Does an Alternative Sunitinib Dosing Schedule Really Improve Survival Outcomes Over a Conventional Dosing Schedule in Patients with Metastatic Renal Cell Carcinoma? An Updated Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Study Eligibility
2.3. Data Extraction
2.4. Study Quality Assessments
2.5. Statistical Analysis
3. Results
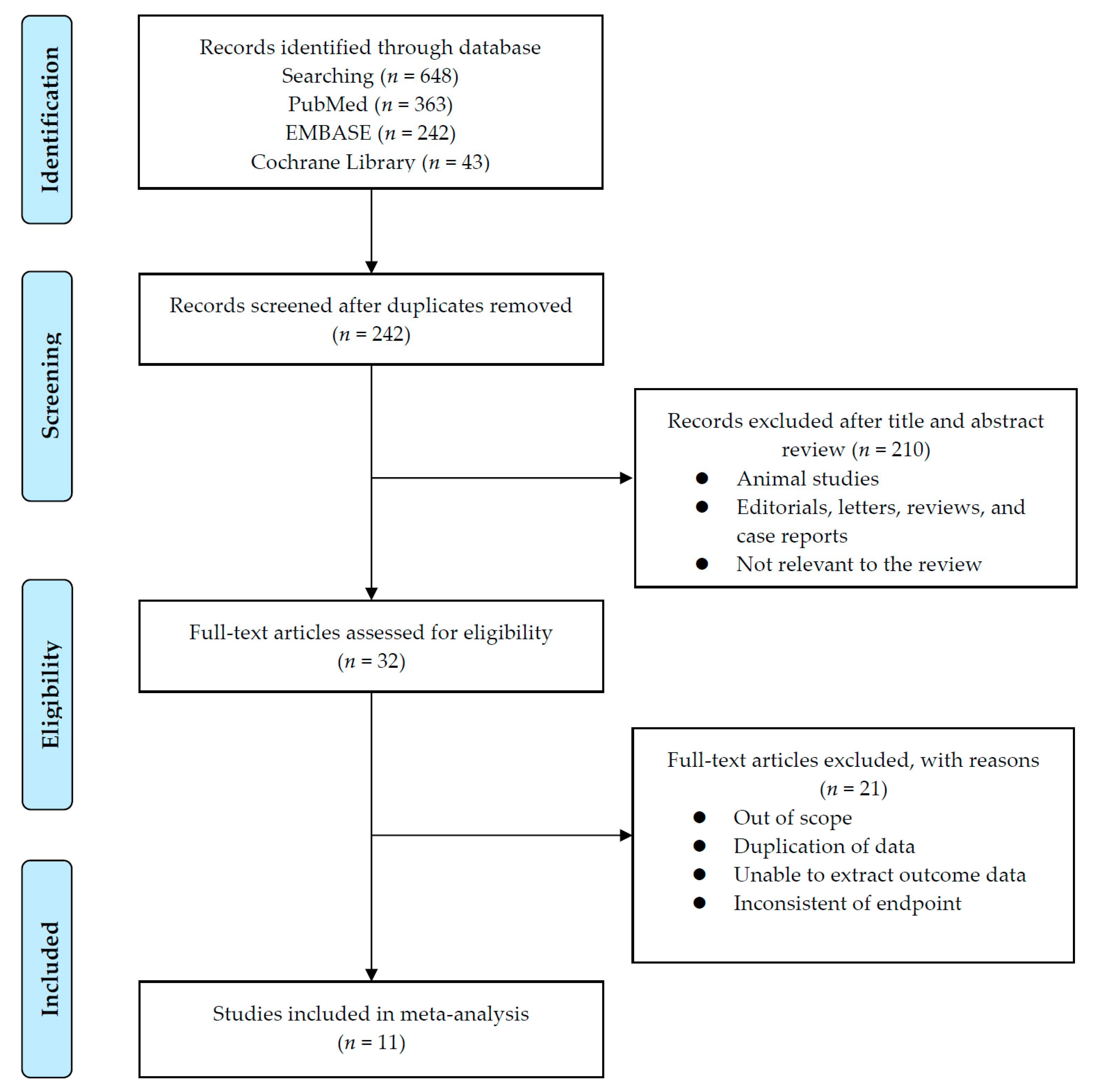
3.1. Systematic Review Process
3.2. Quality Assessment
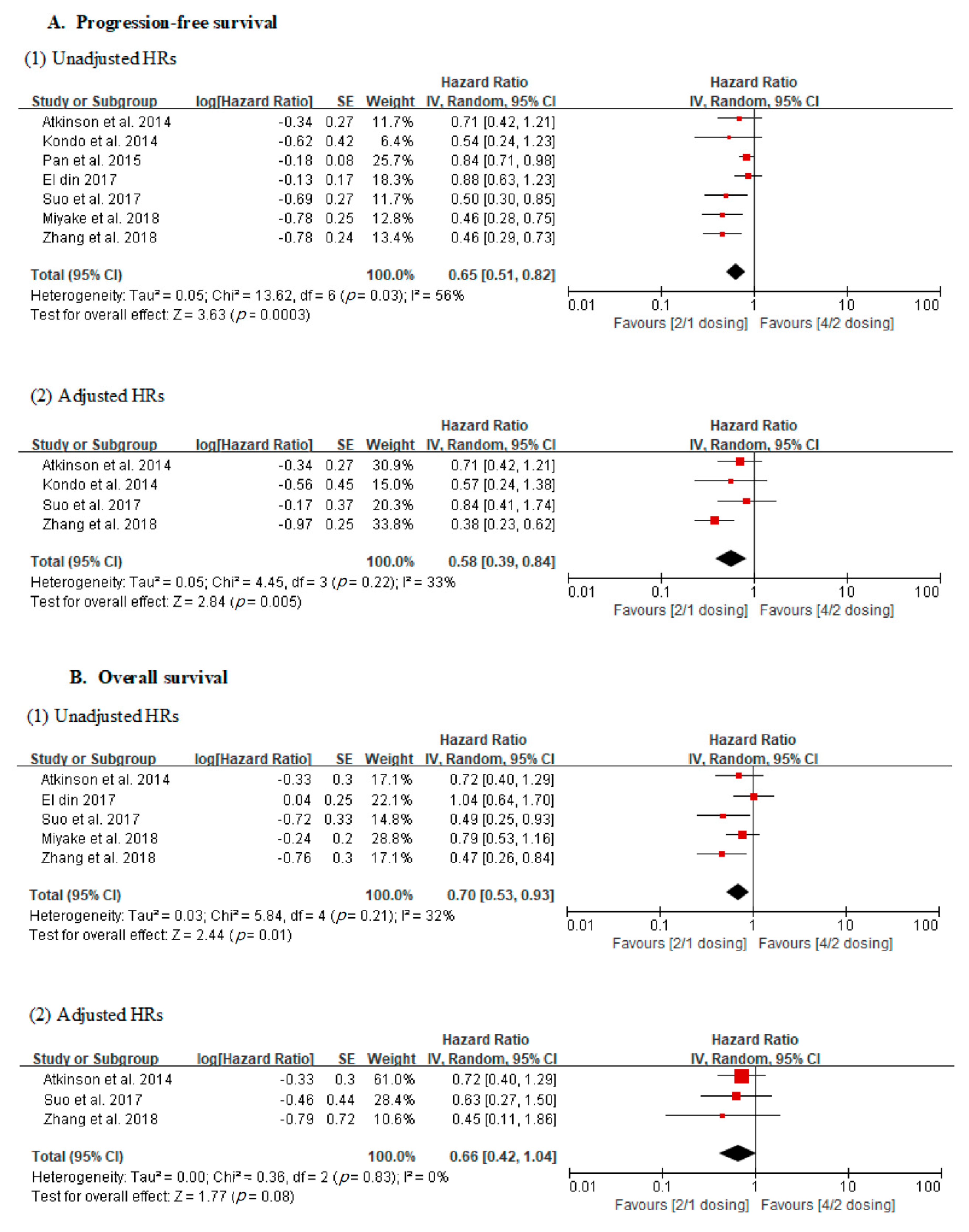
3.3. Oncological Outcomes; Progression-Free Survival and Overall Survival
3.4. Incidence of Adverse Events
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Najjar, Y.G.; Rini, B.I. Novel agents in renal carcinoma: A reality check. Ther. Adv. Med. Oncol. 2012, 4, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Takagi, T.; Kobayashi, H.; Iizuka, J.; Nozaki, T.; Hashimoto, Y.; Ikezawa, E.; Yoshida, K.; Omae, K.; Tanabe, K. Superior tolerability of altered dosing schedule of sunitinib with 2-weeks-on and 1-week-off in patients with metastatic renal cell carcinoma--comparison to standard dosing schedule of 4-weeks-on and 2-weeks-off. Jpn. J. Clin. Oncol. 2014, 44, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Najjar, Y.G.; Mittal, K.; Elson, P.; Wood, L.; Garcia, J.A.; Dreicer, R.; Rini, B.I. A 2 weeks on and 1 week off schedule of sunitinib is associated with decreased toxicity in metastatic renal cell carcinoma. Eur. J. Cancer 2014, 50, 1084–1089. [Google Scholar] [CrossRef]
- Bracarda, S.; Iacovelli, R.; Boni, L.; Rizzo, M.; Derosa, L.; Rossi, M.; Galli, L.; Procopio, G.; Sisani, M.; Longo, F.; et al. Sunitinib administered on 2/1 schedule in patients with metastatic renal cell carcinoma: The RAINBOW analysis. Ann. Oncol. 2015, 26, 2107–2113. [Google Scholar] [CrossRef]
- Lee, J.L.; Kim, M.K.; Park, I.; Ahn, J.H.; Lee, D.H.; Ryoo, H.M.; Song, C.; Hong, B.; Hong, J.H.; Ahn, H. RandomizEd phase II trial of Sunitinib four weeks on and two weeks off versus Two weeks on and One week off in metastatic clear-cell type REnal cell carcinoma: RESTORE trial. Ann. Oncol. 2015, 26, 2300–2305. [Google Scholar] [CrossRef]
- Miyake, H.; Harada, K.; Miyazaki, A.; Fujisawa, M. Improved health-related quality of life of patients with metastatic renal cell carcinoma treated with a 2 weeks on and 1 week off schedule of sunitinib. Med. Oncol. 2015, 32. [Google Scholar] [CrossRef]
- Pan, X.; Huang, H.; Huang, Y.; Liu, B.; Cui, X.; Gan, S.; Ye, J.; Xu, D.; Chen, L.; Zhou, Q.; et al. Sunitinib dosing schedule 2/1 improves tolerability, efficacy, and health-related quality of life in Chinese patients with metastatic renal cell carcinoma. Urol. Oncol. 2015, 33, 268.e9–268.e15. [Google Scholar] [CrossRef]
- El Din, M.E. Sunitinib 4/2 Versus 2/1 Schedule for Patients With Metastatic Renal Cell Carcinoma: Tertiary Care Hospital Experience. Clin. Genitourin. Cancer 2017, 15, E455–E462. [Google Scholar] [CrossRef]
- Suo, A.; Iqbal, U.; Lim, J.; Lee, C.; Gesy, K.; Iqbal, N.; Abbas, T. Outcomes and Drug Costs of Sunitinib Regimens for Metastatic Renal Cell Carcinoma: A Provincial Population-Based Study. Clin. Genitourin. Cancer 2017, 15, e397–e404. [Google Scholar] [CrossRef]
- Miyake, H.; Matsushita, Y.; Watanabe, H.; Tamura, K.; Suzuki, T.; Motoyama, D.; Ito, T.; Sugiyama, T.; Otsukav, A. Significance of introduction of alternative dosing schedule for sunitinib during first-line treatment of patients with metastatic renal cell carcinoma. Med. Oncol. 2018, 35, 133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Sun, G.X.; Zhao, J.G.; Shu, K.P.; Zhao, P.; Liu, J.D.; Yang, Y.J.; Tang, Q.D.; Chen, J.R.; Shen, P.F.; et al. Improved Long-Term Clinical Outcomes And Safety Profile Of Sunitinib Dosing Schedule With 4/2 Switched To 2/1 In Patients With Metastatic Renal Cell Carcinoma. J. Cancer 2018, 9, 3303–3310. [Google Scholar] [CrossRef]
- Atkinson, B.J.; Kalra, S.; Wang, X.; Bathala, T.; Corn, P.; Tannir, N.M.; Jonasch, E. Clinical outcomes for patients with metastatic renal cell carcinoma treated with alternative sunitinib schedules. J. Urol. 2014, 191, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Olsen, M.R.; Hudes, G.R.; Burke, J.M.; Edenfield, W.J.; Wilding, G.; Agarwal, N.; Thompson, J.A.; Cella, D.; et al. Randomized Phase II Trial of Sunitinib on an Intermittent Versus Continuous Dosing Schedule As First-Line Therapy for Advanced Renal Cell Carcinoma. J. Clin. Oncol. 2012, 30, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Jonasch, E.; Slack, R.S.; Geynisman, D.M.; Hasanov, E.; Milowsky, M.I.; Rathmell, W.K.; Stovall, S.; Juarez, D.; Gilchrist, T.R.; Pruitt, L.; et al. Phase II Study of Two Weeks on, One Week off Sunitinib Scheduling in Patients With Metastatic Renal Cell Carcinoma. J. Clin. Oncol. 2018, 36, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Fang, H.; Jiao, Y.; Zhou, Y.; Guo, Q.; Lv, Z. Clinical Efficacy and Complication Rate of Sunitinib 2/1 Versus 4/2 Schedule for the Treatment of Metastatic Renal Cell Cancer: A Systematic Review and Meta-Analysis. Clin. Genitourin. Cancer 2019. [Google Scholar] [CrossRef]
- Sun, Y.; Li, J.; Yang, X.; Zhang, G.; Fan, X. The Alternative 2/1 Schedule of Sunitinib is Superior to the Traditional 4/2 Schedule in Patients with Metastatic Renal Cell Carcinoma: A Meta-analysis. Clin. Genitourin. Cancer 2019. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schunemann, H.J.; Group, G.W. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Berkey, C.S.; Hoaglin, D.C.; Mosteller, F.; Colditz, G.A. A random-effects regression model for meta-analysis. Stat. Med. 1995, 14, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Faber, T.; Ravaud, P.; Riveros, C.; Perrodeau, E.; Dechartres, A. Meta-analyses including non-randomized studies of therapeutic interventions: A methodological review. BMC Med. Res. Methodol. 2016, 16, 35. [Google Scholar] [CrossRef]
- Voils, C.I.; Crandell, J.L.; Chang, Y.; Leeman, J.; Sandelowski, M. Combining adjusted and unadjusted findings in mixed research synthesis. J. Eval. Clin. Pract. 2011, 17, 429–434. [Google Scholar] [CrossRef]
- Amzal, B.; Fu, S.; Meng, J.; Lister, J.; Karcher, H. Cabozantinib versus everolimus, nivolumab, axitinib, sorafenib and best supportive care: A network meta-analysis of progression-free survival and overall survival in second line treatment of advanced renal cell carcinoma. PLoS ONE 2017, 12, e0184423. [Google Scholar] [CrossRef]
- Porta, C.; Szczylik, C.; Casciano, R.; Fu, S.; Amzal, B.; Lister, J.; Karcher, H.; Meng, J.; Neumann, M.; Dinet, J. Second-line cabozantinib versus nivolumab in advanced renal cell carcinoma: Systematic review and indirect treatment comparison. Crit. Rev. Oncol. Hematol. 2019, 139, 143–148. [Google Scholar] [CrossRef]
- Cella, D. Quality of life in patients with metastatic renal cell carcinoma: The importance of patient-reported outcomes. Cancer Treat. Rev. 2009, 35, 733–737. [Google Scholar] [CrossRef]
- Cella, D.; Davis, M.P.; Negrier, S.; Figlin, R.A.; Michaelson, M.D.; Bushmakin, A.G.; Cappelleri, J.C.; Sandin, R.; Korytowsky, B.; Charbonneau, C.; et al. Characterizing Fatigue Associated With Sunitinib and Its Impact on Health-Related Quality of Life in Patients With Metastatic Renal Cell Carcinoma. Cancer 2014, 120, 1871–1880. [Google Scholar] [CrossRef]
- Houk, B.E.; Bello, C.L.; Poland, B.; Rosen, L.S.; Demetri, G.D.; Motzer, R.J. Relationship between exposure to sunitinib and efficacy and tolerability endpoints in patients with cancer: Results of a pharmacokinetic/pharmacodynamic meta-analysis. Cancer Chemother. Pharmacol. 2010, 66, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Chung, H.S.; Hwang, E.C.; Jung, S.I.; Kwon, D.D.; Hwang, J.E.; Bae, W.K.; Park, J.Y.; Jeong, C.W.; Kwak, C.; et al. Efficacy of First-Line Targeted Therapy in Real-World Korean Patients with Metastatic Renal Cell Carcinoma: Focus on Sunitinib and Pazopanib. J. Korean Med. Sci. 2018, 33, e325. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, G.A.; Knox, J.J.; Kollmannsberger, C.K.; Soulieres, D.; Ernst, D.S.; Zalewski, P.; Canil, C.M.; Winquist, E.; Hotte, S.J.; North, S.A.; et al. The efficacy and safety of sunitinib given on an individualised schedule as first-line therapy for metastatic renal cell carcinoma: A phase 2 clinical trial. Eur. J. Cancer 2019, 108, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, M.C.; Pal, S.K.; Wood, L.S.; Tomer, J.M.; Hobbs, B.P.; Jia, X.S.; Allman, K.D.; Martin, A.; Olencki, T.; Davis, N.B.; et al. Individualised axitinib regimen for patients with metastatic renal cell carcinoma after treatment with checkpoint inhibitors: A multicentre, single-arm, phase 2 study. Lancet Oncol. 2019, 20, 1386–1394. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Motzer, R.J.; Hutson, T.E.; Choueiri, T.K.; Kollmannsberger, C.; Bjarnason, G.A.; Paul, N.; Porta, C.; Grunwald, V.; Dezzani, L.; et al. COMPARZ Post Hoc Analysis: Characterizing Pazopanib Responders With Advanced Renal Cell Carcinoma. Clin. Genitourin. Cancer 2019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author(s) (Year) | Country | Study Design | Study Summary |
| Schedule | No. of Patients | Follow up (Months) | PFS (Months, IQR) | OS (Months, IQR) |
|---|---|---|---|---|---|---|---|---|---|
| Atkinson et al. (2014) | USA | Retrospective | Comparisons of oncological outcomes and incidence of adverse events between two groups: 2/1 and 4/2, 4/2 to 2/1 switch |
| 2/1 dosing | 24 | NR | Median 11.6 (5.8–18.3) | Median 27.7 (21.2–NE) |
| 4/2 dosing | 98 | Median 4.3 (3.4–6.4) | Median 17.7 (10.8–22.2) | ||||||
| Kondo et al. (2014) | Japan | Retrospective | Comparisons of oncological outcomes and incidence of adverse events between two groups: 2/1 and 4/2 |
| 2/1 dosing | 26 | Mean 11.9 ± 8.1 (range 2.6–31.6) | Median 18.4 (NR) | NR |
| 4/2 dosing | 22 | Mean 13.3 ± 10.1 (range 1.5–39.1) | Median 9.1 (NR) | ||||||
| Najjar et al. (2014) | Japan | Retrospective | Comparisons of incidence of adverse events between two groups: 2/1 and 4/2 |
| 2/1 dosing | 30 | Median 11.9 (range 0.9–73.3) | NR | NR |
| 4/2 dosing | 30 | Median 12.6 (range 1.2–62) | |||||||
| Bracarda et al. (2015) | Europe | Retrospective | Comparisons of oncological outcomes and incidence of adverse events among three groups: 2/1, 4/2, and 4/2 to 2/1 switch |
| 2/1 dosing | 41 | Median 7.8 (IQR 5.8–22.4) | NR | NR |
| 4/2 dosing | 208 | Median 4.3 (IQR 2.0–12.0) | |||||||
| Lee et al. (2015) | South Korea | Randomized controlled | Comparisons of oncological outcomes and incidence of adverse events between two groups: 2/1 and 4/2 |
| 2/1 dosing | 38 | Median 30.0 (IQR 19.5–53.6) | Median 12.1 (4.0–25.3) | Median 30.5 (18.9–42.0) |
| 4/2 dosing | 36 | Median 10.1 (7.5–12.7) | Median 28.4 (11.3–45.4) | ||||||
| Miyake et al. (2015) | Japan | Retrospective | Comparisons of incidence of adverse events between two groups: 2/1 and 4/2 |
| 2/1 dosing | 45 | Median 3.4 (range 1.3–19.7) | NR | NR |
| 4/2 dosing | 45 | Median 8.9 (range 2.3–21.4) | |||||||
| Pan et al. (2015) | China | Retrospective | Comparisons of oncological outcomes and incidence of adverse events among three groups: 2/1, 4/2, and 4/2 to 2/1 switch |
| 2/1 dosing | 32 | Median 1.5 years (range 1.0–2.2) | Median 11.2 (NR) | NR |
| 4/2 dosing | 50 | Median 1.9 years (range 1.3–2.7) | Median 9.5 (NR) | NR | |||||
| El Din (2017) | Egypt | Retrospective | Comparisons of oncological outcomes and incidence of adverse events between two groups: 2/1 and 4/2 |
| 2/1 dosing | 26 | Median 23 (range 3–43) | Median 17 (2–43) | Median 24 (2–42) |
| 4/2 dosing | 30 | Median 24 (range 2–42) | Median 15 (1–42) | Median 23 (3–43) | |||||
| Suo et al. (2017) | Canada | Retrospective | Comparisons of oncological outcomes and incidence of adverse events among three groups: 2/1, 4/2, 2/1 modified dosing (37.5 mg, 25 mg, or 12.5 mg) and continuous dosing (37.5 mg, 25 mg, or 12.5 mg) |
| 2/1 dosing | 9 | NR | Median 6.0 (NR) | Median 23.1 (NR) |
| 4/2 dosing | 59 | Median 3.0 (NR) | Median 11.2 (NR) | ||||||
| Miyake et al. (2018) | Japan | Retrospective | Comparisons of oncological outcomes and incidence of adverse events among three groups: 2/1, 4/2, and 4/2 to 2/1 switch |
| 2/1 dosing | 47 | NR | Median 13.8 (NR) | Median 39.2 (NR) |
| 4/2 dosing | 62 | Median 6.3 (NR) | Median 30.8 (NR) | ||||||
| Zhang et al. (2018) | China | Retrospective | Comparisons of oncological outcomes and incidence of adverse events among three groups: 2/1, 4/2, and 4/2 to 2/1 switch |
| 2/1 dosing | 24 | Median 37 | Median 11 (NR) | Median 28 (NR) |
| 4/2 dosing | 30 | Median 12.5 (NR) | Median 21 (NR) |
| A. Quality assessment of a randomized controlled trial | |||||||||||
| Author(s) (Year) | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data Addressed (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | ||||
| Lee et al. (2015) | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Unclear | ||||
| B. Quality assessment of nonrandomized studies | |||||||||||
| Author(s) (Year) | Selection (4) | Comparability (2) | Exposure (3) | Total score | |||||||
| Adequate Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Control for Important Factor or Additional Factor | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | ||||
| Atkinson et al. (2014) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Kondo et al. (2014) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Najjar et al. (2014) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Bracarda et al. (2015) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Miyake et al. (2015) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Pan et al. (2015) | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 0 | 5 | ||
| El Din (2017) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Suo et al. (2017) | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 0 | 5 | ||
| Miyake et al. (2018) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 | ||
| Zhang et al. (2018) | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 0 | 5 | ||
| No. of Studies | Study Design | Risk of Bios | Inconsistency | Indirectness | Imprecision | Other Consideration | No. of Patients | Effect | Overall Quality of Evidence | |
|---|---|---|---|---|---|---|---|---|---|---|
| 2/1 Schedule | 4/2 Schedule | |||||||||
| 1. Progression-free survival | ||||||||||
| 7 Unadjusted | observational studies | not serious | not serious | not serious | Serious * | none | 188 | 351 | HR 0.66 (0.54–0.82) | Very low |
| 4 Adjusted | observational studies | not serious | not serious | not serious | Serious ** | none | 83 | 209 | HR 0.58 (0.39–0.84) | Very low |
| 2. Overall survival | ||||||||||
| 5 Unadjusted | observational studies | not serious | not serious | not serious | Serious * | none | 130 | 279 | HR 0.75 (0.57–0.99) | Very low |
| 3 Adjusted | observational studies | not serious | not serious | not serious | Serious ** | none | 57 | 187 | HR 0.66 (0.42–1.04) | Very low |
| Study (year) | Schedule | No. of Patients | Complication (No.) | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hypo-Thyroidism | Leukopenia | Anemia | Thrombo-cytopenia | Liver Dysfunction | Anorexia | Nausea | Vomiting | Diarrhea | Dysgeusia | HFS | HTN | Fatigue | Stomatitis | Skin Color Change | ||||||||||||||||||
| Al * | HG | Al * | HG * | All | HG | All | HG * | All | HG | All | HG | All | HG | All | HG | All * | HG | All * | HG | All * | HG | All * | HG * | All * | HG * | All * | HG * | All * | HG | |||
| Kondo et al. (2014) | 2/1 | 26 | 10 | 0 | 22 | 5 | 20 | 3 | 24 | 5 | 18 | 0 | 11 | 1 | NR | NR | NR | NR | 9 | 0 | 6 | 0 | 15 | 0 | 16 | 0 | 19 | 1 | 10 | 0 | NR | NR |
| 4/2 | 22 | 13 | 0 | 18 | 1 | 19 | 1 | 19 | 6 | 16 | 0 | 14 | 1 | NR | NR | NR | NR | 16 | 1 | 10 | 0 | 19 | 2 | 17 | 0 | 19 | 1 | 13 | 0 | NR | NR | |
| Najjar et al. (2014) | 2/1 | 30 | 13 | 0 | 1 | 1 | NR | NR | 2 | 0 | NR | NR | 2 | 1 | 2 | 1 | NR | NR | 11 | 1 | NR | NR | 5 | 0 | 8 | 2 | 16 | 2 | 3 | 0 | NR | NR |
| 4/2 | 30 | 11 | 2 | 6 | 3 | NR | NR | 6 | 3 | NR | NR | 7 | 2 | 6 | 2 | NR | NR | 12 | 6 | NR | NR | 15 | 8 | 8 | 6 | 21 | 11 | 6 | 2 | NR | NR | |
| Bracarda et al. (2015) | 2/1 | 41 | 11 | 1 | NR | NR | NR | NR | 10 | 0 | NR | NR | 6 | 2 | 8 | 1 | 1 | 0 | 2 | 5 | 7 | 0 | 15 | 2 | 8 | 1 | 26 | 2 | 14 | 1 | NR | NR |
| 4/2 | 208 | 77 | 3 | NR | NR | NR | NR | 69 | 16 | NR | NR | 54 | 5 | 63 | 6 | 18 | 1 | 87 | 8 | 68 | 1 | 116 | 21 | 95 | 19 | 155 | 21 | 127 | 14 | NR | NR | |
| Lee et al. (2015) | 2/1 | 38 | 17 | 0 | 14 | 4 | 27 | 5 | 27 | 9 | 9 | 0 | 21 | 0 | 12 | 0 | 5 | 0 | 14 | 0 | NR | NR | 26 | 7 | 21 | 9 | 22 | 1 | 27 | 1 | 13 | 0 |
| 4/2 | 36 | 13 | 0 | 22 | 10 | 26 | 3 | 28 | 8 | 11 | 0 | 18 | 0 | 9 | 0 | 6 | 0 | 5 | 1 | NR | NR | 27 | 13 | 26 | 12 | 30 | 2 | 31 | 4 | 20 | 0 | |
| Miyake et al. (2015) | 2/1 | 45 | 20 | 0 | 33 | 3 | 26 | 3 | 41 | 13 | NR | NR | NR | NR | NR | NR | NR | NR | 16 | 0 | 10 | 0 | 15 | 1 | 16 | 1 | 13 | 4 | 11 | 0 | 19 | 0 |
| 4/2 | 45 | 28 | 1 | 36 | 8 | 28 | 4 | 44 | 23 | NR | NR | NR | NR | NR | NR | NR | NR | 27 | 1 | 13 | 0 | 25 | 5 | 25 | 5 | 23 | 8 | 13 | 0 | 26 | 0 | |
| Pan et al. (2015) | 2/1 | 32 | 19 | 1 | 8 | 3 | 3 | 1 | 8 | 2 | NR | NR | NR | NR | NR | NR | NR | NR | 10 | 2 | NR | NR | 15 | 2 | 16 | 1 | 16 | 1 | 9 | 1 | NR | NR |
| 4/2 | 50 | 28 | 2 | 33 | 8 | 15 | 2 | 18 | 7 | NR | NR | NR | NR | NR | NR | NR | NR | 32 | 7 | NR | NR | 42 | 5 | 25 | 4 | 43 | 5 | 23 | 1 | NR | NR | |
| El Din (2017) | 2/1 | 26 | 9 | 1 | 10 | 1 | 11 | 1 | 4 | 0 | 2 | 0 | NR | NR | Nausea and vomiting combine number | 3 | NR | NR | NR | 9 | 0 | 6 | 1 | 10 | 1 | 2 | 1 | 3 | NR | |||
| 4/2 | 30 | 12 | 4 | 15 | 1 | 11 | 3 | 13 | 3 | 3 | 2 | NR | NR | NR | NR | NR | NR | 11 | NR | NR | NR | 21 | 6 | 15 | 4 | 21 | 8 | 11 | 6 | 4 | NR | |
| Miyake et al. (2018) | 2/1 | 47 | 23 | 0 | 34 | 4 | 25 | 5 | 43 | 4 | 20 | 0 | NR | NR | NR | NR | NR | NR | 20 | 0 | NR | NR | 21 | 5 | 17 | 2 | 14 | 5 | NR | NR | 20 | 0 |
| 4/2 | 62 | 40 | 2 | 50 | 7 | 42 | 6 | 61 | 17 | 34 | 0 | NR | NR | NR | NR | NR | NR | 40 | 2 | NR | NR | 34 | 6 | 37 | 5 | 42 | 11 | NR | NR | 38 | 0 | |
| Zhang et al. (2018) | 2/1 | 24 | 9 | 0 | 11 | 2 | 6 | 1 | 8 | 2 | 8 | 2 | 5 | 0 | NR | NR | NR | NR | 7 | 1 | NR | NR | 10 | 5 | 4 | 2 | 10 | 3 | 7 | 1 | 4 | 0 |
| 4/2 | 30 | 17 | 2 | 17 | 9 | 16 | 2 | 16 | 2 | 8 | 1 | 12 | 1 | NR | NR | NR | NR | 11 | 4 | NR | NR | 15 | 3 | 12 | 4 | 17 | 7 | 11 | 4 | 6 | 1 | |
| Adverse Events | No. Studies | Dosing Schedule | No. of Patients | RR | p-Value | I2 (%) | pH-Value |
|---|---|---|---|---|---|---|---|
| (95% CI) | |||||||
| Laboratory abnormalities | |||||||
| Hypothyroidism * | 9 | 2/1 | 309 | 0.84 (0.72–0.99) | 0.04 | 0 | 0.53 |
| 4/2 | 513 | ||||||
| Leukopenia * | 8 | 2/1 | 268 | 0.79 (0.63–0.99) | 0.04 | 60 | 0.01 |
| 4/2 | 205 | ||||||
| Anemia | 7 | 2/1 | 238 | 0.86 (0.72–1.03) | 0.10 | 27 | 0.22 |
| 4/2 | 275 | ||||||
| Thrombocytopenia | 9 | 2/1 | 309 | 0.89 (0.77–1.03) | 0.11 | 62 | 0.007 |
| 4/2 | 513 | ||||||
| Liver dysfunction | 5 | 2/1 | 161 | 0.88 (0.70–1.12) | 0.31 | 0 | 0.84 |
| 4/2 | 180 | ||||||
| Gastrointestinal adverse events | |||||||
| Anorexia | 5 | 2/1 | 159 | 0.70 (0.47–1.04) | 0.08 | 38 | 0.17 |
| 4/2 | 326 | ||||||
| Nausea | 3 | 2/1 | 109 | 0.77 (0.42–1.45) | 0.41 | 38 | 0.2 |
| 4/2 | 274 | ||||||
| Vomiting | 2 | 2/1 | 79 | 0.62 (0.24–1.62) | 0.33 | 0 | 0 |
| 4/2 | 244 | ||||||
| Diarrhea * | 8 | 2/1 | 309 | 0.62 (0.44–0.89) | 0.010 | 62 | 0.007 |
| 4/2 | 513 | ||||||
| Dysgeusia * | 3 | 2/1 | 112 | 0.6 (0.39–0.92) | 0.02 | 0 | 0.68 |
| 4/2 | 275 | ||||||
| Other adverse events | |||||||
| Hand–foot syndrome * | 9 | 2/1 | 309 | 0.68 (0.58–0.81) | <0.00001 | 25 | 0.22 |
| 4/2 | 513 | ||||||
| Hypertension * | 9 | 2/1 | 309 | 0.70 (0.58–0.84) | 0.0002 | 16 | 0.30 |
| 4/2 | 513 | ||||||
| Fatigue * | 9 | 2/1 | 309 | 0.69 (0.60–0.81) | <0.00001 | 29 | 0.19 |
| 4/2 | 513 | ||||||
| Stomatitis * | 8 | 2/1 | 262 | 0.70 (0.57–0.86) | 0.0006 | 10 | 0.35 |
| 4/2 | 451 | ||||||
| Skin color change * | 4 | 2/1 | 180 | 0.70 (0.55–0.89) | 0.004 | 0 | 0.98 |
| 4/2 | 203 | ||||||
| Adverse Events | No. Studies | Dosing Schedule | No. of Patients | RR | p-Value | I2 (%) | pH-Value |
|---|---|---|---|---|---|---|---|
| (95% CI) | |||||||
| Laboratory abnormalities | |||||||
| Hypothyroidism | 9 | 2/1 | 309 | 0.46 (0.17–1.23) | 0.12 | 0 | 0.88 |
| 4/2 | 513 | ||||||
| Leukopenia * | 8 | 2/1 | 268 | 0.53 (0.32–0.87) | 0.01 | 0 | 0.52 |
| 4/2 | 305 | ||||||
| Anemia | 7 | 2/1 | 238 | 1.02 (0.55–1.90) | 0.95 | 0 | 0.90 |
| 4/2 | 275 | ||||||
| Thrombocytopenia * | 9 | 2/1 | 309 | 0.58 (0.40–0.83) | 0.003 | 0 | 0.52 |
| 4/2 | 513 | ||||||
| Liver dysfunction | 5 | 2/1 | 161 | 0.91 (0.09–9.42) | 0.94 | 35 | 0.21 |
| 4/2 | 180 | ||||||
| Gastrointestinal adverse events | |||||||
| Anorexia | 5 | 2/1 | 159 | 1.05 (0.34–3.19) | 0.93 | 0 | 0.7 |
| 4/2 | 326 | ||||||
| Nausea | 3 | 2/1 | 109 | 0.67 (0.14–1.45) | 0.41 | 38 | 0.2 |
| 4/2 | 274 | ||||||
| Vomiting | 2 | 2/1 | 79 | 1.66 (0.07–40.02) | 0.76 | N.A | |
| 4/2 | 244 | ||||||
| Diarrhea | 8 | 2/1 | 283 | 0.52 (0.19–1.41) | 0.20 | 42 | 0.10 |
| 4/2 | 483 | ||||||
| Dysgeusia | 3 | 2/1 | 112 | 1.66 (0.07.40.02) | 0.76 | N.A | |
| 4/2 | 275 | ||||||
| Other adverse events | |||||||
| Hand–foot syndrome | 9 | 2/1 | 309 | 0.55 (0.29–1.02) | 0.06 | 30 | 0.18 |
| 4/2 | 513 | ||||||
| Hypertension * | 9 | 2/1 | 309 | 0.51 (0.31–0.83) | 0.008 | 0 | 0.90 |
| 4/2 | 513 | ||||||
| Fatigue * | 9 | 2/1 | 309 | 0.43 (0.26–0.70) | 0.0007 | 0 | 0.89 |
| 4/2 | 513 | ||||||
| Stomatitis * | 8 | 2/1 | 262 | 0.32 (0.13–0.81) | 0.02 | 0 | 0.89 |
| 4/2 | 451 | ||||||
| Skin color change | 4 | 2/1 | 154 | 0.41 (0.02–9.71) | 0.58 | N.A | |
| 4/2 | 173 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, D.Y.; Kang, D.H.; Kim, J.W.; Kim, D.K.; Lee, J.Y.; Hong, C.H.; Cho, K.S. Does an Alternative Sunitinib Dosing Schedule Really Improve Survival Outcomes Over a Conventional Dosing Schedule in Patients with Metastatic Renal Cell Carcinoma? An Updated Systematic Review and Meta-Analysis. Cancers 2019, 11, 1830. https://doi.org/10.3390/cancers11121830
Chung DY, Kang DH, Kim JW, Kim DK, Lee JY, Hong CH, Cho KS. Does an Alternative Sunitinib Dosing Schedule Really Improve Survival Outcomes Over a Conventional Dosing Schedule in Patients with Metastatic Renal Cell Carcinoma? An Updated Systematic Review and Meta-Analysis. Cancers. 2019; 11(12):1830. https://doi.org/10.3390/cancers11121830
Chicago/Turabian StyleChung, Doo Yong, Dong Hyuk Kang, Jong Won Kim, Do Kyung Kim, Joo Yong Lee, Chang Hee Hong, and Kang Su Cho. 2019. "Does an Alternative Sunitinib Dosing Schedule Really Improve Survival Outcomes Over a Conventional Dosing Schedule in Patients with Metastatic Renal Cell Carcinoma? An Updated Systematic Review and Meta-Analysis" Cancers 11, no. 12: 1830. https://doi.org/10.3390/cancers11121830
APA StyleChung, D. Y., Kang, D. H., Kim, J. W., Kim, D. K., Lee, J. Y., Hong, C. H., & Cho, K. S. (2019). Does an Alternative Sunitinib Dosing Schedule Really Improve Survival Outcomes Over a Conventional Dosing Schedule in Patients with Metastatic Renal Cell Carcinoma? An Updated Systematic Review and Meta-Analysis. Cancers, 11(12), 1830. https://doi.org/10.3390/cancers11121830