
Treatment with Idelalisib in Patients with Relapsed or Refractory Follicular Lymphoma: The Observational Italian Multicenter FolIdela Study

 , ,
, ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient’s Characteristics
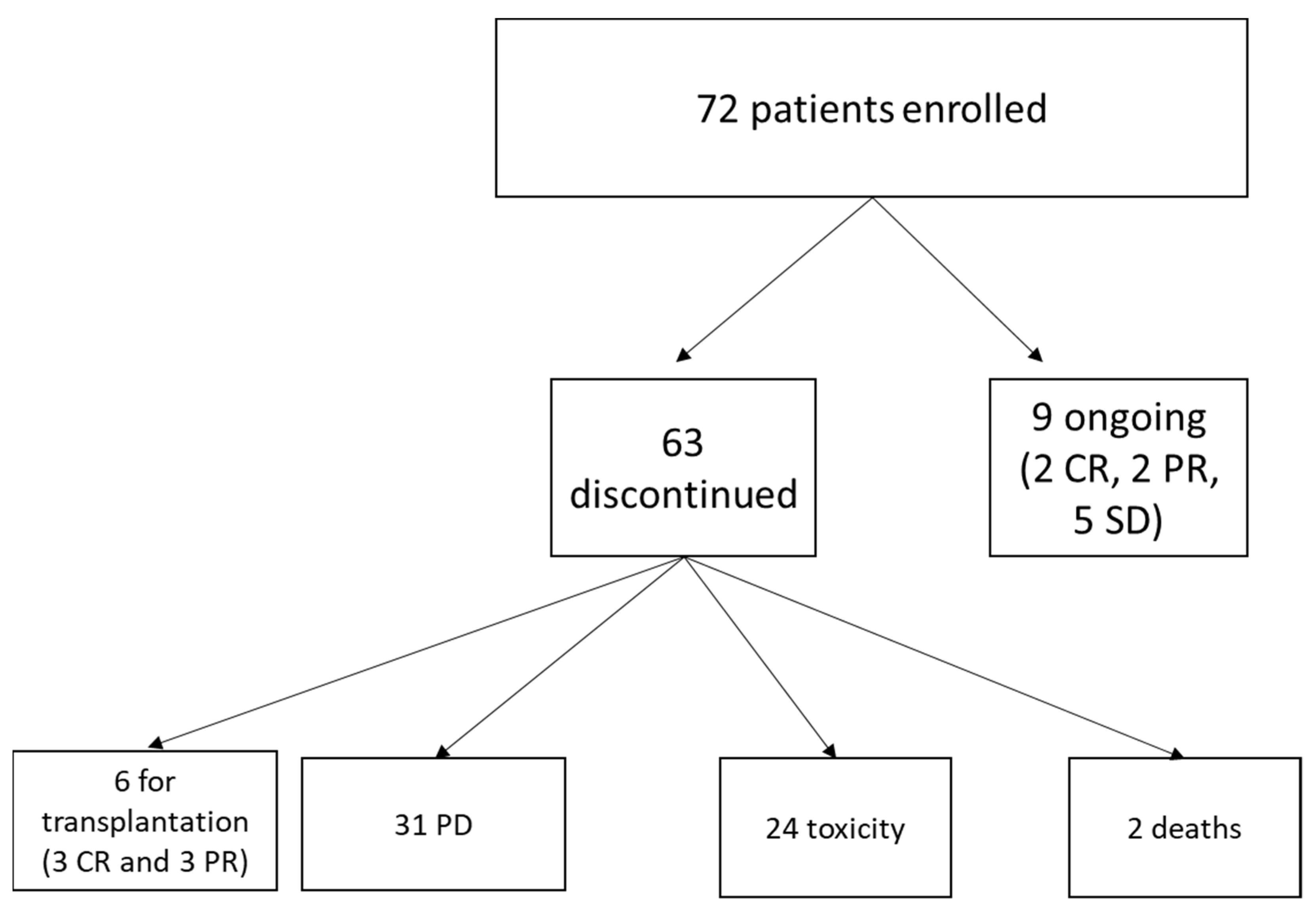
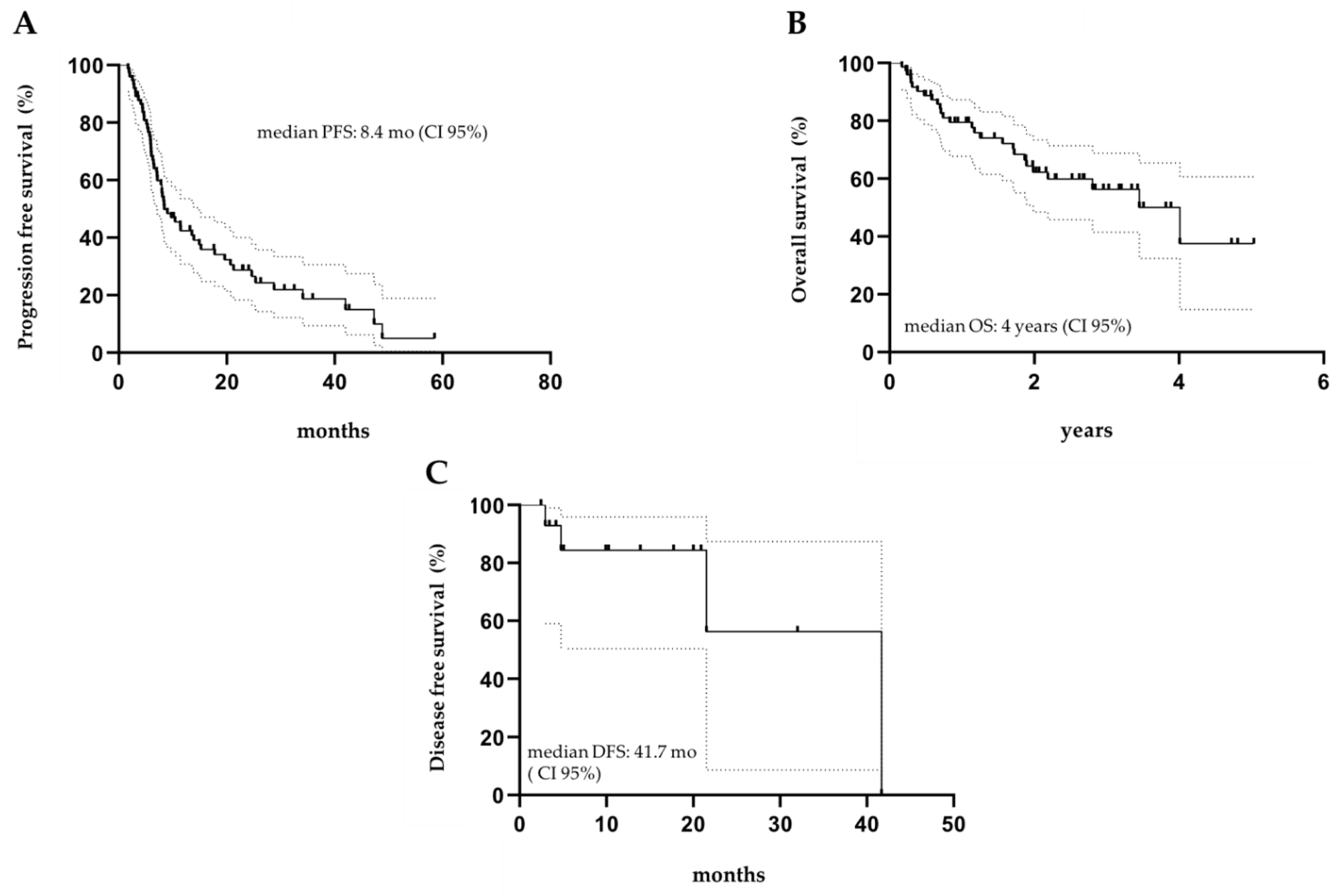
3.2. Efficacy and Outcomes
3.3. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamusrine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open label, multicenter, randomized, phase 3, non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef]
- Flinn, I.W.; van der Jagt, R.; Kahl, B.; Wood, P.; Hawkins, T.; MacDonald, D.; Simpson, D.; Kolibaba, K.; Issa, S.; Chang, J.; et al. First-Line Treatment of Patients With Indolent Non-Hodgkin Lymphoma or Mantle-Cell Lymphoma With Bendamustine Plus Rituximab Versus R-CHOP or R-CVP: Results of the BRIGHT 5-Year Follow-Up Study. J. Clin. Oncol. 2019, 37, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Marcus, R.; Davies, A.; Ando, K.; Klapper, W.; Opat, S.; Owen, C.; Phillips, E.; Sangha, R.; Schlag, R.; Seymour, J.F.; et al. Obinutuzumab for the First-Line Treatment of Follicular Lymphoma. N. Engl. J. Med. 2017, 377, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Moccia, A.A.; Taverna, C.; Schär, S.; Vanazzi, A.; Rondeau, S.; Hitz, F.; Mingrone, W.; Pabst, T.; Cevreska, L.; Del Giglio, A.; et al. Prolonged rituximab maintenance in follicular lymphoma patients: Long-term results of the SAKK 35/03 randomized trial. Blood Adv. 2020, 4, 5951–5957. [Google Scholar] [CrossRef] [PubMed]
- Kothari, J.; Peggs, K.S.; Bird, A.; Thomson, K.J.; Morris, E.; Virchis, A.E.; Lambert, J.; Goldstone, A.H.; Linch, D.C.; Ardeshna, K.M. Autologous stem cell transplantation for follicu- lar lymphoma is of most benefit early in the disease course and can result in durable remis- sions, irrespective of prior rituximab exposure. Br. J. Haematol. 2014, 165, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehn, L.H.; Chua, N.; Mayer, J.; Dueck, G.; Trněný, M.; Bouabdallah, K.; Fowler, N.; Delwail, V.; Press, O.; Salles, G.; et al. Obinutuzumab plus bendamustine versus bendamustine monotherapy in patients with rituximab-refractory indolent non-Hodgkin lymphoma (GADOLIN): A randomised, controlled, open-label, multicentre, phase 3 trial. Lancet Oncol. 2016, 17, 1081–1093. [Google Scholar] [CrossRef]
- Leonard, J.P.; Trneny, M.; Izutsu, K.; Fowler, N.H.; Hong, X.; Zhu, J.; Zhang, H.; Offner, F.; Scheliga, A.; Nowakowski, G.S.; et al. AUGMENT Trial Investigators. AUGMENT: A Phase III Study of Lenalidomide Plus Rituximab Versus Placebo Plus Rituximab in Relapsed or Refractory Indolent Lymphoma. J. Clin. Oncol. 2019, 37, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.B.; Bondly, C.; Micallef, I.N. Ibritumomab tiuxetan for non-Hodgkin’s lymphoma. Expert Rev. Anticancer Ther. 2006, 6, 861. [Google Scholar] [CrossRef] [PubMed]
- Gopal, A.K.; Kahl, B.S.; de Vos, S.; Wagner-Johnston, N.D.; Schuster, S.J.; Jurczak, W.J.; Flinn, I.W.; Flowers, C.R.; Martin, P.; Viardot, A.; et al. PI3Kδ inhibition by idelalisib in patients with relapsed indolent lymphoma. N. Engl. J. Med. 2014, 370, 1008–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhaesebroeck, B.; Guillermet-Guibert, J.; Graupera, M.; Bilanges, B. The emerging mechanisms of isoform-specific PI3K signalling. Nat. Rev. Mol. Cell. Biol. 2010, 11, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Durand, C.A.; Hartvigsen, K.; Fogelstrand, L.; Kim, S.; Iritani, S.; Vanhaesebroeck, B.; Witztum, J.L.; Puri, K.D.; Gold, M.R. Phosphoinositide 3-kinase p110 delta regulates natural antibody production, marginal zone and B-1 B cell function, and autoantibody responses. J. Immunol. 2009, 183, 5673–5684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lannutti, B.J.; Meadows, S.A.; Herman, S.E.; Kashishian, A.; Steiner, B.; Johnson, A.J.; Byrd, J.C.; Tyner, J.W.; Loriaux, M.M.; Deininger, M.; et al. CAL-101, a p110delta selective phosphatidylinositol-3-kinase inhibitor for the treatment of B-cell malignancies, inhibits PI3K signaling and cellular viability. Blood 2011, 117, 591–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graf, S.A.; Gopal, A.K. Idelalisib for the treatment of non-Hodgkin lymphoma. Expert. Opin. Pharm. 2016, 17, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Wagner-Johnston, N.D.; Schuster, S.J.; deVos, S.; Salles, G.; Jurczak, W.J.; Flowers, C.R.; Viardot, A.; Flinn, I.W.; Martin, P.; Xing, G.; et al. Outcomes of patients with up to 6 years of follow-up from a phase 2 study of idelalisib for relapsed indolent lymphomas. Leuk. Lymphoma 2021, 62, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Salles, G.; Schuster, S.J.; de Vos, S.; Wagner-Johnston, N.D.; Viardot, A.; Blum, K.A.; Flowers, C.R.; Jurczak, W.J.; Flinn, I.W.; Kahl, B.S.; et al. Efficacy and safety of idelalisib in patients with relapsed, rituximab- and alkylating agent-refractory follicular lymphoma: A subgroup analysis of a phase 2 study. Haematologica 2017, 102, e156–e159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyre, T.A.; Osborne, W.L.; Gallop-Evans, E.; Ardeshna, K.M.; Kassam, S.; Sadullah, S.; Sidra, G.; Culligan, D.; Arumainathan, A.; Shankara, P.; et al. Results of a multicentre UK-wide compassionate use programme evaluating the efficacy of idelalisib monotherapy in relapsed, refractory follicular lymphoma. Br. J. Haematol. 2018, 181, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.T.; Tian, F.; Flowers, N.; Przepiorka, D.; Wang, R.; Jung, T.H.; Kessler, Z.; Woods, C.; Kim, B.; Miller, B.W.; et al. Idelalisib for Treatment of Relapsed Follicular Lymphoma and Chronic Lymphocytic Leukemia: A Comparison of Treatment Outcomes in Clinical Trial Participants vs Medicare Beneficiaries. JAMA Oncol. 2020, 6, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. International Harmonization Project on Lymphoma. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Sellner, L.; Schetelig, J.; Koster, L.; Choi, G.; Blaise, D.; Beelen, D.; Schianca, F.C.; Passweg, J.; Schanz, U.; Gyan, E.; et al. Idelalisib exposure before allogeneic stem cell transplantation in patients with follicular lymphoma: An EBMT survey. Bone Marrow Transpl. 2020, 55, 2335–2338. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Present | Salles et al. |
|---|---|---|
| Paper (n = 72) | (n = 72) | |
| Median age at diagnosis, years (range) | 57.2 (24.5–82.2) | NA |
| Median age, years (range) | 63.0 (36.4–84.7) | 62 (33.0–84.0) |
| Sex (male), n (%) | 47 (65.3) | 39 (54.2) |
| ECOG < 1, n (%) | 68 (94.4) | 66 (91.7) |
| Stage at diagnosis, n (%) | ||
| I/II | 8 (11.2) | 12 (16.7) |
| III/IV | 64 (88.8) | 60 (83.3) |
| Bone marrow involvement, n (%) | 40 (55.6) | NA |
| LDH > UNL, n (%) | 24 (33.3) * | 21 (29.2) ° |
| FLIPI > 2, n (%) | 41 (56.9) | 57 (79.2) |
| Follicular lymphoma grade 3a, n (%) | 13 (18.1) | 12 (16.7) |
| Median of previous therapy, n (range) | 3 (1–10) | 4 (2–12) |
| Previous ASCT, n (%) | 23 (31.9) | 12 (16.7) |
| Baseline neutropenia | 10 (13.9) | 8 (11.1) |
| Baseline anemia | 9 (12.5) | 8 (11.1) |
| Baseline thrombocytopenia | 7 (9.7) | 5 (6.9) |
| Median time since diagnosis, years (range) | 5.8 (0.5–20) | 4.7 (0.8–18.4) |
| Median time since last relapse, months (range) | 1.6 (0.2–22.9) | NA |
| Refractory (≤6 mo) to the first line of therapy, n (%) | 20 (27.8) | NA |
| Refractory (≤6 mo) to most recent therapy, n (%) | 15 (20.8) | 62 (86.1) |
| Relapsed (>6 mo) to most recent therapy, n (%) | 57 (79.1) | 10 (13.8) |
| Treatment disposition at time of data cutoff, n (%) | ||
| Ongoing | 3 (4.2) | 7 (9.7) |
| Discontinued: | ||
| PD | 31 (43) | 38 (52.8) |
| AE | 24 (33.3) | 15 (20.8) |
| Investigator request | 6 (8.3) § | 4 (5.6) £ |
| Death | 2 (2.7) | 5 (6.9) |
| Withdrew consent | 0 (0) | 3 (4.2) |
| Event or Abnormality, n (%) * | Any | Grade ≥ 3 |
|---|---|---|
| Diarrhea | 10 (23.3) | 6 (13.9) |
| Upper respiratory tract infection | 7 (16.3) | 6 (13.9) |
| Increased ALT/AST | 6 (13.9) | 3 (6.9) |
| Rash | 4 (9.3) | 1 (2.3) |
| Pneumonia | 3 (6.9) | 3 (6.9) |
| Neutropenia | 3 (6.9) | 2 (4.7) |
| Anemia | 3 (6.9) | 3 (6.9) |
| Thrombocytopenia | 2 (4.7) | 2 (4.7) |
| Mucositis | 2 (4.7) | 2 (4.7) |
| Myelodysplastic syndrome | 1 (2.3) | 1 (2.3) |
| Pyrexia | 1 (2.3) | - |
| Vomiting | 1 (2.3) | 1 (2.3) |
| Total | 43 | 30 |
| Event or Abnormality | Grade | Onset Time (Cycle) | Permanent Discontinuation | Time of Discontinuation (Cycle) |
|---|---|---|---|---|
| Vomiting | 1 | 5 | No | - |
| Increased ALT/AST | 3 | 2 | Yes | 4 |
| Pneumonia | 3 | 2 | Yes | 9 |
| Diarrhea | 3 | 3 | Yes | 3 |
| Pneumonia | 3 | 2 | Yes | 4 |
| Upper respiratory tract infection | 3 | 2 | Yes | 4 |
| Diarrhea | 3 | 7 | Yes | 12 |
| Upper respiratory tract infection | 2 | 3 | Yes | 5 |
| Increased ALT/AST | 3 | 2 | No | - |
| Diarrhea | 3 | 3 | Yes | 4 |
| Neutropenia | 3 | 2 | No | - |
| Upper respiratory tract infection | 3 | 4 | Yes | 6 |
| Rash | 3 | 22 | Yes | 40 |
| Pneumonia | 3 | 2 | Yes | 3 |
| Upper respiratory tract infection | 2 | 15 | Yes | 38 |
| Anemia | 2 | 14 | No | - |
| Upper respiratory tract infection | 2 | 3 | Yes | 33 |
| Increased ALT/AST | 2 | 2 | Yes | 5 |
| Increased ALT/AST | 2 | 2 | Yes | 4 |
| Diarrhea | 3 | 4 | Yes | 7 |
| Rash | 2 | 5 | No | - |
| Increased ALT/AST | 2 | 5 | Yes | 6 |
| Increased ALT/AST | 3 | 2 | Yes | 3 |
| Diarrhea | 3 | 3 | No | - |
| Mucositis | 3 | 2 | No | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casadei, B.; Argnani, L.; Broccoli, A.; Patti, C.; Stefani, P.M.; Cuneo, A.; Margiotta Casaluci, G.; Visco, C.; Gini, G.; Pane, F.; et al. Treatment with Idelalisib in Patients with Relapsed or Refractory Follicular Lymphoma: The Observational Italian Multicenter FolIdela Study. Cancers 2022, 14, 654. https://doi.org/10.3390/cancers14030654
Casadei B, Argnani L, Broccoli A, Patti C, Stefani PM, Cuneo A, Margiotta Casaluci G, Visco C, Gini G, Pane F, et al. Treatment with Idelalisib in Patients with Relapsed or Refractory Follicular Lymphoma: The Observational Italian Multicenter FolIdela Study. Cancers. 2022; 14(3):654. https://doi.org/10.3390/cancers14030654
Chicago/Turabian StyleCasadei, Beatrice, Lisa Argnani, Alessandro Broccoli, Caterina Patti, Piero Maria Stefani, Antonio Cuneo, Gloria Margiotta Casaluci, Carlo Visco, Guido Gini, Fabrizio Pane, and et al. 2022. "Treatment with Idelalisib in Patients with Relapsed or Refractory Follicular Lymphoma: The Observational Italian Multicenter FolIdela Study" Cancers 14, no. 3: 654. https://doi.org/10.3390/cancers14030654
APA StyleCasadei, B., Argnani, L., Broccoli, A., Patti, C., Stefani, P. M., Cuneo, A., Margiotta Casaluci, G., Visco, C., Gini, G., Pane, F., D’Alò, F., Luzi, D., Cantonetti, M., Pozzi, S., Musuraca, G., Rosignoli, C., Arcari, A., Kovalchuk, S., Tani, M., ... Zinzani, P. L. (2022). Treatment with Idelalisib in Patients with Relapsed or Refractory Follicular Lymphoma: The Observational Italian Multicenter FolIdela Study. Cancers, 14(3), 654. https://doi.org/10.3390/cancers14030654