

Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
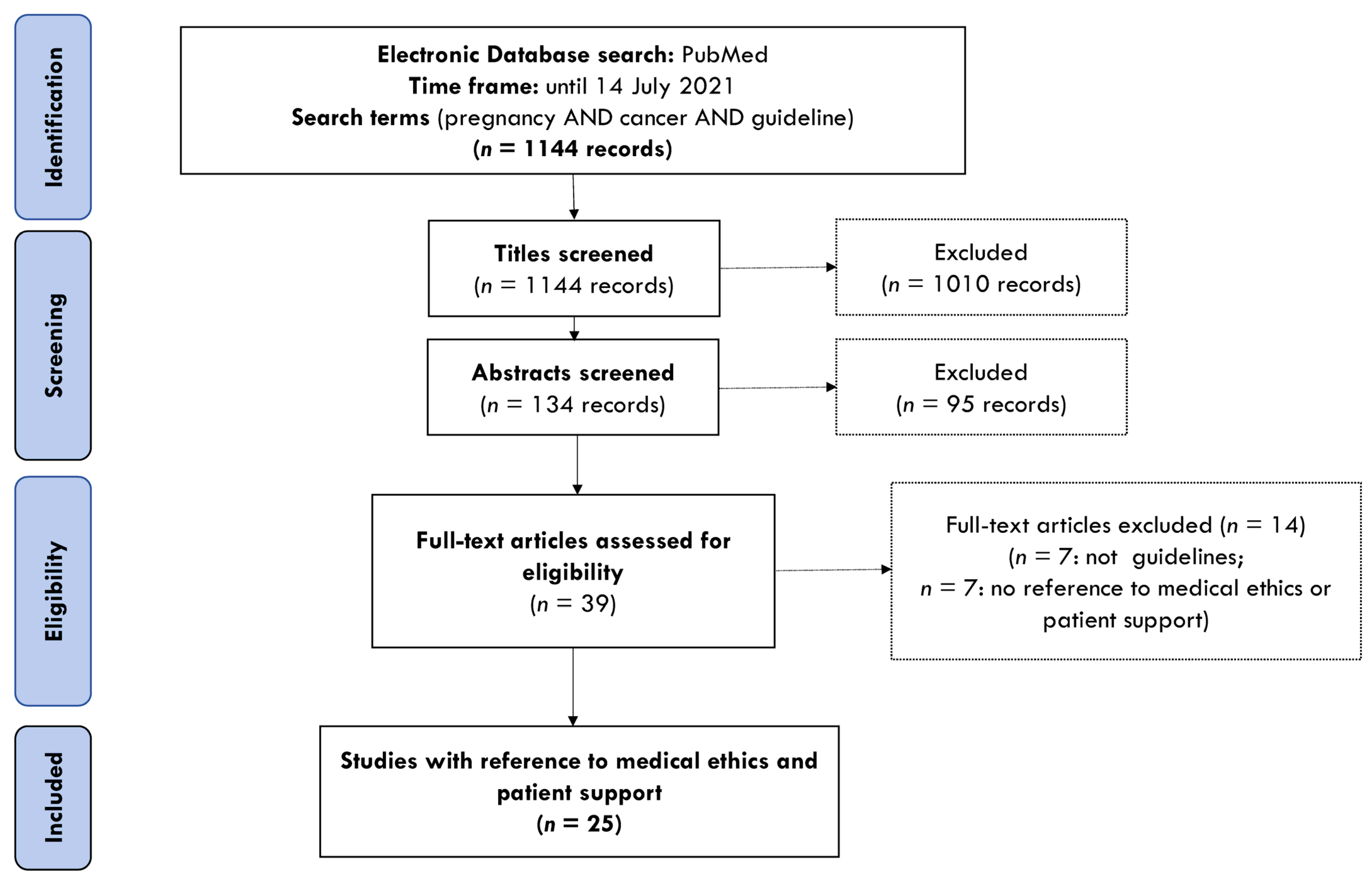
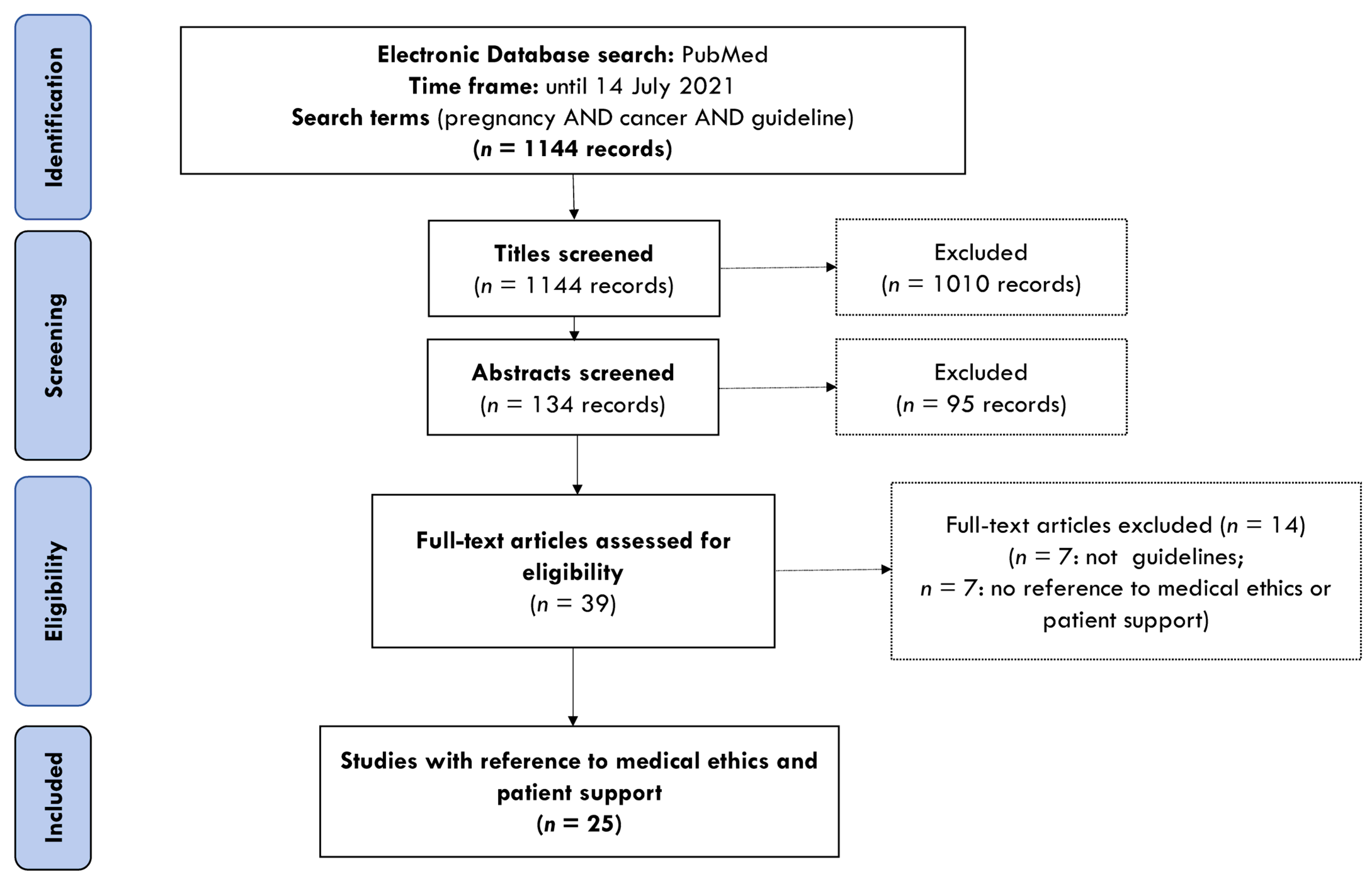
2. Materials and Methods
3. Results

{kind=link}
| Principles | Expressions of the Principle | Guidelines Mentioning This Principle |
|---|---|---|
| Autonomy | ||
| Enabling patients to take informed decisions | Providing patients with the information about available treatment options, including risks and benefits for the mother and the fetus | [22,23,26,27,29,30,31,32,33,34,35,36,37,38,39] |
| Respect for patient’s autonomy | Involving the patient in a decision-making process by informing her about the options and taking patient’s wishes into account when determining the disease management plan. | [21,22,23,27,28,32,33,34,35,36,37,38,39,43] |
| Acknowledging the respect for relational autonomy | Involving the patient and her partner/family in a decision-making process by informing about the options and taking patient wishes into account when determining the disease management plan. | [22,28,30,37,38,40,41,42,43,44] |
| Beneficence | ||
| Balancing maternal and fetal beneficence | Considering maternal health outcomes and fetal risks when determining the disease management plan. | [23,26,29,32,33,35,37,38,40,45] |
| Maternal beneficence | Giving preference to maternal health outcomes over fetal risks, if optimal balance for both is not possible. | [21,24,26,44] |
| Fetal beneficence | Giving more weight for protecting the fetus and allowing pregnancy to continue but offering support for the pregnant patient. | [25] |
| Vulnerability | ||
| Protection of the vulnerable | Proving care and support for those who might be under-represented or not able to defend their position. Could include pregnant women, cancer patients, unborn children/fetuses, neonates, children. | [24,29] |
| Justice | ||
| Reasonable resource allocation | Following a reasonable course of action based on current knowledge, available resources and the needs of the patient to deliver the effective and safe medical care. | [26] |
| No biomedical ethics principles/concepts referenced | ||
| No references to patient care outside clinical aspects | Focuses on providing clinical guidance without making suggestions how patient care should be handled in a light of ethics. | [46,47,48,49,50,51,52] |
| Reference; Organization | Guideline Description | Management Recommendation | Patient Support | Biomedical Ethics Concepts/Principles Referenced in the Guideline |
|---|---|---|---|---|
| Reed et al., 2021 [33]; British Gynaecological Cancer Society (BGCS) | Attempts to cover management of invasive cervical cancer reflecting diagnosis and imaging including new imaging and sentinel lymph node biopsies. | Multidisciplinary team, evidence-based medicine | Feeling informed and in control through the provision of information can lead to women feeling engaged and active in their treatment decisions leading to better patient outcomes. | Balancing maternal and fetal beneficence, autonomy |
| Amant et al., 2019 [40]; International Network on Cancer, Infertility and Pregnancy (INCIP), third international consensus meeting | Promotes effective management of pregnant women with gynecological cancers and their offspring. | Multidisciplinary team, evidence-based medicine | Pregnant cancer patients deserve a careful continuous assessment and support of their psychological wellbeing on a routine basis with follow-up in the postpartum period. Counselling should be offered to both the affected woman and her partner. | Balancing maternal and fetal beneficence, relational autonomy |
| Cibula et al., 2018 [32]; The European Society of Gynaecological Oncology (ESGO), the European Society for Radiotherapy and Oncology (ESTRO), and the European Society of Pathology (ESP) |
Provides clinically relevant and evidence-based guidelines in order to improve the quality of care for women with cervical cancer across Europe and worldwide |
Primary aims of recommended treatment plan are oncological safety of the pregnant woman, as well as survival without additional morbidity of the fetus. | Every patient diagnosed with CCIP must be counselled by a multidisciplinary team. This team should consist of experts in the fields of gynecologic oncology, neonatology, obstetrics, anesthesiology, radiation oncology, medical oncology, psycho-oncology, and, if requested, theology or ethics. |
Multidisciplinary team recommends an individual consensual treatment plan according to patient’s intention, tumor stage, and gestational age of pregnancy at cancer diagnosis (respect to patients’ autonomy, balancing maternal and fetal beneficence) |
| Coccia et al., 2018 [45]; National Comprehensive Cancer Network | Focuses on treatment and management considerations for Adolescent and Young Adult (AYA) patients with cancer. | Women diagnosed with cancer during pregnancy require individualized treatment from a multidisciplinary team involving medical, surgical, and radiation oncologists, gynecologic oncologists, obstetricians, and perinatologists as appropriate. In addition to the disease characteristics in pregnant women, the gestational age of the fetus is a significant factor in the selection of treatment. | Referral to tertiary cancer centers with expertise in the diagnosis of cancer during pregnancy and maternal–fetal medicine and knowledge of the physiologic changes that occur during pregnancy should be strongly encouraged. Offer psychosocial support and counselling to help alleviate distress. | The goals of controlling maternal cancer and providing the fetus the best chance for survival with normal development (treatment recommendations suggest balancing maternal and fetal beneficence) |
| Alexander et al., 2017 [35]; American Thyroid Association (ATA) | Informs clinicians, patients, researchers, and health policy makers on published evidence relating to the diagnosis and management of thyroid disease in women during pregnancy, preconception, and the postpartum period. Offers strength of evidence to support recommendations. | In all women of childbearing age who are thyrotoxic, the possibility of future pregnancy should be discussed. Women with GD seeking future pregnancy should be counselled regarding the complexity of disease management during future gestation, including the association of birth defects with ATD use. ATD dose should be reduced to protect the fetus. | Preconception counselling should review the risks and benefits of all treatment options and the patient’s desired timeline to conception. | A careful balance is required between making a definitive diagnosis and instituting treatment while avoiding interventions that may adversely impact the mother, the health of the fetus, or the maintenance of the pregnancy. Surgery should be performed in the second trimester in order to minimize complications to both the mother and fetus. (balancing maternal and fetal beneficence) |
| Pallera et al., 2017 [37]; National Comprehensive Cancer Network (NCCN) | Provides recommendations for the management of chronic-phase and advanced-phase Chronic Myeloid Leukemia (CML) in adult patients. | Clinical care teams should be prepared to address issues relating to fertility and pregnancy, as well as counsel these patients about the potential risks and benefits of treatment discontinuation and possible resumption of tyrosine kinase inhibitor (TKI) therapy should CML recur during pregnancy. | Before attempting pregnancy, women and their partners should be counselled that no guidelines exist regarding how best to monitor CML during pregnancy, nor how best to manage progressive disease should it occur during pregnancy. Conception while on active TKI therapy is strongly discouraged because of the risk of fetal abnormalities. | Each woman needs to make the decision that fits her best after an in-depth discussion regarding relapse rates off TKI therapy and treatment if needed during pregnancy, and clinical care teams should be supportive of her choice, whatever that choice may be; The potential risk/benefit balance should be carefully evaluated in terms of maternal health and fetal risk before initiation of treatment during pregnancy, especially during the first trimester. (respect for patient’s autonomy; balancing maternal and fetal beneficence) |
| Lishner et al., 2016 [39]; International Consensus Meeting of Prenatal Hematologic Malignancies | Provides guidelines for clinical management of hematologic cancers during the perinatal period, which were developed by a multidisciplinary team including an experienced hematologist/oncologist, a high-risk obstetrics specialist, a neonatologist, and experienced nurses, social workers, and psychologists. | A multidisciplinary team—including, at minimum, an experienced hematologist/oncologist, a high-risk obstetrics specialist, a neonatologist, as well as experienced nurses, social workers, and psychologists, providing close follow-up—is critical to ensuring optimal maternal and fetal outcomes; Diagnosis followed by appropriate staging is essential and should not be delayed due to pregnancy; An overarching goal in the care of all pregnant patients with non-Hodgkin lymphoma (NHL) is delivery at term. | An informed decision to treat needs to be made with the patient, using dosimetry analyses provided by the medical physicist. | The decision to administer antenatal therapy is based on several factors, such as type of non-Hodgkin lymphoma (NHL), gestational age, and patient preference; Pregnancy termination recommended in early pregnancy if aggressive treatment is needed. (balancing maternal and fetal beneficence) |
| Bluemel et al., 2015 [26]; written and approved by the European Association of Nuclear Medicine (EANM), discussed by distinguished experts from the EANM Oncology Committee, national nuclear medicine societies, the European Society of Surgical Oncology (ESSO) and the European Association for Research and Treatment of Cancer (EORTC) melanoma group. The document has been endorsed by the Society of Nuclear Medicine and Molecular Imaging (SNMMI). | Offers practice guidelines for nuclear medicine practitioners to help providing high-quality lymphatic mapping for the care of melanoma patients. | Management by multidisciplinary team; Risks and benefits of the procedures should be carefully discussed with the gynecologist; Radiolocalization of sentinel lymph nodes (SLNs) in patients with melanoma is associated with low levels of radiation exposure. While lymphatic mapping is not contraindicated in pregnant patients, it is common to halve the dose activity and same-day surgery is preferred. |
The resources and facilities available for patient care may vary from one country to another and from one medical institution to another. Pregnant patients may be offered sentinel lymph node biopsy (SLNB) after careful counselling regarding the safety and efficacy of the procedure. | Practitioner will follow a reasonable course of action based on current knowledge, available resources and the needs of the patient to deliver the effective and safe medical care. (respect for patient’s autonomy; balancing maternal and fetal beneficence; justice) |
| Ali et al., 2015 [23]; UK-based medical practitioners with expertise in acute myeloid leukaemia (AML), reviewed by Haemato-oncology Task Force of the British Committee for Standards in Haematology (BCSH), British Society of Haematology (BSH), UK AML National Cancer Research Network (NCRN) | Offers a uniformed consensus which, due to scarcity of the literature, is mainly based on expert opinion than trials for treating AML patients. Includes grade of evidence for all clinical recommendations | Management by multidisciplinary team; Pregnant patients with AML should be treated without delay after full and frank discussion; Beyond 32 weeks gestation it might be reasonable to deliver the fetus before chemotherapy. | The women should be fully informed about the diagnosis, treatment of the disease and possible complications; Reasons for and against elective termination should be discussed with a patient; Offer parents reassurance on baby’s health by performing tests and follow-up during infancy. | Considerations should be given to the health of both mother and fetus and informed wishes of the patient (enabling patients to take informed decisions, respect for patient’s autonomy; balancing maternal and fetal beneficence) |
| Follows et al., 2014 [21]; UK-based medical experts and patients’ representatives; revised by Haemato-oncology Task Force of the British Committee for Standards in Haematology (BCSH) | The guideline for first line management of classical Hodgkin lymphoma | The priority must be the health of the mother and, ideally, management should be in conjunction with an obstetrician experienced in high-risk pregnancies | Patient’s personal priorities should be taken into consideration when making treatment decisions | Attention to patient’s personal wishes (respect for patient’s autonomy); Maternal health and wellbeing should prevail (maternal beneficence) |
| Amant et al., 2014 [24]; European Society of Gynecological Oncology (ESGO) task force “Cancer in Pregnancy” in concert with other international experts | Provides timely and effective guidance for pregnant women and health care providers to optimize maternal treatment and fetal protection and to promote effective management of the mother, fetus, and neonate when administering potentially teratogenic medications in gynecological malignancies | To maximize the maternal outcome, cancer treatment should follow a standard treatment protocol as for non-pregnant patients; Despite limited evidence-based information, cancer treatment during pregnancy can succeed; Iatrogenic prematurity should be avoided; State-of-the-art treatment should be provided for this vulnerable population to preserve maternal and fetal prognosis. | Individualization of the treatment and effective psychological support is imperative to provide throughout the pregnancy period | Maximizing maternal outcome (maternal beneficence) Best treatment for vulnerable population [pregnant women with cancer] (protection of the vulnerable) |
| Peccatori et al., 2013 [41]; European Society of Medical Oncology (ESMO), endorsed by Japanese Society of medical Oncology (JSMO) | Provides Clinical Practice Guidelines for managing patients diagnosed with cancer during pregnancy and provide guidance on fertility considerations for women desiring pregnancy following cancer diagnosis (breast, cervical, lung cancer, leukemia and other tumors) | Referral to institution with expertise; Multidisciplinary team; Standard chemo might not be feasible in all cases; Target full-term delivery whenever possible; Pregnancy termination strongly discouraged | Involving a partner and family in decision-making process; Multidisciplinary care and counselling | Partner and family involvement in decision-making (respect for relational autonomy) |
| Koren et al., 2013 [44]; Chemotherapy During Pregnancy Working Group, approved by the Society of Obstetricians and Gynaecologists of Canada (SOGC) | Reflects clinical and scientific advances and offers recommendations concerning chemotherapy use in pregnant women and women of child-bearing age | It is important to balance maternal and fetal risks; Decisions should be made individually for each patient; Multi-disciplinary team, including physicians and social workers, psychologists, spiritual advisors | Discuss the available options with pregnant patient and her family | Partner and family involvement in decision-making (respect for relational autonomy); Maternal health and wellbeing should prevail (maternal beneficence) |
| Cardoso et al., 2012 [27]; European Society of Breast Cancer Specialists (EUSOMA) | Position paper, recommendations for treating young women with breast cancer | Pregnancy after breast cancer should not in principle be discouraged | Issues of body image, sexuality, fertility and lactation must be discussed with young women with breast cancer; Counselling for family planning and contraception; Involve the partner if present | Informing the patient about treatment effects and family planning (enabling patients to take informed decisions; respect for patient’s autonomy); Partner involvement in decision-making (respect for relational autonomy) |
| Dauer et al., 2012 [22]; Society of Interventional Radiology and the Cardiovascular and Interventional Radiology Society of Europe, endorsed by the Canadian Interventional Radiology Association | Intends to assist interventionalists and their staff in managing and counselling pregnant patients who need fluoroscopically or CT-guided interventional procedures | Interventions should be justified with the aim for doing more good than harm; Concern about the possible side effects of ionizing radiation exposure on the conceptus [fetus] should not preclude medically indicated diagnostic or interventional x-ray procedures when the medical benefit for the mother is justifiable; Conceptus doses lower than 100 mGy should not be considered a reason for terminating a pregnancy | Pregnant patients should be counselled based on sound information about the risks of radiation exposure; If possible pre and post procedure counselling should take place involving the mother and the father | Provide counselling support to patients (enabling patients to take informed decisions); Abortion is an individual decision affected by many factors (respect for patient’s autonomy); Partner involvement (respect for relational autonomy [indirect reference]) |
| De Groot et al., 2012 [34]; Endocrine Society Clinical Practice Guideline (US), reviewed and commented on by members of The Endocrine Society, Asia and Oceania Thyroid Association, and the Latin American Thyroid Society—Section 5. Thyroid Nodules and Cancer | Updates the guidelines for the management of thyroid dysfunction during pregnancy and postpartum published previously | No clear evidence that pregnancy worsens the survival of pregnant patient | Information for the patient making the decision about breastfeeding | Provide information for the patient (enabling patients to take informed decisions; respect for patient’s autonomy [indirect reference]) |
| Royal College of Ob/Gyn, 2011 [28]; Royal College of Obstetricians & Gynaecologists | Provides clinical guidance to health professionals caring for women of childbearing age with a diagnosis or history of breast cancer. Green-top guideline No. 12 | Suggests auditing the referrals and outcomes | People with cancer should be fully informed of potential gonadotoxicity before treatment, and specialist psychological support and counselling should be available; Involve a partner in a discussion with a multidisciplinary team | Informing the patient about treatment effects (respect for patient’s autonomy); Partner and family involvement in decision-making (respect for relational autonomy) |
| Amant et al., 2010 [29]; an international expert Panel | Provides guidance for clinicians about the diagnosis, staging and treatment of breast cancer occurring during an otherwise uncomplicated pregnancy | Serious consideration should be given to continuing of pregnancy whilst treating cancer; Delivery should not be induced before 37 weeks as morbidity mainly associated with prematurity; Treatment should adhere as closely as possible to standard protocols; Breastfeeding shortly after chemotherapy not recommended | Multidisciplinary team should provide patient with clear explanation of treatment options | Seriously consider continuing of pregnancy whilst treating cancer (balancing maternal and fetal beneficence, protection of the vulnerable [indirect reference]); Provide information for the patient (enabling patients to take informed decisions) |
| Marsden et al., 2010 [36]; endorsed or had an input from U.K. Melanoma Study Group, the British Association of Dermatologists, the British Association of Plastic, Reconstructive and Aesthetic Surgeons, the Royal College of Physicians, London, the Association of Cancer Physicians, the Royal College of Radiologists, London, the Royal College of Surgeons of England, the Royal College of Pathologists (pathology section only), the Royal College of General Practitioners, London, and the Department of Health | Guideline for management of cutaneous melanoma presents evidence-based guidance for treatment, with identification of the strength of evidence available at the time of preparation of the guidelines, and a brief overview of epidemiology, diagnosis, investigation and follow up. | Chemotherapy does not have survival benefit in IV stage; Melanoma can metastasize to the placenta and fetus more frequently which has poor prognosis for the mother and the baby | Social and family effects of developing recurrent melanoma during pregnancy or after birth are great. Counselling recommended. | Provide support, information and education to patients (enabling patients to take informed decisions; respect for patient’s autonomy) |
| Papini et al., 2010 [25]; Joint statement for clinical practice by Italian associations on thyroid cancer | Provides guidance to thyroid nodule and differentiated thyroid cancer management in pregnancy | Most tumors are slow growing and surgery after the delivery will not change the prognosis; Pregnancy should never be interrupted | Assurance about prognosis should be given to the affected patients | Never interrupting the pregnancy (fetal beneficence but also care and support for the expectant mother) |
| Pentheroudakis et al., 2010 [42]; European Society of Medical Oncology (ESMO) | Provides a guide with scientific levels of evidence for management of breast and cervical cancers, and melanoma | The optimal therapeutic strategy should be jointly chosen by the medical team, patient and family and will depend on gestational age, nature and stage of cancer, treatment options and patient wishes | All patients at risk of infertility who have not completed childbearing should discuss germ-line storage options with a medical team | Partner and family involvement in decision-making (respect for relational autonomy) |
| Amant et al., 2009 [38]; international experts in the field | Suggests models for treatment of gynecologic cancer in pregnancy | Randomized trials and prospective studies on cancer treatment during pregnancy are lacking; Multidisciplinary expertise should be available; It is advisable to engage the expertise of other members of the healthcare team such as psychologists, social and pastoral workers | Counselling both parents on the maternal prognosis and fetal risk is needed | The parents should be informed about the different treatment options and the possible consequences for the patient and the fetus (enabling patients to take informed decisions; respect for relational autonomy [indirect reference]); The prognosis, treatment modalities, gestational age, and patients’ preference are pivotal in the decision making process on treatment during pregnancy or termination of pregnancy (balancing maternal and fetal beneficence [indirect reference]; respect for patient’s autonomy) |
| Pentheroudakis et al., 2008 [43]; European society of Medical Oncology (ESMO) | Provides recommendations for diagnosis, treatment and follow-up surrounding cancer treatment, fertility preservation and cancer during pregnancy | Pregnancy termination is advised in the case of chemotherapy or radiotherapy administration during the first trimester, need for radical gynecologic surgery, poor maternal life expectancy | The optimal therapeutic strategy should be jointly chosen by the medical team, patient and family and will depend on gestational age, nature and stage of cancer, treatment options and patient wishes. | Inclusion of patient and family in decision-making (respect for relational autonomy [indirect reference]); considering patient’s wishes (respect for patient’s autonomy) |
| Loibl et al., 2006 [30]; Internal expert meeting | Offers guidelines on how to diagnose and treat women with breast carcinoma during pregnancy | Multidisciplinary approach is recommended including psychologist, social workers, and a chaplain; Ongoing psychological support during treatment and delivery should be available for the patient and her family | A supportive patient-physician relationship is required, as is close collaboration and feedback of all disciplines involved in the patient’s care, aiming to assist the patient and her partner towards achieving a true informed consent and commitment to treatment | Informing the patient about the options (enabling patients to take informed decisions); involving partner in consultations (respect for relational autonomy) |
| Helewa et al., 2002 [31]; Breast Disease Committee and Executive Committee and Council, Society of Obstetricians and Gynaecologists of Canada | Provides physicians with up-to-date, accurate information and recommendations regarding pregnancy and lactation impact on cancer risk, prognosis, risk of reoccurrence and feasibility of breastfeeding in women affected by breast cancer; and also offers counselling recommendations | Multidisciplinary approach should be taken; Patients should be counselled regarding the effect of proposed on the fetus and on overall maternal prognosis; Termination of pregnancy should be discussed, but patient should be counselled that prognosis is not altered by termination of pregnancy | Counselling support for breast cancer patients is advocated | Informing the patient about the options (enabling patients to take informed decisions) |
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cottreau, C.M.; Dashevsky, I.; Andrade, S.E.; Li, D.K.; Nekhlyudov, L.; Raebel, M.A.; Ritzwoller, D.P.; Partridge, A.H.; Pawloski, P.A.; Toh, S. Pregnancy-associated cancer: A U.S. Population-based study. J. Women’s Health 2019, 28, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Dalmartello, M.; Negri, E.; La Vecchia, C.; Scarfone, G.; Buonomo, B.; Peccatori, F.A.; Parazzini, F. Frequency of pregnancy-associated cancer: A systematic review of population-based studies. Cancers 2020, 12, 1356. [Google Scholar] [CrossRef] [PubMed]
- Maggen, C.; Wolters, V.E.R.A.; Cardonick, E.; Fumagalli, M.; Halaska, M.J.; Lok, C.A.R.; de Haan, J.; Van Tornout, K.; Van Calsteren, K.; Amant, F. Pregnancy and Cancer: The INCIP Project. Curr. Oncol. Rep. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs PD. World Population Prospects 2019. 2019. Available online: https://population.un.org/wpp/Download/Standard/Fertility/ (accessed on 15 July 2021).
- International Agency for Research on cancer. Breast. Globocan 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/20-Breast-fact-sheet.pdf (accessed on 15 July 2021).
- Hepner, A.; Negrini, D.; Hase, E.A.; Exman, P.; Testa, L.; Trinconi, A.F.; Filassi, J.R.; Francisco, R.P.V.; Zugaib, M.; O’Connor, T.L.; et al. Cancer during Pregnancy: The Oncologist Overview. World J. Oncol. 2019, 10, 28–34. [Google Scholar] [CrossRef]
- Heimovaara, J.H.; Boere, I.A.; de Haan, J.; van Calsteren, K.; Amant, F.; van Zuylen, L.; Lok, C.A.R.; Lok, C.A.R.; van Zuylen, L.; Boere, I.A.; et al. Ten-year experience of a national multidisciplinary tumour board for cancer and pregnancy in the Netherlands. Eur. J. Cancer 2022, 171, 13–21. [Google Scholar] [CrossRef]
- Wolters, V.; Heimovaara, J.; Maggen, C.; Cardonick, E.; Boere, I.; Lenaerts, L.; Amant, F. Management of pregnancy in women with cancer. Int. J. Gynecol. Cancer 2021, 31, 314–322. [Google Scholar] [CrossRef]
- Silverstein, J.; Post, A.L.; Chien, A.J.; Olin, R.; Tsai, K.K.; Ngo, Z.; Van Loon, K. Multidisciplinary Management of Cancer during Pregnancy. JCO Oncol. Pract. 2020, 16, 545–557. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Lambertini, M.; Scarfone, G.; Del Pup, L.; Codacci-Pisanelli, G. Biology, staging, and treatment of breast cancer during pregnancy: Reassessing the evidences. Cancer Biol. Med. 2018, 15, 6. [Google Scholar] [CrossRef]
- Abalo, K.D.; Rage, E.; Leuraud, K.; Richardson, D.B.; Le Pointe, H.D.; Laurier, D.; Bernier, M.-O. Early life ionizing radiation exposure and cancer risks: Systematic review and meta-analysis. Pediatr. Radiol. 2021, 51, 45–56. [Google Scholar] [CrossRef]
- Benoit, L.; Mir, O.; Vialard, F.; Berveiller, P. Cancer during Pregnancy: A Review of Preclinical and Clinical Transplacental Transfer of Anticancer Agents. Cancers 2021, 13, 1238. [Google Scholar] [CrossRef]
- Linkeviciute, A.; Buonomo, B.; Fazio, N.; Spada, F.; Peccatori, F.A. Discussing motherhood when the oncological prognosis is dire: Ethical considerations for physicians. ESMO Open 2020, 5, e000956. [Google Scholar] [CrossRef] [PubMed]
- Linkeviciute, A.; Notarangelo, M.; Buonomo, B.; Bellettini, G.; Peccatori, F.A. Breastfeeding after Breast Cancer: Feasibility, Safety, and Ethical Perspectives. J. Hum. Lact. 2020, 36, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Alpuim Costa, D.; Nobre, J.G.; de Almeida, S.B.; Ferreira, M.H.; Gonçalves, I.; Braga, S.; Pais, D. Cancer during Pregnancy: How to Handle the Bioethical Dilemmas?—A Scoping Review with Paradigmatic Cases-Based Analysis. Front. Oncol. 2020, 10, 598508. [Google Scholar] [CrossRef] [PubMed]
- Linkeviciute, A. Cancer during Pregnancy: A Framework for Ethical Care. 2017. Available online: https://air.unimi.it/handle/2434/449004#.YNNNbFT0ldg (accessed on 15 July 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 7th ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Rendtorff, J.D. Basic ethical principles in European bioethics and biolaw: Autonomy, dignity, integrity and vulnerability—towards a foundation of bioethics and biolaw. Med. Health Care Philos. 2002, 5, 235–244. [Google Scholar] [CrossRef] [PubMed]
- McDougall, R. Systematic reviews in bioethics: Types, challenges, and value. J. Med. Philos. 2014, 39, 89–97. [Google Scholar] [CrossRef]
- Follows, G.A.; Ardeshna, K.M.; Barrington, S.F.; Culligan, D.J.; Hoskin, P.J.; Linch, D.; Sadullah, S.; Williams, M.V.; Wimperis, J.Z. Guidelines for the first line management of classical Hodgkin lymphoma. Br. J. Haematol. 2014, 166, 34–49. [Google Scholar] [CrossRef]
- Dauer, L.T.; Thornton, R.H.; Miller, D.L.; Damilakis, J.; Dixon, R.G.; Marx, M.V.; Schueler, B.A.; Vañó, E.; Venkatesan, A.; Bartal, G.; et al. Radiation Management for Interventions Using Fluoroscopic or Computed Tomographic Guidance during Pregnancy: A Joint Guideline of the Society of Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe with Endorse. J. Vasc. Interv. Radiol. 2012, 23, 19–32. [Google Scholar] [CrossRef]
- Ali, S.; Jones, G.L.; Culligan, D.J.; Marsden, P.J.; Russell, N.; Embleton, N.D.; Craddock, C. Guidelines for the diagnosis and management of acute myeloid leukaemia in pregnancy. Br. J. Haematol. 2015, 170, 487–495. [Google Scholar] [CrossRef]
- Amant, F.; Halaska, M.J.; Fumagalli, M.; Dahl Steffensen, K.; Lok, C.; Van Calsteren, K.; Han, S.N.; Mir, O.; Fruscio, R.; Uzan, C.; et al. Gynecologic cancers in pregnancy: Guidelines of a second international consensus meeting. Int. J. Gynecol. Cancer 2014, 24, 394–403. [Google Scholar] [CrossRef]
- Papini, E.; Negro, R.; Pinchera, A.; Guglielmi, R.; Baroli, A.; Beck-Peccoz, P.; Garofalo, P.; Pisoni, M.; Zini, M.; Elisei, R.; et al. Thyroid nodule and differentiated thyroid cancer management in pregnancy. An Italian Association of Clinical Endocrinologists (AME) and Italian Thyroid Association (AIT) Joint Statement for Clinical Practice. J. Endocrinol. Investig. 2010, 33, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Bluemel, C.; Herrmann, K.; Giammarile, F.; Nieweg, O.E.; Dubreuil, J.; Testori, A.; Audisio, R.A.; Zoras, O.; Lassmann, M.; Chakera, A.H.; et al. EANM practice guidelines for lymphoscintigraphy and sentinel lymph node biopsy in melanoma. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1750–1766. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Loibl, S.; Pagani, O.; Graziottin, A.; Panizza, P.; Martincich, L.; Gentilini, O.; Peccatori, F.; Fourquet, A.; Delaloge, S.; et al. The European Society of Breast Cancer Specialists recommendations for the management of young women with breast cancer. Eur. J. Cancer 2012, 48, 3355–3377. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Obstetricians and Gynaecologists. Pregnancy and Breast Cancer; Royal College of Obstetricians and Gynaecologists: London, UK, 2011. [Google Scholar]
- Amant, F.; Deckers, S.; Van Calsteren, K.; Loibl, S.; Halaska, M.; Brepoels, L.; Beijnen, J.; Cardoso, F.; Gentilini, O.; Lagae, L.; et al. Breast cancer in pregnancy: Recommendations of an international consensus meeting. Eur. J. Cancer 2010, 46, 3158–3168. [Google Scholar] [CrossRef]
- Loibl, S.; Von Minckwitz, G.; Gwyn, K.; Ellis, P.; Blohmer, J.U.; Schlegelberger, B.; Keller, M.; Harder, S.; Theriault, R.L.; Crivellari, D.; et al. Breast carcinoma during pregnancy: International recommendations from an expert meeting. Cancer 2006, 106, 237–246. [Google Scholar] [CrossRef]
- Helewa, M.; Lévesque, P.; Provencher, D.; Lea, R.; Rosolowich, V.; Shapiro, H. Breast cancer, pregnancy, and breastfeeding. J. Obs. Gynaecol. Can. 2002, 24, 164–180. [Google Scholar]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie-Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients with Cervical Cancer. Virchows Arch. 2018, 472, 919–936. [Google Scholar] [CrossRef]
- Reed, N.; Balega, J.; Barwick, T.; Buckley, L.; Burton, K.; Eminowicz, G.; Forrest, J.; Ganesan, R.; Harrand, R.; Holland, C.; et al. British Gynaecological Cancer Society (BGCS) cervical cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 433–465. [Google Scholar] [CrossRef]
- De Groot, L.; Abalovich, M.; Alexander, E.K.; Amino, N.; Barbour, L.; Cobin, R.H.; Eastman, C.J.; Lazarus, J.H.; Luton, D.; Mandel, S.J.; et al. Management of thyroid dysfunction during pregnancy and postpartum: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 2543–2565. [Google Scholar] [CrossRef]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease during Pregnancy and the Postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef]
- Marsden, J.R.; Newton-Bishop, J.A.; Burrows, L.; Cook, M.; Corrie, P.G.; Cox, N.H.; Gore, M.E.; Lorigan, P.; MacKie, R.; Nathan, P.; et al. Revised UK guidelines for the management of cutaneous melanoma 2010. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1401–1419. [Google Scholar] [CrossRef] [PubMed]
- Pallera, A.; Altman, J.K.; Berman, E.; Abboud, C.N.; Bhatnagar, B.; Curtin, P.; DeAngelo, D.J.; Gotlib, J.; Tanner Hagelstrom, R.; Hobbs, G.; et al. NCCN guidelines® insights: Chronic myeloid leukemia, version 1. 2017: Featured updates to the NCCN guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2016, 14, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Van Calsteren, K.; Halaska, M.J.; Beijnen, J.; Lagae, L.; Hanssens, M.; Heyns, L.; Lannoo, L.; Ottevanger, N.P.; Vanden Bogaert, W.; et al. Gynecologic Cancers in Pregnancy. Int. J. Gynecol. Cancer 2009, 19, S1–S12. [Google Scholar] [CrossRef] [PubMed]
- Lishner, M.; Avivi, I.; Apperley, J.F.; Dierickx, D.; Evens, A.M.; Fumagalli, M.; Nulman, I.; Oduncu, F.S.; Peccatori, F.A.; Robinson, S.; et al. Hematologic malignancies in pregnancy: Management guidelines from an international consensus meeting. J. Clin. Oncol. 2016, 34, 501–508. [Google Scholar] [CrossRef]
- Amant, F.; Berveiller, P.; Boere, I.A.; Cardonick, E.; Fruscio, R.; Fumagalli, M.; Halaska, M.J.; Hasenburg, A.; Johansson, A.L.V.; Lambertini, M.; et al. Gynecologic cancers in pregnancy: Guidelines based on a third international consensus meeting. Ann. Oncol. 2019, 30, 1601–1612. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Azim, H.A.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. S6), 160–170. [Google Scholar] [CrossRef]
- Pentheroudakis, G.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N. Cancer, fertility and pregnancy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, 266–273. [Google Scholar] [CrossRef]
- Pentheroudakis, G.; Pavlidis, N.; Castiglione, M. Cancer, fertility and pregnancy: ESMO Clinical Recommendations for diagnosis, treatment and follow-up. Ann. Oncol. 2008, 19, ii108–ii109. [Google Scholar] [CrossRef]
- Koren, G.; Carey, N.; Gagnon, R.; Maxwell, C.; Nulman, I.; Senikas, V. Cancer Chemotherapy and Pregnancy. J. Obstet. Gynaecol. Canada 2013, 35, 263–278. [Google Scholar] [CrossRef]
- Coccia, P.F.; Pappo, A.S.; Beaupin, L.; Borges, V.F.; Borinstein, S.C.; Chugh, R.; Dinner, S.; Folbrecht, J.; Frazier, A.L.; Goldsby, R.; et al. Adolescent and young adult oncology, version 2.2018: Clinical practice guidelines in oncology. JNCCN J. Natl. Compr. Cancer Netw. 2018, 16, 66–97. [Google Scholar] [CrossRef]
- Morice, P.; Narducci, F.; Mathevet, P.; Marret, H.; Darai, E.; Querleu, D. French Recommendations on the Management of Invasive Cervical Cancer During Pregnancy. Int. J. Gynecol. Cancer 2009, 19, 1638–1641. [Google Scholar] [CrossRef] [PubMed]
- Abalovich, M.; Amino, N.; Barbour, L.A.; Cobin, R.H.; De Groot, L.J.; Glinoer, D.; Mandel, S.J.; Stagnaro-Green, A.; Edwards, H. Clinical practice guideline: Management of thyroid dysfunction during pregnancy and postpartum: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2007, 92, S1–S47. [Google Scholar] [CrossRef] [PubMed]
- Stagnaro-Green, A.; Abalovich, M.; Alexander, E.; Azizi, F.; Mestman, J.; Negro, R.; Nixon, A.; Pearce, E.N.; Soldin, O.P.; Sullivan, S.; et al. Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease during Pregnancy and Postpartum. Thyroid 2011, 21, 1081–1125. [Google Scholar] [CrossRef] [PubMed]
- Galofré, J.C.; Riesco-Eizaguirre, G.; Álvarez-Escolá, C. Clinical guidelines for management of thyroid nodule and cancer during pregnancy. Endocrinol. Nutr. 2014, 61, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Cwynarski, K.; Marzolini, M.A.V.; Barrington, S.F.; Follows, G.; Illidge, T.; Stern, S.; Davies, A. The management of primary mediastinal B-cell lymphoma: A British Society for Haematology Good Practice Paper. Br. J. Haematol. 2019, 185, 402–409. [Google Scholar] [CrossRef]
- Bourdel, N.; Huchon, C.; Abdel Wahab, C.; Azaïs, H.; Bendifallah, S.; Bolze, P.A.; Brun, J.L.; Canlorbe, G.; Chauvet, P.; Chereau, E.; et al. Borderline ovarian tumors: French guidelines from the CNGOF. Part 2. Surgical management, follow-up, hormone replacement therapy, fertility management and preservation. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101966. [Google Scholar] [CrossRef]
- Gradishar, W.; Moran, M.; Abraham, J.; Aft, R.; Agnese, M.; Allison, K.; Blair, S.; Kumar, R. Breast Cancer, Version 4. 2021 Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2021, 19, 484–494. [Google Scholar] [CrossRef]
- Hurst, S.A. Vulnerability in research and health care; Describing the elephant in the room? Bioethics 2008, 22, 191–202. [Google Scholar] [CrossRef]
- Ten Have, H. Respect for Human Vulnerability: The Emergence of a New Principle in Bioethics. J. Bioeth. Inq. 2015, 12, 395–408. [Google Scholar] [CrossRef]
- Yeoman, G.; Furlong, P.; Seres, M.; Binder, H.; Chung, H.; Garzya, V.; Jones, R.R.M. Defining patient centricity with patients for patients and caregivers: A collaborative endeavour. BMJ Innov. 2017, 3, 76–83. [Google Scholar] [CrossRef]
- Cavolo, A.; de Casterlé, B.D.; Naulaers, G.; Gastmans, C. Neonatologists’ decision-making for resuscitation and non-resuscitation of extremely preterm infants: Ethical principles, challenges, and strategies—A qualitative study. BMC Med. Ethics 2021, 22, 129. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linkeviciute, A.; Canario, R.; Peccatori, F.A.; Dierickx, K. Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians. Cancers 2022, 14, 4325. https://doi.org/10.3390/cancers14174325
Linkeviciute A, Canario R, Peccatori FA, Dierickx K. Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians. Cancers. 2022; 14(17):4325. https://doi.org/10.3390/cancers14174325
Chicago/Turabian StyleLinkeviciute, Alma, Rita Canario, Fedro Alessandro Peccatori, and Kris Dierickx. 2022. "Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians" Cancers 14, no. 17: 4325. https://doi.org/10.3390/cancers14174325
APA StyleLinkeviciute, A., Canario, R., Peccatori, F. A., & Dierickx, K. (2022). Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians. Cancers, 14(17), 4325. https://doi.org/10.3390/cancers14174325