A Randomized Double-Blind Trial of the Effect of Liupao Tea on Metabolic Parameters, Body Composition, and Gut Microbiota in Adults with Metabolic Syndrome





Abstract
1. Introduction
2. Materials and Methods
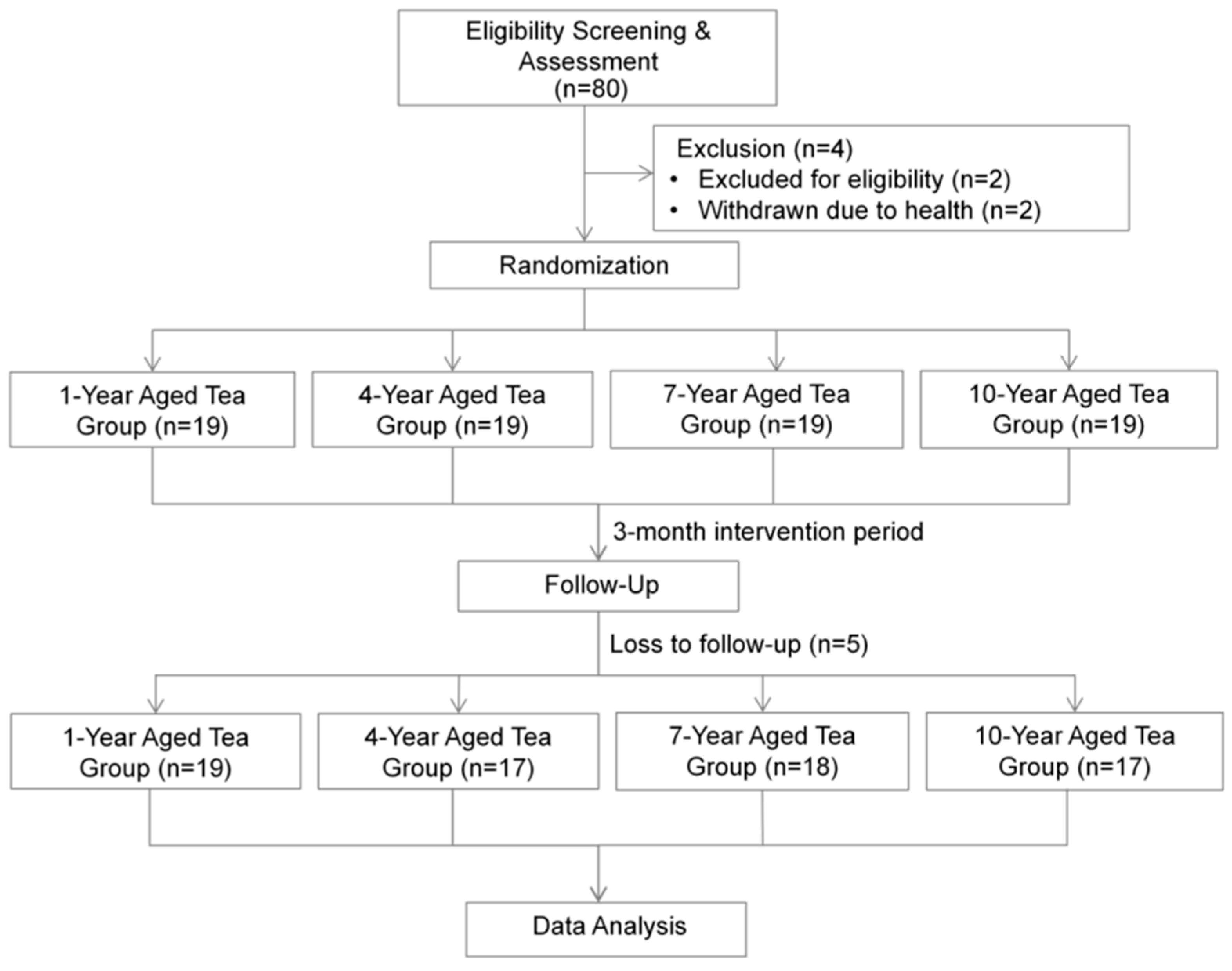
2.1. Study Design
2.2. Study Population
2.3. Sample Size Estimation
2.4. Randomization and Blinding
2.5. Intervention and Adherence Monitoring
2.6. Questionnaire Survey and Clinical Parameter Measurement
2.7. Body Composition Measurement
2.8. DNA Extraction and Amplification Library Construction
2.9. Bioinformatics Analysis and Diversity Analysis
2.10. Statistical Analysis
3. Results
3.1. Basic Characteristics of Participants
3.2. Impact of LPT on Metabolic Parameters in MetS Patients
3.3. Impact of LPT on Body Weight and Body Composition Parameters in MetS Patients
3.4. Comparison of LPT Interventions with Different Aging Times on Metabolic and Physical Parameters
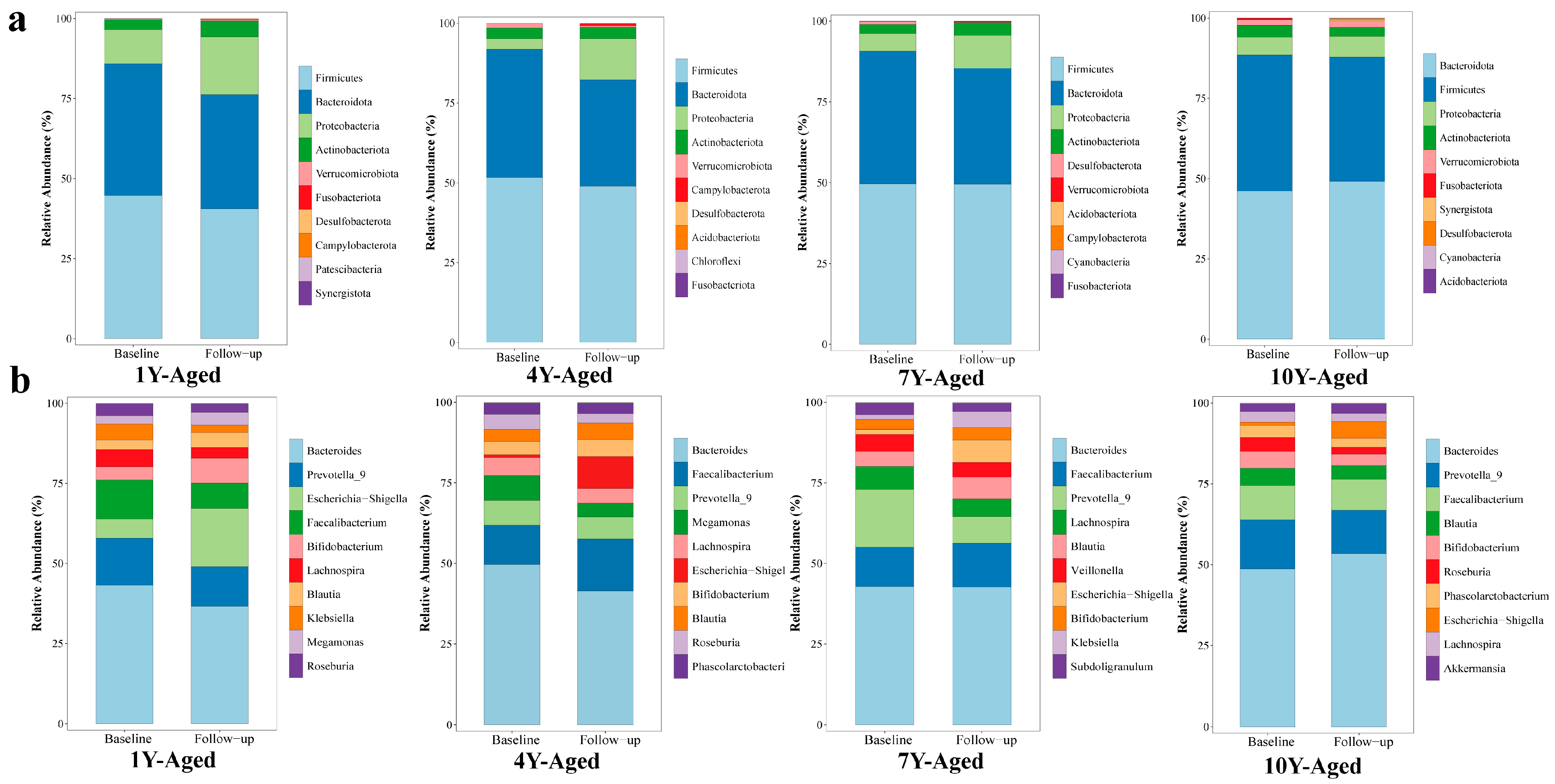
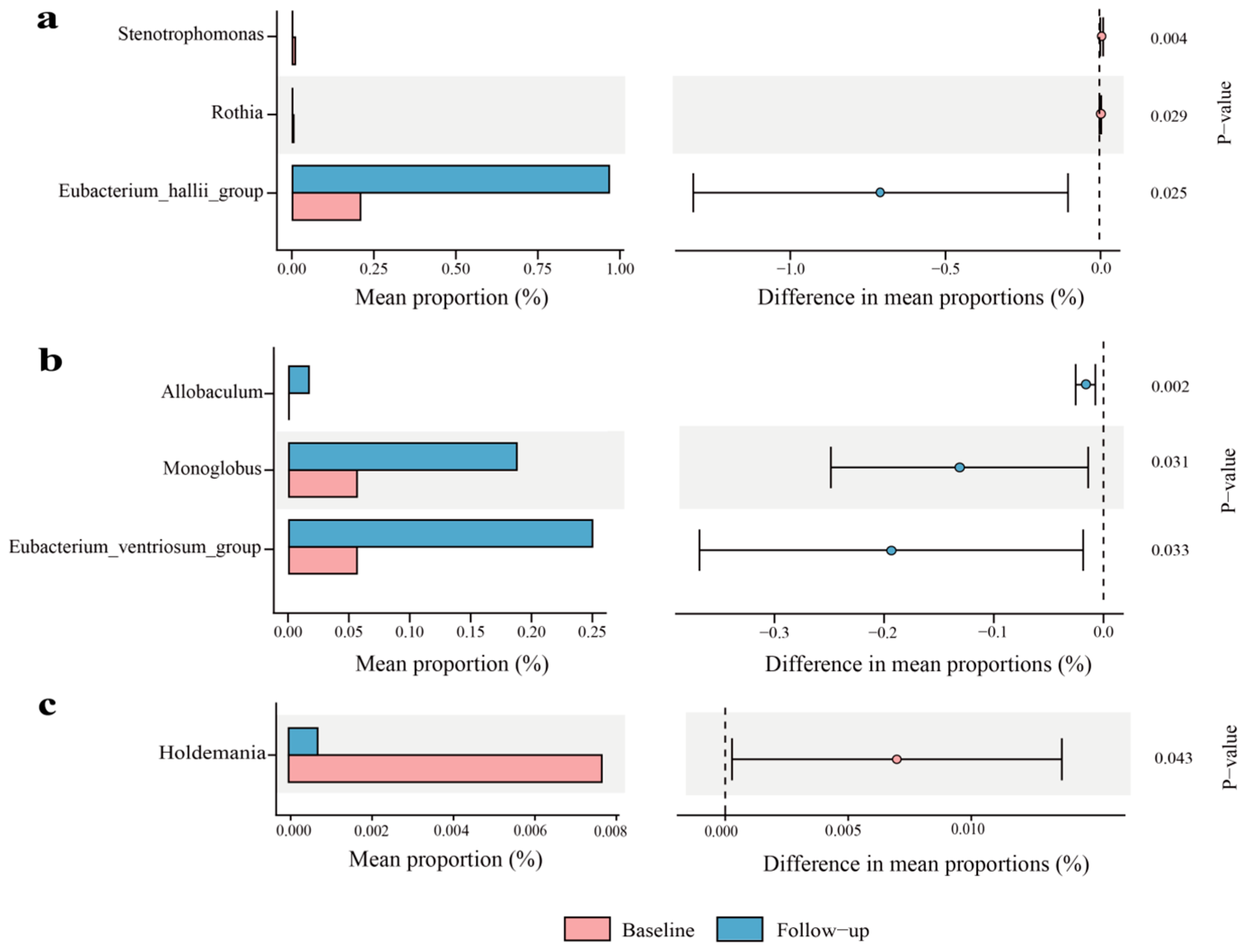
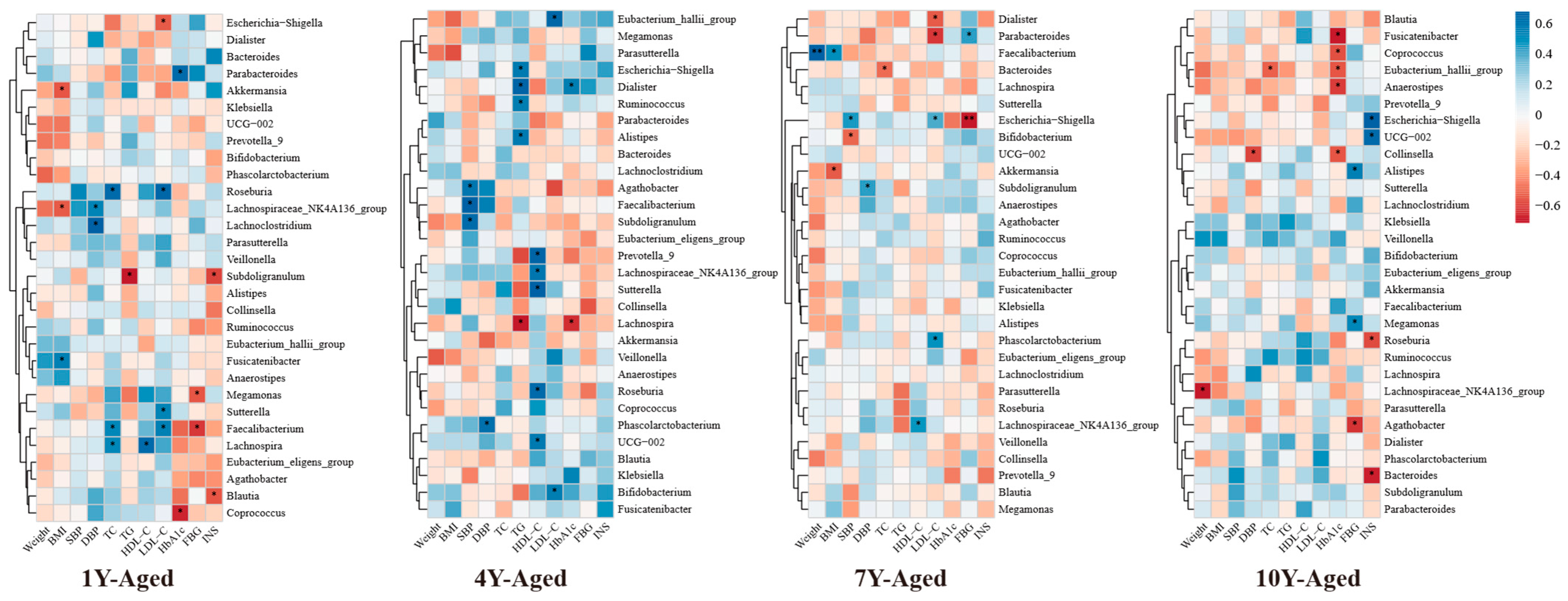
3.5. Effects of LPT with Different Aging Years on the Gut Microbiota of MetS Patients
4. Discussion
4.1. Major Findings and Comparison with Previous Research
4.2. The Limitations of the Study
4.3. Practical Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Ndoadoumgue, A.L.; et al. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals. Diabetes Res. Clin. Pract. 2022, 188, 109924. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Huang, J.L.W.; Withers, M.; Chien, K.-L.; Trihandini, I.; Elcarte, E.; Chung, V.; Wong, M.C.S. Prevalence of metabolic syndrome in Chinese women and men: A systematic review and meta-analysis of data from 734, 511 individuals. Lancet 2018, 392, S14. [Google Scholar] [CrossRef]
- Chong, K.S.; Chang, Y.H.; Yang, C.T.; Chou, C.K.; Ou, H.T.; Kuo, S. Longitudinal economic burden of incident complications among metabolic syndrome populations. Cardiovasc. Diabetol. 2024, 23, 246. [Google Scholar] [CrossRef] [PubMed]
- Scholze, J.; Alegria, E.; Ferri, C.; Langham, S.; Stevens, W.; Jeffries, D.; Uhl-Hochgraeber, K. Epidemiological and economic burden of metabolic syndrome and its consequences in patients with hypertension in Germany, Spain and Italy; a prevalence-based model. BMC Public Health 2010, 10, 529. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Zeng, Y.; Peng, J.; Zhang, K.; Wang, L.; Feng, T.; Nhamdriel, T.; Fan, G. Phytochemicals for the treatment of metabolic diseases: Evidence from clinical studies. Biomed. Pharmacother. 2023, 165, 115274. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liu, C.; Fang, W.; Tang, Q.; Zhan, L.; Shi, Y.; Tang, M.; Liu, Z.; Zhang, S.; Liu, A. Research progress on the lipid-lowering and weight loss effects of tea and the mechanism of its functional components. J. Nutr. Biochem. 2023, 112, 109210. [Google Scholar] [CrossRef] [PubMed]
- Esmaeelpanah, E.; Razavi, B.M.; Hosseinzadeh, H. Green tea and metabolic syndrome: A 10-year research update review. Iran. J. Basic Med. Sci. 2021, 24, 1159–1172. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.H.T.; Burlutsky, G.; Gopinath, B.; Flood, V.M.; Mitchell, P.; Louie, J.C.Y. The longitudinal association between coffee and tea consumption and the risk of metabolic syndrome and its component conditions in an older adult population. J. Nutr. Sci. 2022, 11, e79. [Google Scholar] [CrossRef] [PubMed]
- Sae-tan, S.; Grove, K.A.; Lambert, J.D. Weight control and prevention of metabolic syndrome by green tea. Pharmacol. Res. 2011, 64, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yu, D.; Piao, W.; Huang, K.; Zhao, L. Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017. Nutrients 2022, 14, 3502. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.; Bao, Y.Y.; Wei, G.F.; Wang, W.; Xu, H.Q.; Chen, J.Y.; Xu, Y.N.; Han, D.; Tao, L.; Ni, J.T. Association of tea and coffee consumption with the risk of all-cause and cause-specific mortality among individuals with metabolic syndrome: A prospective cohort study. Diabetol. Metab. Syndr. 2023, 15, 241. [Google Scholar] [CrossRef] [PubMed]
- Vernarelli, J.A.; Lambert, J.D. Tea consumption is inversely associated with weight status and other markers for metabolic syndrome in US adults. Eur. J. Nutr. 2013, 52, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Salomone, F.; Godos, J.; Pluchinotta, F.; Del Rio, D.; Mistretta, A.; Grosso, G. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: A systematic review and meta-analysis of observational studies. Clin. Nutr. 2016, 35, 1269–1281. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.Z.; Li, N.; Zhou, F.; Ouyang, J.; Lu, D.M.; Xu, W.; Li, J.; Lin, H.Y.; Zhang, Z.; Xiao, J.B.; et al. Microbial bioconversion of the chemical components in dark tea. Food Chem. 2020, 312, 126043. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Chai, S.; Li, Y.; Huang, J.; Luo, Y.; Xiao, L.; Liu, Z. Biochemical Components Associated With Microbial Community Shift During the Pile-Fermentation of Primary Dark Tea. Front. Microbiol. 2018, 9, 1509. [Google Scholar] [CrossRef] [PubMed]
- Qiong, S.; Xishuang, Y. History of Pu’er Tea and comparative study for the effect of its various extracts on lipid-lowering diet. Pak. J. Pharm. Sci. 2014, 27, 1015–1022. [Google Scholar] [PubMed]
- Feng, X.; Chen, M.; Song, H.; Ma, S.; Ou, C.; Li, Z.; Hu, H.; Yang, Y.; Zhou, S.; Pan, Y.; et al. A systemic review on Liubao tea: A time-honored dark tea with distinctive raw materials, process techniques, chemical profiles, and biological activities. Compr. Rev. Food Sci. Food Saf. 2023, 22, 5063–5085. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Sun, H.; Yi, R.; Tan, F.; Zhao, X. Anti-obesity effect of Liupao tea extract by modulating lipid metabolism and oxidative stress in high-fat-diet-induced obese mice. J. Food Sci. 2021, 86, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Chinese Elderly Type 2 Diabetes Prevention and Treatment of Clinical Guidelines Writing Group; Geriatric Endocrinology and Metabolism Branch of Chinese Geriatric Society; Geriatric Endocrinology and Metabolism Branch of Chinese Geriatric Health Care Society; Geriatric Professional Committee of Beijing Medical Award Foundation; National Clinical Medical Research Center for Geriatric Diseases (PLA General Hospital). Clinical guidelines for prevention and treatment of type 2 diabetes mellitus in the elderly in China (2022 edition). Zhonghua Nei Ke Za Zhi 2022, 61, 12–50. [Google Scholar] [CrossRef]
- Chu, S.L.; Fu, H.; Yang, J.X.; Liu, G.X.; Dou, P.; Zhang, L.; Tu, P.F.; Wang, X.M. A randomized double-blind placebo-controlled study of Pu’er tea extract on the regulation of metabolic syndrome. Chin. J. Integr. Med. 2011, 17, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wan, C.; Huang, Y.; Li, M. Effects of tea consumption on metabolic syndrome: A systematic review and meta-analysis of randomized clinical trials. Phytother. Res. 2020, 34, 2857–2866. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.M.; Puddey, I.B.; Woodman, R.J.; Mulder, T.P.; Fuchs, D.; Scott, K.; Croft, K.D. Effects of black tea on blood pressure: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Chen, X.; Zhu, X.; Liu, S.; Li, J.; Xu, J.; Zhao, J.; Ji, X. Pu-Erh Tea Relaxes the Thoracic Aorta of Rats by Reducing Intracellular Calcium. Front. Pharmacol. 2019, 10, 1430. [Google Scholar] [CrossRef] [PubMed]
- Xiao, T.; Li, Y.; Li, H.; Wang, K.; Huang, J.; Liu, Z.; Zhu, M. Tea consumption in relation with metabolic syndrome and obesity: A systematic review and meta-analysis of randomized clinical trials. Food Biosci. 2024, 61, 104322. [Google Scholar] [CrossRef]
- Huang, S.; Chen, H.; Teng, J.; Wu, Z.; Huang, L.; Wei, B.; Xia, N. Antihyperlipidemic effect and increased antioxidant enzyme levels of aqueous extracts from Liupao tea and green tea in vivo. J. Food Sci. 2022, 87, 4203–4220. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Zhang, B.; Zheng, W.; Chen, X.; Zhang, J.; Yan, R.; Zhang, T.; Yu, L.; Dong, Y.; Ma, B. Liupao tea extract alleviates diabetes mellitus and modulates gut microbiota in rats induced by streptozotocin and high-fat, high-sugar diet. Biomed. Pharmacother. 2019, 118, 109262. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Sanchez, K.; Leyva, M.J.; Wu, M.; Betts, N.M.; Aston, C.E.; Lyons, T.J. Green tea supplementation affects body weight, lipids, and lipid peroxidation in obese subjects with metabolic syndrome. J. Am. Coll. Nutr. 2010, 29, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.Y.; Chou, J.I.; Ueng, K.C.; Chou, M.Y.; Yang, J.J.; Lin-Shiau, S.Y.; Hu, M.E.; Lin, J.K. Weight reduction effect of Puerh tea in male patients with metabolic syndrome. Phytother. Res. 2014, 28, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Dai, W.; Zhang, X.; Lu, J.; Song, F.; Li, H. Chemical components of Fu brick tea and its potential preventive effects on metabolic syndrome. Food Sci. Nutr. 2024, 12, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Zhang, Z.; Cui, Y.; Peng, C.; Fan, Y.; Tan, C.; Wang, Q.; Liu, Z.; Gong, J. Pu-erh tea and theabrownin ameliorate metabolic syndrome in mice via potential microbiota-gut-liver-brain interactions. Food Res. Int. 2022, 162, 112176. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Huang, L.; Du, L.; Sun, Q.; Chen, C.; Tang, J.; Teng, J.; Wei, B. Structural Characterization and In Vitro Antioxidant, Hypoglycemic and Hypolipemic Activities of a Natural Polysaccharide from Liupao Tea. Foods 2023, 12, 2226. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, X.; She, Z.; Huang, L.; Wei, H.; Yang, S.; Wei, Z.; Chen, H.; Yang, B.; Hu, Z.; et al. Combining bioinformatics and multiomics strategies to investigate the key microbiota and active components of Liupao tea ameliorating hyperlipidemia. J. Ethnopharmacol. 2024, 333, 118438. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Zhu, M.Z.; Tang, J.Y.; Ou-Yang, J.; Shang, B.H.; Liu, C.W.; Wang, J.; Liu, Q.; Huang, J.A.; Liu, Z.H. Six types of tea extracts attenuated high-fat diet-induced metabolic syndrome via modulating gut microbiota in rats. Food Res. Int. 2022, 161, 111788. [Google Scholar] [CrossRef] [PubMed]
- Yue, S.; Peng, C.; Zhao, D.; Xia, X.; Tan, C.; Wang, Q.; Gong, J. Theabrownin isolated from Pu-erh tea regulates Bacteroidetes to improve metabolic syndrome of rats induced by high-fat, high-sugar and high-salt diet. J. Sci. Food Agric. 2022, 102, 4250–4265. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Liu, X.; Lan, L.; Yu, W.; Qiu, R.; Wu, J.; Teng, C.; Huang, L.; Yu, C.; Zeng, Y. Protective effects of Liupao tea against high-fat diet/cold exposure-induced irritable bowel syndrome in rats. Heliyon 2023, 9, e16613. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; Vogensen, F.K.; van den Berg, F.W.; Nielsen, D.S.; Andreasen, A.S.; Pedersen, B.K.; Al-Soud, W.A.; Sorensen, S.J.; Hansen, L.H.; Jakobsen, M. Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS ONE 2010, 5, e9085. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Slaven, B.; Clarke, L.G.; Ludwig, J.; Shields, R.K. Clinical and microbiologic outcomes of Stenotrophomonas maltophilia bloodstream infections. Infection, 2025; online ahead of print. [Google Scholar] [CrossRef]
- Sato, F.T.; Yap, Y.A.; Crisma, A.R.; Portovedo, M.; Murata, G.M.; Hirabara, S.M.; Ribeiro, W.R.; Marcantonio Ferreira, C.; Cruz, M.M.; Pereira, J.N.B.; et al. Tributyrin Attenuates Metabolic and Inflammatory Changes Associated with Obesity through a GPR109A-Dependent Mechanism. Cells 2020, 9, 2007. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, J.; Zhang, M.; Li, B.; Pan, X.; Dong, X.; Pan, L.L.; Sun, J. GPR109a Regulates Phenotypic and Functional Alterations in Macrophages and the Progression of Type 1 Diabetes. Mol. Nutr. Food Res. 2022, 66, e2200300. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Hou, Y.; Lao, X. The Role of Akkermansia muciniphila in Disease Regulation. Probiotics Antimicrob. Proteins, 2025; online ahead of print. [Google Scholar] [CrossRef]
- Costa, M.A.C.; da Silva Duarte, V.; Fraiz, G.M.; Cardoso, R.R.; da Silva, A.; Martino, H.S.D.; Dos Santos D’Almeida, C.T.; Ferreira, M.S.L.; Corich, V.; Hamaker, B.R.; et al. Regular Consumption of Black Tea Kombucha Modulates the Gut Microbiota in Individuals with and without Obesity. J. Nutr. 2025, 155, 1331–1349. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jiang, H.; Peng, X.H.; Zhao, Y.L.; Huang, X.J.; Yuan, K.; Yang, Y.F.; Du, Y.; Ji, S.; Tang, D.Q. Mulberry leaf improves type 2 diabetes in mice via gut microbiota-SCFAs-GPRs axis and AMPK signaling pathway. Phytomedicine 2025, 145, 156970. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Liu, Z.; Pang, Y.; Li, M.; Zheng, S.; Pan, F.; Guo, C.; Wu, Q.; Chen, T.; Li, Q.; et al. Effects of storage durations on flavour and bacterial communities in Liupao tea. Food Chem. 2025, 470, 142697. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liu, H.; Wang, J.; Zhang, R.; Zhang, Y.; Liu, Z.; Pang, Y.; Yang, C.; Nie, J. Impact of the long-term storage on flavor quality of Liupao tea using sensory evaluation combined with metabolomics analysis. Food Res. Int. 2024, 198, 115386. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Population Group (n = 71) | 1-Year-Aged Group (n = 19) | 4-Year-Aged Group (n = 17) | 7-Year-Aged Group (n = 18) | 10-Year-Aged Group (n = 17) | p |
|---|---|---|---|---|---|---|
| Age (years), mean ± SD | 53.5 ± 16.3 | 53.6 ±17.8 | 55.2 ±14.2 | 50.5 ± 18.7 | 54.9 ± 14.7 | 0.825 |
| Gender, n (%) | 0.901 | |||||
| Male | 19 (26.8) | 5 (26.3) | 4 (23.5) | 6 (33.3) | 4 (23.5) | |
| Female | 52 (73.2) | 14 (73.7) | 13 (76.3) | 12 (66.7) | 13 (76.5) | |
| Marital Status, n (%) | 0.501 | |||||
| Married/Cohabiting | 56 (78.9) | 15 (78.9) | 15 (88.2) | 12 (66.7) | 14 (82.4) | |
| Single/Divorced/Widowed | 15 (21.1) | 4 (21.1) | 2 (11.8) | 6 (33.3) | 3 (17.6) | |
| Educational Level, n (%) | 0.935 | |||||
| Junior high school and below | 5 (7.0) | 1 (5.3) | 1 (5.9) | 2 (11.1) | 1 (5.9) | |
| High school | 11 (15.5)) | 3 (15.8) | 2 (11.8) | 2 (11.1) | 4 (23.5) | |
| Bachelor’s degree and above | 55 (77.5) | 15 (78.9) | 14 (82.4) | 14 (77.8) | 12 (70.6) | |
| Average Monthly Income, n (%) | 0.324 | |||||
| RMB < 3000 | 9 (12.6) | 3 (15.8) | 0 (0.0) | 4 (22.2) | 2 (11.8) | |
| RMB 3000~8000 | 31 (43.7) | 8 (42.1) | 9 (52.9) | 4 (22.2) | 10 (58.8) | |
| RMB ≥ 8000 | 31 (43.7) | 8 (42.1) | 8 (47.1) | 10 (55.6) | 5 (29.4) | |
| Smoking, n (%) | 0.119 | |||||
| Never smoked | 66 (93.0) | 17 (89.5) | 14 (82.4) | 18 (100.0) | 17 (100.0) | |
| Former smoker | 3 (4.2) | 2 (10.5) | 1 (5.9) | 0 (0.0) | 0 (0.0) | |
| Current smoker | 2 (2.8) | 0 (0.0) | 2 (11.8) | 0 (0.0) | 0 (0.0) | |
| Alcohol Consumption, n (%) | 0.179 | |||||
| Never drinks | 63 (88.7) | 18 (94.7) | 13 (76.5) | 16 (88.9) | 16 (94.1) | |
| Former drinker | 6 (8.5) | 1 (5.3) | 4 (23.5) | 1 (5.6) | 0 (0.0) | |
| Current drinker | 2 (2.8) | 0 (0.0) | 0 (0.0) | 1 (5.6) | 1 (5.9) | |
| Frequent Tea Drinking, n(%) | 0.411 | |||||
| Yes | 33 (46.5) | 9 (47.4) | 9 (52.9) | 10 (55.6) | 5 (29.4) | |
| No | 38 (53.5) | 10 (52.6) | 8 (47.1) | 8 (44.4) | 12 (70.6) |
| Parameters | 1-Year-Aged Group (n = 19) | 4-Year-Aged Group (n = 17) | 7-Year-Aged Group (n = 18) | 10-Year-Aged Group (n = 17) | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | |
| Metabolic parameters | ||||||||
| SBP, mmHg | 128.58 ± 22.29 | 124.00 ± 18.69 | 129.06 ± 15.43 | 120.76 ± 17.64 * | 134.11 ± 13.63 | 116.34 ± 27.12 * | 132.41 ± 16.53 | 124.41 ± 15.78 * |
| DBP, mmHg | 74.95 ± 12.99 | 72.79 ± 12.21 | 77.65 ± 9.77 | 73.88 ± 10.16 | 79.72 ± 10.47 | 75.83 ± 17.44 | 85.24 ± 15.47 | 75.35 ± 10.70 * |
| TC, mmol/L | 5.43 ± 1.03 | 5.11 ± 0.85 * | 5.51 ± 1.09 | 5.36 ± 1.03 | 5.44 ± 0.90 | 5.57 ± 0.86 | 5.60 ± 0.70 | 5.15 ± 0.88 |
| TG, mmol/L | 1.34 ± 0.92 | 1.37 ± 1.00 | 1.51 ± 1.31 | 1.21 ± 0.58 | 1.82 ± 0.92 | 1.87 ± 1.26 | 2.10 ± 2.17 | 1.88 ± 1.88 |
| HDL-C, mmol/L | 1.36 ± 0.41 | 1.39 ± 0.34 | 1.28 ± 0.22 | 1.40 ± 0.21 * | 1.29 ± 0.31 | 1.38 ± 0.26 * | 1.34 ± 0.26 | 1.37 ± 0.18 |
| LDL-C, mmol/L | 3.13 ± 0.62 | 2.77 ± 0.54 ** | 3.29 ± 0.80 | 3.03 ± 0.72 * | 3.28 ± 0.60 | 3.02 ± 0.54 * | 3.15 ± 0.47 | 2.73 ± 0.59 * |
| APOA1, g/L | 1.34 ± 0.26 | 1.26 ± 0.22 * | 1.31 ± 0.16 | 1.26 ± 0.12 | 1.31 ± 0.16 | 1.24 ± 0.12 * | 1.37 ± 0.17 | 1.26 ± 0.13 ** |
| APOB, g/L | 0.90 ± 0.15 | 0.86 ± 0.14 * | 0.94 ± 0.19 | 0.93 ± 0.24 | 0.94 ± 0.14 | 0.89 ± 0.12 | 0.88 ± 0.15 | 0.85 ± 0.15 |
| HbA1c, % | 5.58 ± 1.07 | 5.65 ± 1.07 | 5.74 ± 0.76 | 5.74 ± 0.75 | 6.04 ± 1.34 | 6.03 ± 1.20 | 6.01 ± 1.51 | 6.08 ± 1.62 |
| FBG, mmol/L | 5.90 ± 2.06 | 5.82 ± 2.27 | 5.89 ± 1.35 | 5.70 ± 1.16 | 9.43 ± 13.26 | 6.28 ± 1.86 | 6.49 ± 2.90 | 6.28 ± 2.30 |
| INS, pmol/L | 71.11 ± 35.14 | 71.25 ± 48.32 | 67.57 ± 28.76 | 61.07 ± 30.41 | 74.24 ± 29.98 | 72.88 ± 37.20 | 92.59 ± 58.33 | 80.92 ± 52.34 |
| Body composition | ||||||||
| Weight, kg | 66.82 ± 13.10 | 65.68 ± 13.16 * | 66.42 ± 7.18 | 64.60 ± 7.07 * | 68.83 ± 10.70 | 66.26 ± 11.29 * | 69.75 ± 10.13 | 68.15 ± 11.60 * |
| BFM, kg | 21.27 ± 5.01 | 19.92 ± 4.72 ** | 21.48 ± 4.11 | 19.82 ± 4.07 ** | 21.25 ± 4.78 | 19.11 ± 4.27 ** | 22.09 ± 6.08 | 20.12 ± 5.43 ** |
| LBM, kg | 45.87 ± 10.01 | 46.50 ± 10.64 | 44.95 ± 5.22 | 45.32 ± 5.72 | 47.56 ± 8.34 | 47.73 ± 9.13 | 46.66 ± 7.77 | 47.17 ± 8.49 |
| MM, kg | 42.06 ± 9.30 | 42.71 ± 9.92 * | 41.17 ± 4.88 | 41.03 ± 5.51 | 43.65 ± 7.77 | 43.91 ± 8.52 | 42.71 ± 7.23 | 43.26 ± 7.90 |
| BMI, kg/m2 | 25.28 ± 2.96 | 24.95 ± 3.07 | 25.81 ± 2.51 | 25.13 ± 2.46 * | 25.36 ± 2.72 | 24.48 ± 2.85 * | 26.60 ± 2.93 | 26.03 ± 3.24 * |
| WC, cm | 83.95 ± 8.35 | 82.24 ± 7.54 ** | 84.26 ± 6.45 | 81.45 ± 5.78 * | 85.37 ± 8.12 | 82.69 ± 7.81 ** | 85.92 ± 7.79 | 79.34 ± 20.64 |
| BFP, % | 31.24 ± 5.42 | 30.11 ± 4.96 * | 32.28 ± 4.63 | 30.38 ± 4.89 * | 30.87 ± 5.37 | 28.66 ± 4.99 ** | 33.28 ± 5.05 | 31.31 ± 5.11 ** |
| VFA, cm2 | 98.72 ± 35.66 | 87.78 ± 33.37 ** | 104.47 ± 36.07 | 84.76 ± 31.59 * | 95.50 ± 30.15 | 80.28 ± 27.30 ** | 109.5 ± 34.77 | 93.75 ± 31.89 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Hu, Q.; Jiang, Q.; Jiang, J.; Li, B.; Ma, D. A Randomized Double-Blind Trial of the Effect of Liupao Tea on Metabolic Parameters, Body Composition, and Gut Microbiota in Adults with Metabolic Syndrome. Nutrients 2025, 17, 2371. https://doi.org/10.3390/nu17142371
Wang Y, Hu Q, Jiang Q, Jiang J, Li B, Ma D. A Randomized Double-Blind Trial of the Effect of Liupao Tea on Metabolic Parameters, Body Composition, and Gut Microbiota in Adults with Metabolic Syndrome. Nutrients. 2025; 17(14):2371. https://doi.org/10.3390/nu17142371
Chicago/Turabian StyleWang, Yuyang, Qiang Hu, Qiliu Jiang, Jiamin Jiang, Biandi Li, and Defu Ma. 2025. "A Randomized Double-Blind Trial of the Effect of Liupao Tea on Metabolic Parameters, Body Composition, and Gut Microbiota in Adults with Metabolic Syndrome" Nutrients 17, no. 14: 2371. https://doi.org/10.3390/nu17142371
APA StyleWang, Y., Hu, Q., Jiang, Q., Jiang, J., Li, B., & Ma, D. (2025). A Randomized Double-Blind Trial of the Effect of Liupao Tea on Metabolic Parameters, Body Composition, and Gut Microbiota in Adults with Metabolic Syndrome. Nutrients, 17(14), 2371. https://doi.org/10.3390/nu17142371