The Prescription of Drugs That Inhibit Organic Anion Transporters 1 or 3 Is Associated with the Plasma Accumulation of Uremic Toxins in Kidney Transplant Recipients


 ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
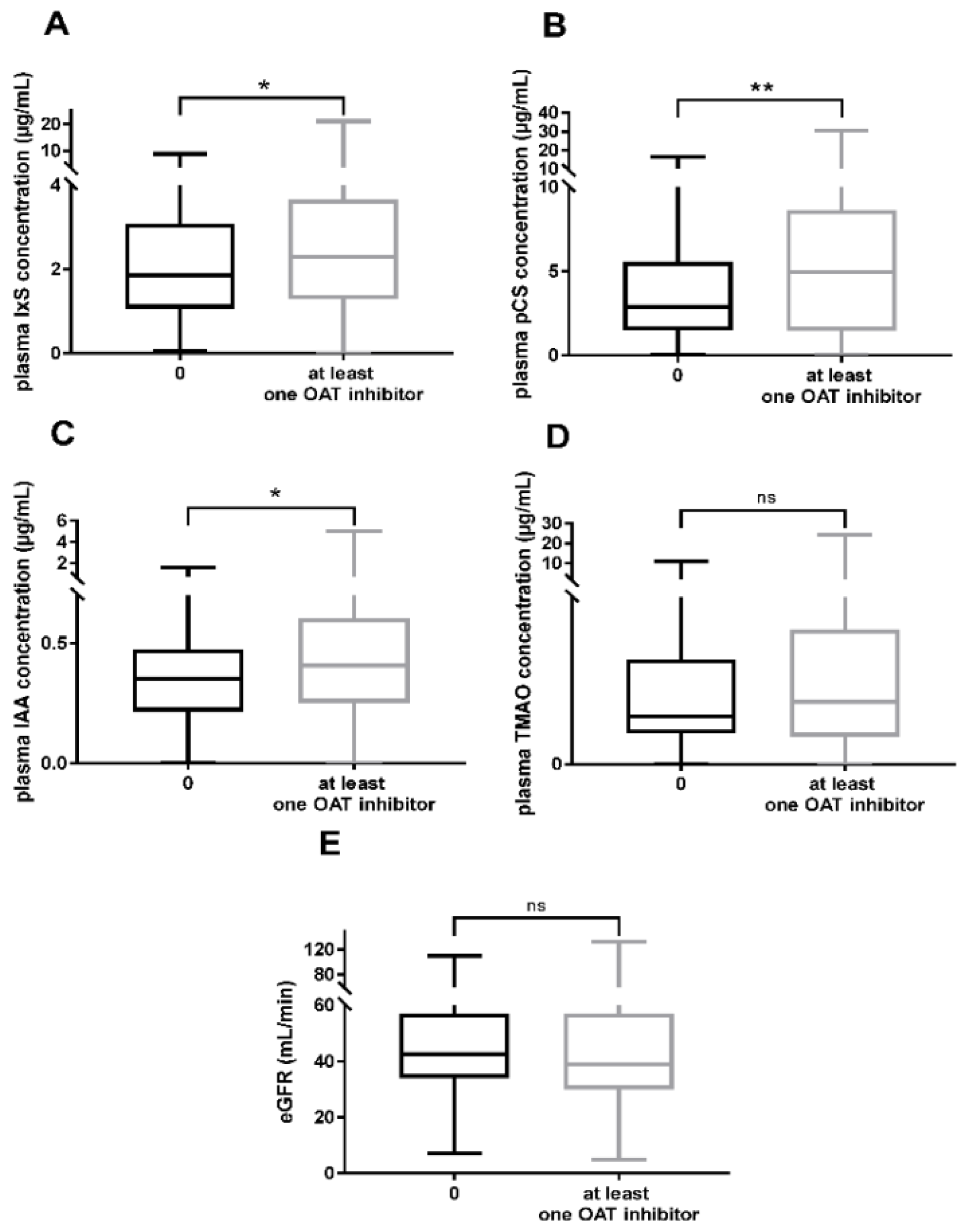
2.2. Plasma Accumulation of UTs in Patients Taking OAT1/OAT3 Inhibitors
2.3. Factors Associated with the Plasma Accumulation of UTs
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design and Participants
5.2. Study Endpoints
5.3. Collected Data
5.4. Identification of Drugs That Inhibit OAT1/OAT3
5.5. Uremic Toxin Assays
5.6. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vanholder, R.; de Smet, R.; Glorieux, G.; Argilés, A.; Baurmeister, U.; Brunet, P.; Clark, W.; Cohen, G.; de Deyn, P.P.; Deppisch, R.; et al. Review on Uremic Toxins: Classification, Concentration, and Interindividual Variability. Kidney Int. 2003, 63, 1934–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanholder, R.; Pletinck, A.; Schepers, E.; Glorieux, G. Biochemical and Clinical Impact of Organic Uremic Retention Solutes: A Comprehensive Update. Toxins 2018, 10, 33. [Google Scholar] [CrossRef] [Green Version]
- Hénaut, L.; Chillon, J.M.; Kamel, S.; Massy, Z.A. Updates on the Mechanisms and the Care of Cardiovascular Calcification in Chronic Kidney Disease. Semin. Nephrol. 2018, 38, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Six, I.; Flissi, N.; Lenglet, G.; Louvet, L.; Kamel, S.; Gallet, M.; Massy, Z.A.; Liabeuf, S. Uremic Toxins and Vascular Dysfunction. Toxins 2020, 12, 404. [Google Scholar] [CrossRef]
- Assem, M.; Lando, M.; Grissi, M.; Kamel, S.; Massy, Z.A.; Chillon, J.M.; Hénaut, L. The Impact of Uremic Toxins on Cerebrovascular and Cognitive Disorders. Toxins 2018, 10, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, H.; Goto, S.; Fukagawa, M. Role of Uremic Toxins for Kidney, Cardiovascular, and Bone Dysfunction. Toxins 2018, 10, 202. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.; Boenink, R.; Noordzij, M.; Bosdriesz, J.R.; Stel, V.S.; Beltrán, P.; Ruiz, J.C.; Seyahi, N.; Farnés, J.C.; Stendahl, M.; et al. The ERA-EDTA Registry Annual Report 2017: A Summary. Clin. Kidney J. 2020, 13, 693–709. [Google Scholar] [CrossRef]
- Huang, S.T.; Shu, K.H.; Cheng, C.H.; Wu, M.J.; Yu, T.M.; Chuang, Y.W.; Chen, C.H. Serum Total P-Cresol and Indoxyl Sulfate Correlated with Stage of Chronic Kidney Disease in Renal Transplant Recipients. Transplant. Proc. 2012, 44, 621–624. [Google Scholar] [CrossRef]
- Marienne, J.; Laville, S.M.; Caillard, P.; Batteux, B.; Gras-Champel, V.; Masmoudi, K.; Choukroun, G.; Liabeuf, S. Evaluation of Changes Over Time in the Drug Burden and Medication Regimen Complexity in ESRD Patients Before and After Renal Transplantation. Kidney Int. Rep. 2021, 6, 128–137. [Google Scholar] [CrossRef]
- Laville, S.M.; Gras-Champel, V.; Moragny, J.; Metzger, M.; Jacquelinet, C.; Combe, C.; Fouque, D.; Laville, M.; Frimat, L.; Robinson, B.M.; et al. Adverse Drug Reactions in Patients with CKD. Clin. J. Am. Soc. Nephrol. 2020, 15, 1090–1102. [Google Scholar] [CrossRef]
- Nigam, S.K.; Bush, K.T.; Martovetsky, G.; Ahn, S.Y.; Liu, H.C.; Richard, E.; Bhatnagar, V.; Wu, W. The Organic Anion Transporter (OAT) Family: A Systems Biology Perspective. Physiol. Rev. 2015, 95, 83–123. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Bush, K.T.; Nigam, S.K. Key Role for the Organic Anion Transporters, OAT1 and OAT3, in the in Vivo Handling of Uremic Toxins and Solutes. Sci. Rep. 2017, 7, 4939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, S.S.; Yu, C.P.; Hsieh, Y.W.; Chao, P.D.L.; Sweet, D.H.; Hou, Y.C.; Lin, S.P. Effects of Antibiotics on the Pharmacokinetics of Indoxyl Sulfate, a Nephro-Cardiovascular Toxin. Xenobiotica 2020, 50, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Y.; Wang, Z.; Jia, X.; Yan, D.; Shih, D.M.; Hazen, S.L.; Lusis, A.J.; Tang, W.H.W. Loop Diuretics Inhibit Renal Excretion of Trimethylamine N-Oxide. JACC Basic Transl. Sci. 2021, 6, 103–115. [Google Scholar] [CrossRef]
- Liabeuf, S.; Barreto, D.V.; Barreto, F.C.; Meert, N.; Glorieux, G.; Schepers, E.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A. Free P-Cresylsulphate Is a Predictor of Mortality in Patients at Different Stages of Chronic Kidney Disease. Nephrol. Dial. Transplant. 2010, 25, 1183–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.J.; Wu, V.; Wu, P.C.; Wu, C.J. Meta-Analysis of the Associations of p-Cresyl Sulfate (PCS) and Indoxyl Sulfate (IS) with Cardiovascular Events and All-Cause Mortality in Patients with Chronic Renal Failure. PLoS ONE 2015, 10, e0132589. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Zhu, J.; Zhu, Z.; Ni, J.; Du, R.; Dai, Y.; Chen, Y.; Wu, Z.; Lu, L.; Zhang, R. P-Cresyl Sulfate Aggravates Cardiac Dysfunction Associated with Chronic Kidney Disease by Enhancing Apoptosis of Cardiomyocytes. J. Am. Heart Assoc. 2015, 4, e001852. [Google Scholar] [CrossRef] [Green Version]
- Jing, Y.J.; Ni, J.W.; Ding, F.H.; Fang, Y.H.; Wang, X.Q.; Wang, H.B.; Chen, X.N.; Chen, N.; Zhan, W.W.; Lu, L.; et al. P-Cresyl Sulfate Is Associated with Carotid Arteriosclerosis in Hemodialysis Patients and Promotes Atherogenesis in ApoE-/- Mice. Kidney Int. 2016, 89, 439–449. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Zou, J.Z.; Chen, J.; Tan, X.; Xiang, F.F.; Shen, B.; Hu, J.C.; Wang, J.L.; Wang, Y.Q.; Yu, J.B.; et al. Association of Trimethylamine N-Oxide with Cardiovascular and All-Cause Mortality in Hemodialysis Patients. Ren. Fail. 2020, 42, 1004–1014. [Google Scholar] [CrossRef]
- Narumi, K.; Sato, Y.; Kobayashi, M.; Furugen, A.; Kasashi, K.; Yamada, T.; Teshima, T.; Iseki, K. Effects of Proton Pump Inhibitors and Famotidine on Elimination of Plasma Methotrexate: Evaluation of Drug-Drug Interactions Mediated by Organic Anion Transporter 3. Biopharm. Drug Dispos. 2017, 38, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Ikemura, K.; Hamada, Y.; Kaya, C.; Enokiya, T.; Muraki, Y.; Nakahara, H.; Fujimoto, H.; Kobayashi, T.; Iwamoto, T.; Okuda, M. Lansoprazole Exacerbates Pemetrexed-Mediated Hematologic Toxicity by Competitive Inhibition of Renal Basolateral Human Organic Anion Transporter 3. Drug Metab. Dispos. 2016, 44, 1543–1549. [Google Scholar] [CrossRef] [Green Version]
- Ni, Y.; Duan, Z.; Zhou, D.; Liu, S.; Wan, H.; Gui, C.; Zhang, H. Identification of Structural Features for the Inhibition of OAT3-Mediated Uptake of Enalaprilat by Selected Drugs and Flavonoids. Front. Pharmacol. 2020, 11, 633. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.P.; Sweet, D.H.; Peng, Y.H.; Hsieh, Y.W.; Chao, P.D.L.; Hou, Y.C.; Lin, S.P. Effects of Nonsteroidal Anti-Inflammatory Drugs on the Renal Excretion of Indoxyl Sulfate, a Nephro-Cardiovascular Toxin, in Rats. Eur. J. Pharm. Sci. 2017, 101, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuki, S.; Asaba, H.; Takanaga, H.; Deguchi, T.; Hosoya, K.I.; Otagiri, M.; Terasaki, T. Role of Blood-Brain Barrier Organic Anion Transporter 3 (OAT3) in the Efflux of Indoxyl Sulfate, a Uremic Toxin: Its Involvement in Neurotransmitter Metabolite Clearance from the Brain. J. Neurochem. 2002, 83, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.J.; Sidor, N.A.; Tonial, N.C.; Che, A.; Urquhart, B.L. Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets. Toxins 2021, 13, 142. [Google Scholar] [CrossRef]
- Sirich, T.L.; Plummer, N.S.; Gardner, C.D.; Hostetter, T.H.; Meyer, T.W. Effect of Increasing Dietary Fiber on Plasma Levels of Colon-Derived Solutes in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1603–1610. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.; Johnson, D.W.; Xu, H.; Carrero, J.J.; Pascoe, E.; French, C.; Campbell, K.L. Dietary Protein-Fiber Ratio Associates with Circulating Levels of Indoxyl Sulfate and p-Cresyl Sulfate in Chronic Kidney Disease Patients. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Li, F.X.; Wang, M.H.; Wang, J.P.; Li, R.S.; Zhang, Y.Q. Alterations to the Gut Microbiota and Their Correlation with Inflammatory Factors in Chronic Kidney Disease. Front. Cell. Infect. Microbiol. 2019, 9, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gryp, T.; De Paepe, K.; Vanholder, R.; Kerckhof, F.M.; Van Biesen, W.; Van de Wiele, T.; Verbeke, F.; Speeckaert, M.; Joossens, M.; Couttenye, M.M.; et al. Gut Microbiota Generation of Protein-Bound Uremic Toxins and Related Metabolites Is Not Altered at Different Stages of Chronic Kidney Disease. Kidney Int. 2020, 97, 1230–1242. [Google Scholar] [CrossRef] [Green Version]
- Vanholder, R.; Van Landschoot, N.; De Smet, R.; Schoots, A.; Ringoir, S. Drug Protein Binding in Chronic Renal Failure: Evaluation of Nine Drugs. Kidney Int. 1988, 33, 996–1004. [Google Scholar] [CrossRef] [Green Version]
- André, C.; Choukroun, G.; Bennis, Y.; Kamel, S.; Lemaire-Hurtel, A.S.; Masmoudi, K.; Bodeau, S.; Liabeuf, S. Potential Interactions between Uraemic Toxins and Drugs: An Application in Kidney Transplant Recipients Treated with Calcineurin Inhibitors. Nephrol. Dial. Transplant. 2021, gfab114. [Google Scholar] [CrossRef]
- Florens, N.; Yi, D.; Juillard, L.; Soulage, C.O. Using Binding Competitors of Albumin to Promote the Removal of Protein-Bound Uremic Toxins in Hemodialysis: Hope or Pipe Dream? Biochimie 2018, 144, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, V.; Thijssen, S.; Tao, X.; Fuertinger, D.H.; Kappel, F.; Kotanko, P. In Silico Comparison of Protein-Bound Uremic Toxin Removal by Hemodialysis, Hemodiafiltration, Membrane Adsorption, and Binding Competition. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Neafsey, P.; Ginsberg, G.; Hattis, D.; Johns, D.O.; Guyton, K.Z.; Sonawane, B. Genetic Polymorphism in CYP2E1: Population Distribution of CYP2E1 Activity. J. Toxicol. Environ. Health Part B Crit. Rev. 2009, 12, 362–388. [Google Scholar] [CrossRef]
- Masereeuw, R.; Mutsaers, H.A.M.; Toyohara, T.; Abe, T.; Jhawar, S.; Sweet, D.H.; Lowenstein, J. The Kidney and Uremic Toxin Removal: Glomerulus or Tubule? Semin. Nephrol. 2014, 34, 191–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takada, T.; Yamamoto, T.; Matsuo, H.; Tan, J.K.; Ooyama, K.; Sakiyama, M.; Miyata, H.; Yamanashi, Y.; Toyoda, Y.; Higashino, T.; et al. Identification of ABCG2 as an Exporter of Uremic Toxin Indoxyl Sulfate in Mice and as a Crucial Factor Influencing CKD Progression. Sci. Rep. 2018, 8, 11147. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Stevens, P.E.; Levin, A. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Morrissey, K.M.; Wen, C.C.; Johns, S.J.; Zhang, L.; Huang, S.M.; Giacomini, K.M. The UCSF-FDA Transportal: A Public Drug Transporter Database. Clin. Pharmacol. Ther. 2012, 92, 545–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holazox, A.A.; Colburn, W.A.; Gustafson, J.H.; Young, R.L.; Parsonnet, M. Pharmacokinetics of Bumetanide Following Intravenous, Intramuscular, and Oral Administrations to Normal Subjects. J. Pharm. Sci. 1984, 73, 1108–1113. [Google Scholar] [CrossRef]
- Davies, D.L.; Lant, A.F.; Millard, N.R.; Smith, A.J.; Ward, J.W.; Wilson, G.M. Renal Action, Therapeutic Use, and Pharmacokinetics of the Diuretic Bumetanide. Clin. Pharmacol. Ther. 1974, 15, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Iwersen-Bergmann, S.; Andresen, H.; Schmoldt, A. Therapeutic and Toxic Blood Concentrations of Nearly 1000 Drugs and Other Xenobiotics. Crit. Care 2012, 16, R136. [Google Scholar] [CrossRef] [Green Version]
- Niemi, M.; Schaeffeler, E.; Lang, T.; Fromm, M.F.; Neuvonen, M.; Kyrklund, C.; Backman, J.T.; Kerb, R.; Schwab, M.; Neuvonen, P.J.; et al. High Plasma Pravastatin Concentrations Are Associated with Single Nucleotide Polymorphisms and Haplotypes of Organic Anion Transporting Polypeptide-C (OATP-C, SLCO1B1). Pharmacogenetics 2004, 14, 429–440. [Google Scholar] [CrossRef]
- Caruso, F.S.; Szabadi, R.R.; Vukovich, R.A. Pharmacokinetics and Clinical Pharmacology of Indapamide. Am. Heart J. 1983, 106, 212–220. [Google Scholar] [CrossRef]
- Wang, C.; Wang, C.; Liu, Q.; Meng, Q.; Cang, J.; Sun, H.; Peng, J.; Ma, X.; Huo, X.; Liu, K. Aspirin and Probenecid Inhibit Organic Anion Transporter 3–Mediated Renal Uptake of Cilostazol and Probenecid Induces Metabolism of Cilostazol in the Rat. Drug Metab. Dispos. 2014, 42, 996–1007. [Google Scholar] [CrossRef] [Green Version]
- Benedek, I.H.; Joshi, A.S.; Pieniaszek, H.J.; King, S.-Y.P.; Kornhauser, D.M. Variability in the Pharmacokinetics and Pharmacodynamics of Low Dose Aspirin in Healthy Male Volunteers. J. Clin. Pharmacol. 1995, 35, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Hasannejad, H.; Takeda, M.; Taki, K.; Shin, H.J.; Babu, E.; Jutabha, P.; Khamdang, S.; Aleboyeh, M.; Onozato, M.L.; Tojo, A.; et al. Interactions of Human Organic Anion Transporters with Diuretics. J. Pharmacol. Exp. Ther. 2004, 308, 1021–1029. [Google Scholar] [CrossRef]
- Khamdang, S.; Takeda, M.; Noshiro, R.; Narikawa, S.; Enomoto, A.; Anzai, N.; Piyachaturawat, P.; Endou, H. Interactions of Human Organic Anion Transporters and Human Organic Cation Transporters with Nonsteroidal Anti-Inflammatory Drugs. J. Pharmacol. Exp. Ther. 2002, 303, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Hassan-Alin, M.; Andersonn, T.; Bredberg, E.; Röhss, K. Pharmacokinetics of Esomeprazole after Oral and Intravenous Administration of Single and Repeated Doses to Healthy Subjects. Eur. J. Clin. Pharmacol. 2000, 56, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Chu, X.-Y.; Bleasby, K.; Yabut, J.; Cai, X.; Chan, G.H.; Hafey, M.J.; Xu, S.; Bergman, A.J.; Braun, M.P.; Dean, D.C.; et al. Transport of the Dipeptidyl Peptidase-4 Inhibitor Sitagliptin by Human Organic Anion Transporter 3, Organic Anion Transporting Polypeptide 4C1, and Multidrug Resistance P-Glycoprotein. J. Pharmacol. Exp. Ther. 2007, 321, 673–683. [Google Scholar] [CrossRef] [Green Version]
- Takeda, M.; Noshiro, R.; Onozato, M.L.; Tojo, A.; Hasannejad, H.; Huang, X.-L.; Narikawa, S.; Endou, H. Evidence for a Role of Human Organic Anion Transporters in the Muscular Side Effects of HMG-CoA Reductase Inhibitors. Eur. J. Pharmacol. 2004, 483, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Nakagomi-Hagihara, R.; Nakai, D.; Tokui, T. Inhibition of Human Organic Anion Transporter 3 Mediated Pravastatin Transport by Gemfibrozil and the Metabolites in Humans. Xenobiotica 2007, 37, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Chioukh, R.; Noel-Hudson, M.-S.; Ribes, S.; Fournier, N.; Becquemont, L.; Verstuyft, C. Proton Pump Inhibitors Inhibit Methotrexate Transport by Renal Basolateral Organic Anion Transporter HOAT3. Drug Metab. Dispos. 2014, 42, 2041–2048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karol, M.D.; Machinist, J.M.; Cavanaugh, J.M. Lansoprazole Pharmacokinetics in Subjects with Various Degrees of Kidney Function. Clin. Pharmacol. Ther. 1997, 61, 450–458. [Google Scholar] [CrossRef]
- Regenthal, R.; Krueger, M.; Koeppel, C.; Preiss, R. Drug levels: Therapeutic and toxic serum/plasma concentrations of common drugs. J. Clin. Monit. Comput. 1999, 15, 529–544. [Google Scholar] [CrossRef]
- Sato, M.; Iwanaga, T.; Mamada, H.; Ogihara, T.; Yabuuchi, H.; Maeda, T.; Tamai, I. Involvement of Uric Acid Transporters in Alteration of Serum Uric Acid Level by Angiotensin II Receptor Blockers. Pharm. Res. 2008, 25, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Stangier, J.; Su, C.; Roth, W. Pharmacokinetics of Orally and Intravenously Administered Telmisartan in Healthy Young and Elderly Volunteers and in Hypertensive Patients. J. Int. Med. Res. 2000, 28, 149–167. [Google Scholar] [CrossRef]
- André, C.; Bennis, Y.; Titeca-Beauport, D.; Caillard, P.; Cluet, Y.; Kamel, S.; Choukroun, G.; Maizel, J.; Liabeuf, S.; Bodeau, S. Two Rapid, Accurate Liquid Chromatography Tandem Mass Spectrometry Methods for the Quantification of Seven Uremic Toxins: An Application for Describing Their Accumulation Kinetic Profile in a Context of Acute Kidney Injury. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2020, 1152, 122234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Patients (n = 403) | Patients Not Prescribed OAT1/OAT3 Inhibitors (n = 92) | Patients Prescribed at Least One OAT1/OAT3 Inhibitor (n = 311) | p-Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years) | 56 (48–66) | 52 (43–61) | 58 (49–670) | 0.002 |
| Males | 250 (62.0) | 59 (64.1) | 191 (61.4) | 0.727 |
| BMI (kg/m2) | 26.5 (23.4–29.7) | 24.6 (22.5–28.4) | 26.9 (23.9–30.4) | <0.001 |
| Clinical characteristics | ||||
| Time since transplantation (months) | 78.0 (40.0–158.5) | 76.0 (39.8–218.3) | 78.0 (40.0–146.5) | 0.281 |
| CKD stage | ||||
| 1 | 13 (3.2) | 1 (1.1) | 12 (3.9) | |
| 2 | 68 (16.9) | 17 (18.5) | 51 (16.4) | |
| 3A + 3B | 228 (56.5) | 57 (62.0) | 171 (55.0) | 0.393 |
| 4 | 84 (20.8) | 16 (17.4) | 68 (21.9) | |
| 5 | 10 (2.5) | 1 (1.1) | 9 (2.9) | |
| Cause of CKD, n (%) | ||||
| Diabetes | 20 (4.9) | 0 (0) | 20 (6.4) | |
| Vascular disease | 26 (6.5) | 1 (1.1) | 25 (8.0) | |
| Chronic glomerulonephritis | 38 (9.4) | 12 (13.0) | 26 (8.4) | |
| Polycystic kidney disease | 62 (15.4) | 15 (16.3) | 47 (15.1) | 0.043 |
| Interstitial nephritis | 5 (1.2) | 1 (1.1) | 4 (1.3) | |
| Autoimmune disorder | 72 (17.9) | 17 (18.5) | 55 (17.7) | |
| Genetic disorder | 45 (11.2) | 15 (16.3) | 30 (9.6) | |
| Other causes | 135 (33.5) | 31 (33.7) | 104 (33.4) | |
| SBP (mmHg) | 142 (132–158) | 142 (130–156) | 142 (132–158) | 0.700 |
| DBP (mmHg) | 80 (72–87) | 81 (74–90) | 80 (72–86) | 0.111 |
| PP (mmHg) | 64 (54–75) | 62 (50–71) | 64 (54–75) | 0.156 |
| Hypertension | 392 (97.3) | 90 (97.8) | 301 (96.8) | 1.000 |
| Liver disease | 1 (0.3) | 0 (0) | 1 (0.3) | 1.000 |
| Characteristics of calcineurin inhibitors | ||||
| Cyclosporine | 155 (38.46) | 38 (41.30) | 117 (37.62) | 0.524 |
| Tacrolimus | 248 (61.54) | 54 (58.70) | 194 (62.38) | |
| Laboratory data | ||||
| eGFR (MDRD) (mL/min/1.73 m2) | 41 (30–57) | 42.5 (34–57) | 39 (30–57) | 0.128 |
| Creatinine (µmol/L) | 146 (116–187) | 142 (116–177) | 148 (116–192) | 0.387 |
| Calcium (mmol/L) | 2.41 (2.32–2.49) | 2.41 (2.33–2.50) | 2.41 (2.32–2.49) | 0.769 |
| Phosphate (mmol/L) | 1.05 (0.91–1.20) | 1.03 (0.89–1.13) | 1.05 (0.91–1.23) | 0.084 |
| Uric acid (µmol/L) | 471 (390–565) | 483 (399–540) | 458 (388–573) | 0.906 |
| CRP (mg/L) | 3.70 (0.60–9.00) | 1.80 (0.30–4.20) | 4.50 (0.90–11.20) | 0.007 |
| Protein (g/L) | 67 (64–70) | 67 (63–69) | 67 (64–70) | 0.984 |
| Albumin (g/L) | 38.9 (36.7–41.1) | 39.8 (38.0–41.7) | 38.8 (36.5–40.9) | 0.010 |
| Glucose (mmol/L) | 5.4 (4.8–6.3) | 5.1 (4.6–5.8) | 5.5 (4.9–6.5) | <0.001 |
| Uremic toxins | ||||
| IxS (µg/mL) | 2.22 (1.22–3.43) | 1.86 (1.09–3.04) | 2.30 (1.29–3.60) | 0.030 |
| PCS (µg/mL) | 4.32 (1.52–7.76) | 2.90 (1.52–5.48) | 4.96 (1.57–8.56) | 0.008 |
| TMAO (µg/mL) | 0.71 (0.35–1.54) | 0.58 (0.38–1.25) | 0.75 (0.33–1.61) | 0.347 |
| IAA (µg/mL) | 0.39 (0.25–0.57) | 0.36 (0.23–0.47) | 0.41 (0.26–0.60) | 0.015 |
| A | ||
| Crude Model | ||
| Plasma pCS Concentration (µg/mL) | ||
| OR (95%CI) | p-Value | |
| Age (years) | 1.03 (1.02; 1.05) | <0.0001 |
| BMI (kg/m2) | 1.02 (0.98; 1.06) | 0.245 |
| Sex (male) | 1.25 (0.84; 1.87) | 0.276 |
| Time since transplantation (months) | 1.002 (1.000; 1.004) | 0.088 |
| Albumin (g/L) | 0.95 (0.91; 1.00) | 0.065 |
| At least one OAT1/OAT3 inhibitor | 2.23 (1.38; 3.65) | 0.001 |
| eGFR (mL/min) | 0.96 (0.95; 0.97) | <0.0001 |
| B | ||
| Plasma pCS Concentration (µg/mL) | ||
| OR (95%CI) | p-Value | |
| Unadjusted | ||
| At least one OAT1/OAT3 inhibitor | 2.23 (1.38; 3.65) | 0.001 |
| Model 1 | ||
| At least one OAT1/OAT3 inhibitor | 1.98 (1.21; 3.27) | 0.007 |
| Age (years) | 1.03 (1.02; 1.05) | 0.0002 |
| Model 2 | ||
| At least one OAT1/OAT3 inhibitor | 1.99 (1.19; 3.35) | 0.009 |
| Age (years) | 1.02 (1.01; 1.04) | 0.005 |
| eGFR (mL/min) | 0.96 (0.95; 0.98) | <0.0001 |
| Model 3 | ||
| At least one OAT1/OAT3 inhibitor | 2.04 (1.22; 3.47) | 0.007 |
| Age (years) | 1.03 (1.01; 1.05) | 0.002 |
| eGFR (mL/min) | 0.96 (0.95; 0.97) | <0.0001 |
| Albumin (g/L) | 1.04 (0.98; 1.11) | 0.151 |
| Model 4 | ||
| At least one OAT1/OAT3 inhibitor | 2.11 (1.26; 3.61) | 0.005 |
| Age (years) | 1.03 (1.01; 1.05) | 0.003 |
| eGFR (mL/min) | 0.96 (0.95; 0.97) | <0.0001 |
| Albumin (g/L) | 1.05 (0.99; 1.11) | 0.123 |
| Time since transplantation (months) | 1.00 (1.00; 1.00) | 0.401 |
| A | ||
| Crude Model | ||
| Plasma IxS Concentration (µg/mL) | ||
| OR (95%CI) | p-Value | |
| Age (years) | 1.02 (1.01; 1.04) | 0.002 |
| BMI (kg/m2) | 1.04 (0.09; 0.79) | 0.016 |
| Sex (male) | 0.82 (0.55; 1.23) | 0.336 |
| Time since transplantation (months) | 1.00 (1.00; 1.01) | 0.011 |
| Albumin (g/L) | 0.93 (0.88; 0.98) | 0.004 |
| At least one OAT1/OAT3 inhibitor | 1.57 (0.98; 2.52) | 0.062 |
| eGFR (mL/min) | 0.92 (0.90; 0.93) | <0.0001 |
| B | ||
| Crude Model | ||
| Plasma IAA Concentration (µg/mL) | ||
| OR (95%CI) | p-Value | |
| Age (years) | 1.01 (1.00; 1.03) | 0.015 |
| BMI (kg/m2) | 1.02 (0.98; 1.06) | 0.330 |
| Sex (men) | 1.62 (1.08; 2.43) | 0.021 |
| Time since transplantation (months) | 1.00 (0.69; 1.29) | 0.653 |
| Albumin (g/L) | 1.02 (0.98; 1.08) | 0.304 |
| At least one OAT1/OAT3 inhibitor | 1.57 (0.98; 2.52) | 0.062 |
| eGFR (mL/min) | 0.98 (0.97; 0.99) | <0.0001 |
| Drug | Number of Prescriptions | Mean Dose Level (mg per Day) (Min–Max) | OAT Concerned by the Inhibition | In Vitro Data on OAT1/OAT3 Inhibition | Plasma Therapeutic Concentration Range (µg/mL) | References | ||
|---|---|---|---|---|---|---|---|---|
| Cell System | Substrate Used | IC50 (µg/mL) | ||||||
| Acetyl salicylate | 153 | 91 (37.5–300) | OAT3 | OAT3-HEK293 | Cilostazol | 2.3 | 3.2–5.1 | [45,46] |
| Bumetanide | 2 | 6.5 (3–10) | OAT3 | S2-hOAT3 | Estrone 3-sulfate | 0.27–2.80 | 0.03–0.40 | [40,41,47] |
| Diclofenac | 1 | NA | OAT1 | S2-hOAT1 | Para-aminohippurate | 1.3 | 0.5–3.0 | [42,48] |
| OAT3 | S2-hOAT3 | Estrone 3-sulfate | 2.3 | |||||
| Esomeprazole | 45 | 23 (20–80) | OAT3 | OAT3-HEK293 | Methotrexate | 0.41 | 0.78–1.07 | [20,49] |
| Fenofibrate | 3 | 111 (67–200) | OAT3 | CHO-OAT3 | Sitagliptin | 0.8 | 5–30 | [42,50] |
| Fluvastatin | 6 | 53 (20–80) | OAT3 | S2-hOAT3 | Estrone 3-sulfate | 0.24 | 0.05–0.40 | [42,51] |
| Furosemide | 90 | 68.5 (20–750) | OAT1 | S2-hOAT1 | Para-aminohippurate | 5.9 | 2–10 | [42,47] |
| OAT3 | S2-hOAT3 | Estrone 3-sulfate | 0.56 | [42,50] | ||||
| CHO-OAT3 | Sitagliptine | 2.4 | [42,47] | |||||
| Gemfibrozil | 1 | 450 | OAT3 | S2-hOAT3 | Pravastatin | 1.7 | 25 | [42,52] |
| Lansoprazole | 7 | 22.5 (15–30) | OAT1 | OAT1-HEK293 | Para-aminohippurate | 2.8 | 1.1–3.6 | [20,53,54] |
| OAT3 | OAT3-HEK293 | Methotrexate | 0.15–0.42 | |||||
| Losartan | 2 | 50 | OAT3 | OAT3-HEK293 | Uric acid | 0.68 | 0.20–0.65 | [42,55] |
| Omeprazole | 32 | 18.5 (10–20) | OAT1 | OAT1-HEK293 | Para-aminohippurate | 1.7 | 0.05–4.00 | [20,42,53] |
| OAT3 | OAT3-HEK293 | Methotrexate | 2.1–2.6 | |||||
| Pantoprazole | 159 | 25 (10–80) | OAT3 | OAT3-HEK293 | Methotrexate | 1.7 | 2.0–4.6 | [42,53] |
| Telmisartan | 2 | 40 | OAT1 | OAT1-HEK293 | Uric acid | 0.24 | 0.03–0.37 | [56,57] |
| OAT3 | OAT3-HEK293 | 0.82 | ||||||
| Valsartan | 9 | 124.5 (40–160) | OAT1 | OAT1-HEK293 | Uric acid | 7 | 0.8–6.0 | [42,56] |
| OAT3 | OAT3-HEK293 | 0.87 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
André, C.; Mernissi, T.; Choukroun, G.; Bennis, Y.; Kamel, S.; Liabeuf, S.; Bodeau, S. The Prescription of Drugs That Inhibit Organic Anion Transporters 1 or 3 Is Associated with the Plasma Accumulation of Uremic Toxins in Kidney Transplant Recipients. Toxins 2022, 14, 15. https://doi.org/10.3390/toxins14010015
André C, Mernissi T, Choukroun G, Bennis Y, Kamel S, Liabeuf S, Bodeau S. The Prescription of Drugs That Inhibit Organic Anion Transporters 1 or 3 Is Associated with the Plasma Accumulation of Uremic Toxins in Kidney Transplant Recipients. Toxins. 2022; 14(1):15. https://doi.org/10.3390/toxins14010015
Chicago/Turabian StyleAndré, Camille, Touria Mernissi, Gabriel Choukroun, Youssef Bennis, Saïd Kamel, Sophie Liabeuf, and Sandra Bodeau. 2022. "The Prescription of Drugs That Inhibit Organic Anion Transporters 1 or 3 Is Associated with the Plasma Accumulation of Uremic Toxins in Kidney Transplant Recipients" Toxins 14, no. 1: 15. https://doi.org/10.3390/toxins14010015
APA StyleAndré, C., Mernissi, T., Choukroun, G., Bennis, Y., Kamel, S., Liabeuf, S., & Bodeau, S. (2022). The Prescription of Drugs That Inhibit Organic Anion Transporters 1 or 3 Is Associated with the Plasma Accumulation of Uremic Toxins in Kidney Transplant Recipients. Toxins, 14(1), 15. https://doi.org/10.3390/toxins14010015