

Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking


 , ,
, ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
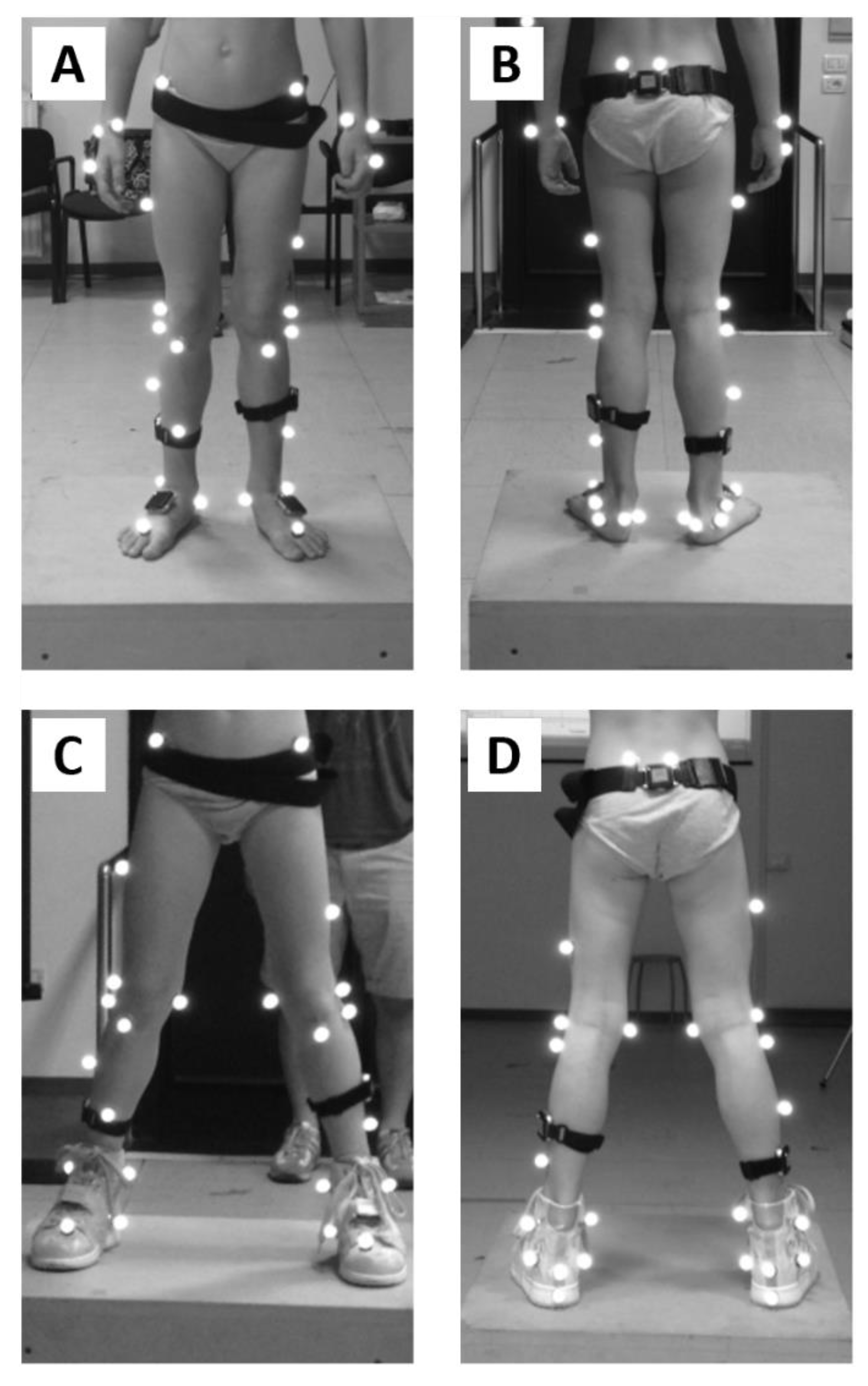
2.2. Experimental Procedure
2.3. Data Analysis
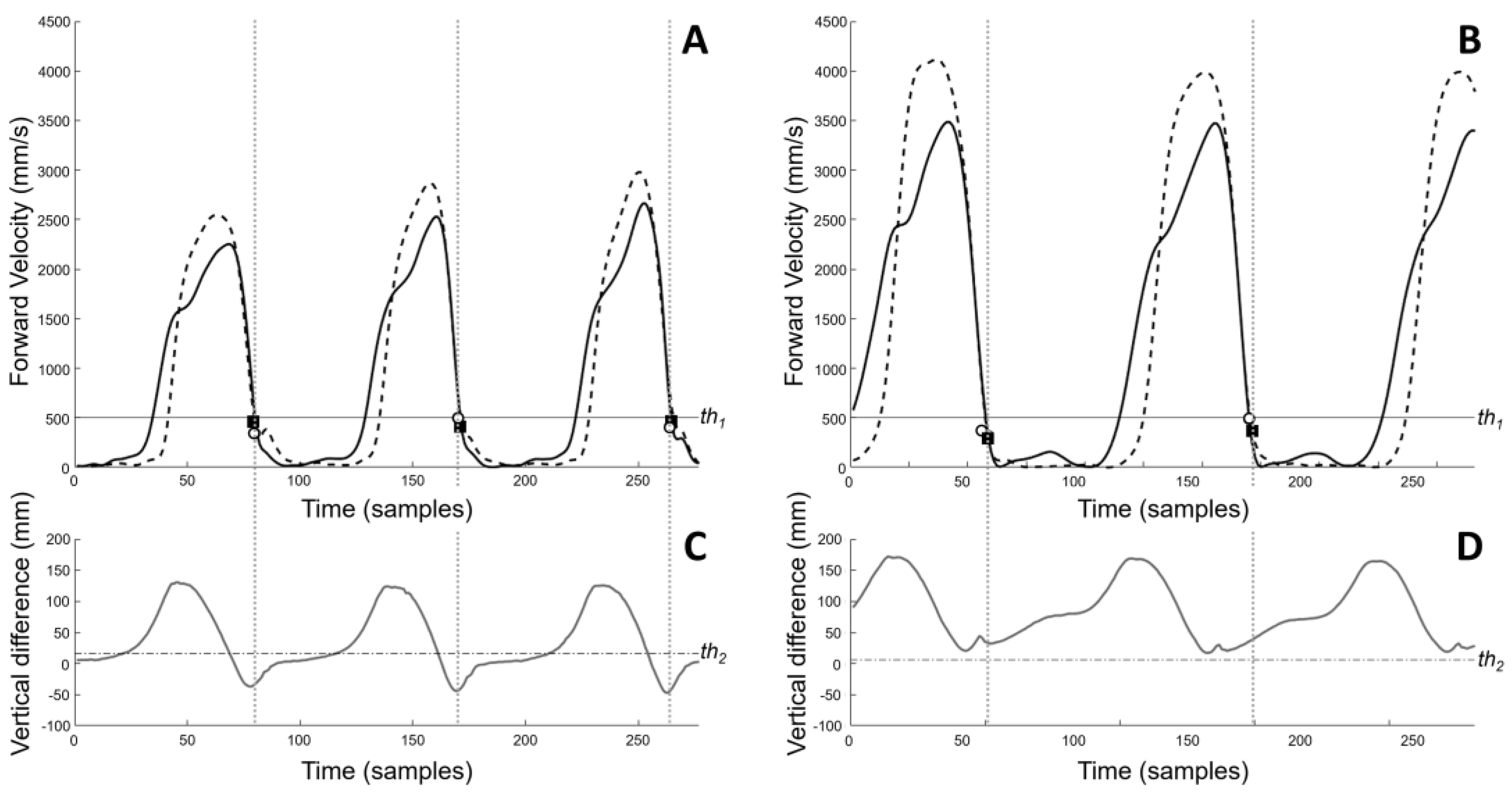
2.3.1. Lab-Based Gait Events Identification
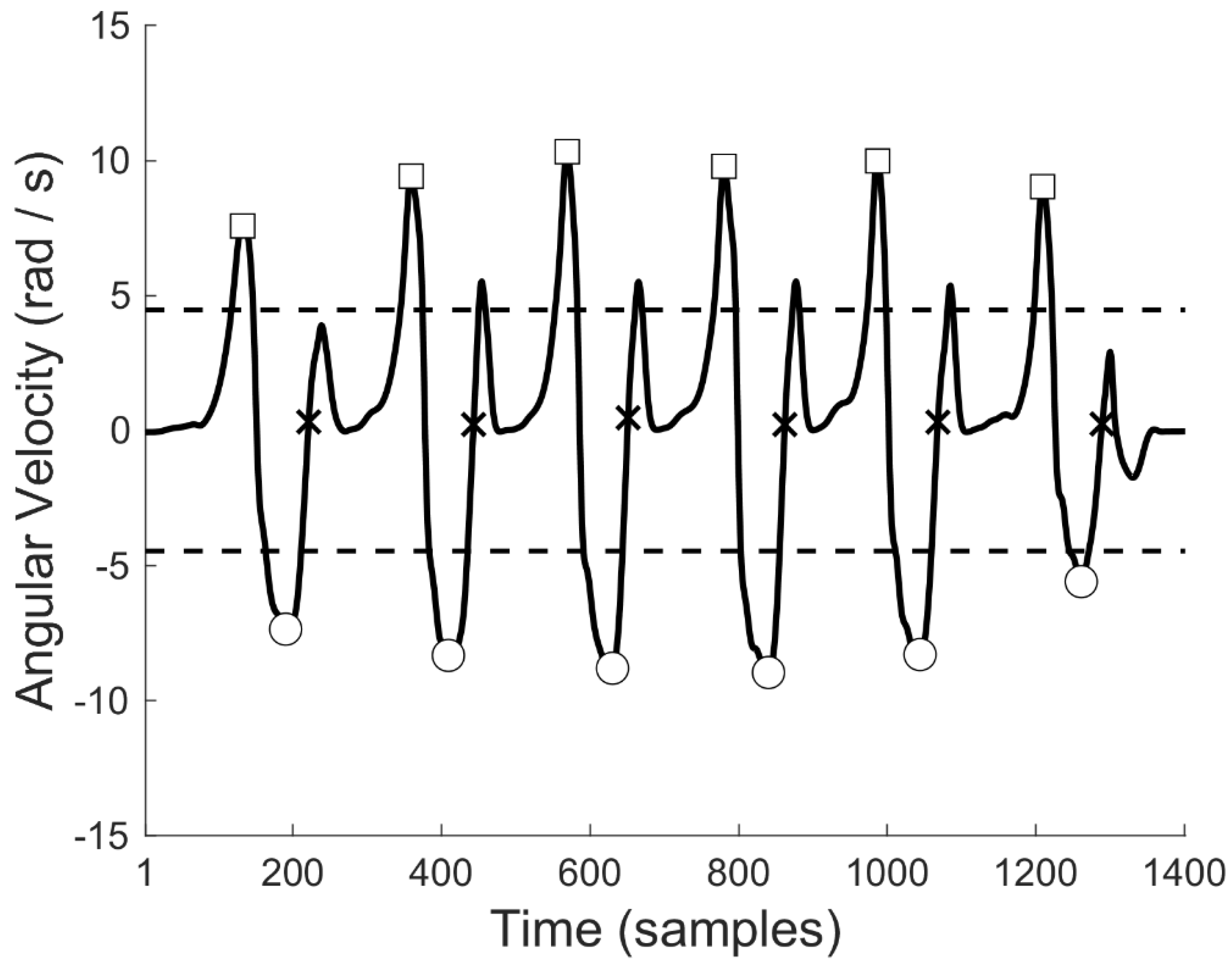
2.3.2. MIMU-Based Gait Events Identification
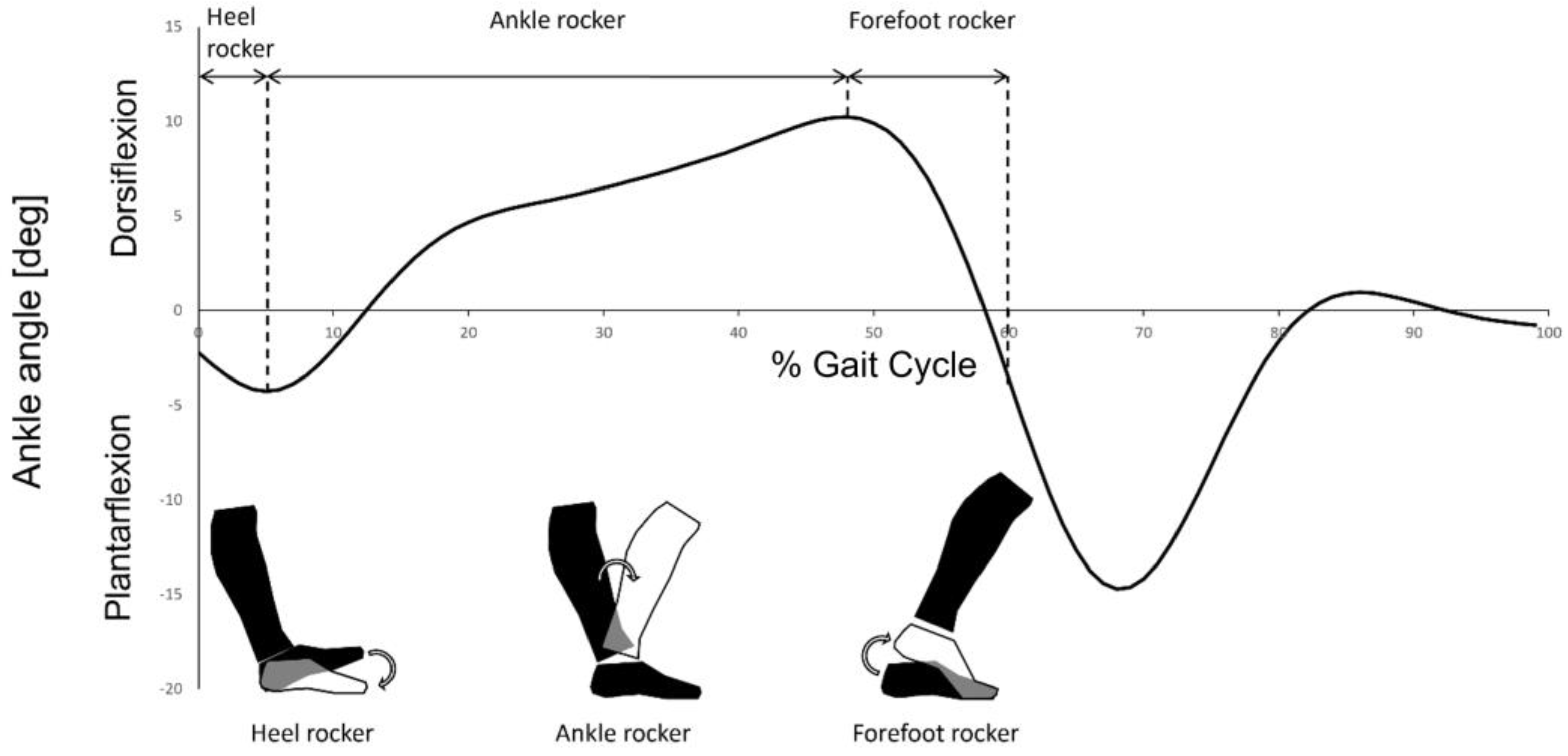
2.4. Characterization of Heel and Forefoot Rockers
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sutherland, D. The development of mature gait. Gait Posture 1997, 6, 163–170. [Google Scholar] [CrossRef]
- Engström, P.; Tedroff, K. Idiopathic toe-walking: Prevalence and natural history from birth to ten years of age. J. Bone Jt. Surg. 2018, 100, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Engström, P.; Tedroff, K. The prevalence and course of idiopathic toe-walking in 5-year-old children. Pediatrics 2012, 130, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, G.; Wagner, B. The natural history of idiopathic toe-walking: A long-term follow-up of fourteen conservatively treated children. Acta Paediatr. 2007, 93, 196–199. [Google Scholar] [CrossRef]
- Sobel, E.; Caselli, M.; Velez, Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J. Am. Podiatr. Med. Assoc. 1997, 87, 17–22. [Google Scholar] [CrossRef]
- Oetgen, M.E.; Peden, S. Idiopathic toe walking. J. Am. Acad. Orthop. Surg. 2012, 20, 292–300. [Google Scholar] [CrossRef]
- Pendharkar, G.; Percival, P.; Morgan, D.; Lai, D. Automated method to distinguish toe walking strides from normal strides in the gait of idiopathic toe walking children from heel accelerometry data. Gait Posture 2012, 35, 478–482. [Google Scholar] [CrossRef]
- Alvarez, C.; De Vera, M.; Beauchamp, R.; Ward, V.; Black, A. Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait Posture 2007, 26, 428–435. [Google Scholar] [CrossRef]
- Perry, J. Ankle foot complex. In Gait Analysis: Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992; ISBN 978-1-55642-192-1. [Google Scholar]
- Caserta, A.J.; Pacey, V.; Fahey, M.C.; Gray, K.; Engelbert, R.H.; Williams, C.M. Interventions for idiopathic toe walking. Cochrane Database Syst. Rev. 2019, 10, CD012363. [Google Scholar] [CrossRef]
- Ruzbarsky, J.J.; Scher, D.; Dodwell, E. Toe walking: Causes, epidemiology, assessment, and treatment. Curr. Opin. Pediatr. 2016, 28, 40–46. [Google Scholar] [CrossRef]
- Clark, E.; Sweeney, J.K.; Yocum, A.; McCoy, S.W. Effects of motor control intervention for children with idiopathic toe walking: A 5-case series. Pediatr. Phys. Ther. 2010, 22, 417–426. [Google Scholar] [CrossRef]
- Brasiliano, P.; Alvini, M.; Di Stanislao, E.; Vannozzi, G.; Di Rosa, G.; Camomilla, V. Effects of wearing a foot orthosis on ankle function in children with idiopathic toe walking during gait. Heliyon 2022, 8, e11021. [Google Scholar] [CrossRef]
- Herrin, K.; Geil, M. A comparison of orthoses in the treatment of idiopathic toe walking: A Randomized Controlled Trial. Prosthet. Orthot. Int. 2015, 40, 262–269. [Google Scholar] [CrossRef]
- Michalitsis, J.; Murphy, A.T.; Rawicki, B.; Haines, T.P.; Williams, C. Full length foot orthoses have an immediate treatment effect and modify gait of children with idiopathic toe walking. Gait Posture 2019, 68, 227–231. [Google Scholar] [CrossRef]
- Contini, B.G.; Bergamini, E.; Alvini, M.; Di Stanislao, E.; Di Rosa, G.; Castelli, E.; Vannozzi, G.; Camomilla, V. A wearable gait analysis protocol to support the choice of the appropriate ankle-foot orthosis: A comparative assessment in children with Cerebral Palsy. Clin. Biomech. 2019, 70, 177–185. [Google Scholar] [CrossRef]
- Pomarino, D.; Llamas, J.R.; Martin, S.; Pomarino, A. Literature review of idiopathic toe walking: Etiology, prevalence, classification, and treatment. Foot Ankle Speéc. 2017, 10, 337–342. [Google Scholar] [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.-Z. Toward pervasive gait analysis with wearable sensors: A systematic review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Celik, Y.; Stuart, S.; Woo, W.; Godfrey, A. Gait analysis in neurological populations: Progression in the use of wearables. Med. Eng. Phys. 2021, 87, 9–29. [Google Scholar] [CrossRef]
- Caruso, M.; Sabatini, A.; Laidig, D.; Seel, T.; Knaflitz, M.; Della Croce, U.; Cereatti, A. Analysis of the accuracy of ten algorithms for orientation estimation using inertial and magnetic sensing under optimal conditions: One size does not fit all. Sensors 2021, 21, 2543. [Google Scholar] [CrossRef]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- Weygers, I.; Kok, M.; Konings, M.; Hallez, H.; De Vroey, H.; Claeys, K. Inertial sensor-based lower limb joint kinematics: A methodological systematic review. Sensors 2020, 20, 673. [Google Scholar] [CrossRef] [PubMed]
- Brasiliano, P.; Alvini, M.; Di Stanislao, E.; Vannozzi, G.; Camomilla, V. Ankle kinematics of children with idiopathic toe walking using single-segment and multi-segment foot models. In Proceedings of the 16th International Symposium on 3D-Ananlysis of Human Movement, Virtual Conference, 25 May 2021. [Google Scholar]
- Mascia, G.; Brasiliano, P.; Di Feo, P.; Cereatti, A.; Camomilla, V. A functional calibration protocol for ankle plantar-dorsiflexion estimate using magnetic and inertial measurement units: Repeatability and reliability assessment. J. Biomech. 2022, 141, 111202. [Google Scholar] [CrossRef] [PubMed]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Caravaggi, P.; Theologis, T.; Stebbins, J. Multi-segment foot models and their use in clinical populations. Gait Posture 2019, 69, 50–59. [Google Scholar] [CrossRef]
- Prasanth, H.; Caban, M.; Keller, U.; Courtine, G.; Ijspeert, A.; Vallery, H.; von Zitzewitz, J. Wearable sensor-based real-time gait detection: A systematic review. Sensors 2021, 21, 2727. [Google Scholar] [CrossRef]
- Ghassemi, N.H.; Hannink, J.; Martindale, C.F.; Gaßner, H.; Müller, M.; Klucken, J.; Eskofier, B.M. Segmentation of Gait Sequences in Sensor-Based Movement Analysis: A Comparison of Methods in Parkinson’s Disease. Sensors 2018, 18, 145. [Google Scholar] [CrossRef]
- Pacini Panebianco, G.; Bisi, M.C.; Stagni, R.; Fantozzi, S. Analysis of the performance of 17 algorithms from a systematic review: Influence of sensor position, analysed variable and computational approach in gait timing estimation from IMU measurements. Gait Posture 2018, 66, 76–82. [Google Scholar] [CrossRef]
- Taborri, J.; Scalona, E.; Palermo, E.; Rossi, S.; Cappa, P. Validation of inter-subject training for hidden Markov models applied to gait phase detection in children with Cerebral Palsy. Sensors 2015, 15, 24514–24529. [Google Scholar] [CrossRef]
- Behboodi, A.; Zahradka, N.; Wright, H.; Alesi, J.; Lee, S.C.K. Real-time detection of seven phases of gait in children with Cerebral Palsy using two gyroscopes. Sensors 2019, 19, 2517. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Hughes, G.T.; Camomilla, V.; Vanwanseele, B.; Harrison, A.J.; Fong, D.T.; Bradshaw, E.J. Novel technology in sports biomechanics: Some words of caution. Sports Biomech. 2021, 1–9. [Google Scholar] [CrossRef]
- Wu, J.; Kuruvithadam, K.; Schaer, A.; Stoneham, R.; Chatzipirpiridis, G.; Easthope, C.; Barry, G.; Martin, J.; Pané, S.; Nelson, B.; et al. An intelligent in-shoe system for gait monitoring and analysis with optimized sampling and real-time visualization capabilities. Sensors 2021, 21, 2869. [Google Scholar] [CrossRef]
- Ghoussayni, S.; Stevens, C.; Durham, S.; Ewins, D. Assessment and validation of a simple automated method for the detection of gait events and intervals. Gait Posture 2004, 20, 266–272. [Google Scholar] [CrossRef]
- Visscher, R.M.; Sansgiri, S.; Freslier, M.; Harlaar, J.; Brunner, R.; Taylor, W.R.; Singh, N.B. Towards validation and standardization of automatic gait event identification algorithms for use in paediatric pathological populations. Gait Posture 2021, 86, 64–69. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Thorpe, S.K.; O’Malley, M.J.; Vaughan, C.L. Automatic detection of gait events using kinematic data. Gait Posture 2007, 25, 469–474. [Google Scholar] [CrossRef]
- Trojaniello, D.; Cereatti, A.; Pelosin, E.; Avanzino, L.; Mirelman, A.; Hausdorff, J.M.; Della Croce, U. Estimation of step-by-step spatio-temporal parameters of normal and impaired gait using shank-mounted magneto-inertial sensors: Application to elderly, hemiparetic, parkinsonian and choreic gait. J. Neuroeng. Rehabil. 2014, 11, 152. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.; Dehollain, C.; Blanc, Y.; Burkhard, P.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef]
- Hsu, Y.-L.; Chung, P.-C.J.; Wang, W.-H.; Pai, M.-C.; Wang, C.-Y.; Lin, C.-W.; Wu, H.-L.; Wang, J.-S. Gait and balance analysis for patients with Alzheimer’s disease using an inertial-sensor-based wearable instrument. IEEE J. Biomed. Health Inform. 2014, 18, 1822–1830. [Google Scholar] [CrossRef]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors 2014, 14, 18625–18649. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brasiliano, P.; Mascia, G.; Di Feo, P.; Di Stanislao, E.; Alvini, M.; Vannozzi, G.; Camomilla, V. Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking. Micromachines 2023, 14, 277. https://doi.org/10.3390/mi14020277
Brasiliano P, Mascia G, Di Feo P, Di Stanislao E, Alvini M, Vannozzi G, Camomilla V. Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking. Micromachines. 2023; 14(2):277. https://doi.org/10.3390/mi14020277
Chicago/Turabian StyleBrasiliano, Paolo, Guido Mascia, Paolo Di Feo, Eugenio Di Stanislao, Martina Alvini, Giuseppe Vannozzi, and Valentina Camomilla. 2023. "Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking" Micromachines 14, no. 2: 277. https://doi.org/10.3390/mi14020277
APA StyleBrasiliano, P., Mascia, G., Di Feo, P., Di Stanislao, E., Alvini, M., Vannozzi, G., & Camomilla, V. (2023). Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking. Micromachines, 14(2), 277. https://doi.org/10.3390/mi14020277