | 67 | Male | 0.187 | |
| 12 | Second portion | 71 | Female | 0.041 | |
| 13 | Second portion | 79 | Male | 0.218 | |
| 14 | Second portion | 55 | Male | 0.185 | |
| 15 | Second portion | 67 | Male | 0.346 | |
| 16 | Second portion | 69 | Male | 0.478 | |
| 17 | Second portion | 73 | Male | 0.313 | |
| 18 | Rectum | 60 | Female | 0 | |
| 19 | 83 | Female | 0.3 | ||
| 20 | 52 | Male | 0 | ||
| 21 | 70 | Female | 0 | ||
| 22 | 40 | Male | 0 | ||
| 23 | 62 | Male | 0.1 | ||
| 24 | 51 | Female | 0 | ||
| 25 | 81 | Female | 0.2 | ||
| 26 | 75 | Male | 0 | ||
| 27 | 70 | Female | 0.043 | ||
| 28 | 56 | Female | 0.043 | ||
| 29 | 87 | Female | 0 | ||
| 30 | 79 | Female | 0 | ||
| 31 | 77 | Male | 0.058 | ||
| 32 | 37 | Male | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, H.; Fujishima, F.; Komoto, I.; Imamura, M.; Hijioka, S.; Hara, K.; Yatabe, Y.; Kudo, A.; Masui, T.; Tsuchikawa, T.; et al. Somatostatin Receptor 2 Expression Profiles and Their Correlation with the Efficacy of Somatostatin Analogues in Gastrointestinal Neuroendocrine Tumors. Cancers 2022, 14, 775. https://doi.org/10.3390/cancers14030775
Watanabe H, Fujishima F, Komoto I, Imamura M, Hijioka S, Hara K, Yatabe Y, Kudo A, Masui T, Tsuchikawa T, et al. Somatostatin Receptor 2 Expression Profiles and Their Correlation with the Efficacy of Somatostatin Analogues in Gastrointestinal Neuroendocrine Tumors. Cancers. 2022; 14(3):775. https://doi.org/10.3390/cancers14030775
Chicago/Turabian StyleWatanabe, Hirofumi, Fumiyoshi Fujishima, Izumi Komoto, Masayuki Imamura, Susumu Hijioka, Kazuo Hara, Yasushi Yatabe, Atsushi Kudo, Toshihiko Masui, Takahiro Tsuchikawa, and et al. 2022. "Somatostatin Receptor 2 Expression Profiles and Their Correlation with the Efficacy of Somatostatin Analogues in Gastrointestinal Neuroendocrine Tumors" Cancers 14, no. 3: 775. https://doi.org/10.3390/cancers14030775
APA StyleWatanabe, H., Fujishima, F., Komoto, I., Imamura, M., Hijioka, S., Hara, K., Yatabe, Y., Kudo, A., Masui, T., Tsuchikawa, T., Sakamoto, K., Shiga, H., Nakamura, T., Nakaya, N., Motoi, F., Unno, M., & Sasano, H. (2022). Somatostatin Receptor 2 Expression Profiles and Their Correlation with the Efficacy of Somatostatin Analogues in Gastrointestinal Neuroendocrine Tumors. Cancers, 14(3), 775. https://doi.org/10.3390/cancers14030775