
Implication of Hepsin from Primary Tumor in the Prognosis of Colorectal Cancer Patients

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract

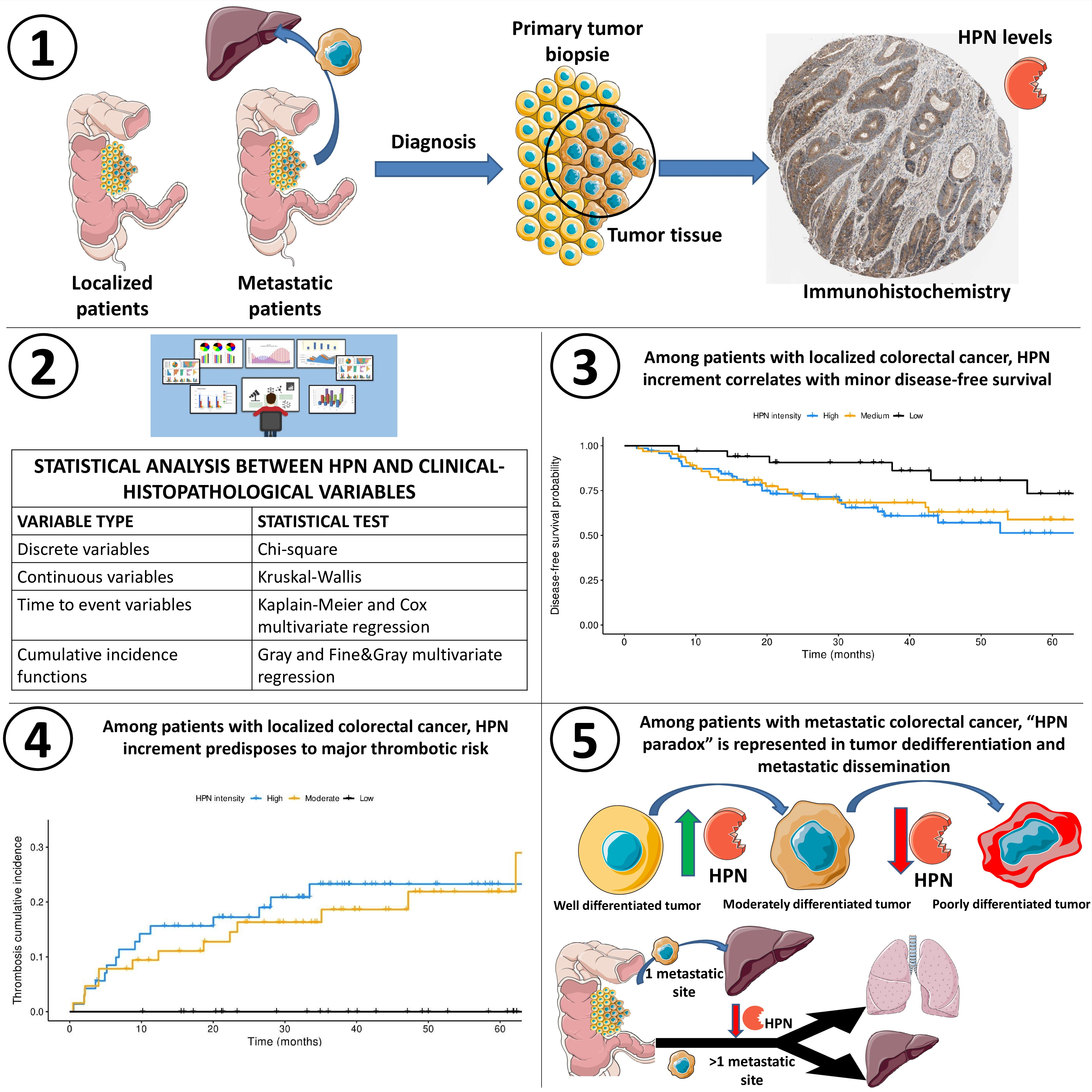
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tissue Microarrays and Immunohistochemistry
2.3. Clinical and Histopathological Variables of the Patients
2.4. Statistics
3. Results
3.1. Patients and Clinical-Histopathologic Data
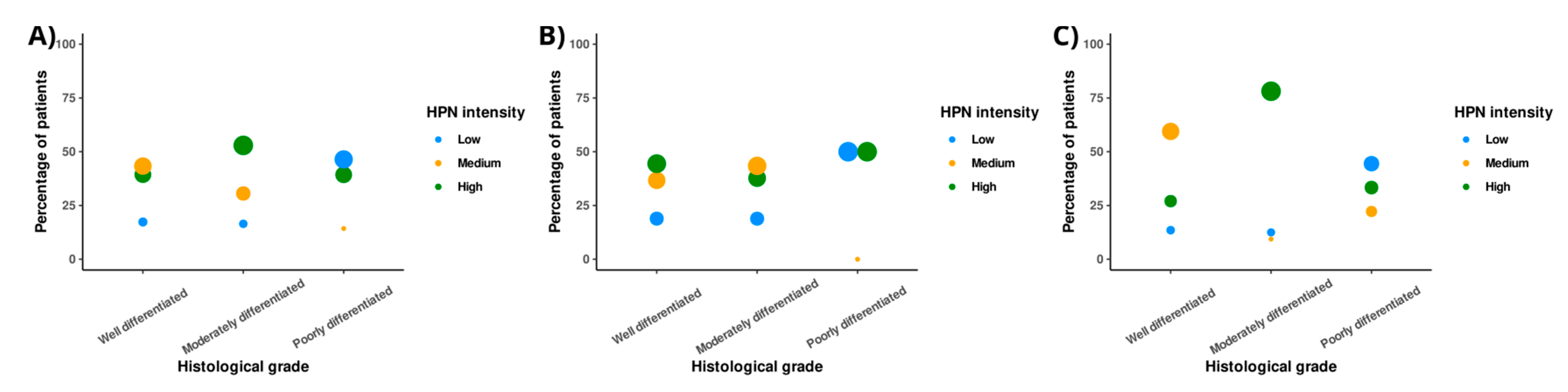
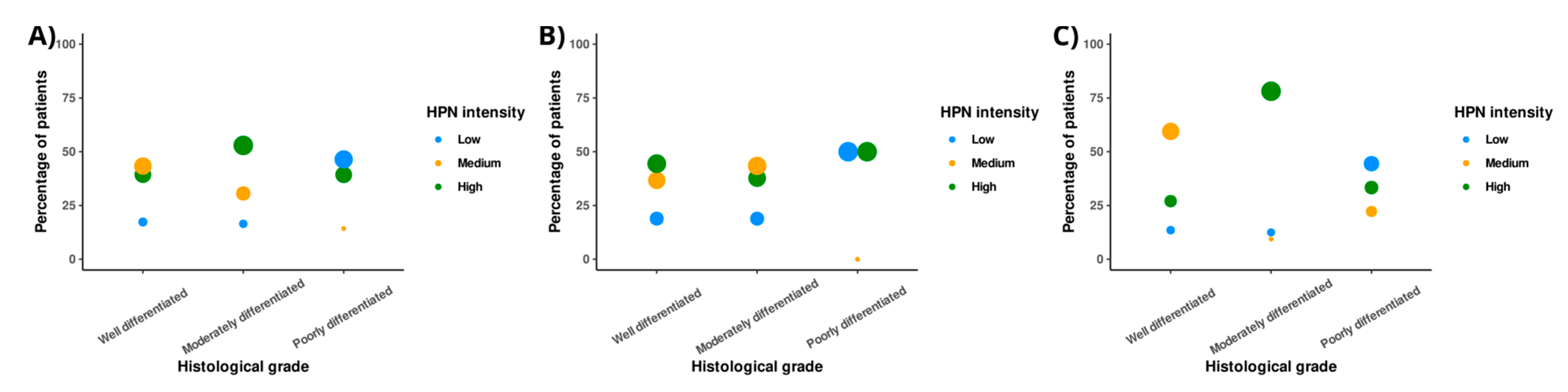
3.2. Low HPN Staining Intensity Predisposes to Poor CRC Differentiation
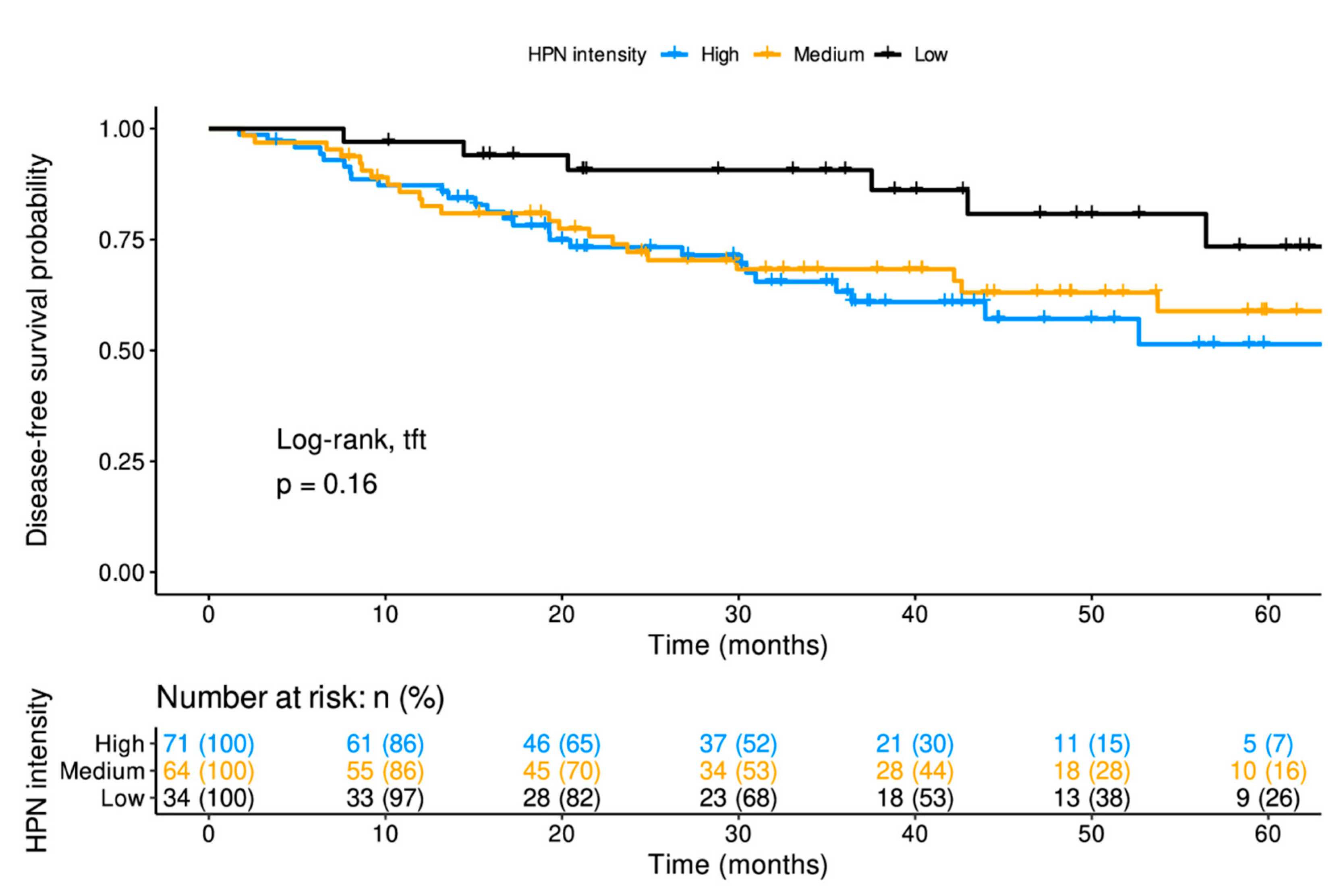
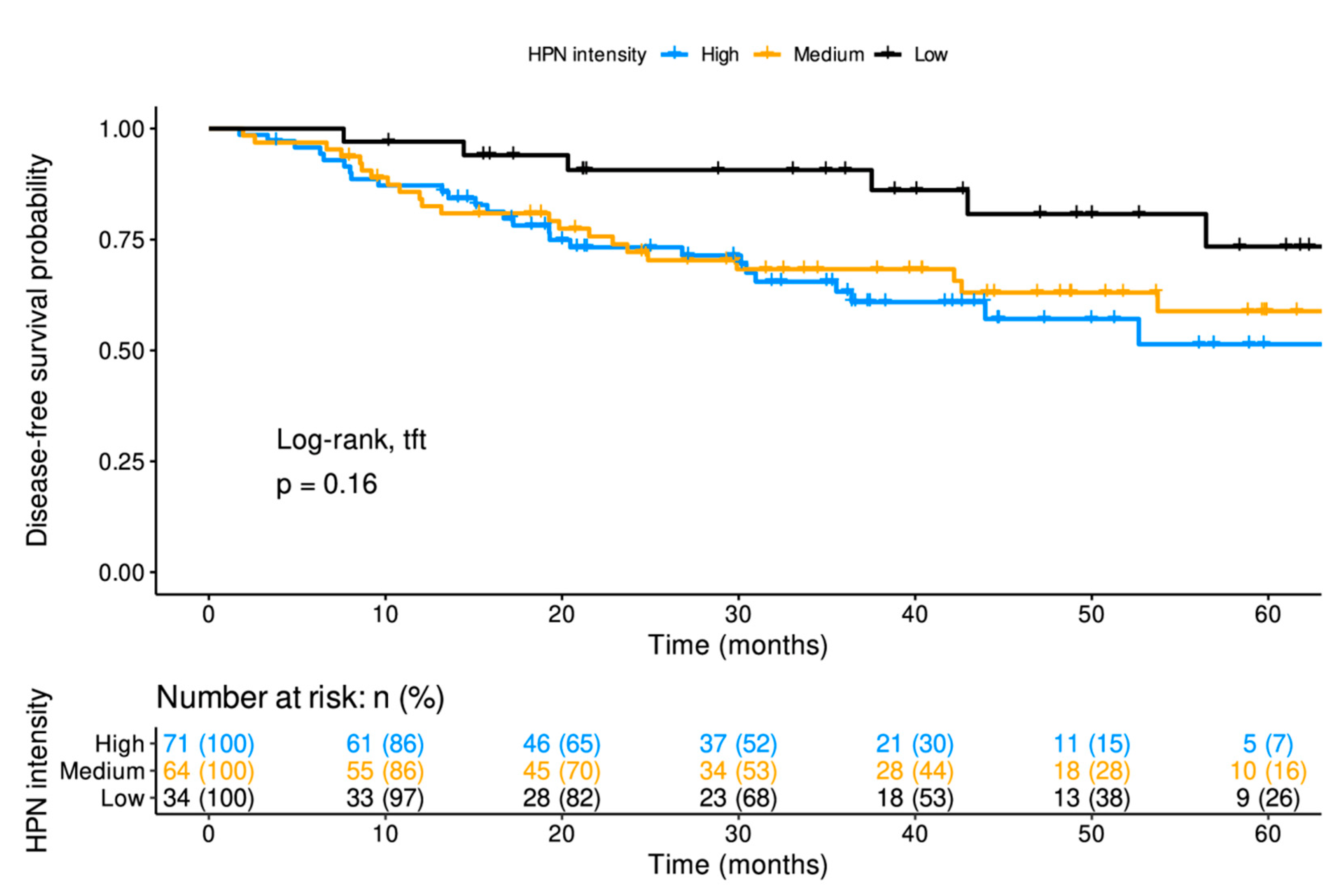
3.3. In Patients with Localized Disease, High-Intensity HPN Staining Decreases DFS
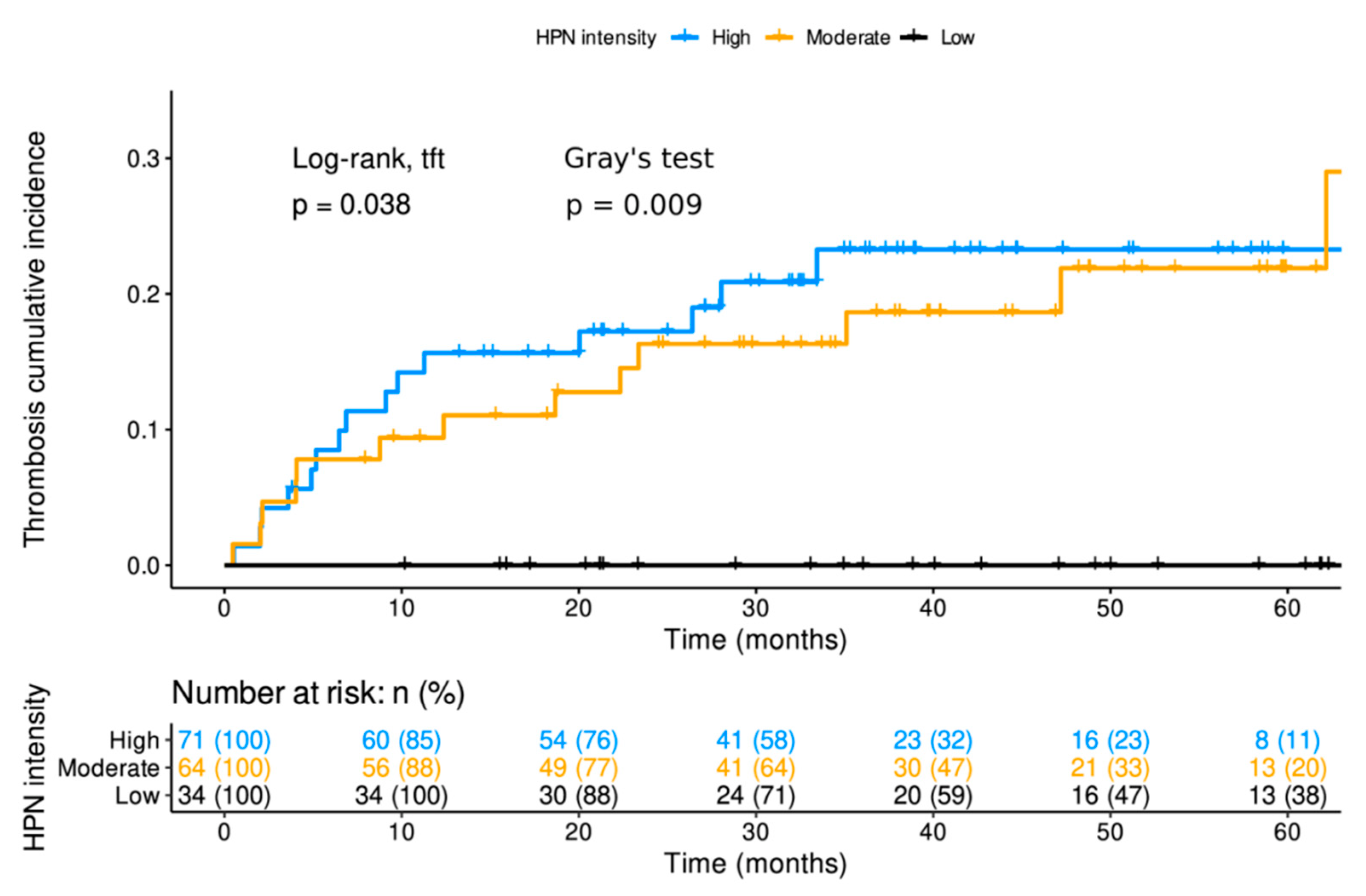
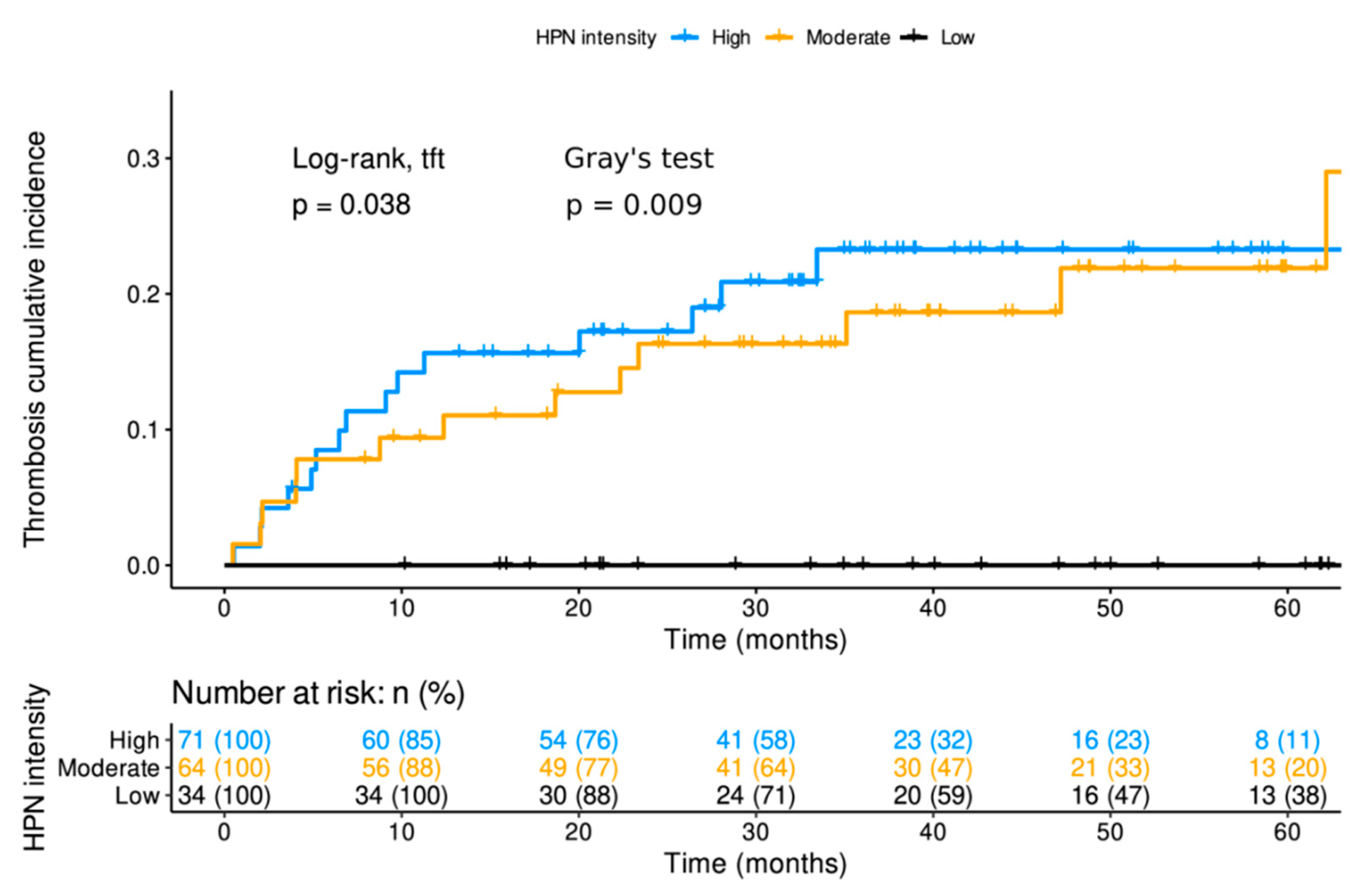
3.4. The Intensity of HPN Staining in Patients with Localized Disease at Diagnosis was Related to the Cumulative Incidence of Thrombosis
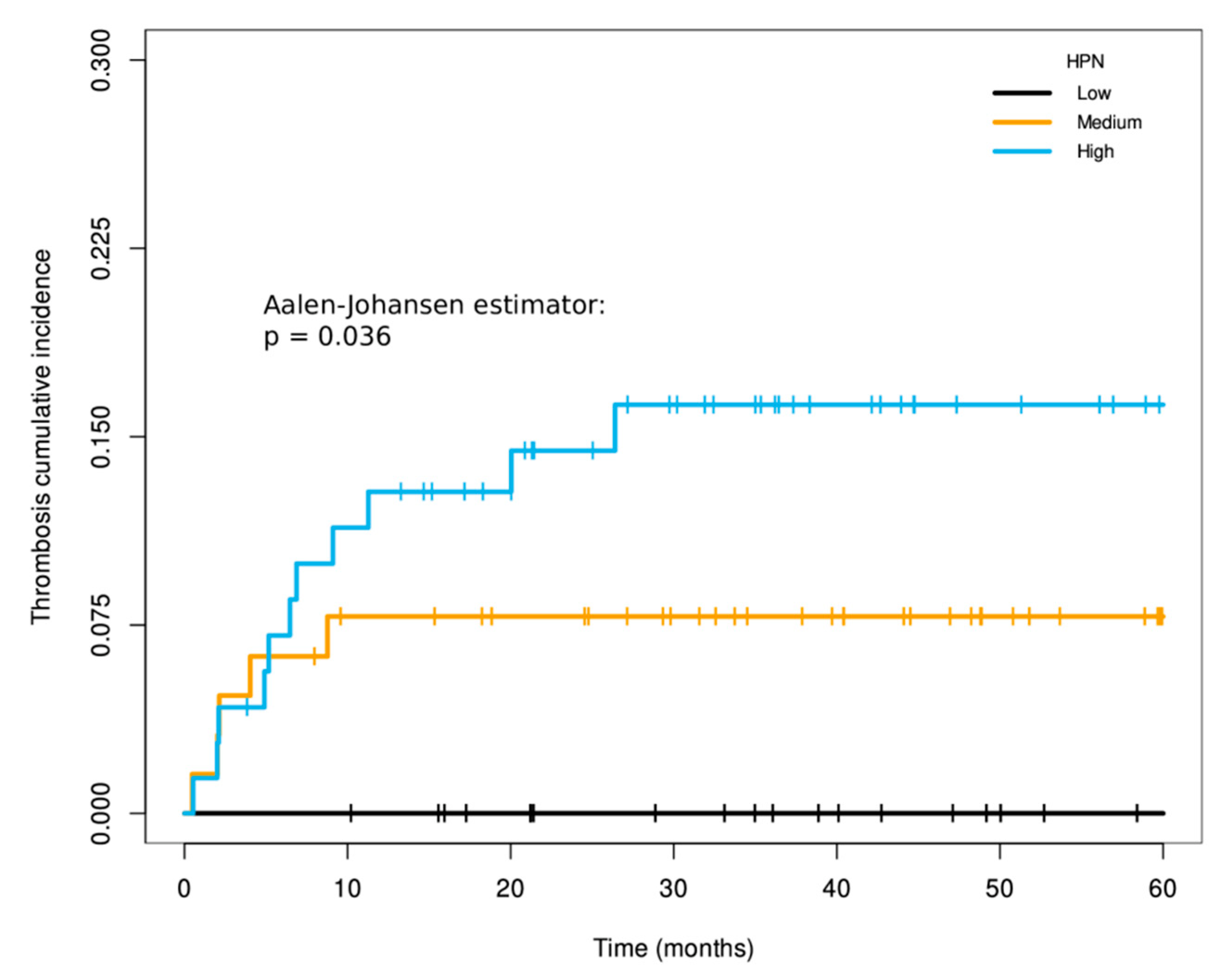
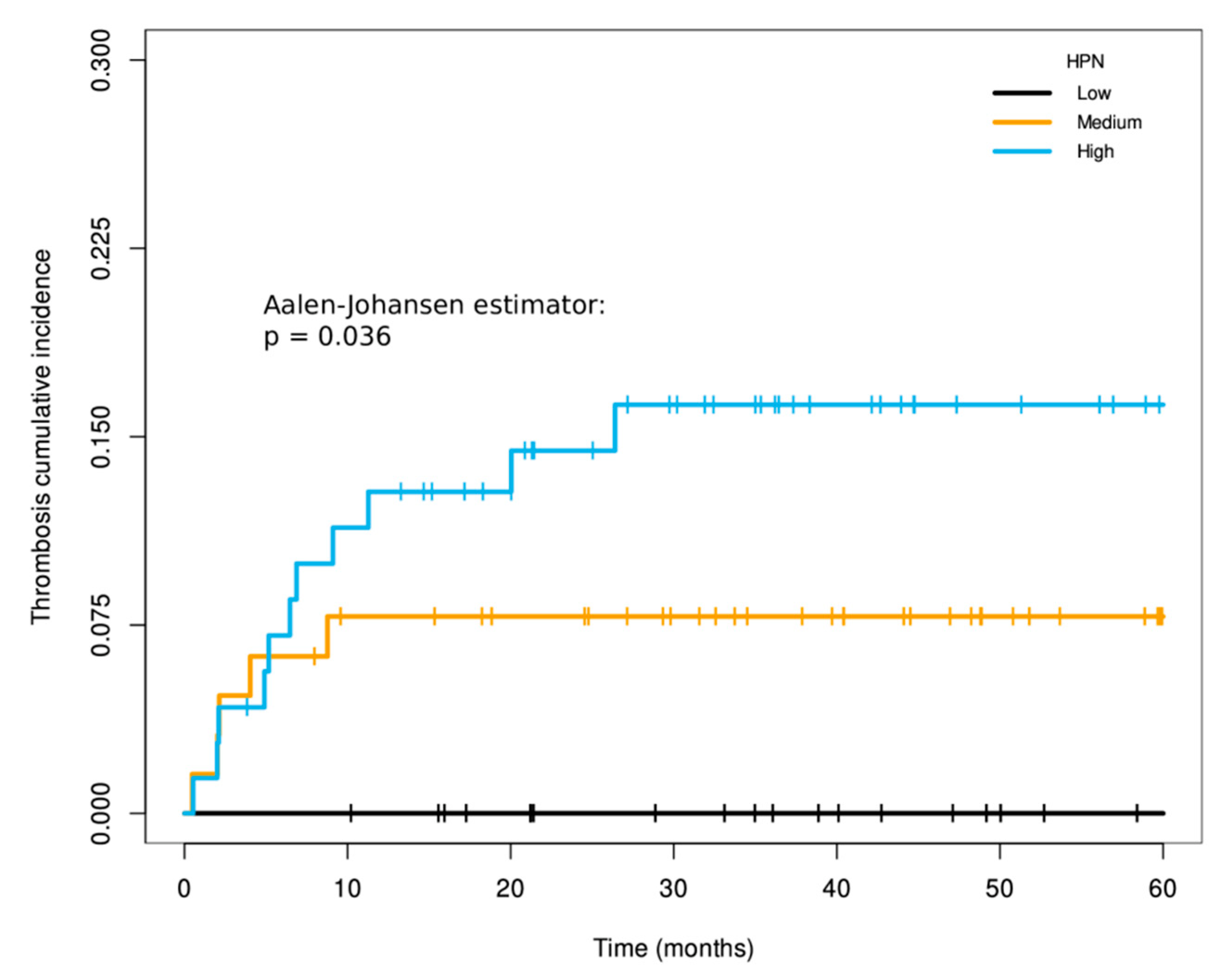
3.5. Association of HPN with the Prognosis of Metastatic Patients and Their Cumulative Incidence of Thrombosis
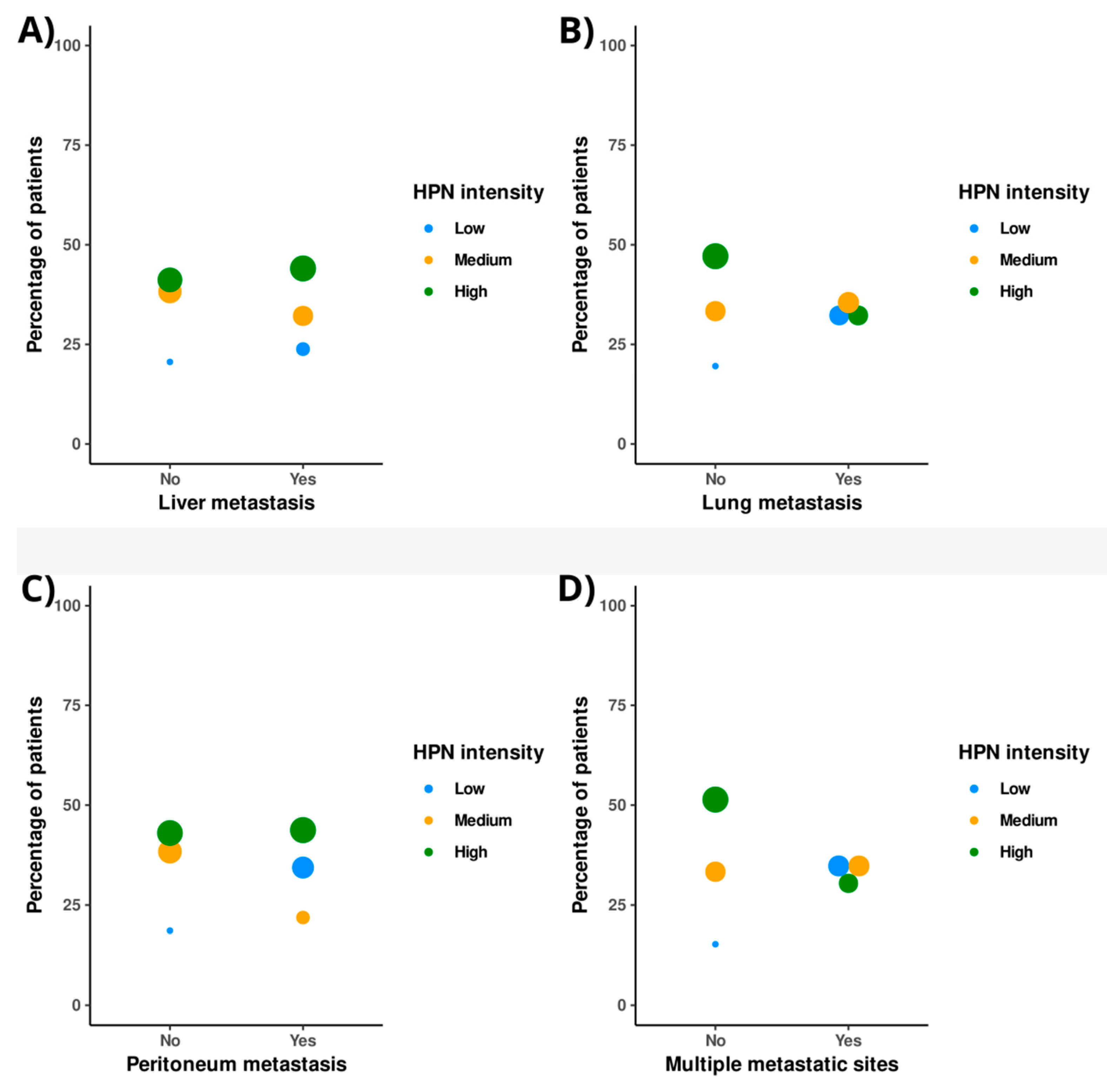
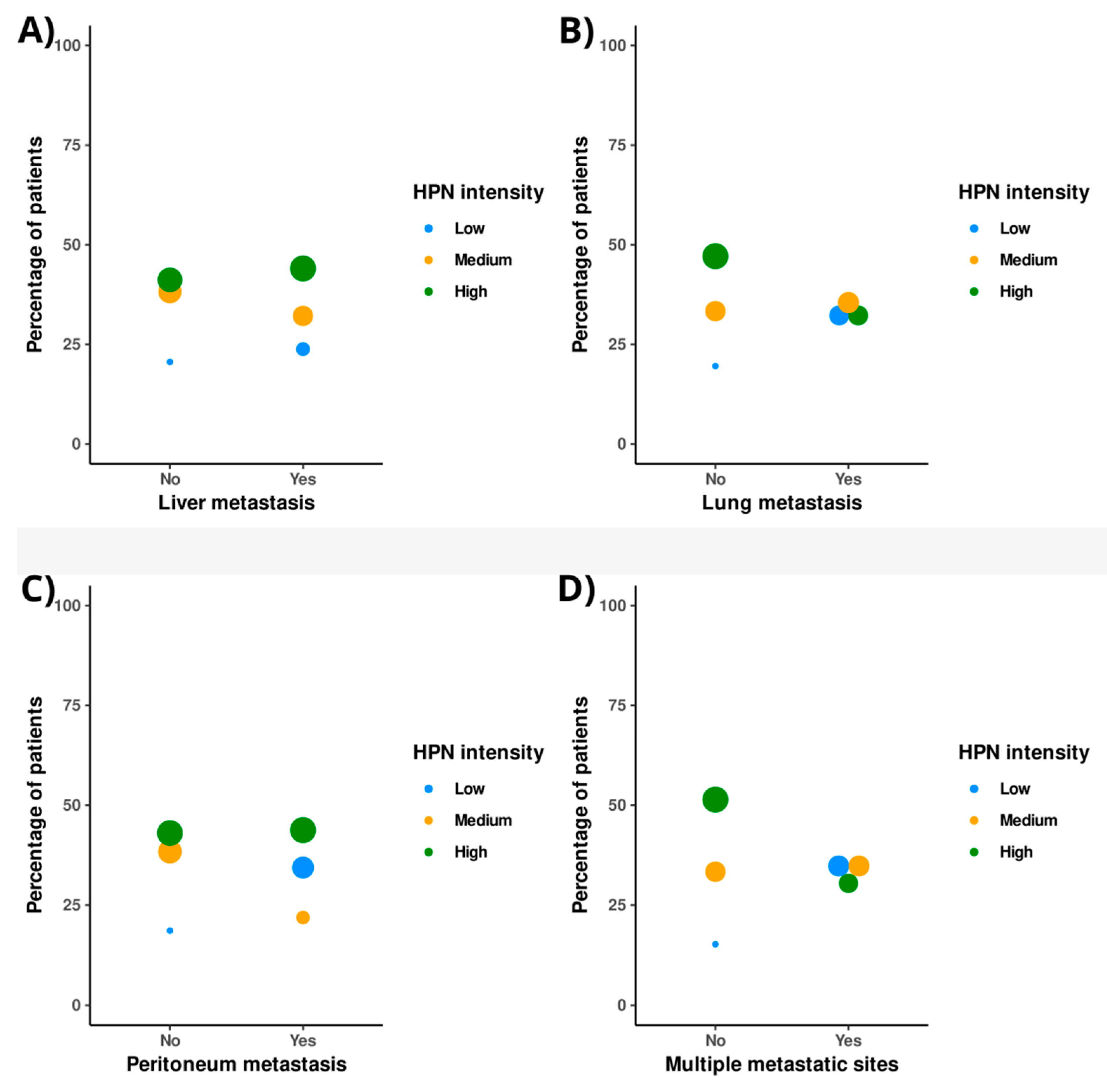
3.6. Association of HPN with the Pattern of Tumor Dissemination in Metastatic Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tanabe, L.M.; List, K. The role of type II transmembrane serine protease-mediated signaling in cancer. FEBS J. 2017, 284, 1421–1436. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, L.; Sun, S.; Wu, Q. Hepsin: A multifunctional transmembrane serine protease in pathobiology. FEBS J. 2021, 288, 5252–5264. [Google Scholar] [CrossRef] [PubMed]
- Torres-Rosado, A.; O’Shea, K.S.; Tsuji, A.; Chou, S.H.; Kurachi, K. Hepsin, a putative cell-surface serine protease, is required for mammalian cell growth. Proc. Natl. Acad. Sci. USA 1993, 90, 7181–7185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Peng, J.; Wang, H.; Zhang, W.; Brown, J.M.; Zhou, Y.; Wu, Q. Hepsin enhances liver metabolism and inhibits adipocyte browning in mice. Proc. Natl. Acad. Sci. USA 2020, 117, 12359–12367. [Google Scholar] [CrossRef]
- Wilkinson, D.J.; Desilets, A.; Lin, H.; Charlton, S.; Del Carmen Arques, M.; Falconer, A.; Bullock, C.; Hsu, Y.C.; Birchall, K.; Hawkins, A.; et al. The serine proteinase hepsin is an activator of pro-matrix metalloproteinases: Molecular mechanisms and implications for extracellular matrix turnover. Sci. Rep. 2017, 7, 16693. [Google Scholar] [CrossRef] [Green Version]
- Kazama, Y.; Hamamoto, T.; Foster, D.C.; Kisiel, W. Hepsin, a putative membrane-associated serine protease, activates human factor VII and initiates a pathway of blood coagulation on the cell surface leading to thrombin formation. J. Biol. Chem. 1995, 270, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Khandekar, G.; Iyer, N.; Jagadeeswaran, P. Prostasin and hepatocyte growth factor B in factor VIIa generation: Serine protease knockdowns in zebrafish. Res. Pract. Thromb. Haemost. 2020, 4, 1150–1157. [Google Scholar] [CrossRef]
- Murray, A.S.; Varela, F.A.; List, K. Type II transmembrane serine proteases as potential targets for cancer therapy. Biol. Chem. 2016, 397, 815–826. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Li, J.; Yang, H.; Bai, Y.; Hu, C.; Wu, H.; Jiang, H.; Wang, Q. Hepsin Promotes Epithelial-Mesenchymal Transition and Cell Invasion Through the miR-222/PPP2R2A/AKT Axis in Prostate Cancer. OncoTargets Ther. 2020, 13, 12141–12149. [Google Scholar] [CrossRef]
- Willbold, R.; Wirth, K.; Martini, T.; Sültmann, H.; Bolenz, C.; Wittig, R. Excess hepsin proteolytic activity limits oncogenic signaling and induces ER stress and autophagy in prostate cancer cells. Cell Death Dis. 2019, 10, 601. [Google Scholar] [CrossRef]
- Miao, J.; Mu, D.; Ergel, B.; Singavarapu, R.; Duan, Z.; Powers, S.; Oliva, E.; Orsulic, S. Hepsin colocalizes with desmosomes and induces progression of ovarian cancer in a mouse model. Int. J. Cancer 2008, 123, 2041–2047. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Takamoto, N.; Abarzua, F.; Hongo, A.; Kodama, J.; Nasu, Y.; Kumon, H.; Hiramatsu, Y. Hepsin inhibits the cell growth of endometrial cancer. Int. J. Mol. Med. 2008, 22, 389–397. [Google Scholar] [CrossRef]
- Zhang, M.; Zhao, J.; Tang, W.; Wang, Y.; Peng, P.; Li, L.; Song, S.; Wu, H.; Li, C.; Yang, C.; et al. High Hepsin expression predicts poor prognosis in Gastric Cancer. Sci. Rep. 2016, 6, 36902. [Google Scholar] [CrossRef] [Green Version]
- Pelkonen, M.; Luostari, K.; Tengström, M.; Ahonen, H.; Berdel, B.; Kataja, V.; Soini, Y.; Kosma, V.M.; Mannermaa, A. Low expression levels of hepsin and TMPRSS3 are associated with poor breast cancer survival. BMC Cancer 2015, 15, 431. [Google Scholar] [CrossRef] [Green Version]
- Herszényi, L.; Barabás, L.; Hritz, I.; István, G.; Tulassay, Z. Impact of proteolytic enzymes in colorectal cancer development and progression. World J. Gastroenterol. 2014, 20, 13246–13257. [Google Scholar] [CrossRef] [Green Version]
- Tieng, F.Y.F.; Abu, N.; Sukor, S.; Mohd Azman, Z.A.; Mahamad Nadzir, N.; Lee, L.H.; Mutalib, N.S.A. L1CAM, CA9, KLK6, HPN, and ALDH1A1 as Potential Serum Markers in Primary and Metastatic Colorectal Cancer Screening. Diagnostics 2020, 10, 444. [Google Scholar] [CrossRef]
- Alcalay, A.; Wun, T.; Khatri, V.; Chew, H.K.; Harvey, D.; Zhou, H.; White, R.H. Venous thromboembolism in patients with colorectal cancer: Incidence and effect on survival. J. Clin. Oncol. 2006, 24, 1112–1118. [Google Scholar] [CrossRef]
- The Human Protein Atlas. HPN. Available online: https://www.proteinatlas.org/ENSG00000105707-HPN/pathology (accessed on 1 October 2020).
- Xu, W.; He, Y.; Wang, Y.; Li, X.; Young, J.; Ioannidis, J.P.A.; Dunlop, M.G.; Theodoratou, E. Risk factors and risk prediction models for colorectal cancer metastasis and recurrence: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18, 172. [Google Scholar] [CrossRef]
- Luo, D.; Liu, Q.; Yu, W.; Ma, Y.; Zhu, J.; Lian, P.; Cai, S.; Li, Q.; Li, X. Prognostic value of distant metastasis sites and surgery in stage IV colorectal cancer: A population-based study. Int. J. Colorectal. Dis. 2018, 33, 1241–1249. [Google Scholar] [CrossRef]
- Hamza, M.S.; Mousa, S.A. Cancer-Associated Thrombosis: Risk Factors, Molecular Mechanisms, Future Management. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620954282. [Google Scholar] [CrossRef]
- Abdol Razak, N.B.; Jones, G.; Bhandari, M.; Berndt, M.C.; Metharom, P. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018, 10, 380. [Google Scholar] [CrossRef] [Green Version]
- Dickmann, B.; Ahlbrecht, J.; Ay, C.; Dunkler, D.; Thaler, J.; Scheithauer, W.; Quehenberger, P.; Zielinski, C.; Pabinger, I. Regional lymph node metastases are a strong risk factor for venous thromboembolism: Results from the Vienna Cancer and Thrombosis Study. Haematologica 2013, 98, 1309–1314. [Google Scholar] [CrossRef] [Green Version]
- Sudoyo, A.W.; Rachman, A.; Harimurti, K. Angiogenesis, inflammation, platelets count, and metastatic status as a predictor for thrombosis risk in nasopharyngeal carcinoma patients. Acta. Med. Indones. 2015, 47, 11–15. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 3 December 2021).
- Therneau, T. A Package for Survival Analysis in R. R Package Version 3.2-13. 2021. Available online: https://CRAN.R-project.org/package=survival (accessed on 5 December 2021).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model, 1st ed.; Springer: New York, NY, USA, 2000. [Google Scholar]
- Dignam, J.J.; Kocherginsky, M.N. Choice and interpretation of statistical tests used when competing risks are present. J. Clin. Oncol. 2008, 26, 4027–4034. [Google Scholar] [CrossRef]
- Li, J.; Scheike, T.H.; Zhang, M.J. Checking Fine and Gray subdistribution hazards model with cumulative sums of residuals. Lifetime Data Anal. 2015, 21, 197–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allignol, A.; Schumacher, M.; Beyersmann, J. A note on variance estimation of the Aalen-Johansen estimator of the cumulative incidence function in competing risks, with a view towards left-truncated data. Biom. J. 2010, 52, 126–137. [Google Scholar] [CrossRef]
- Satten, G.A.; Datta, S. Kaplan–Meier representation of competing risk estimates. Stat. Probab. Lett. 1999, 42, 299–304. [Google Scholar] [CrossRef]
- Therneau, T.M.; Lumley, T. Package ‘Survival’ 2016. Available online: https://cran.r-project.org/package=survival (accessed on 5 December 2021).
- Package Cmprsk. Available online: https://cran.r-project.org/web/packages/cmprsk/cmprsk.pdf (accessed on 6 February 2022).
- Tervonen, T.A.; Pant, S.M.; Belitškin, D.; Englund, J.I.; Närhi, K.; Haglund, C.; Kovanen, P.E.; Verschuren, E.W.; Klefström, J. Oncogenic Ras Disrupts Epithelial Integrity by Activating the Transmembrane Serine Protease Hepsin. Cancer Res. 2021, 81, 1513–1527. [Google Scholar] [CrossRef] [PubMed]
- Dienstmann, R.; Salazar, R.; Tabernero, J. Personalizing colon cancer adjuvant therapy: Selecting optimal treatments for individual patients. J. Clin. Oncol. 2015, 33, 1787–1796. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Rees, P.A.; Clouston, H.W.; Duff, S.; Kirwan, C.C. Colorectal cancer and thrombosis. Int. J. Colorectal. Dis. 2018, 33, 105–108. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, K.; Kawai, K.; Tsuno, N.H.; Sunami, E.; Kitayama, J. Impact of preoperative thrombocytosis on the survival of patients with primary colorectal cancer. World J. Surg. 2012, 36, 192–200. [Google Scholar] [CrossRef]
- Stender, M.T.; Larsen, T.B.; Sørensen, H.T.; Thorlacius-Ussing, O. Preoperative plasma D-dimer predicts 1-year survival in colorectal cancer patients with absence of venous thromboembolism (VTE): A prospective clinical cohort study. J. Thromb. Haemost. 2012, 10, 2027–2031. [Google Scholar] [CrossRef]
- Tang, L.; Liu, K.; Wang, J.; Wang, C.; Zhao, P.; Liu, J. High preoperative plasma fibrinogen levels are associated with distant metastases and impaired prognosis after curative resection in patients with colorectal cancer. J. Surg. Oncol. 2010, 102, 428–432. [Google Scholar] [CrossRef]
- Wang, W.S.; Lin, J.K.; Lin, T.C.; Chiou, T.J.; Liu, J.H.; Yen, C.C.; Chen, P.M. Plasma von Willebrand factor level as a prognostic indicator of patients with metastatic colorectal carcinoma. World J. Gastroenterol. 2005, 11, 2166–2170. [Google Scholar] [CrossRef]
- Klezovitch, O.; Chevillet, J.; Mirosevich, J.; Roberts, R.L.; Matusik, R.J.; Vasioukhin, V. Hepsin promotes prostate cancer progression and metastasis. Cancer Cell 2004, 6, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Stephan, C.; Yousef, G.M.; Scorilas, A.; Jung, K.; Jung, M.; Kristiansen, G.; Hauptmann, S.; Kishi, T.; Nakamura, T.; Loening, S.A.; et al. Hepsin is highly over expressed in and a new candidate for a prognostic indicator in prostate cancer. J. Urol. 2004, 171, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Xing, P.; Li, J.G.; Jin, F.; Zhao, T.T.; Liu, Q.; Dong, H.T.; Wei, X.L. Clinical and biological significance of hepsin overexpression in breast cancer. J. Investig. Med. 2011, 59, 803–810. [Google Scholar] [CrossRef]
- Nandana, S.; Ellwood-Yen, K.; Sawyers, C.; Wills, M.; Weidow, B.; Case, T.; Vasioukhin, V.; Matusik, R. Hepsin cooperates with MYC in the progression of adenocarcinoma in a prostate cancer mouse model. Prostate 2010, 70, 591–600. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Chang, W.; Mao, Y.; He, G.; Zheng, P.; Tang, W.; Wei, Y.; Ren, L.; Zhu, D.; Ji, M.; et al. Tumor-associated Macrophages as Prognostic and Predictive Biomarkers for Postoperative Adjuvant Chemotherapy in Patients with Stage II Colon Cancer. Clin. Cancer Res. 2019, 25, 3896–3907. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Parry, G. Hepsin and prostate cancer. Front. Biosci. 2007, 12, 5052–5059. [Google Scholar] [CrossRef]
- Rentsch, M.; Schiergens, T.; Khandoga, A.; Werner, J. Surgery for Colorectal Cancer—Trends, Developments, and Future Perspectives. Visc. Med. 2016, 32, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, M.; Nandana, S.; Yamashita, H.; Ganesan, R.; Kirchhofer, D.; Quaranta, V. Laminin-332 is a substrate for hepsin, a protease associated with prostate cancer progression. J. Biol. Chem. 2008, 283, 30576–30584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasioukhin, V. Hepsin paradox reveals unexpected complexity of metastatic process. Cell Cycle 2004, 3, 1394–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrissey, C.; True, L.D.; Roudier, M.P.; Coleman, I.M.; Hawley, S.; Nelson, P.S.; Coleman, R.; Wang, Y.C.; Corey, E.; Lange, P.H.; et al. Differential expression of angiogenesis associated genes in prostate cancer bone, liver and lymph node metastases. Clin. Exp. Metastasis 2008, 25, 377–388. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical/Histopathological Features | Overall Cohort N 1 = 287 | Localized Patients N = 169 (58.9%) | Metastatic Patients N = 118 (41.1%) |
|---|---|---|---|
| Median age at diagnosis (Range) (years) | 66 (22–88) | 64 (22–83) | 68 (26–88) |
| Males: N (%) | 187 (65.2) | 109 (64.5) | 78 (66.1) |
| Median follow-up (Range) (months) | 35.1 (1.4–194) | 41.2 (3.8–190.8) | 24.5 (1.4–194) |
| ECOG 2 at diagnosis < 2: N (%) | 237 (82.6) | 152 (89.9) | 85 (72) |
| Median survival (95% CI 3, LL 4-UL 5) (months) | 64.5 (55.4–82.9) | 93 (83.2–118.2) | 24.7 (21.5–33.5) |
| Localized patients at diagnosis who undergo metastatic relapse during follow-up: N (%) | NA | 54 (32) | NA |
| Patients with disease progression after first-line chemotherapy: N (%) | 145 (50.5) | 43 (25.4) | 102 (86.4) |
| 5-year cumulative incidence of thrombosis (%; 95% CI, LL-UL) | 25.91; 20.49–32.43 | 18.24; 12.69–25.84 | 39.39; 29.05–51.85 |
| Primary tumor | |||
| Ascending colon: N (%) | 83 (28.9) | 48 (28.4) | 35 (29.7) |
| Descending colon: N (%) | 14 (4.9) | 9 (5.3) | 5 (4.2) |
| Transverse colon: N (%) | 15 (5.2) | 10 (5.9) | 5 (4.2) |
| Sigmoid colon: N (%) | 67 (23.3) | 36 (21.3) | 31 (26.3) |
| Rectal: N (%) | 99 (34.5) | 64 (37.9) | 35 (29.7) |
| Multiple synchronous locations: N (%) | 9 (3.1) | 2 (1.2) | 7 (5.9) |
| Localization of metastases at diagnosis | |||
| Liver: N (%) | NA | NA | 84 (71.2) |
| Lung: N (%) | NA | NA | 31 (26.3) |
| Peritoneum: N (%) | NA | NA | 32 (27.1) |
| Other affectations: N (%) | NA | NA | 4 (3.4) |
| More than one metastatic site: N (%) | NA | NA | 46 (39) |
| Histological grade at diagnosis | |||
| Well differentiated: N (%) | 127 (44.3) | 90 (53.3) | 37 (31.4) |
| Moderately differentiated: N (%) | 85 (29.6) | 53 (31.4) | 32 (27.1) |
| Poorly differentiated: N (%) | 28 (9.8) | 10 (5.9) | 18 (15.3) |
| Lymphovascular invasion at diagnosis: N (%) | 123 (42.9) | 76 (45) | 47 (39.8) |
| Perineural invasion at diagnosis: N (%) | 57 (19.9) | 33 (19.5) | 24 (20.3) |
| T-stage 6 > 2 at diagnosis: N (%) | 191 (66.6) | 127 (75.1) | 85 (72) |
| N-stage 7 > 0 at diagnosis: N (%) | 139 (48.4) | 90 (53.3) | 49 (41.5) |
| HPN staining intensity at diagnosis | |||
| High: N (%) | 122 (42.5) | 71 (42) | 51 (43.2) |
| Medium: N (%) | 104 (36.2) | 64 (37.9) | 40 (33.9) |
| Low: N (%) | 61 (21.3) | 34 (20.1) | 27 (22.9) |
| Multivariate Cox Regression for DFS 1 | ||||||
|---|---|---|---|---|---|---|
| Regressions | Coef 2 | Exp (Coef) 3 | LL 5 95% CI 4 of Exp (Coef) | UL 6 95% CI of Exp (Coef) | Se (Coef) 7 | p8 |
| HPN 9 Medium | 1.04 | 2.84 | 1.08 | 7.49 | 0.50 | 0.035 * |
| HPN High | 1.20 | 3.30 | 1.30 | 8.41 | 0.48 | 0.012 * |
| HPN Low (reference) | - | - | - | - | - | - |
| Moderately differentiated histological grade | 0.53 | 1.69 | 0.95 | 3.02 | 0.29 | 0.073 |
| Poorly differentiated histological grade | 0.97 | 2.65 | 0.84 | 8.29 | 0.58 | 0.095 |
| Well-differentiated histological grade (reference) | - | - | - | - | - | - |
| Lymphovascular invasion | −0.45 | 0.63 | 0.34 | 1.17 | 0.31 | 0.146 |
| Absent lymphovascular invasion (reference) | - | - | - | - | - | - |
| TNM stage III 11 | −0.08 | 0.93 | 0.51 | 1.68 | 0.30 | 0.802 |
| TNM stage II 10 (reference) | - | - | - | - | - | - |
| Overall, N (%) 1 | Localized, N (%) | Metastatic, N (%) | |
|---|---|---|---|
| Head and neck | 4 (6.2) | 2 (6.6) | 2 (5.7) |
| Head and neck + PE 2 | 3 (4.6) | 0 (0) | 3 (8.6) |
| Catheter related | 2 (3.1) | 0 (0) | 2 (5.7) |
| Catheter related + PE | 1 (1.5) | 1 (3.3) | 0 (0) |
| Splanchnic | 9 (13.8) | 6 (20) | 3 (8.6) |
| Splanchnic + PE | 3 (4.6) | 0 (0) | 3 (8.6) |
| Femoral | 10 (15.4) | 4 (13.3) | 6 (17.1) |
| Femoral + PE | 2 (3.1) | 1 (3.3) | 1 (2.9) |
| Calf vein 5 | 2 (3.1) | 1 (3.3) | 1 (2.9) |
| Calf vein + PE | 1 (1.5) | 0 (0) | 1 (2.9) |
| Lower extremity, NOS | 5 (7.7) | 5 (16.7) | 0 (0) |
| DVT 3, NOS 4 | 1 (1.5) | 1 (3.3) | 0 (0) |
| PE, NOS | 22 (33.8) | 9 (30) | 13 (3.9) |
| Total | 65 (100) | 30 (100) | 35 (100) |
| Multivariate Fine and Gray Regression for Cumulative Incidence of Thrombosis | ||||||
|---|---|---|---|---|---|---|
| Regressions | Coef 1 | Exp (Coef) 2 | LL 4 95% CI 3 of Exp (Coef) | UL 5 95% CI of Exp (Coef) | Se (Coef) 6 | p 7 |
| HPN 8 Medium | 2.04 | 7.71 | 1.06 | 55.92 | 1.01 | 0.043 * |
| HPN High | 2.20 | 9.02 | 1.27 | 63.80 | 0.998 | 0.028 * |
| HPN Low (reference) | - | - | - | - | - | - |
| Moderately differentiated histological grade | 0.10 | 1.11 | 0.54 | 2.29 | 0.37 | 0.780 |
| Poorly differentiated histological grade | 0.26 | 0.77 | 0.08 | 7.18 | 1.14 | 0.820 |
| Well-differentiated histological grade (reference) | - | - | - | - | - | - |
| Lymphovascular invasion | 0.37 | 1.45 | 0.68 | 3.07 | 0.38 | 0.330 |
| Absent lymphovascular invasion (reference) | - | - | - | - | - | - |
| TNM stage III 10 | −0.56 | 0.57 | 0.28 | 1.17 | 0.36 | 0.130 |
| TNM stage II 9 (reference) | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaragoza-Huesca, D.; Nieto-Olivares, A.; García-Molina, F.; Ricote, G.; Montenegro, S.; Sánchez-Cánovas, M.; Garrido-Rodríguez, P.; Peñas-Martínez, J.; Vicente, V.; Martínez, F.; et al. Implication of Hepsin from Primary Tumor in the Prognosis of Colorectal Cancer Patients. Cancers 2022, 14, 3106. https://doi.org/10.3390/cancers14133106
Zaragoza-Huesca D, Nieto-Olivares A, García-Molina F, Ricote G, Montenegro S, Sánchez-Cánovas M, Garrido-Rodríguez P, Peñas-Martínez J, Vicente V, Martínez F, et al. Implication of Hepsin from Primary Tumor in the Prognosis of Colorectal Cancer Patients. Cancers. 2022; 14(13):3106. https://doi.org/10.3390/cancers14133106
Chicago/Turabian StyleZaragoza-Huesca, David, Andrés Nieto-Olivares, Francisco García-Molina, Guillermo Ricote, Sofía Montenegro, Manuel Sánchez-Cánovas, Pedro Garrido-Rodríguez, Julia Peñas-Martínez, Vicente Vicente, Francisco Martínez, and et al. 2022. "Implication of Hepsin from Primary Tumor in the Prognosis of Colorectal Cancer Patients" Cancers 14, no. 13: 3106. https://doi.org/10.3390/cancers14133106
APA StyleZaragoza-Huesca, D., Nieto-Olivares, A., García-Molina, F., Ricote, G., Montenegro, S., Sánchez-Cánovas, M., Garrido-Rodríguez, P., Peñas-Martínez, J., Vicente, V., Martínez, F., Lozano, M. L., Carmona-Bayonas, A., & Martínez-Martínez, I. (2022). Implication of Hepsin from Primary Tumor in the Prognosis of Colorectal Cancer Patients. Cancers, 14(13), 3106. https://doi.org/10.3390/cancers14133106