
Lifestyle and Perceived Well-Being in Children and Teens: Importance of Exercise and Sedentary Behavior

 , , , , and
, , , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Clinical Assessment
2.2. Lifestyle Assessment
- Nutrition was assessed using the American Heart Association (AHA) Healthy Diet Score [19], adapted to Italian eating habits [18], considering fruit/vegetables, fish, sweetened beverages, whole grains, and sodium consumption. The AHA score assumes integer values from 0 (“worst quality”) to 5 (“best quality”).
- Physical activity (total activity volume) was assessed by a modified version of the commonly employed short version of the International Physical Activity Questionnaire (IPAQ) [20,21], which focuses on intensity (nominally estimated in Metabolic Equivalents (METs) according to the type of activity) and duration (in minutes) of physical activity. We decided to employ this questionnaire (as in [20]), even if designed for adults, because it has the advantage of providing a numeric parameter of exercise volume (expressed in METs) that can reflect the total exercise volume. This study considered the following levels: activities of moderate intensity (≈4.0 METs/minute) and activities of vigorous intensity (≈8.0 METs/minute). These levels were used to calculate the total weekly exercise volume of structured exercise using the formula:where METsMV stands for moderate and vigorous (MV) physical activity volume expressed in METs minutes/week; M is the number of minutes/day of moderate-intensity activities performed in a number dM of days/week; V is the number of minutes/day of vigorous-intensity activities performed in a number dV of days/week.METsMV = 4 × M × dM + 8 × V × dV,
- The lifestyle questionnaire also inquired about the hours of sleep per night, the hours of sedentary behavior per week (considering the time spent in activities such as studying, reading, screen media use, and transportation), and the individual perception of the quality of sleep, health, and academic performance. These latter were assessed using ordinal evaluation scales ranging from 0 (“worst quality”) to 10 (“best quality”).
2.3. Statistical Analysis
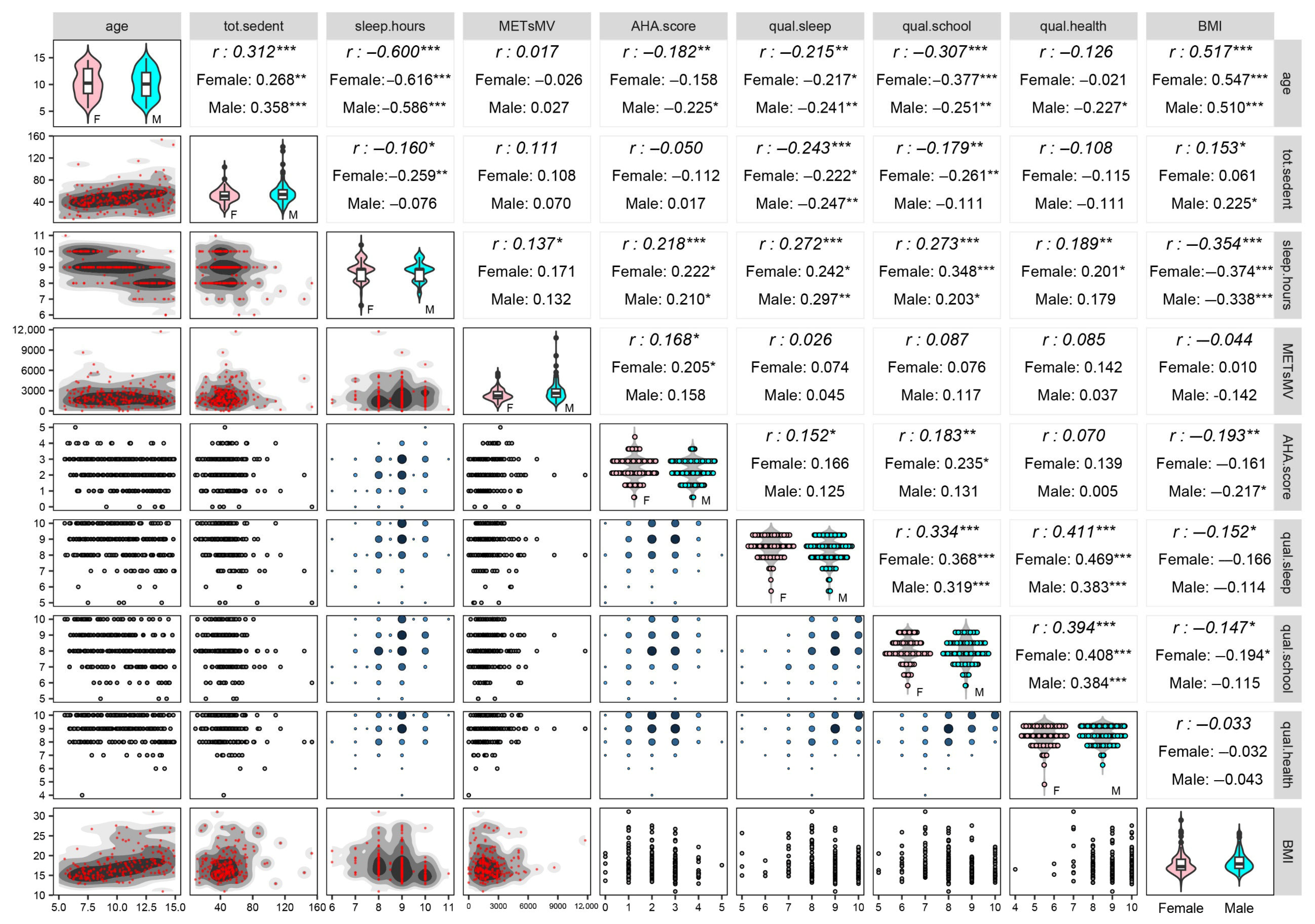
- Providing preliminary descriptive statistics and nonparametric significance tests [23]. Preliminarily, the sex-by-age-classes distribution of the 225 participants was inspected by testing the equality of age distribution between females and males (or, equivalently, the equality of sex distribution across age classes) through the Chi-square test (with a Monte Carlo (MC) procedure to obtain the p-value). Next, descriptive statistics of anthropometric, hemodynamic, and lifestyle variables and perceived quality scales were computed as median ± MAD (Median Absolute Deviation) both within sex and age classes and over all the participants. Then, we performed the two-tailed Kruskal–Wallis and median MC tests for each variable to evaluate the null hypothesis of the absence of differences between males and females and across age classes. Besides this, we constructed the correlogram of the ten variables we selected for their relevance to our investigation, i.e., sex (used as a stratification variable), age, BMI, lifestyle variables, and perceived quality scales (Appendix A Table A1). Spearman’s rank correlation coefficients were reported for every pair of variables on the upper triangular part of the correlogram, along with significance test results for uncorrelation concerning the whole set of 225 participants and the distinction between females and males. Moreover, on the correlogram diagonal, graphs displaying the univariate within-sex distributions were built for each variable, while in the lower triangular part, bivariate plots displaying the joint distributions of each pair of variables were built consistently with their measurement level.
- Setting up lifestyle indicators. We applied the nonlinear (or categorical) principal component analysis method, i.e., a nonlinear multivariate data analysis technique for dimensionality reduction, also known as PRINCALS [15], to account for the relationships among the four lifestyle variables, i.e., sedentary time, sleep hours, physical activity volume, and nutrition quality, and obtain a few standardized and uncorrelated dimensions, which we regarded as lifestyle statistical indicators. Unlike the standard principal component analysis, PRINCALS allows variables with different measurement levels to be jointly handled in a unique analysis through an optimal scaling procedure (Appendix A Table A1), through which qualitative variables are iteratively quantified during the extraction process of dimensions [15]. Component loadings (i.e., the correlation coefficients between the optimally scaled variables and the obtained PRINCALS dimensions) were rotated through the varimax method to simplify the interpretation of the dimensions. We used a threshold of 0.6 in absolute value on component loadings to identify the variables that more strongly contributed to the dimension construction and interpretation. We kept in analysis a number q of the first dimensions such that each explained at least 20% of the total variance of the optimally scaled variables and together accounted for a cumulative percentage of this variance of not less than 60%. To be used as lifestyle indicators, the retained dimensions were then checked to assume scores in a direction consistent with the meaning of the original lifestyle variables. Specifically, because the dimensions are zero-mean by construction, higher and positive dimension scores were supposed to represent children/teens with the healthiest lifestyles, while lower and negative scores had to indicate children/teens with the least healthy lifestyles.Lastly, we assessed the stability of the extracted dimensions by applying the nonparametric stratified balanced bootstrap [24]. In practice, B = 5000 bootstrap samples were generated at random so that each subject appeared exactly B times over the whole set of the nB = 225(5000) = 1,125,000 replicates (balanced bootstrap), and the same percentages of sex-by-age classes were reproduced in each sample (stratified bootstrap). The first q dimensions were extracted on each bootstrap sample with the component loadings rotated through the varimax method. Then, Procrustes rotations were employed to overcome the problem of configurations not aligned with the PRINCALS solution in the original dataset [25]. The stability of the indicators was subsequently assessed by computing 90% bootstrap confidence intervals (CIs) for the “Variance Accounted For” (VAF) measure and the component loadings using the bias-corrected and accelerated (BCa) method and the option “infinitesimal jackknife” [24].
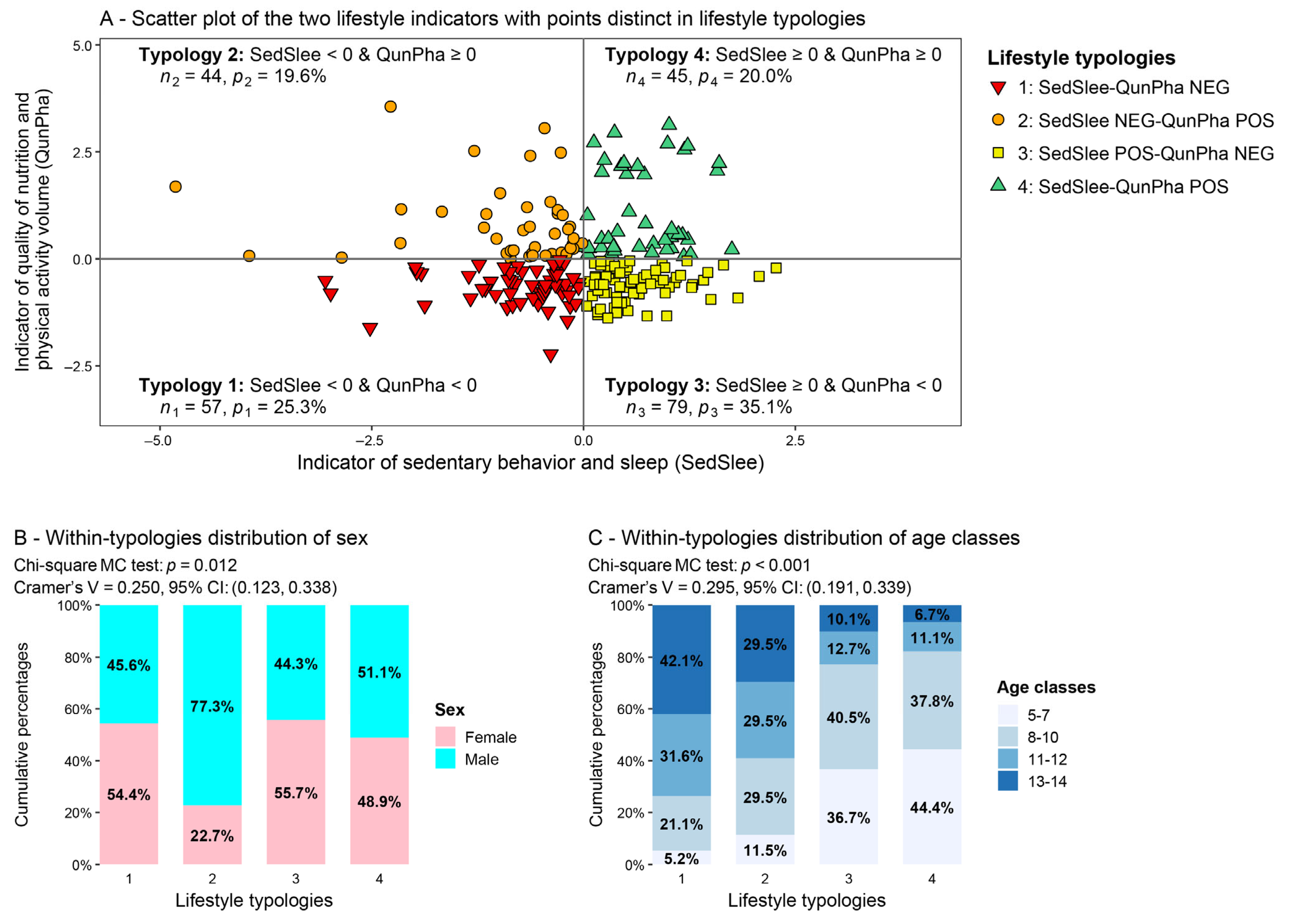
- Defining lifestyle typologies based on the obtained lifestyle indicators. We set up lifestyle typologies of children and teens by combining their negative or nonnegative (i.e., positive or equal to zero) scores on the lifestyle indicators. Nonnegative scores on all indicators characterized the healthiest lifestyle typology, while negative scores denoted the least healthy lifestyle typology; additionally, indicator scores with discordant signs defined intermediate typologies. Once the typologies were defined, we analyzed the sex and age classes composition of each of them to disclose any possible differences. In particular, we tested the equality of sex and age-class distributions across the typologies through the Chi-square MC test. Cramer’s V, along with 95% bootstrap CIs (built with the BCa method based on B = 1000 bootstrap samples), was also computed to provide a measure of the strength of association between lifestyle typologies and sex, and lifestyle typologies and age classes, respectively.
- Setting up perceived quality and BMI indicators and inspecting their distributions within the lifestyle typologies. Similarly to the construction of lifestyle indicators, we applied the PRINCALS method to account for the interrelationships among the three ordinal perceived quality scales and BMI (Appendix A Table A1) and set up standardized and uncorrelated dimensions. We applied the same approach described before for the lifestyle indicators to rotate the component loadings, choose the ideal number of dimensions to keep in analysis, assess the direction of dimension scores, and evaluate the stability of the VAF measure and component loadings through 90% bootstrap CIs. After that, to investigate whether different lifestyles affect perceived quality and BMI, we first depicted the score distributions of these indicators within the lifestyle typologies using violin plots (with box plots on their inside). Then, we tested the overall null hypothesis of no typology effects on them using the two-tailed Kruskal–Wallis and median MC tests, as well as the one-tailed Jonckheere–Terpstra permutation test, this latter having as the alternative hypothesis the progressive bettering of perceived quality and BMI with healthier lifestyles. In rejecting the overall null hypothesis, we deepened the analysis by comparing the distribution of the same indicator between every two typologies with the one-tailed Kolmogorov–Smirnov MC test and the Jonckheere–Terpstra permutation test. To preserve the nominal significance level of the overall null hypothesis, in these pairwise comparisons, we adjusted the p-values using the False Discovery Rate (FDR) method [26].
3. Results
3.1. Preliminary Descriptive Statistics and Nonparametric Significance Tests
3.2. Lifestyle Indicators
3.3. Lifestyle Typologies
3.4. Perceived Quality and BMI Indicators and Analysis Within the Lifestyle Typologies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHA | American Heart Association |
| BMI | Body Mass Index |
| CDC | Centers for Disease Control and Prevention |
| CNCD | Chronic Noncommunicable Diseases |
| DAP | Diastolic arterial pressure |
| ECG | Electrocardiogram |
| FDR | False Discovery Rate |
| IPAQ | International Physical Activity Questionnaire |
| IRCCS | Istituto di Ricovero e Cura a Carattere Scientifico (Scientific Institute for Research, Hospitalization and Healthcare) |
| MAD | Median Absolute Deviation |
| MC | Monte Carlo |
| METs | Metabolic Equivalents |
| METsMV | Moderate and Vigorous Physical Activity Volume Expressed in METs |
| NEG | Negative |
| POS | Positive |
| PRINCALS | Nonlinear (or categorical) Principal Component Analysis |
| QunPha | Indicator of the Quality of Nutrition and Physical Activity Volume |
| SAP | Systolic Arterial Pressure |
| SedSlee | Indicator of Sedentary Behavior and Sleep |
| VAF | Variance Accounted For |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| List of Variables and Their Description | Labels of Variables | Levels of Scaling of the Variables Involved in the PRINCALS Analysis |
|---|---|---|
| Sex. 0 = Female; 1 = Male. Sex distribution is in Appendix A Table A2 | sex | |
| Age in years. Distribution of age classes is in Appendix A Table A2 | age | |
| Anthropometric variables | ||
| Weight (in kg) | weight | |
| Height (in cm) | height | |
| Waist circumference (in cm) | WC | |
| Body mass index—BMI (in kg/m2) | BMI | metric |
| BMI in percentiles computed according to the guidelines in [16] | pct.BMI | |
| Hemodynamic variables | SAP | |
| Systolic arterial pressure (SAP) by sphygmomanometer (in mmHg) | DAP | |
| Diastolic arterial pressure (DAP) by sphygmomanometer (in mmHg) | pct.SAP | |
| SAP in percentiles computed according to the guidelines in [17] | pct.DAP | |
| DAP in percentiles computed according to the guidelines in [17] | SAP | |
| Lifestyle variables | ||
| Self-reported number of hours per week of sedentary time. Percentage distribution with values in intervals: [9, 36): 23.1%; [36, 50): 35.1%; [50, 65): 29.3%; [65, 154): 12.5% | tot.sedent | metric |
| Self-reported number of hours per night of sleep. Percentage distribution with values in intervals: [6, 8): 5.3%; [8, 9): 27.6%; [9, 10): 48.9%; [10, 11]: 18.2% | sleep.hours | metric |
| Metabolic Equivalents of moderate and vigorous physical activity per week. Percentage distribution with values in intervals: [0, 1200): 19.6%; [1200, 11,760]: 80.4% | METsMV | metric |
| American Heart Association Healthy Diet Score (in integer scores from 0 to 5). Percentage distribution: 0: 2.2%; 1: 18.7%; 2: 35.1%; 3: 36%; 4: 7.6%; 5: 0.4% | AHA.score | Ordinal 1—Merged scores: 0–1: 20.9%; 4–5: 8.0% |
| Perceived quality scales | ||
| Scale of perceived sleep quality (in integer scores from 0 to 10). Percentage distribution: 5: 1.8%; 6: 1.3%; 7: 8.0%; 8: 25.8%; 9: 36.0%; 10: 27.1% | qual.sleep | Ordinal 1—Merged scores: 5–7: 11.1% |
| Scale of perceived quality of academic performance (in integer scores from 0 to 10). Percentage distribution: 5: 1.3%; 6: 6.2%; 7: 15.6%; 8: 34.7%; 9: 26.2%; 10: 16.0% | qual.school | Ordinal 1—Merged scores: 5–6: 7.5% |
| Scale of perceived quality of overall health (in integer scores from 0 to 10). Percentage distribution: 4: 0.4%; 6: 0.9%; 7: 4.0%; 8: 23.6%; 9: 36.0%; 10: 35.1% | qual.health | Ordinal 1—Merged scores: 4–7: 5.3% |
| Age Classes (in Years Old) | |||||||
|---|---|---|---|---|---|---|---|
| 5–7 | 8–10 | 11–12 | 13–14 | Total | |||
| Sex | Female | N | 25 | 38 | 17 | 27 | 107 |
| % within sex | 23.4% | 35.5% | 15.9% | 25.2% | 100.0% | ||
| % within age class | 43.9% | 51.4% | 37.0% | 56.3% | 47.6% | ||
| Male | N | 32 | 36 | 29 | 21 | 118 | |
| % within sex | 27.1% | 30.5% | 24.6% | 17.8% | 100.0% | ||
| % within age class | 56.1% | 48.6% | 63.0% | 43.8% | 52.4% | ||
| Total | N | 57 | 74 | 46 | 48 | 225 | |
| % within age class | 25.3% | 32.9% | 20.4% | 21.3% | 100.0% | ||
| 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | |||
References
- Turco, J.V.; Inal-Veith, A.; Fuster, V. Cardiovascular Health Promotion: An Issue That Can No Longer Wait. J. Am. Coll. Cardiol. 2018, 72, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Wang, N.; Ware, R.S.; Sha, Y.; Xu, F. Lifestyle-related Behaviors and Health-related Quality of Life Among Children and Adolescents in China. Health Qual. Life Outcomes 2021, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Isma, G.E.; Rämgård, M.; Enskär, K. Perceptions of Health Among School-aged Children Living in Socially Vulnerable Areas in Sweden. Front. Public Health 2023, 11, 1136832. [Google Scholar] [CrossRef] [PubMed]
- Yandrapalli, S.; Nabors, C.; Goyal, A.; Aronow, W.S.; Frishman, W.H. Modifiable Risk Factors in Young Adults with First Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 573–584. [Google Scholar] [CrossRef]
- Herbert, C. Enhancing Mental Health, Well-being and Active Lifestyles of University Students by means of Physical Activity and Exercise Research Programs. Front. Public Health 2022, 10, 849093. [Google Scholar] [CrossRef]
- Sabolova, K.; Birdsey, N.; Stuart-Hamilton, I.; Cousins, A.L. A Cross-cultural Exploration of Children’s Perceptions of Well-being: Understanding Protective and Risk Factors. Child. Youth Serv. Rev. 2020, 110, 10477. [Google Scholar] [CrossRef]
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5–17 Years: Summary of the Evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)–Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef]
- Curran, F.; Blake, C.; Cunningham, C.; Perrotta, C.; van der Ploeg, H.; Matthews, J.; O’Donoghue, G. Efficacy, Characteristics, Behavioural Models and Behaviour Change Strategies, of Non-workplace Interventions Specifically Targeting Sedentary Behaviour; A Systematic Review and Meta-analysis of Randomised Control Trials in Healthy Ambulatory Adults. PLoS ONE 2021, 16, e0256828. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Lancet Physical Activity Series 2 Executive Committee; Lancet Sedentary Behaviour Working Group. Does Physical Activity Attenuate, or Even Eliminate, the Detrimental Association of Sitting Time with Mortality? A Harmonised Meta-analysis of Data from More Than 1 Million Men and Women. Lancet 2016, 388, 1302–1310. [Google Scholar]
- Stenlund, S.; Koivumaa-Honkanen, H.; Sillanmäki, L.; Lagström, H.; Rautava, P.; Suominen, S. Changed Health Behavior Improves Subjective Well-being and Vice Versa in a Follow-up of 9 Years. Health Qual. Life Outcomes 2022, 20, 66. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling Health Behaviour Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar]
- Davidson, K.W.; Scholz, U. Understanding and Predicting Health Behaviour Change: A Contemporary View through the Lenses of Meta-reviews. Health Psychol. Rev. 2020, 14, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. Circulation 2019, 140, 596–646. [Google Scholar] [CrossRef] [PubMed]
- Gifi, A. Nonlinear Multivariate Analysis; Wiley: Chichester, UK, 1990. [Google Scholar]
- CDC (Centers for Disease Control and Prevention). BMI Percentile Calculator for Child and Teen. 2023. Available online: https://www.cdc.gov/bmi/child-teen-calculator/index.html (accessed on 13 July 2025).
- USDA/ARS Children’s Nutrition Research Center, Baylor College of Medicine. Age-Based Pediatric Blood Pressure Reference Charts. 2024. Available online: https://www.bcm.edu/bodycomplab/BPappZjs/BPvAgeAPPz.html (accessed on 11 January 2024).
- Lucini, D.; Zanuso, S.; Blair, S.; Pagani, M. A Simple Healthy Lifestyle Index as a Proxy of Wellness: A Proof of Concept. Acta Diabetol. 2015, 52, 81–89. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. American Heart Association Strategic Planning Task Force and Statistics Committee. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef]
- Calcaterra, V.; Bernardelli, G.; Malacarne, M.; Vandoni, M.; Mannarino, S.; Pellino, V.C.; Larizza, C.; Pagani, M.; Zuccotti, G.; Lucini, D. Effects of Endurance Exercise Intensities on Autonomic and Metabolic Controls in Children with Obesity: A Feasibility Study Employing Online Exercise Training. Nutrients 2023, 15, 1054. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Giussani, M.; Antolini, L.; Brambilla, P.; Pagani, M.; Zuccotti, G.; Lucini, D.; Genovesi, S. Cardiovascular Risk Assessment in Children: Role of Physical Activity, Family History and Parental Smoking on Body Mass Index and Blood Pressure. J. Hypertens. 2013, 31, 983–992. [Google Scholar] [CrossRef]
- Hollander, M.; Wolfe, D.A.; Chicken, E. Nonparametric Statistical Methods, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Davison, A.C.; Hinkley, D.V. Bootstrap Methods and Their Applications; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Linting, M.; Meulman, J.J.; Groenen, P.J.F.; van der Kooij, A.J. Stability of Nonlinear Principal Components Analysis: An Empirical Study Using the Balanced Bootstrap. Psychol. Methods 2007, 12, 359–379. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Koenker, R. Quantile Regression; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Koenker, R.; Machado, J.A.F. Goodness of Fit and Related Inference Processes for Quantile Regression. J. Am. Stat. Assoc. 1999, 94, 1296–1310. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://www.r-project.org/ (accessed on 5 November 2024).
- Canty, A.; Ripley, B. boot: Bootstrap R (S-Plus) Functions; R Package Version 11.3-30. 2024. Available online: https://CRAN.R-project.org/package=boot (accessed on 17 June 2025).
- Hothorn, T.; Hornik, K.; van de Wiel, M.A.; Zeileis, A. Implementing a Class of Permutation Tests: The coin Package. J. Stat. Softw. 2008, 28, 1–23. [Google Scholar] [CrossRef]
- Signorell, A. DescTools: Tools for Descriptive Statistics; R Package Version 0.99.54. 2024. Available online: https://CRAN.R-project.org/package=DescTools (accessed on 17 June 2025).
- Mair, P.; De Leeuw, J. Gifi: Multivariate Analysis with Optimal Scaling; R Package Version 0.4-0. 2022. Available online: https://CRAN.R-project.org/package=Gifi (accessed on 17 June 2025).
- Schloerke, B.; Cook, D.; Larmarange, J.; Briatte, F.; Marbach, M.; Thoen, E.; Elberg, A.; Crowley, J. GGally: Extension to “ggplot2”; R Package Version 2.2.0. 2023. Available online: https://CRAN.R-project.org/package=GGally (accessed on 17 June 2025).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Springer: New York, NY, USA, 2016. [Google Scholar]
- Koenker, R. quantreg: Quantile Regression; R Package Version 6.1. 2025. Available online: https://CRAN.R-project.org/package=quantreg (accessed on 11 July 2025).
- Long, J.A. jtools: Analysis and Presentation of Social Scientific Data; R Package Version 2.2.0. 2022. Available online: https://cran.r-project.org/package=jtools (accessed on 11 July 2025).
- Mangiafico, S.S. rcompanion: Functions to Support Extension Education Program Evaluation; R Package Version 2.5.0. 2025. Available online: https://CRAN.R-project.org/package=rcompanion (accessed on 11 July 2025).
- Baker-Smith, C.M.; Flynn, J.T. 2023 European Pediatric Hypertension Guidelines: Has Anything Changed? Nephrol. Dial. Transpl. 2023, 39, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Bahls, M.; Groß, S. The Complexities of Modeling Lifetime Risk in the General Population. Eur. J. Prev. Cardiol. 2024, 31, 1700–1701. [Google Scholar] [CrossRef]
- Holtrop, J.; Bhatt, D.L.; Ray, K.K.; Mach, F.; Smulders, Y.M.; Carballo, D.; Steg, P.G.; Visseren, F.L.J.; Dorresteijn, J.A.N. Impact of the 2021 European Society for Cardiology Prevention Guideline’s Stepwise Approach for Cardiovascular Risk Factor Treatment in Patients with Established Atherosclerotic Cardiovascular Disease. Eur. J. Prev. Cardiol. 2024, 31, 754–762. [Google Scholar] [CrossRef]
- Matheson, G.O.; Witteman, H.O.; Mochar, T.G. Disease Prevention: What’s Really Important? Br. J. Sports Med. 2015, 49, 1483–1484. [Google Scholar] [CrossRef]
- Hancox, R.J.; Milne, B.J.; Poulton, R. Association between Child and Adolescent Television Viewing and Adult Health: A Longitudinal Birth Cohort Study. Lancet 2004, 364, 257–262. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, E.; Capria, F.; Galiano, M.; Marchese, M.; Cribellati, S.; Parati, G. Age Influences on Lifestyle and Stress Perception in the Working Population. Nutrients 2023, 15, 399. [Google Scholar] [CrossRef]
- Cárdenas, D.; Lattimore, F.; Steinberg, D.; Reynolds, K.J. Youth Well-being Predicts Later Academic Success. Sci. Rep. 2022, 12, 2134. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, E.; Capria, F.; Galliano, M.; Marchese, M.; Cribellati, S. Evidence of Better Psychological Profile in Working Population Meeting Current Physical Activity Recommendations. Int. J. Environ. Res. Public Health 2021, 18, 8991. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response Associations between Accelerometry Measured Physical Activity and Sedentary Time and All Cause Mortality: Systematic Review and Harmonised Meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]
- Piko, B.F.; Bak, J. Children’s Perceptions of Health and Illness: Images and Lay Concepts in Preadolescence. Health Educ. Res. 2006, 21, 643–653. [Google Scholar] [CrossRef]
- Chanfreau, J.; Lloyd, C.; Byron, C.; Roberts, C.; Craig, R.; De Feo, D.; McManus, S. Predicting Wellbeing; NatCen Social Research: London, UK, 2014; Available online: https://www.researchgate.net/publication/266302779_Predicting_wellbeing (accessed on 17 June 2025).
- Sharma, H. How Short or Long Should Be a Questionnaire for Any Research? Researchers Dilemma in Deciding the Appropriate Questionnaire Length. Saudi J. Anaesth. 2022, 16, 65–68. [Google Scholar] [CrossRef]
- Kost, R.G.; de Rosa, J.C. Impact of Survey Length and Compensation on Validity, Reliability, and Sample Characteristics for Ultrashort-, Short-, and Long-Research Participant Perception Surveys. J. Clin. Transl. Sci. 2018, 2, 31–37. [Google Scholar] [CrossRef]
- Mei, Z.; Grummer-Strawn, L.M. Standard Deviation of Anthropometric Z-scores as a Data Quality Assessment Tool Using the 2006 WHO Growth Standards: A Cross Country Analysis. B World Health Organ. 2007, 85, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2016 Update: A Report from the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [PubMed]
- Martin, S.S.; Aday, A.W.; Allen, N.B.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Bansal, N.; Beaton, A.Z.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Committee. 2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation 2025, 151, e41–e660. [Google Scholar] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]

| Variables | Female | Male | All |
|---|---|---|---|
| Age (years) | 10.25 ± 2.50 | 10.08 ± 2.17 | 10.25 ± 2.33 |
| Anthropometrics and hemodynamics | |||
| Weight (kg) | 32.30 ± 7.60 | 35.25 ± 9.60 | 34.40 ± 8.40 |
| Height (cm) | 140.00 ± 12.00 | 143.75 ± 12.00 | 143.00 ± 12.50 |
| Waist circumference (cm) **,†† | 61.00 ± 5.00 | 65.00 ± 6.00 | 63.00 ± 6.00 |
| Body Mass Index—BMI (kg/m2) † | 16.18 ± 1.79 | 17.05 ± 1.67 | 16.60 ± 1.68 |
| BMI percentiles * | 43.00 ± 27.00 | 55.50 ± 24.50 | 48.00 ± 27.00 |
| Systolic arterial pressure—SAP (mmHg) **,†† | 100.00 ± 10.00 | 110.00 ± 7.50 | 105.00 ± 5.00 |
| Diastolic arterial pressure—DAP (mmHg) | 60.00 ± 5.00 | 65.00 ± 5.00 | 62.00 ± 3.00 |
| SAP percentiles * | 61.00 ± 25.00 | 74.50 ± 17.50 | 65.00 ± 23.00 |
| DAP percentiles * | 53.00 ± 18.00 | 65.00 ± 20.00 | 59.00 ± 18.00 |
| Lifestyle variables | |||
| Hours/week of sedentary behavior | 44.00 ± 9.00 | 47.50 ± 10.50 | 46.00 ± 9.60 |
| Hours/night of sleep | 9.00 ± 1.00 | 9.00 ± 0.25 | 9.00 ± 0.50 |
| Volume of moderate and vigorous physical activity (METs, minutes/week) **,† | 1680.00 ± 480.00 | 2120.00 ± 760.00 | 1840.00 ± 720.00 |
| American Heart Association Healthy Diet Score | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 |
| Perceived quality scales | |||
| Sleep | 9.00 ± 1.00 | 9.00 ± 1.00 | 9.00 ± 1.00 |
| Academic performance | 8.00 ± 1.00 | 8.00 ± 1.00 | 8.00 ± 1.00 |
| Health | 9.00 ± 1.00 | 9.00 ± 1.00 | 9.00 ± 1.00 |
| Variables | 5–7 Years | 8–10 Years | 11–12 Years | 13–14 Years |
|---|---|---|---|---|
| Anthropometrics and hemodynamics | ||||
| Weight (kg) ***,††† | 24.20 ± 2.30 | 30.85 ± 4.20 | 41.95 ± 4.95 | 50.55 ± 4.95 |
| Height (cm) ***,††† | 125.00 ± 4.00 | 137.75 ± 5.75 | 151.50 ± 4.00 | 166.00 ± 5.25 |
| Waist circumference (cm) ***,††† | 57.00 ± 3.00 | 61.00 ± 5.00 | 66.50 ± 3.50 | 70.00 ± 4.50 |
| Body Mass Index—BMI (kg/m2) ***,††† | 15.32 ± 0.86 | 16.41 ± 1.43 | 17.97 ± 1.66 | 18.77 ± 1.90 |
| BMI percentiles | 43.00 ± 22.00 | 46.50 ± 23.00 | 54.50 ± 30.50 | 53.50 ± 28.50 |
| Systolic arterial pressure—SAP (mmHg) ***,††† | 100.00 ± 5.00 | 110.00 ± 5.00 | 105.00 ± 10.00 | 110.00 ± 10.00 |
| Diastolic arterial pressure—DAP (mmHg) | 62.00 ± 3.00 | 65.00 ± 5.00 | 60.00 ± 1.50 | 60.00 ± 2.50 |
| SAP percentiles ***,††† | 67.00 ± 12.00 | 83.50 ± 8.50 | 63.50 ± 29.50 | 39.50 ± 21.00 |
| DAP percentiles ***,††† | 71.00 ± 15.00 | 68.00 ± 18.00 | 45.00 ± 9.50 | 39.50 ± 13.50 |
| Lifestyle variables | ||||
| Hours/week of sedentary behavior ***,††† | 38.50 ± 7.00 | 47.00 ± 6.45 | 52.25 ± 12.50 | 54.25 ± 10.75 |
| Hours/night of sleep ***,††† | 9.00 ± 1.00 | 9.00 ± 0.00 | 8.50 ± 0.50 | 8.00 ± 0.00 |
| Volume of moderate and vigorous physical activity (METs, minutes/week) | 1920.00 ± 720.00 | 1740.00 ± 660.00 | 1780.00 ± 820.00 | 1920.00 ± 720.00 |
| American Heart Association Healthy Diet Score * | 3.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 | 2.00 ± 1.00 |
| Perceived quality scales | ||||
| Sleep * | 9.00 ± 1.00 | 9.00 ± 1.00 | 9.00 ± 1.00 | 8.50 ± 0.50 |
| Academic performance ***,††† | 9.00 ± 1.00 | 9.00 ± 1.00 | 8.00 ± 1.00 | 8.00 ± 1.00 |
| Health | 9.00 ± 1.00 | 9.00 ± 1.00 | 9.00 ± 1.00 | 9.00 ± 1.00 |
| Dimension 1 | Dimension 2 | |||||
|---|---|---|---|---|---|---|
| Variables | Loadings 1 | 90% Bootstrap CIs 2 | Loadings 1 | 90% Bootstrap CIs 2 | ||
| Hours/week of sedentary time | −0.773 • | −0.844 | −0.656 | 0.292 | 0.010 | 0.501 |
| Hours/night of sleep | 0.752 • | 0.647 | 0.826 | 0.351 | 0.161 | 0.489 |
| AHA score | 0.224 | −0.039 | 0.519 | 0.740 • | 0.384 | 0.840 |
| METs of moderate and vigorous physical activity | −0.201 | −0.381 | 0.216 | 0.678 • | 0.417 | 0.860 |
| Variance Accounted For—VAF (%) | 32.63% | 31.43% | 37.69% | 29.12% | 25.53% | 31.34% |
| Cumulative VAF (%) | 32.63% | 31.43% | 37.69% | 61.75% | 59.46% | 66.33% |
| Dimension 1 | Dimension 2 | |||||
|---|---|---|---|---|---|---|
| Variables | Loadings 1 | 90% Bootstrap CIs 2 | Loadings 1 | 90% Bootstrap CIs 2 | ||
| Perceived health quality | 0.808 ▲ | 0.716 | 0.849 | 0.103 | −0.169 | 0.342 |
| Perceived academic performance quality | 0.756 ▲ | 0.629 | 0.806 | −0.151 | −0.390 | 0.030 |
| Perceived sleep quality | 0.748 ▲ | 0.572 | 0.813 | −0.193 | −0.497 | 0.033 |
| BMI | −0.087 | −0.225 | −0.019 | 0.981 ▲ | 0.953 | 0.999 |
| Variance Accounted For—VAF (%) | 46.82% | 43.25% | 51.94% | 23.79% | 22.08% | 26.76% |
| Cumulative VAF (%) | 46.82% | 43.25% | 51.94% | 70.62% | 68.41% | 75.32% |
| 1st Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | −1.225 | (−1.721, −0.729) | −4.867 | <0.001 | −1.013 | (−1.516, −0.509) | −1.519 | <0.001 |
| Typology 2 | 0.528 | (−0.160, 1.215) | 1.513 | 0.132 | 0.572 | (−0.107, 1.251) | 1.652 | 0.098 |
| Typology 3 | 0.723 | (0.129, 1.317) | 2.400 | 0.017 | 0.672 | (0.036, 1.308) | 2.077 | 0.038 |
| Typology 4 | 1.091 | (0.397, 1.785) | 3.096 | 0.002 | 0.902 | (0.231, 1.572) | 2.645 | 0.009 |
| sex | −0.193 | (−0.666, 0.280) | 0.974 | 0.423 | ||||
| age | 0.014 | (−0.264, 0.292) | 0.100 | 0.920 | ||||
| sex-by-age | −0.252 | (−0.650, 0.145) | −1.250 | 0.213 | ||||
| 2nd Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | −0.200 | (−0.591, 0.190) | −1.012 | 0.313 | −0.188 | (−0.581, 0.205) | −0.941 | 0.348 |
| Typology 2 | 0.135 | (−0.285, 0.556) | 0.634 | 0.527 | 0.146 | (−0.399, 0.691) | 0.528 | 0.598 |
| Typology 3 | 0.458 | (−0.011, 0.927) | 1.925 | 0.056 | 0.455 | (−0.049, 0.959) | 1.779 | 0.077 |
| Typology 4 | 0.484 | (−0.007, 0.975) | 1.942 | 0.053 | 0.475 | (−0.103, 1.052) | 1.620 | 0.107 |
| sex | −0.031 | (−0.442, 0.380) | −0.150 | 0.881 | ||||
| age | 0.008 | (−0.256, 0.273) | 0.063 | 0.950 | ||||
| sex-by-age | −0.135 | (−0.537, 0.266) | −0.665 | 0.507 | ||||
| 3rd Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age 0.084 | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | 0.208 | (−0.166, 0.583) | 1.095 | 0.275 | 0.353 | (−0.174, 0.880) | 1.320 | 0.188 |
| Typology 2 | 0.261 | (−0.264, 0.785) | 0.980 | 0.328 | 0.250 | (−0.315, 0.815) | 0.871 | 0.385 |
| Typology 3 | 0.682 | (0.147, 1.216) | 2.513 | 0.013 | 0.595 | (0.061, 1.130) | 2.194 | 0.029 |
| Typology 4 | 0.955 | (0.401, 1.509) | 3.399 | <0.001 | 0.718 | (0.025, 1.411) | 2.043 | 0.042 |
| sex | −0.176 | (−0.511, 0.159) | −1.036 | 0.301 | ||||
| age | −0.264 | (−0.487, −0.041) | −2.336 | 0.020 | ||||
| sex-by-age | 0.071 | (−0.321, 0.464) | 0.358 | 0.721 | ||||
| 1st Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | −0.466 | (−0.818, −0.114) | −2.608 | 0.010 | −0.572 | (−0.853, −0.291) | −4.008 | <0.001 |
| Typology 2 | −0.117 | (−0.513, 0.279) | −0.582 | 0.561 | −0.205 | (−0.567, 0.157) | −1.119 | 0.265 |
| Typology 3 | −0.237 | (−0.621, 0.146) | −1.220 | 0.224 | −0.099 | (−0.419, 0.220) | −0.613 | 0.541 |
| Typology 4 | −0.399 | (−0.812, 0.015) | −1.899 | 0.059 | −0.119 | (−0.475, 0.236) | −0.662 | 0.509 |
| sex | 0.175 | (−0.041, 0.390) | 1.598 | 0.112 | ||||
| age | 0.339 | (0.187, 0.492) | 4.395 | <0.001 | ||||
| sex-by-age | −0.114 | (−0.344, 0.116) | −0.975 | 0.331 | ||||
| 2nd Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | −0.041 | (−0.323, 0.240) | −0.290 | 0.772 | −0.345 | (−0.609, −0.081) | −2.578 | 0.011 |
| Typology 2 | −0.061 | (−0.502, 0.381) | −0.270 | 0.787 | 0.110 | (−0.348, 0.568) | 0.474 | 0.636 |
| Typology 3 | −0.302 | (−0.641, 0.038) | −1.753 | 0.081 | 0.122 | (−0.243, 0.486) | 0.658 | 0.511 |
| Typology 4 | −0.423 | (−0.762, −0.084) | −2.461 | 0.015 | 0.118 | (−0.276, 0.511) | 0.589 | 0.557 |
| sex | 0.210 | (−0.082, 0.501) | 1.416 | 0.158 | ||||
| age | 0.463 | (0.279, 0.647) | 4.957 | <0.001 | ||||
| sex-by-age | −0.112 | (−0.383, 0.159) | −0.816 | 0.416 | ||||
| 3rd Quartile () | ||||||||
| No adjustment for sex and age | Adjusting for sex and age | |||||||
| Variables | Stand.est. | 95% CIs | t Value | p-Value | Stand.est. | 95% CIs | t Value | p-Value |
| Intercept | 0.843 | (0.389, 1.296) | 3.664 | <0.001 | 0.376 | (−0.223, 0.975) | 1.236 | 0.218 |
| Typology 2 | −0.281 | (−1.045, 0.483) | −0.724 | 0.470 | −0.312 | (−0.959, 0.336) | −0.948 | 0.344 |
| Typology 3 | −0.516 | (−1.032, −0.001) | −1.974 | 0.050 | −0.122 | (−0.790, 0.547) | −0.359 | 0.720 |
| Typology 4 | −0.921 | (−1.481, −0.362) | −3.245 | 0.001 | −0.192 | (−0.914, 0.529) | −0.525 | 0.600 |
| sex | 0.218 | (−0.165, 0.601) | 1.120 | 0.264 | ||||
| age | 0.536 | (0.248, 0.824) | 3.670 | <0.001 | ||||
| sex-by-age | 0.011 | (−0.355, 0.377) | 0.059 | 0.953 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solaro, N.; Oggionni, G.; Bernardelli, G.; Malacarne, M.; Pagani, E.; Ferrari, M.; Parati, G.; Lucini, D. Lifestyle and Perceived Well-Being in Children and Teens: Importance of Exercise and Sedentary Behavior. Nutrients 2025, 17, 2370. https://doi.org/10.3390/nu17142370
Solaro N, Oggionni G, Bernardelli G, Malacarne M, Pagani E, Ferrari M, Parati G, Lucini D. Lifestyle and Perceived Well-Being in Children and Teens: Importance of Exercise and Sedentary Behavior. Nutrients. 2025; 17(14):2370. https://doi.org/10.3390/nu17142370
Chicago/Turabian StyleSolaro, Nadia, Gianluigi Oggionni, Giuseppina Bernardelli, Mara Malacarne, Eleonora Pagani, Mariacarla Ferrari, Gianfranco Parati, and Daniela Lucini. 2025. "Lifestyle and Perceived Well-Being in Children and Teens: Importance of Exercise and Sedentary Behavior" Nutrients 17, no. 14: 2370. https://doi.org/10.3390/nu17142370
APA StyleSolaro, N., Oggionni, G., Bernardelli, G., Malacarne, M., Pagani, E., Ferrari, M., Parati, G., & Lucini, D. (2025). Lifestyle and Perceived Well-Being in Children and Teens: Importance of Exercise and Sedentary Behavior. Nutrients, 17(14), 2370. https://doi.org/10.3390/nu17142370