The Binding of Aripiprazole to Plasma Proteins in Chronic Renal Failure Patients

 , ,
, , 
 , , and
, , and 
Abstract
:1. Introduction
2. Results
2.1. Patients
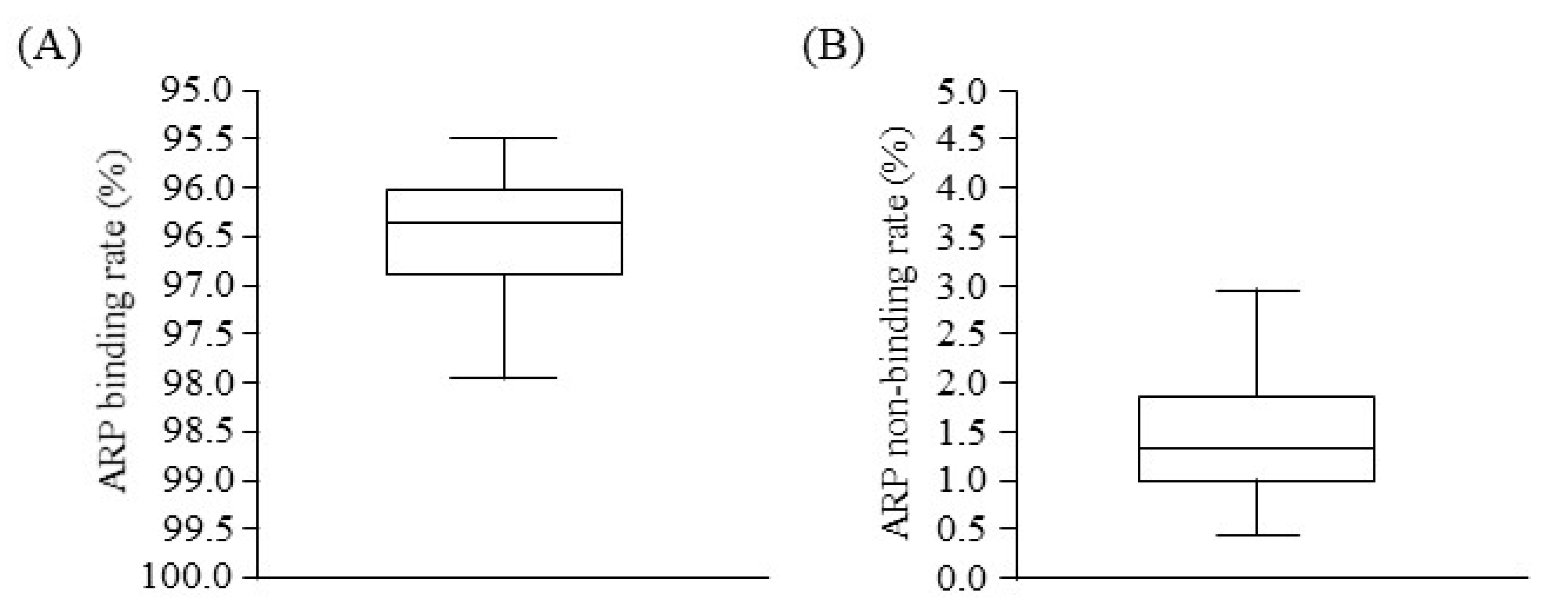
2.2. Binding of ARP to Plasma
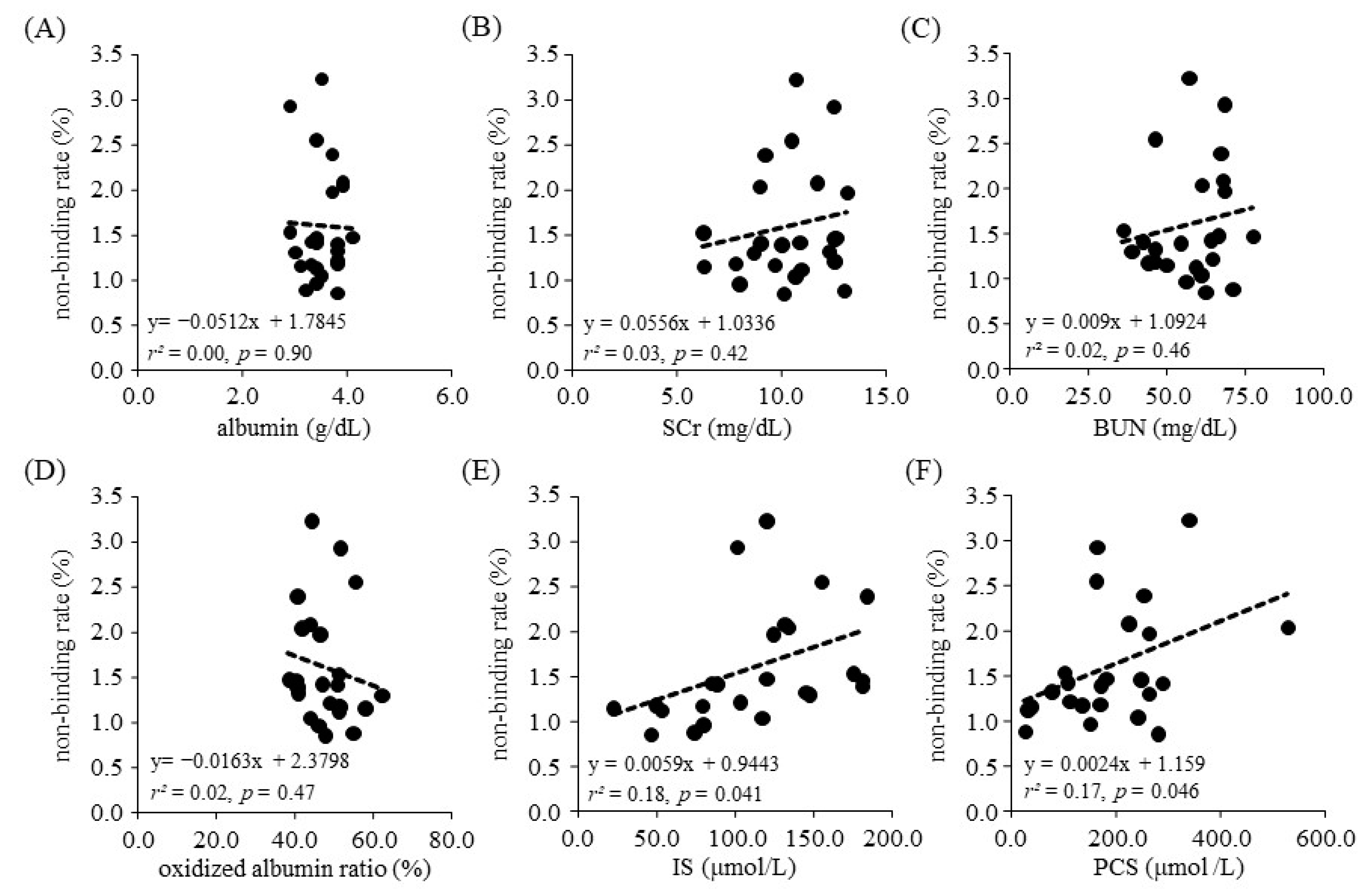
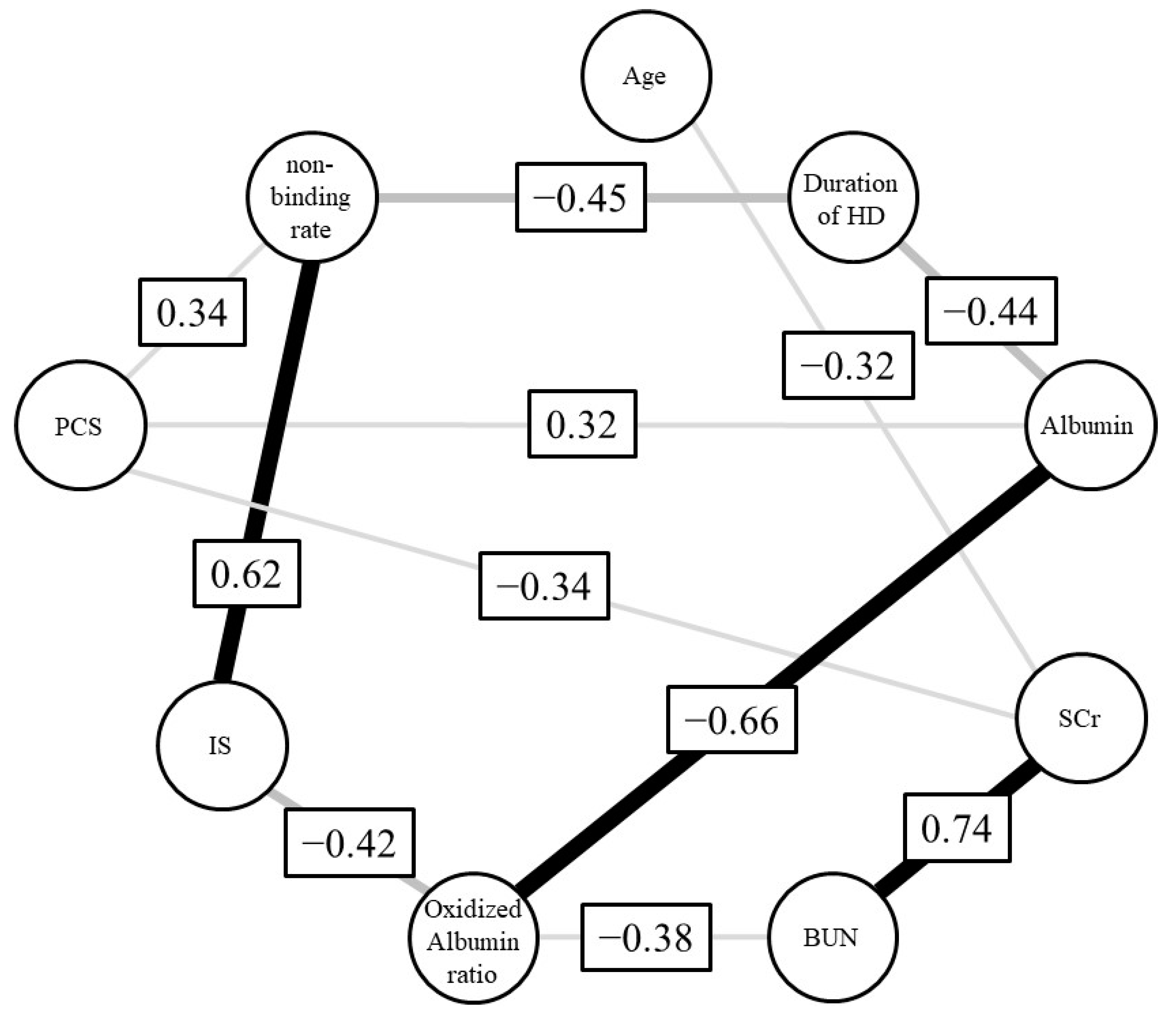
2.3. Relationship between ARP Binding and Biochemical Parameters
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Chemicals and Materials
5.2. Chromatography of Oxidized Albumin
5.3. Chromatography Analyses of Uremic Toxins and Drug
5.4. Equilibrium Dialysis
5.5. Statistical Analysis
5.6. Ethics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reidenberg, M.M.; Affrime, M. Influence of Disease on Binding of Drugs to Plasma Proteins. Ann. N. Y. Acad. Sci. 1973, 226, 115–126. [Google Scholar] [CrossRef]
- Sakurama, K.; Kawai, A.; Tuan Giam Chuang, V.; Kanamori, Y.; Osa, M.; Taguchi, K.; Seo, H.; Maruyama, T.; Imoto, S.; Yamasaki, K.; et al. Analysis of the Binding of Aripiprazole to Human Serum Albumin: The Importance of a Chloro-Group in the Chemical Structure. ACS Omega 2018, 3, 13790–13797. [Google Scholar] [CrossRef]
- Nishi, K.; Sakurama, K.; Kobashigawa, Y.; Morioka, H.; Udo, N.; Hashimoto, M.; Imoto, S.; Yamasaki, K.; Otagiri, M. Interaction of Aripiprazole With Human A1-Acid Glycoprotein. J. Pharm. Sci. 2019, 108, 3911–3916. [Google Scholar] [CrossRef]
- Crespo-Facorro, B.; de la Foz, V.O.-G.; Mata, I.; Ayesa-Arriola, R.; Suarez-Pinilla, P.; Valdizan, E.M.; Martinez-Garcia, O.; Pérez-Iglesias, R. Treatment of First-Episode Non-Affective Psychosis: A Randomized Comparison of Aripiprazole, Quetiapine and Ziprasidone over 1 Year. Psychopharmacology 2014, 231, 357–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakurama, K.; Nishi, K.; Chuang, V.T.G.; Hashimoto, M.; Yamasaki, K.; Otagiri, M. Effects of Oxidation of Human Serum Albumin on the Binding of Aripiprazole. Biol. Pharm. Bull. 2020, 43, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Nishi, K.; Sakurama, K.; Watanabe, H.; Maruyama, T.; Yamasaki, K.; Otagiri, M. Effects of Uremic Toxins on the Binding of Aripiprazole to Human Serum Albumin. Biol. Pharm. Bull. 2021, 44, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Skrede, S.; Blomhoff, J.P.; Elgjo, K.; Gjone, E. Serum Proteins in Diseases of the Liver. Scand. J. Clin. Lab. Investig. 1975, 35, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Lindup, W.E.; Henderson, S.J.; Barker, C.E. Drug Binding in renal Disease. In Plasma Binding of Drugs and Its Consequences; Belpaire, F., Bogaert, M., Tillement, J.P., Verbekk, R., Eds.; Academic Press: Ghent, Belgium, 1991; pp. 103–120. [Google Scholar]
- Yamasaki, K.; Chuang, V.T.G.; Maruyama, T.; Otagiri, M. Albumin-Drug Interaction and Its Clinical Implication. Biochim. Biophys. Acta 2013, 1830, 5435–5443. [Google Scholar] [CrossRef]
- Mera, K.; Anraku, M.; Kitamura, K.; Nakajou, K.; Maruyama, T.; Otagiri, M. The Structure and Function of Oxidized Albumin in Hemodialysis Patients: Its Role in Elevated Oxidative Stress via Neutrophil Burst. Biochem. Biophys. Res. Commun. 2005, 334, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Duranton, F.; Cohen, G.; De Smet, R.; Rodriguez, M.; Jankowski, J.; Vanholder, R.; Argiles, A. Normal and Pathologic Concentrations of Uremic Toxins. J. Am. Soc. Nephrol. 2012, 23, 1258–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Noguchi, T.; Miyamoto, Y.; Kadowaki, D.; Kotani, S.; Nakajima, M.; Miyamura, S.; Ishima, Y.; Otagiri, M.; Maruyama, T. Interaction between Two Sulfate-Conjugated Uremic Toxins, p-Cresyl Sulfate and Indoxyl Sulfate, during Binding with Human Serum Albumin. Drug Metab. Dispos. 2012, 40, 1423–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.F. Removal of Fatty Acids from Serum Albumin by Charcoal Treatment. J. Biol. Chem. 1967, 242, 173–181. [Google Scholar] [CrossRef]
- Anraku, M.; Kitamura, K.; Shinohara, A.; Adachi, M.; Suenaga, A.; Maruyama, T.; Miyanaka, K.; Miyoshi, T.; Shiraishi, N.; Nonoguchi, H.; et al. Intravenous Iron Administration Induces Oxidation of Serum Albumin in Hemodialysis Patients. Kidney Int. 2004, 66, 841–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenett, D.Y.; Tumminello, M.; Madi, A.; Gur-Gershgoren, G.; Mantegna, R.N.; Ben-Jacob, E. Dominating Clasp of the Financial Sector Revealed by Partial Correlation Analysis of the Stock Market. PLoS ONE 2010, 5, e15032. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Healthy Volunteers (n = 4) | HD Patients (n = 24) | p-Value | |
|---|---|---|---|
| Age, median (IQR) | 24.50 (23.50, 25.50) | 78.50 (72.75, 84.00) | 0.002 |
| Gender, (Male/Female) | 2/2 | 14/10 | 1.00 |
| Duration of HD (Year), median (IQR) | - | 7.50 (3.00, 12.00) | - |
| SCr (mg/dL), median (IQR) | 0.66 (0.56, 0.74) | 10.53 (8.95, 12.31) | <0.001 |
| BUN (mg/dL), median (IQR) | 10.10 (9.60, 11.10) | 56.65 (45.95, 66.20) | 0.002 |
| Albumin (g/dL), median (IQR) | 4.30 (4.25, 4.32) | 3.45 (3.30, 3.80) | 0.002 |
| Oxidized albumin ratio (%), median (IQR) | 21.89 (20.05, 24.98) | 47.08 (43.10, 50.95) | 0.002 |
| IS (mol/L), median (IQR) | 5.20 (4.75, 6.02) | 118.56 (79.53, 145.57) | <0.001 |
| PCS (mol/L), median (IQR) | 10.85 (3.47, 23.06) | 170.02 (110.01, 255.26) | 0.001 |
| Arp non-binding rate (%), median (IQR) | 0.64 (0.58, 0.67) | 1.42 (1.19, 2.01) | <0.001 |
| Age | Duration of HD | SCr | BUN | Albumin | Oxidized Albumin Ratio | IS | PCS | Arp Non-Binding Rate | |
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| Duration of HD | 0.07 (0.75) | ||||||||
| SCr | −0.32 (0.13) | 0.07 (0.74) | |||||||
| BUN | −0.16 (0.46) | −0.01 (0.97) | 0.74 (<0.001) | ||||||
| Albumin | −0.44 (0.03) | −0.26 (0.22) | 0.23 (0.29) | 0.23 (0.28) | |||||
| Oxidized albumin ratio | 0.44 (0.03) | −0.04 (0.87) | −0.27 (0.2) | −0.37 (0.08) | −0.7 (<0.001) | ||||
| IS | −0.24 (0.25) | 0.07 (0.76) | 0.07 (0.73) | 0.04 (0.85) | 0.16 (0.47) | −0.47 (0.02) | |||
| PCS | −0.17 (0.43) | −0.06 (0.78) | −0.07 (0.74) | 0.11 (0.62) | 0.40 (0.06) | −0.40 (0.06) | 0.33 (0.12) | ||
| Arp non- binding rate | −0.11 (0.59) | −0.26 (0.21) | 0.15 (0.48) | 0.18 (0.4) | 0.10 (0.64) | −0.24 (0.25) | 0.64 (0.001) | 0.39 (0.06) |
| Age | Duration of HD | SCr | BUN | Albumin | Oxidized Albumin Ratio | IS | PCS | Arp Non-Binding Rate | |
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| Duration of HD | 0.11 (0.68) | ||||||||
| SCr | −0.32 (0.21) | 0.26 (0.31) | |||||||
| BUN | 0.22 (0.41) | −0.15 (0.57) | 0.74 (0.001) | ||||||
| Albumin | −0.11 (0.67) | −0.44 (0.08) | 0.24 (0.35) | −0.22 (0.4) | |||||
| Oxidized albumin ratio | 0.17 (0.53) | −0.28 (0.29) | 0.2 (0.44) | −0.38 (0.14) | −0.66 (0.004) | ||||
| IS | −0.11 (0.68) | 0.21 (0.43) | 0.02 (0.93) | −0.22 (0.39) | −0.18 (0.49) | −0.42 (0.09) | |||
| PCS | −0.06 (0.81) | 0.21 (0.42) | −0.34 (0.18) | 0.2 (0.43) | 0.32 (0.21) | 0.01 (0.98) | −0.01 (0.97) | ||
| Arp non- binding rate | 0.1 (0.72) | −0.45 (0.07) | 0.17 (0.51) | 0.06 (0.83) | −0.16 (0.53) | 0.05 (0.84) | 0.62 (0.008) | 0.34 (0.18) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirata, K.; Ikeda, T.; Watanabe, H.; Maruyama, T.; Tanaka, M.; Chuang, V.T.G.; Uchida, Y.; Sakurama, K.; Nishi, K.; Yamasaki, K.; et al. The Binding of Aripiprazole to Plasma Proteins in Chronic Renal Failure Patients. Toxins 2021, 13, 811. https://doi.org/10.3390/toxins13110811
Hirata K, Ikeda T, Watanabe H, Maruyama T, Tanaka M, Chuang VTG, Uchida Y, Sakurama K, Nishi K, Yamasaki K, et al. The Binding of Aripiprazole to Plasma Proteins in Chronic Renal Failure Patients. Toxins. 2021; 13(11):811. https://doi.org/10.3390/toxins13110811
Chicago/Turabian StyleHirata, Kenshiro, Tokunori Ikeda, Hiroshi Watanabe, Toru Maruyama, Motoko Tanaka, Victor Tuan Giam Chuang, Yuji Uchida, Keiki Sakurama, Koji Nishi, Keishi Yamasaki, and et al. 2021. "The Binding of Aripiprazole to Plasma Proteins in Chronic Renal Failure Patients" Toxins 13, no. 11: 811. https://doi.org/10.3390/toxins13110811
APA StyleHirata, K., Ikeda, T., Watanabe, H., Maruyama, T., Tanaka, M., Chuang, V. T. G., Uchida, Y., Sakurama, K., Nishi, K., Yamasaki, K., & Otagiri, M. (2021). The Binding of Aripiprazole to Plasma Proteins in Chronic Renal Failure Patients. Toxins, 13(11), 811. https://doi.org/10.3390/toxins13110811