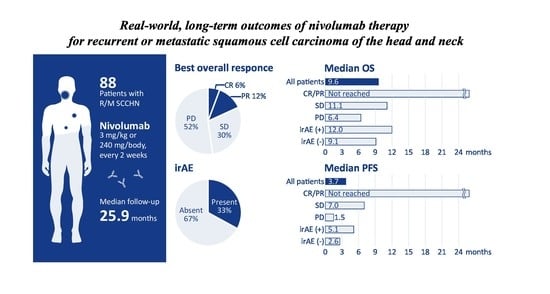
Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
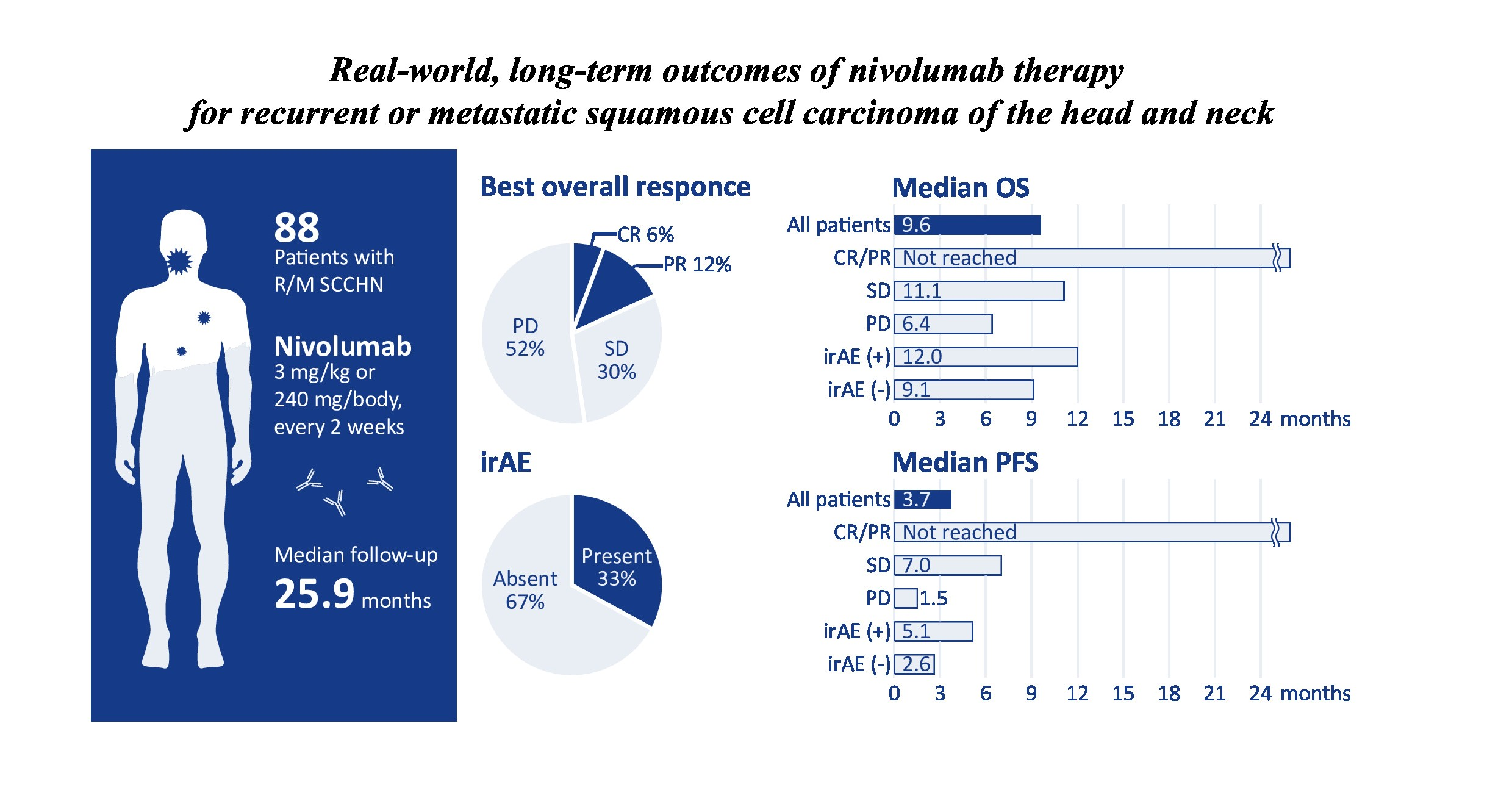
2.2. Treatment Outcomes
2.3. Immune-Related Adverse Events
2.4. Impact of Background Factors on Patient Survival
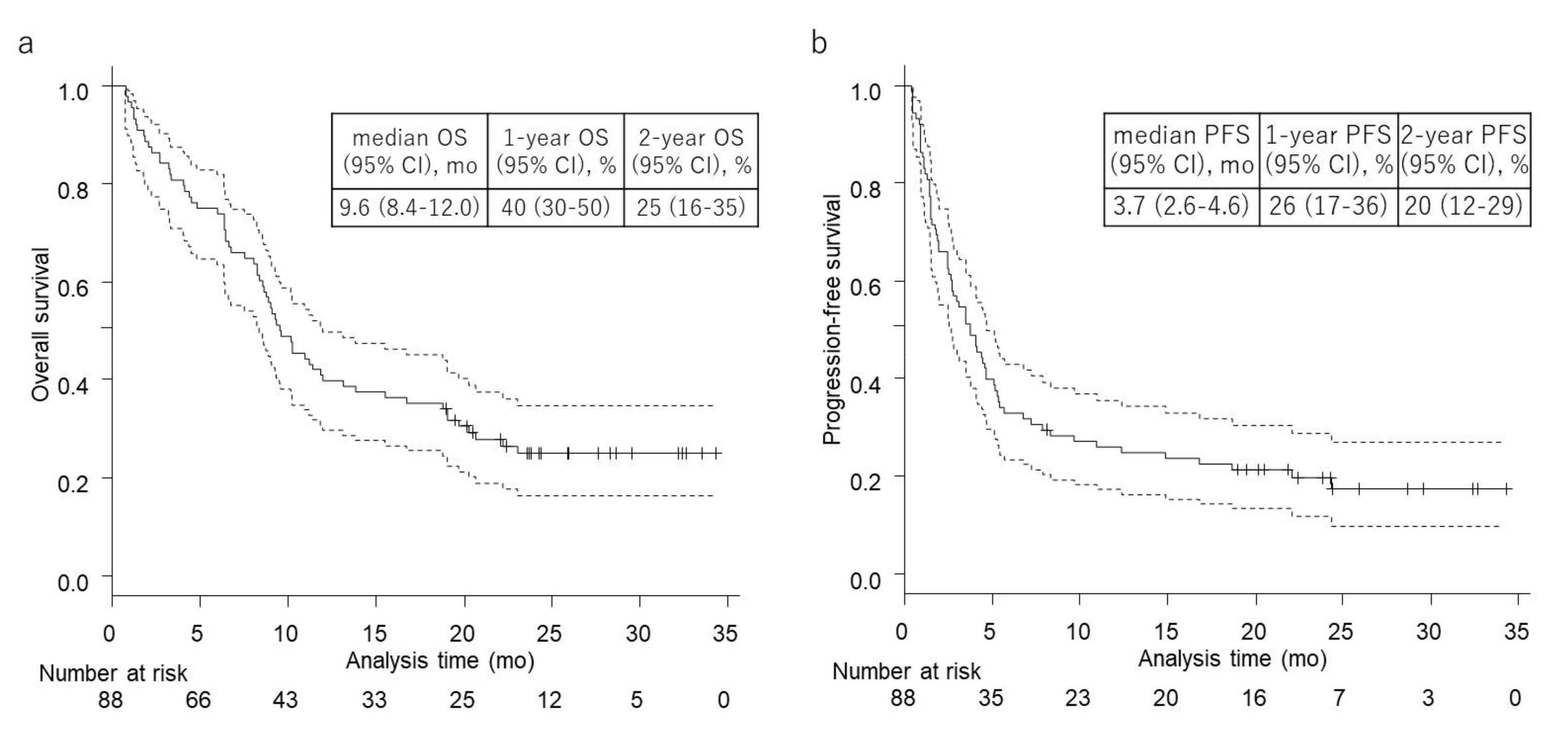
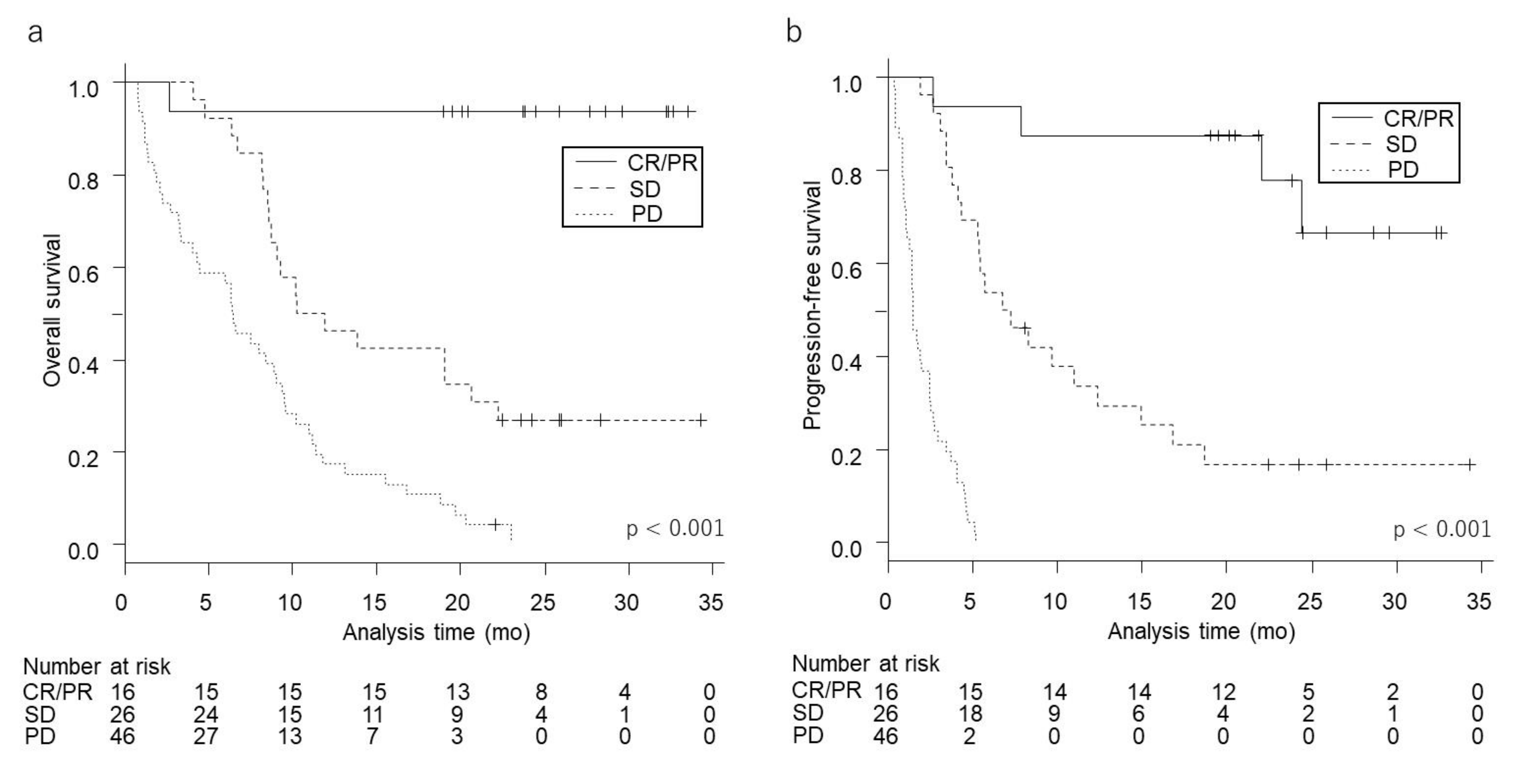
2.5. Survival According to Best Overall Response
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment and Follow-up
4.3. Outcomes
4.4. Immune-Relate Adverse Events
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kiyota, N.; Hasegawa, Y.; Takahashi, S.; Yokota, T.; Yen, C.J.; Iwae, S.; Shimizu, Y.; Hong, R.L.; Goto, M.; Kang, J.H.; et al. A randomized, open-label, Phase III clinical trial of nivolumab vs. therapy of investigator’s choice in recurrent squamous cell carcinoma of the head and neck: A subanalysis of Asian patients versus the global population in checkmate 141. Oral Oncol. 2017, 73, 138–146. [Google Scholar] [CrossRef]
- Hori, R.; Shinohara, S.; Kojima, T.; Kagoshima, H.; Kitamura, M.; Tateya, I.; Tamaki, H.; Kumabe, Y.; Asato, R.; Harada, H.; et al. Real-World Outcomes and Prognostic Factors in Patients Receiving Nivolumab Therapy for Recurrent or Metastatic Head and Neck Carcinoma. Cancers 2019, 11, 1317. [Google Scholar] [CrossRef]
- Ueki, Y.; Takahashi, T.; Ota, H.; Shodo, R.; Yamazaki, K.; Horii, A. Predicting the treatment outcome of nivolumab in recurrent or metastatic head and neck squamous cell carcinoma: Prognostic value of combined performance status and modified Glasgow prognostic score. Eur. Arch. Otorhinolaryngol. 2020, 277, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.; Yokota, T.; Hamauchi, S.; Onozawa, Y.; Kawakami, T.; Shirasu, H.; Notsu, A.; Yasui, H.; Onitsuka, T. Pre-treatment tumor size impacts on response to nivolumab in head and neck squamous cell carcinoma. Auris Nasus Larynx 2020, 47, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, C.; Kiyota, N.; Imamura, Y.; Rikitake, J.; Sai, S.; Koyama, T.; Hyogo, Y.; Nagatani, Y.; Funakoshi, Y.; Toyoda, M.; et al. Effect of tumor burden and growth rate on treatment outcomes of nivolumab in head and neck cancer. Int. J. Clin. Oncol. 2020, 25, 1270–1277. [Google Scholar] [CrossRef] [PubMed]
- Niwa, K.; Kawakita, D.; Nagao, T.; Takahashi, H.; Saotome, T.; Okazaki, M.; Yamazaki, K.; Okamoto, I.; Hirai, H.; Saigusa, N.; et al. Multicentre, retrospective study of the efficacy and safety of nivolumab for recurrent and metastatic salivary gland carcinoma. Sci. Rep. 2020, 10, 16988. [Google Scholar] [CrossRef] [PubMed]
- Fushimi, C.; Okamoto, I.; Matsuki, T.; Masubuchi, T.; Okada, T.; Sato, H.; Tsukahara, K.; Kondo, T.; Yamashita, T.; Hanyu, K.; et al. Salvage Chemotherapy After Nivolumab for Recurrent or Metastatic Head and Neck Carcinoma. Anticancer Res. 2020, 40, 5277–5283. [Google Scholar] [CrossRef]
- Matsuo, M.; Yasumatsu, R.; Masuda, M.; Toh, S.; Wakasaki, T.; Hashimoto, K.; Taura, M.; Uchi, R.; Nakagawa, T. Relationship between immune-related adverse events and the long-term outcomes in recurrent/metastatic head and neck squamous cell carcinoma treated with nivolumab. Oral Oncol. 2020, 101, 104525. [Google Scholar] [CrossRef]
- Okamoto, I.; Sato, H.; Kondo, T.; Koyama, N.; Fushimi, C.; Okada, T.; Miura, K.; Matsuki, T.; Yamashita, T.; Omura, G.; et al. Efficacy and safety of nivolumab in 100 patients with recurrent or metastatic head and neck cancer—A retrospective multicentre study. Acta Otolaryngol 2019, 139, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Matsuki, T.; Okamoto, I.; Fushimi, C.; Sawabe, M.; Kawakita, D.; Sato, H.; Tsukahara, K.; Kondo, T.; Okada, T.; Tada, Y.; et al. Hematological predictive markers for recurrent or metastatic squamous cell carcinomas of the head and neck treated with nivolumab: A multicenter study of 88 patients. Cancer Med. 2020, 9, 5015–5024. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Okamoto, I.; Sato, H.; Koyama, N.; Fushimi, C.; Okada, T.; Masubuchi, T.; Miura, K.; Matsuki, T.; Yamashita, T.; et al. Age-based efficacy and safety of nivolumab for recurrent or metastatic head and neck squamous cell carcinoma: A multicenter retrospective study. Asia Pac. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef]
- Nishikawa, D.; Suzuki, H.; Koide, Y.; Beppu, S.; Kadowaki, S.; Sone, M.; Hanai, N. Prognostic Markers in Head and Neck Cancer Patients Treated with Nivolumab. Cancers 2018, 10, 466. [Google Scholar] [CrossRef]
- Antonia, S.J.; Borghaei, H.; Ramalingam, S.S.; Horn, L.; De Castro Carpeño, J.; Pluzanski, A.; Burgio, M.A.; Garassino, M.; Chow, L.Q.M.; Gettinger, S.; et al. Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: A pooled analysis. Lancet Oncol. 2019, 20, 1395–1408. [Google Scholar] [CrossRef]
- Ishihara, H.; Takagi, T.; Kondo, T.; Tachibana, H.; Fukuda, H.; Yoshida, K.; Iizuka, J.; Kobayashi, H.; Okumi, M.; Ishida, H.; et al. Correlation between the magnitude of best tumor response and patient survival in nivolumab therapy for metastatic renal cell carcinoma. Med. Oncol. 2019, 36, 35. [Google Scholar] [CrossRef] [PubMed]
- Rogado, J.; Sánchez-Torres, J.M.; Romero-Laorden, N.; Ballesteros, A.I.; Pacheco-Barcia, V.; Ramos-Leví, A.; Arranz, R.; Lorenzo, A.; Gullón, P.; Donnay, O.; et al. Immune-related adverse events predict the therapeutic efficacy of anti-PD-1 antibodies in cancer patients. Eur. J. Cancer 2019, 109, 21–27. [Google Scholar] [CrossRef]
- Teraoka, S.; Fujimoto, D.; Morimoto, T.; Kawachi, H.; Ito, M.; Sato, Y.; Nagata, K.; Nakagawa, A.; Otsuka, K.; Uehara, K.; et al. Early Immune-Related Adverse Events and Association with Outcome in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab: A Prospective Cohort Study. J. Thorac. Oncol. 2017, 12, 1798–1805. [Google Scholar] [CrossRef]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of Immune-Related Adverse Events With Nivolumab Efficacy in Non-Small-Cell Lung Cancer. JAMA Oncol. 2018, 4, 374–378. [Google Scholar] [CrossRef]
- Ma, G.; Deng, Y.; Jiang, H.; Li, W.; Wu, Q.; Zhou, Q. The prognostic role of programmed cell death-ligand 1 expression in non-small cell lung cancer patients: An updated meta-analysis. Clin. Chim. Acta 2018, 482, 101–107. [Google Scholar] [CrossRef]
- Wang, Z.; Peng, S.; Xie, H.; Guo, L.; Cai, Q.; Shang, Z.; Jiang, N.; Niu, Y. Prognostic and clinicopathological significance of PD-L1 in patients with renal cell carcinoma: A meta-analysis based on 1863 individuals. Clin. Exp. Med. 2018, 18, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Sun, H.; Zhao, S.; Wang, Y.; Pu, H.; Wang, Y.; Zhang, Q. Expression of PD-L1 and prognosis in breast cancer: A meta-analysis. Oncotarget 2017, 8, 31347–31354. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Caponio, V.C.A.; Zhurakivska, K.; Arena, C.; Pannone, G.; Mascitti, M.; Santarelli, A.; Lo Muzio, L. High PD-L1 expression in the tumour cells did not correlate with poor prognosis of patients suffering for oral squamous cells carcinoma: A meta-analysis of the literature. Cell Prolif. 2019, 52, e12537. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.Q.; Yang, B.; Wen, L.L.; Mu, W.X.; Wang, Z.; Cheng, B. Prognostic value of immune checkpoint molecules in head and neck cancer: A meta-analysis. Aging 2019, 11, 501–522. [Google Scholar] [CrossRef] [PubMed]
- Queirolo, P.; Spagnolo, F. Atypical responses in patients with advanced melanoma, lung cancer, renal-cell carcinoma and other solid tumors treated with anti-PD-1 drugs: A systematic review. Cancer Treat. Rev. 2017, 59, 71–78. [Google Scholar] [CrossRef]
- Lauber, K.; Dunn, L. Immunotherapy Mythbusters in Head and Neck Cancer: The Abscopal Effect and Pseudoprogression. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 352–363. [Google Scholar] [CrossRef]
- Ferrara, R.; Pilotto, S.; Caccese, M.; Grizzi, G.; Sperduti, I.; Giannarelli, D.; Milella, M.; Besse, B.; Tortora, G.; Bria, E. Do immune checkpoint inhibitors need new studies methodology? J. Thorac. Dis. 2018, 10, S1564–S1580. [Google Scholar] [CrossRef]
- Vivot, A.; Créquit, P.; Porcher, R. Use of Late-Life Expectancy for Assessing the Long-Term Benefit of Immune Checkpoint Inhibitors. J. Natl. Cancer Inst. 2019, 111, 519–521. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 88 | (%) |
|---|---|---|
| Sex | ||
| Male | 71 | (81) |
| Female | 17 | (19) |
| Age | ||
| <65 years | 39 | (44) |
| ≥65 years | 49 | (56) |
| ECOG performance status | ||
| 0 | 59 | (67) |
| 1 | 24 | (27) |
| ≥2 | 5 | (6) |
| Primary site | ||
| Nasopharynx | 10 | (11) |
| Oropharynx | 19 | (22) |
| p16-positive | 8 | (9) |
| Hypopharynx | 21 | (24) |
| Larynx | 10 | (11) |
| Oral cavity | 17 | (19) |
| Paranasal sinus | 6 | (7) |
| Salivary gland | 2 | (2) |
| External auditory canal | 3 | (3) |
| Histology | ||
| Squamous cell carcinoma | 88 | (100) |
| Smoking | ||
| Ever | 61 | (69) |
| Never | 26 | (30) |
| Unknown | 1 | (1) |
| Alcohol | ||
| Ever | 69 | (78) |
| Never | 17 | (19) |
| Unknown | 2 | (2) |
| Distant metastasis | ||
| Present | 26 | (30) |
| Absent | 52 | (59) |
| Previous exposure to cetuximab | ||
| Yes | 30 | (34) |
| No | 58 | (66) |
| Platinum refractoriness a | ||
| Yes | 28 | (32) |
| No | 60 | (68) |
| Previous radiotherapy | ||
| Yes | 17 | (19) |
| No | 71 | (81) |
| Previous number of chemotherapy regimens b | ||
| 1 | 37 | (42) |
| 2 | 35 | (40) |
| ≥3 | 16 | (18) |
| PD-L1 expression | (0) | |
| Positive (≥1%) | 37 | (42) |
| Negative (<1%) | 7 | (8) |
| Unknown | 44 | (50) |
| Institution | (0) | |
| TMU | 41 | (47) |
| IUHW | 24 | (27) |
| KU | 15 | (17) |
| TMU/HMC | 8 | (9) |
| Best Overall Response | N = 88 | (%) |
|---|---|---|
| Complete response (CR) | 5 | (6) |
| Partial response (PR) | 11 | (13) |
| Stable disease (SD) | 26 | (30) |
| Progressive disease (PD) | 46 | (52) |
| Response rate (CR + PR) | 16 | (18) |
| Disease control rate (CR + PR + SD) | 42 | (48) |
| Immune-Related Adverse Events | Any Grade | Grade 3–5 |
|---|---|---|
| Interstitial lung disease | 13 | 5 |
| Thyroid dysfunction | 8 | 0 |
| Liver dysfunction | 5 | 3 |
| Skin disorders | 4 | 1 |
| Enteritis | 1 | 1 |
| Adrenal insufficiency | 1 | 0 |
| Infusion reactions | 1 | 0 |
| Myositis | 1 | 0 |
| Parathyroid dysfunction | 1 | 0 |
| Pituitary dysfunction | 1 | 0 |
| Renal dysfunction | 1 | 0 |
| Rheumatoid arthritis | 1 | 0 |
| Total | 38 | 10 |
| (29 patients) | (9 patients) |
| Overall Survival | Progression-Free Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| Background Factors | Crude | Adjusted a | Crude | Adjusted a | ||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Sex | ||||||||
| Male (Ref. Female) | 1.03 (0.54–1.98) | 0.922 | 0.54 (0.22–1.34) | 0.185 | 1.19 (0.64–2.23) | 0.581 | 0.64 (0.28–1.45) | 0.281 |
| Age | ||||||||
| ≥65 years (Ref. < 65 years) | 1.37 (0.83–2.24) | 0.216 | 1.27 (0.76–2.14) | 0.362 | 0.97 (0.61–1.56) | 0.914 | 0.79 (0.48–1.30) | 0.354 |
| ECOG performance status | ||||||||
| 2–3 (Ref. 0–1) | 16.91 (5.69–50.32) | <0.001 | 20.07 (6.35–63.39) | <0.001 | 6.00 (2.31–15.53) | <0.001 | 7.87 (2.77–22.35) | <0.001 |
| Smoking | ||||||||
| Ever (Ref. Never) | 1.17 (0.67–2.04) | 0.583 | 0.86 (0.42–1.75) | 0.669 | 1.16 (0.69–1.94) | 0.587 | 0.86 (0.45–1.66) | 0.660 |
| Alcohol consumption | ||||||||
| Ever (Ref. Never) | 1.51 (0.77–2.98) | 0.230 | 1.64 (0.67–4.03) | 0.278 | 1.61 (0.84–3.08) | 0.149 | 1.60 (0.71–3.60) | 0.257 |
| Distant metastasis | ||||||||
| Present (Ref. Absent) | 0.94 (0.57–1.55) | 0.818 | 0.95 (0.59–1.53) | 0.844 | ||||
| Previous exposure to cetuximab | ||||||||
| Yes (Ref. No) | 1.43 (0.84–2.45) | 0.188 | 1.71 (1.02–2.88) | 0.042 | ||||
| Platinum refractoriness | ||||||||
| Yes (Ref. No) | 1.69 (0.98–2.91) | 0.060 | 1.55 (0.80–3.01) | 0.196 | 1.80 (1.07–3.05) | 0.028 | 1.78 (0.96–3.30) | 0.067 |
| Previous radiotherapy | ||||||||
| Yes (Ref. No) | 1.05 (0.56–1.96) | 0.883 | 0.83 (0.46–1.50) | 0.539 | ||||
| Previous number of chemotherapy regimens | ||||||||
| two or more (Ref. 1) | 1.05 (0.63–1.73) | 0.860 | 1.12 (0.70–1.80) | 0.640 | ||||
| PD-L1 expression | ||||||||
| Positive (Ref. Negative) | 0.58 (0.25–1.35) | 0.203 | 0.50 (0.21–1.19) | 0.117 | ||||
| p16 expression | ||||||||
| Positive (Ref. Negative or Unknown) | 0.66 (0.28–1.53) | 0.332 | 0.76 (0.35–1.66) | 0.490 | ||||
| Immune-related adverse events | ||||||||
| Yes (Ref. No) | 0.60 (0.35–1.03) | 0.065 | 0.54 (0.31–0.96) | 0.036 | 0.59 (0.35–0.98) | 0.040 | 0.53 (0.31–0.92) | 0.023 |
| Overall Survival | |||||||||||
| Crude | |||||||||||
| N = 88 | (%) | median (months) | (95% CI) | 1-year OS (%) | (95% CI) | 2-year OS (%) | (95% CI) | HR | (95% CI) | p-value | |
| CR/PR | 16 | (18) | NR | 94 | (63–99) | 94 | (63–99) | 0.02 | (0.003–0.15) | <0.001 | |
| SD | 26 | (30) | 11.1 | (8.6–20.7) | 46 | (27–64) | 27 | (12–45) | 0.37 | (0.21–0.65) | 0.001 |
| PD | 46 | (52) | 6.4 | (3.3–9.0) | 17 | (8–30) | 0 | (NA-NA) | 1 (reference) | ||
| Progression-Free Survival | |||||||||||
| Crude | |||||||||||
| N = 88 | (%) | median (months) | (95% CI) | 1-year PFS (%) | (95% CI) | 2-year PFS (%) | (95% CI) | HR | (95% CI) | p-value | |
| CR/PR | 16 | (18) | NR | (22.1-NA) | 88 | (59–97) | 78 | (44–93) | 0.02 | (0.005–0.06) | <0.001 |
| SD | 26 | (30) | 7.0 | (4.3–12.4) | 34 | (16–52) | 17 | (5–34) | 0.10 | (0.05–0.22) | <0.001 |
| PD | 46 | (52) | 1.5 | (1.1–2.5) | NA | (NA-NA) | 0 | (NA-NA) | 1 (reference) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuki, T.; Okamoto, I.; Fushimi, C.; Takahashi, H.; Okada, T.; Kondo, T.; Sato, H.; Ito, T.; Tokashiki, K.; Tsukahara, K.; et al. Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients. Cancers 2020, 12, 3427. https://doi.org/10.3390/cancers12113427
Matsuki T, Okamoto I, Fushimi C, Takahashi H, Okada T, Kondo T, Sato H, Ito T, Tokashiki K, Tsukahara K, et al. Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients. Cancers. 2020; 12(11):3427. https://doi.org/10.3390/cancers12113427
Chicago/Turabian StyleMatsuki, Takashi, Isaku Okamoto, Chihiro Fushimi, Hideaki Takahashi, Takuro Okada, Takahito Kondo, Hiroki Sato, Tatsuya Ito, Kunihiko Tokashiki, Kiyoaki Tsukahara, and et al. 2020. "Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients" Cancers 12, no. 11: 3427. https://doi.org/10.3390/cancers12113427
APA StyleMatsuki, T., Okamoto, I., Fushimi, C., Takahashi, H., Okada, T., Kondo, T., Sato, H., Ito, T., Tokashiki, K., Tsukahara, K., Hanyu, K., Masubuchi, T., Tada, Y., Miura, K., Omura, G., Sawabe, M., Kawakita, D., & Yamashita, T. (2020). Real-World, Long-Term Outcomes of Nivolumab Therapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck and Impact of the Magnitude of Best Overall Response: A Retrospective Multicenter Study of 88 Patients. Cancers, 12(11), 3427. https://doi.org/10.3390/cancers12113427