
Exercise and Nutrition for Sarcopenia: A Systematic Review and Meta-Analysis with Subgroup Analysis by Population Characteristics


Abstract
1. Introduction
2. Materials and Methods
2.1. Protocols and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Screening Criteria for Studies
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Data Synthesis and Analysis
3. Results
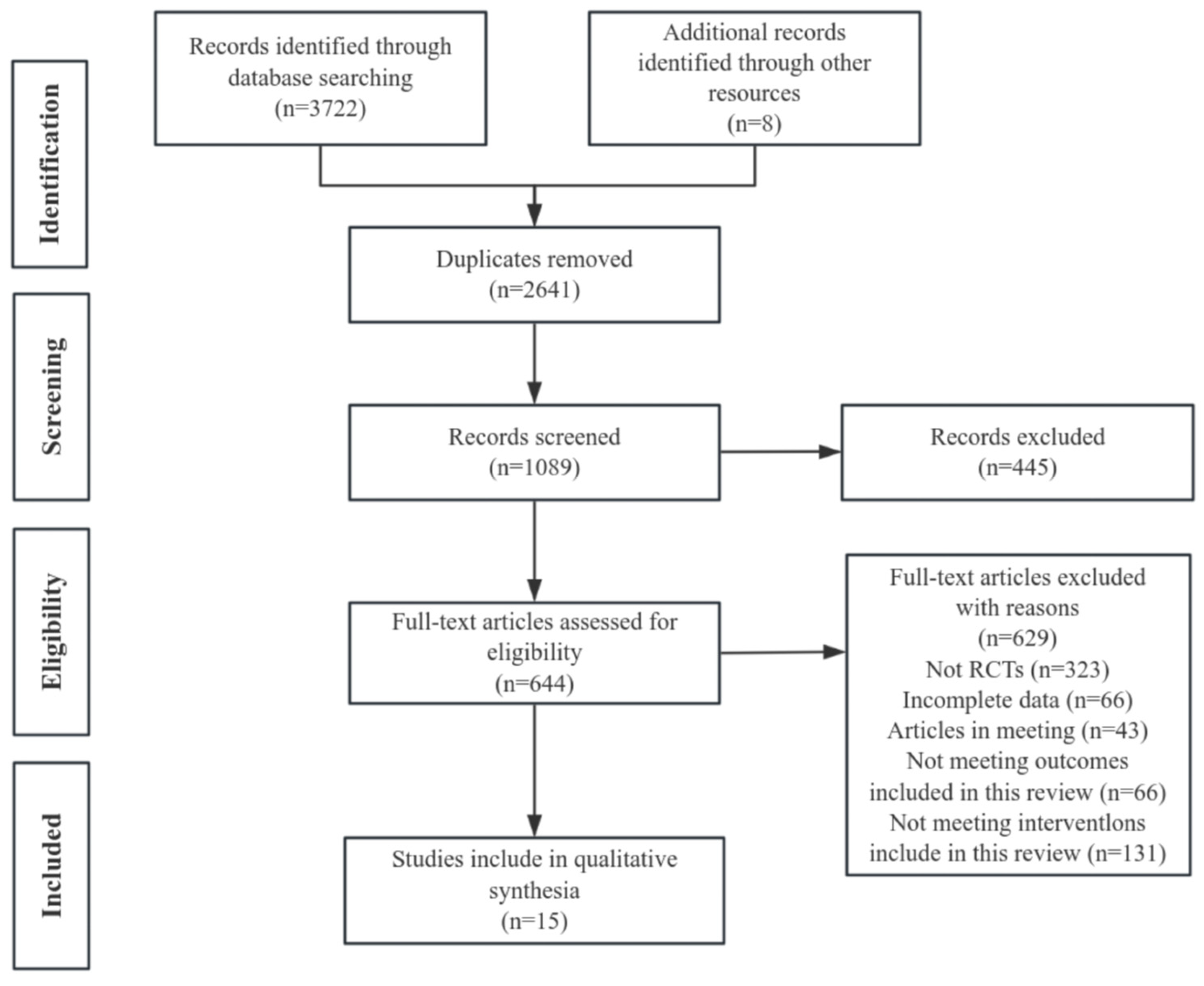
3.1. Study Selection
3.2. Study Characteristics
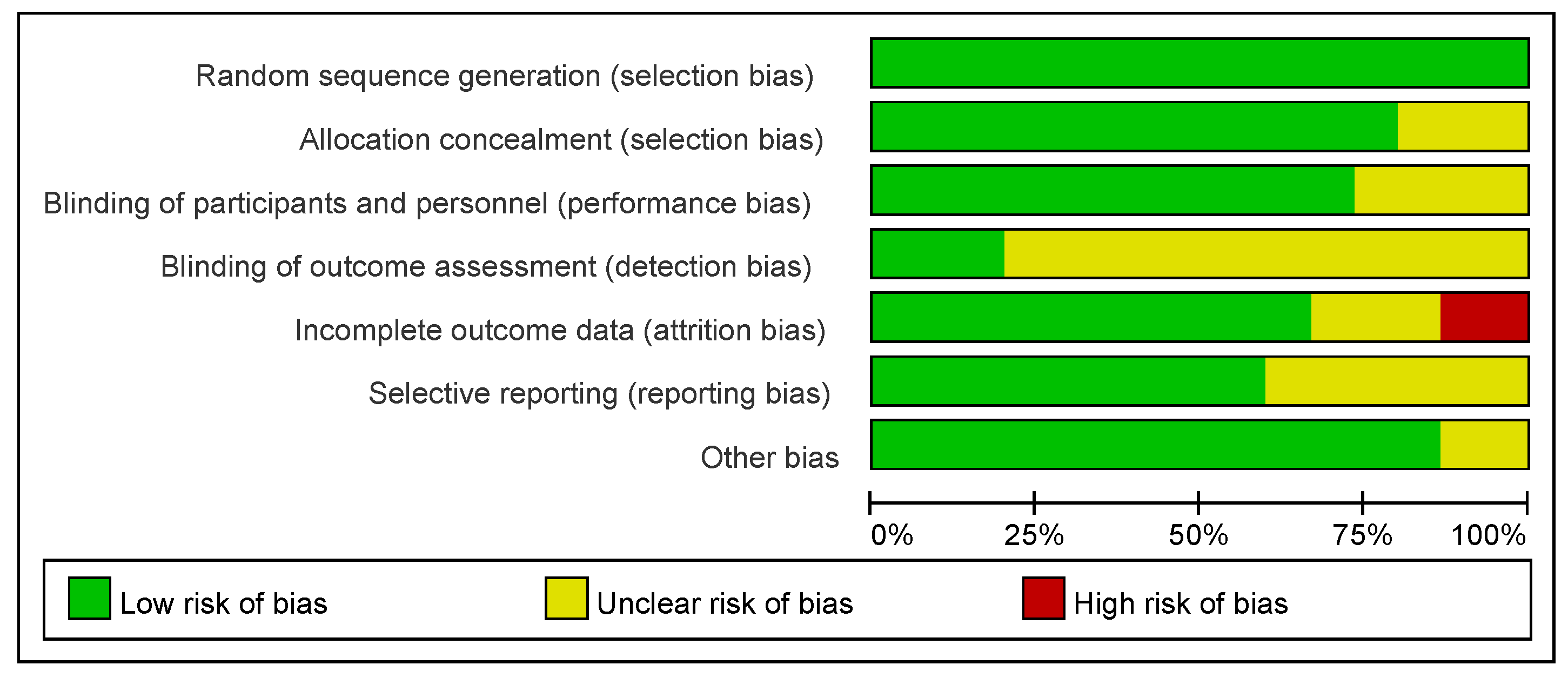
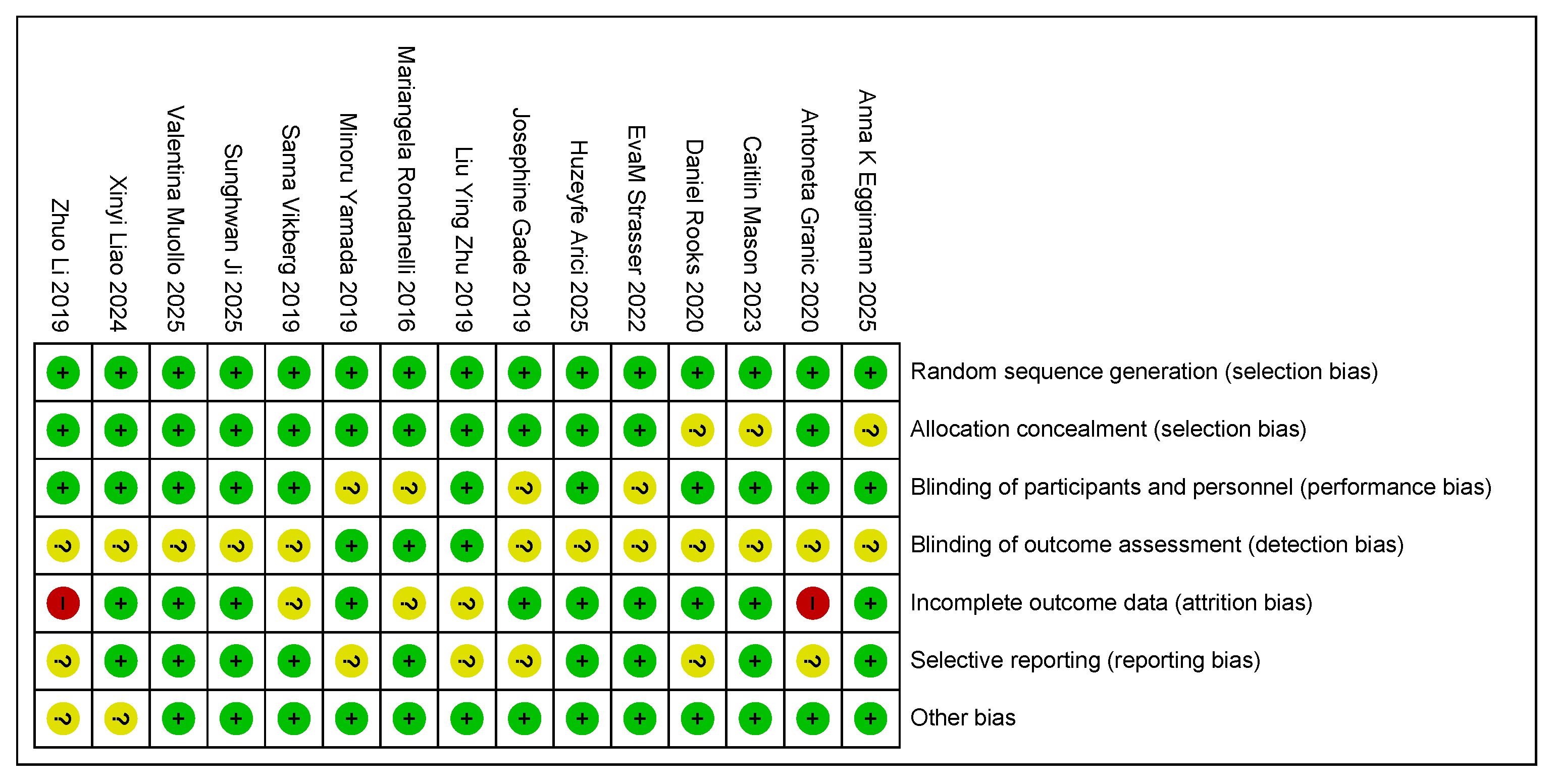
3.3. Risk of Bias
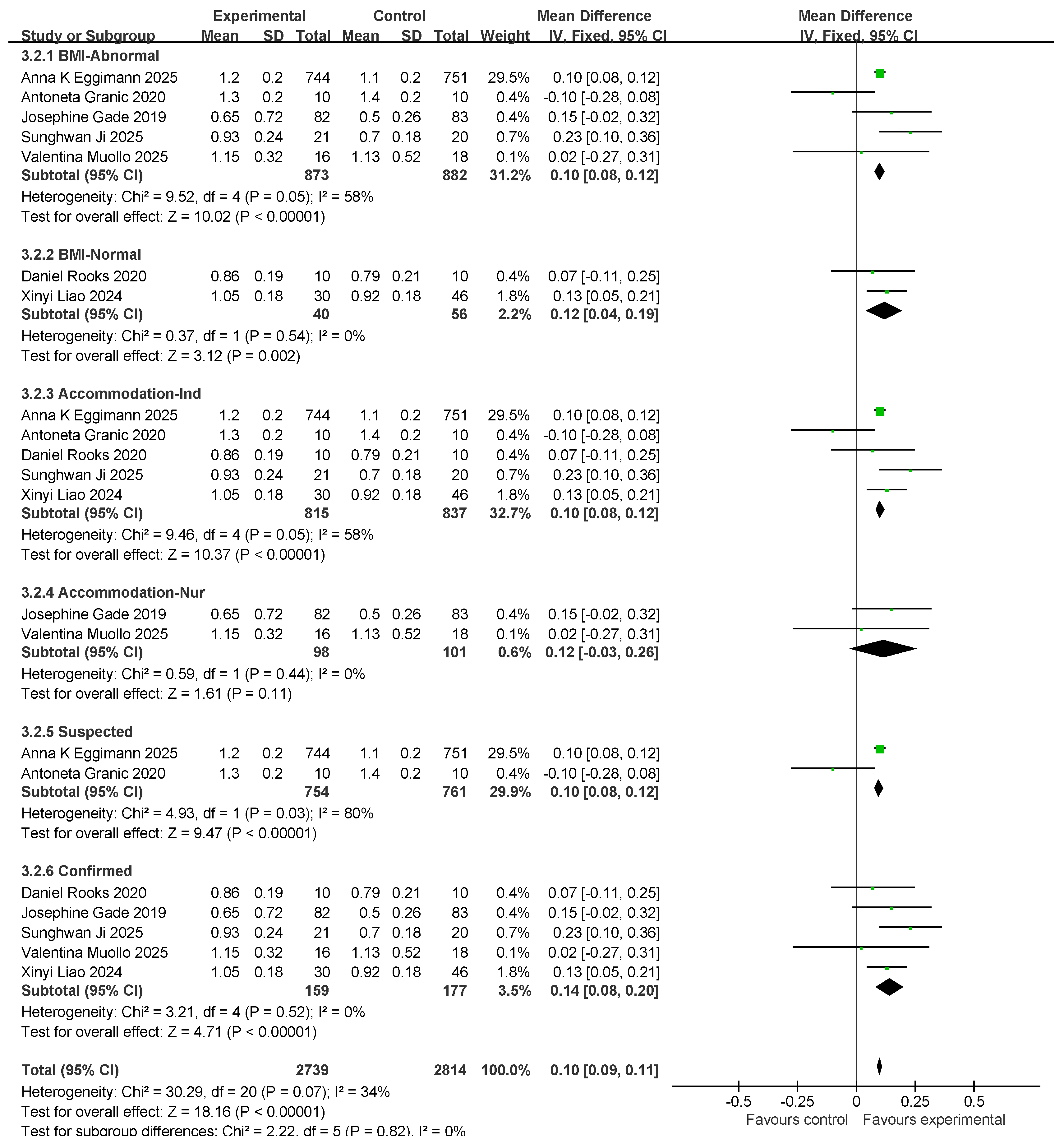
3.4. Grip Strength Results and Subgroup Analysis
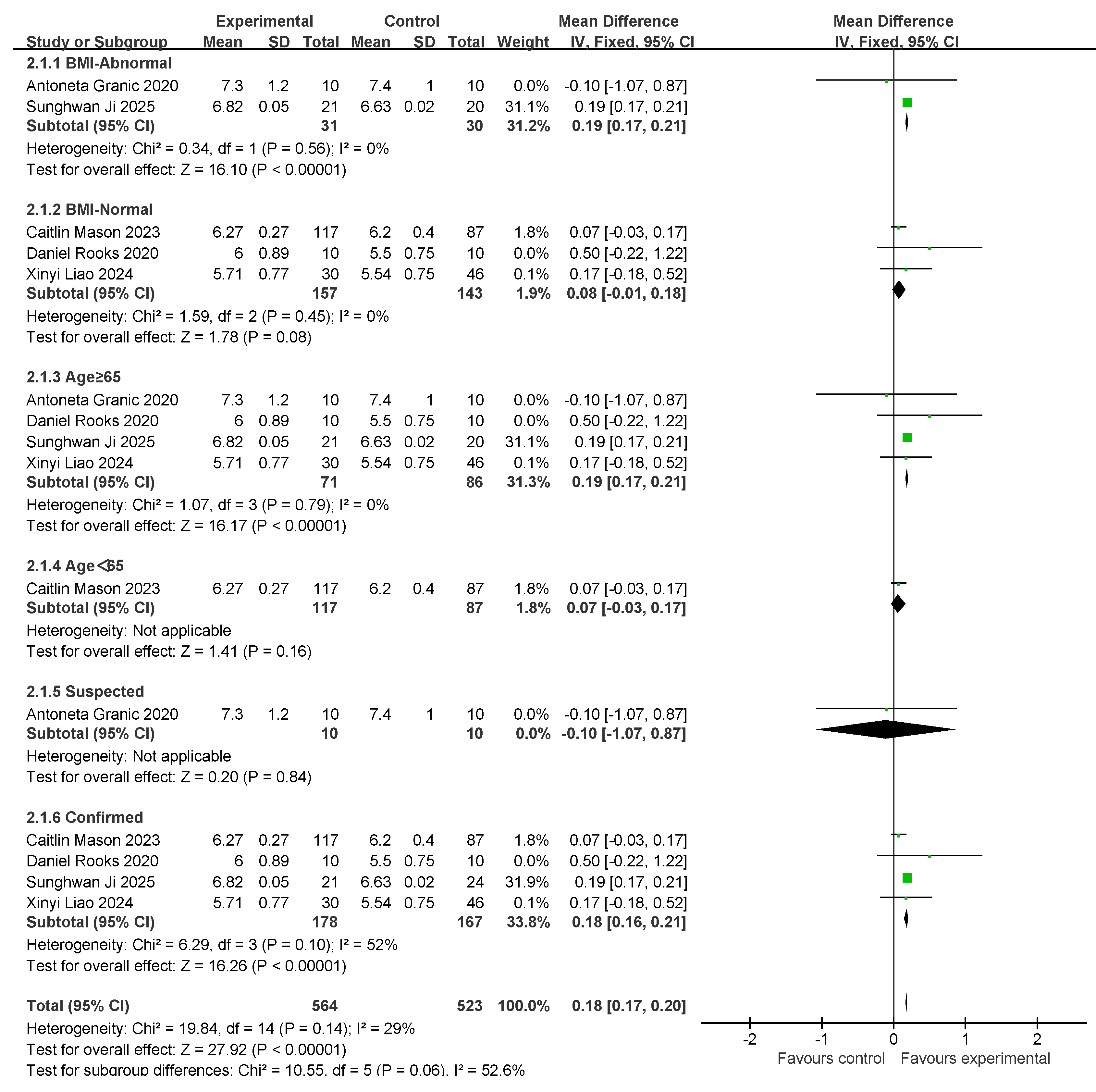
3.5. SMI Results and Subgroup Analysis
3.6. Gait Speed Results and Subgroup Analysis
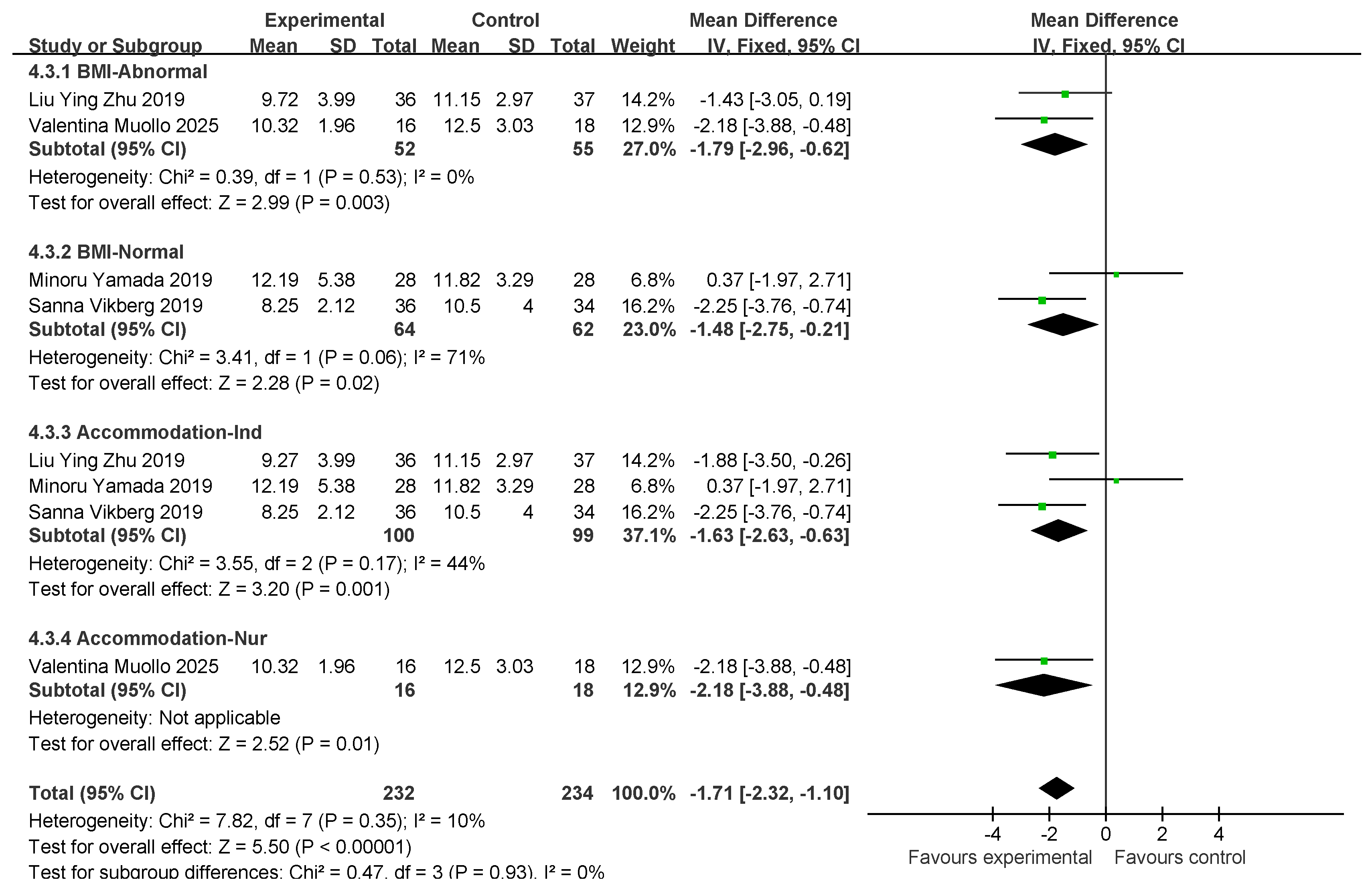
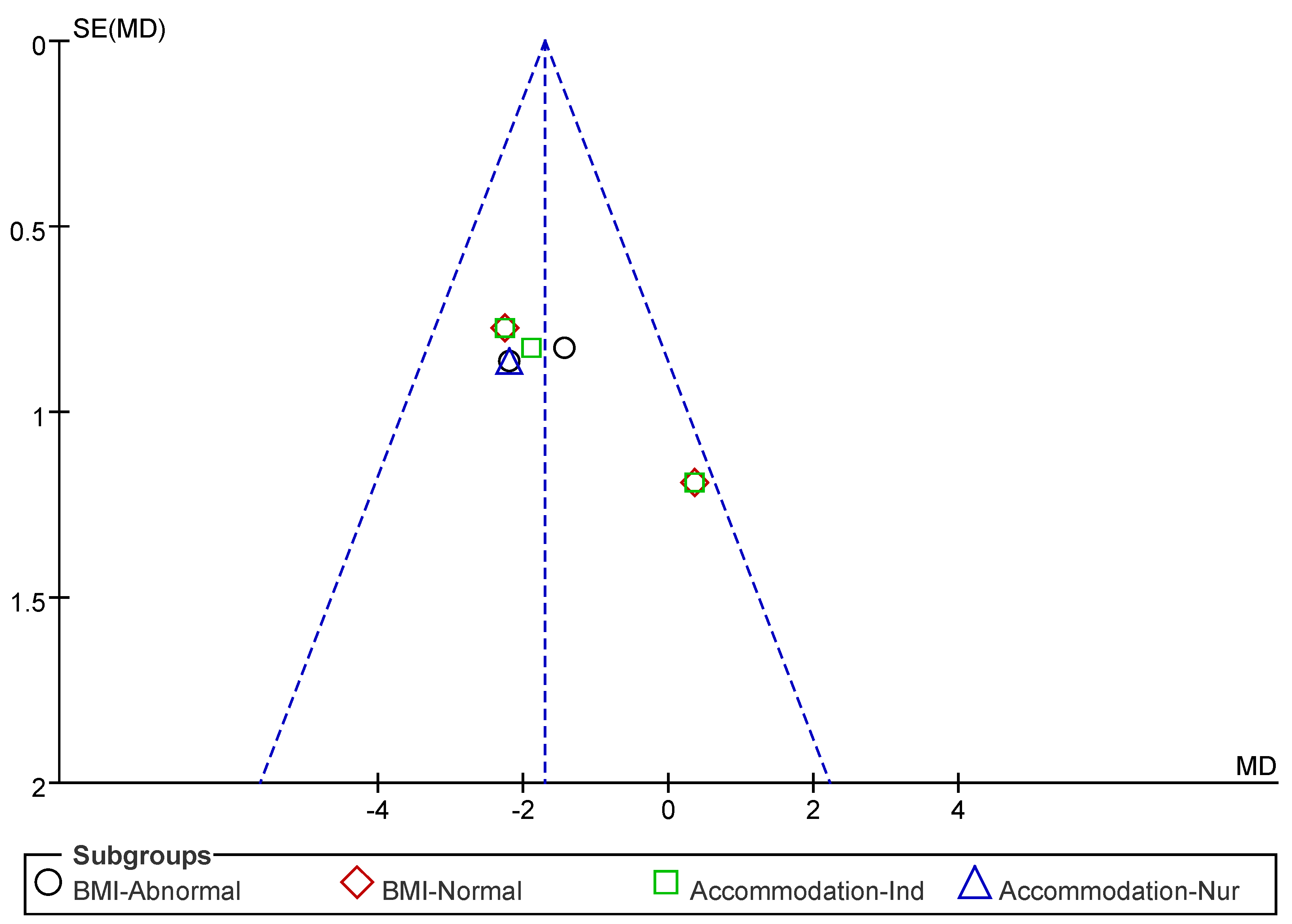
3.7. Five-Times Sit-to-Stand Results and Subgroup Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- Zanchetta, M.B.; Abdala, R.; Massari, F.; Rey, P.; Spivacow, R.; Miechi, L.; Longobardi, V.; Brun, L.R.M. Postmenopausal women with sarcopenia have higher prevalence of falls and vertebral fractures. Medicina 2021, 81, 47–53. [Google Scholar]
- Beaudart, C.; Dawson, A.; Shaw, S.; Harvey, N.C.; Kanis, J.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.; Bruyère, O. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef]
- Bosaeus, I.; Rothenberg, E. Nutrition and physical activity for the prevention and treatment of age-related sarcopenia. Proc. Nutr. Soc. 2016, 75, 174–180. [Google Scholar] [CrossRef]
- Welch, A. Micronutrient malnutrition across the life course, sarcopenia and frailty. Proc. Nutr. Soc. 2021, 80, 279–282. [Google Scholar] [CrossRef]
- Millward, D.J. Nutrition and sarcopenia: Evidence for an interaction. Proc. Nutr. Soc. 2012, 71, 566–575. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef]
- Kim, H.I.; Ahn, S.H.; Kim, Y.; Lee, J.E.; Choi, E.; Seo, S.K. Effects of sarcopenia and sarcopenic obesity on joint pain and degenerative osteoarthritis in postmenopausal women. Sci. Rep. 2022, 12, 13543. [Google Scholar] [CrossRef]
- Follis, S.; Cook, A.; Bea, J.W.; Going, S.B.; Laddu, D.; Cauley, J.A.; Shadyab, A.H.; Stefanick, M.L.; Chen, Z. Association between sarcopenic obesity and falls in a multiethnic cohort of postmenopausal women. J. Am. Geriatr. Soc. 2018, 66, 2314–2320. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Sezgin, D.; O’Donovan, M.R.; Molloy, D.W.; Clegg, A.; Rockwood, K.; Liew, A. Prevalence of frailty in 62 countries across the world: A systematic review and meta-analysis of population-level studies. Age Ageing 2021, 50, 96–104. [Google Scholar] [CrossRef]
- Liu, J.H. Sarcopenia and menopause. Menopause 2023, 30, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S.; Morley, J.E.; Anker, S.D. From muscle wasting to sarcopenia and myopenia: Update 2012. J. Cachexia Sarcopenia Muscle 2012, 3, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Ding, Z.; Chen, J. Deciphering the role of IGFBP5 in delaying fibrosis and sarcopenia in aging skeletal muscle: Therapeutic implications and molecular mechanisms. Front. Pharmacol. 2025, 16, 1557703. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Hung, C.-C.; Chiang, Y.-Y.; Chen, C.-Y.; Liao, L.-C.; Ma, M.H.-M.; Hwang, J.-J.; Hsu, C.-C.; Li, C.-Y.; Fu, S.-H.; et al. Effects of osteoporosis treatment and multicomponent integrated care on intrinsic capacity and happiness among rural community-dwelling older adults: The Healthy Longevity and Ageing in Place (HOPE) randomised controlled trial. Age Ageing 2025, 54, afaf017. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Egan, B.; Zierath, J.R. Exercise Metabolism and the Molecular Regulation of Skeletal Muscle Adaptation. Cell Metab. 2013, 17, 162–184. [Google Scholar] [CrossRef]
- Tessier, A.-J.; Chevalier, S. An Update on Protein, Leucine, Omega-3 Fatty Acids, and Vitamin D in the Prevention and Treatment of Sarcopenia and Functional Decline. Nutrients 2018, 10, 1099. [Google Scholar] [CrossRef]
- Therdyothin, A.; Phiphopthatsanee, N.; Isanejad, M. The Effect of Omega-3 Fatty Acids on Sarcopenia: Mechanism of Action and Potential Efficacy. Mar. Drugs 2023, 21, 399. [Google Scholar] [CrossRef]
- Devries, M.C.; Phillips, S.M. Supplemental Protein in Support of Muscle Mass and Health: Advantage Whey. J. Food Sci. 2015, 80, A8–A15. [Google Scholar] [CrossRef]
- Montenegro, K.R.; Cruzat, V.; Carlessi, R.; Newsholme, P. Mechanisms of vitamin D action in skeletal muscle. Nutr. Res. Rev. 2019, 32, 192–204. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Arribalzaga, S.; Gutiérrez-Abejón, E.; Azarbayjani, M.A.; Mielgo-Ayuso, J.; Roche, E. Omega-3 fatty acid supplementation on post-exercise inflammation, muscle damage, oxidative response, and sports performance in physically healthy adults—A systematic review of randomized controlled trials. Nutrients 2024, 16, 2044. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Shi, Q.; Nong, K.; Li, S.; Yue, J.; Huang, J.; Dong, B.; Beauchamp, M.; Hao, Q. Exercise for sarcopenia in older people: A systematic review and network meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Sun, Y.; Zhang, T.; Zou, L.; Wu, X.; Wang, D.; Chen, Z. Exercise Programs for Muscle Mass, Muscle Strength and Physical Performance in Older Adults with Sarcopenia: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 863. [Google Scholar] [CrossRef]
- Cheng, F.; Li, N.; Yang, J.; Yang, J.; Yang, W.; Ran, J.; Sun, P.; Liao, Y. The effect of resistance training on patients with secondary sarcopenia: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 28784. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-H.; Chiu, W.-C.; Hsu, Y.-P.; Lo, Y.-L.; Wang, Y.-H. Effects of Omega-3 Fatty Acids on Muscle Mass, Muscle Strength and Muscle Performance among the Elderly: A Meta-Analysis. Nutrients 2020, 12, 3739. [Google Scholar] [CrossRef]
- Whaikid, P.; Piaseu, N. The effectiveness of protein supplementation combined with resistance exercise programs among community-dwelling older adults with sarcopenia: A systematic review and meta-analysis. Epidemiol. Health 2024, 46, e2024030. [Google Scholar] [CrossRef]
- Hernández-Lepe, M.A.; Miranda-Gil, M.I.; Valbuena-Gregorio, E.; Olivas-Aguirre, F.J. Exercise Programs Combined with Diet Supplementation Improve Body Composition and Physical Function in Older Adults with Sarcopenia: A Systematic Review. Nutrients 2023, 15, 1998. [Google Scholar] [CrossRef]
- Wu, P.-Y.; Huang, K.-S.; Chen, K.-M.; Chou, C.-P.; Tu, Y.-K. Exercise, Nutrition, and Combined Exercise and Nutrition in Older Adults with Sarcopenia: A Systematic Review and Network Meta-analysis. Maturitas 2021, 145, 38–48. [Google Scholar] [CrossRef]
- Song, Z.; Pan, T.; Tong, X.; Yang, Y.; Zhang, Z. The effects of nutritional supplementation on older sarcopenic individuals who engage in resistance training: A meta-analysis. Front. Nutr. 2023, 10, 1109789. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, H.; Gong, Y.; Tang, Y.; Su, H.; Zhang, Z.; Tong, P.; Chen, G. Clinical outcome changes in sarcopenic obesity: A meta-analysis of exercise training methods. BMC Geriatr. 2025, 25, 33. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Tu, S.; Hao, X.; Chen, X.; Pan, D.; Liao, W.; Wu, R.; Yang, L.; Xia, H.; Wang, S.; et al. Exercise, Nutrition, and Neuromuscular Electrical Stimulation for Sarcopenic Obesity: A Systematic Review and Meta-Analysis of Management in Middle-Aged and Older Adults. Nutrients 2025, 17, 1504. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.-Y.; Chan, R.; Kwok, T.; Cheng, K.C.-C.; Ha, A.; Woo, J. Effects of exercise and nutrition supplementation in community-dwelling older Chinese people with sarcopenia: A randomized controlled trial. Age Ageing 2019, 48, 220–228. [Google Scholar] [CrossRef]
- Li, Z.; Cui, M.; Yu, K.; Zhang, X.-W.; Li, C.-W.; Nie, X.-D.; Wang, F. Effects of nutrition supplementation and physical exercise on muscle mass, muscle strength and fat mass among sarcopenic elderly: A randomized controlled trial. Appl. Physiol. Nutr. Metab. 2021, 46, 494–500. [Google Scholar] [CrossRef]
- Liao, X.; Cheng, D.; Li, J.; Zhu, L.; Zhang, S.; Jing, X.; Shi, L. Effects of oral oligopeptide preparation and exercise intervention in older people with sarcopenia: A randomized controlled trial. BMC Geriatr. 2024, 24, 260. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Otobe, Y.; Tanaka, T.; Ohji, S.; Koyama, S.; Sato, A.; Suzuki, M.; et al. Synergistic effect of bodyweight resistance exercise and protein supplementation on skeletal muscle in sarcopenic or dynapenic older adults. Geriatr. Gerontol. Int. 2019, 19, 429–437. [Google Scholar] [CrossRef]
- Ji, S.; Baek, J.Y.; Go, J.; Lee, C.K.; Yu, S.S.; Lee, E.; Jung, H.-W.; Jang, I.-Y. Effect of Exercise and Nutrition Intervention for Older Adults with Impaired Physical Function with Preserved Muscle Mass (Functional Sarcopenia): A Randomized Controlled Trial. Clin. Interv. Aging 2025, 20, 161–170. [Google Scholar] [CrossRef]
- Arıcı, H.; Tor, Y.B.; Altınkaynak, M.; Erten, N.; Saka, B.; Bayramlar, O.F.; Karakuş, Z.N.; Akpınar, T.S. Personalized Diet With or Without Physical Exercise Improves Nutritional Status, Muscle Strength, Physical Performance, and Quality of Life in Malnourished Older Adults: A Prospective Randomized Controlled Study. Nutrients 2025, 17, 675. [Google Scholar] [CrossRef]
- Rooks, D.; Swan, T.; Goswami, B.; Filosa, L.A.; Bunte, O.; Panchaud, N.; Coleman, L.A.; Miller, R.R.; Garcia Garayoa, E.; Praestgaard, J.; et al. Bimagrumab vs Optimized Standard of Care for Treatment of Sarcopenia in Community-Dwelling Older Adults. JAMA Netw. Open 2020, 3, e2020836. [Google Scholar] [CrossRef]
- Mason, C.; Xiao, L.; Imayama, I.; Duggan, C.R.; Foster-Schubert, K.E.; Kong, A.; Campbell, K.L.; Wang, C.-Y.; Villasenor, A.; Neuhouser, M.L.; et al. Influence of Diet, Exercise, and Serum Vitamin D on Sarcopenia in Postmenopausal Women. Med. Sci. Sports Exerc. 2013, 45, 607–614. [Google Scholar] [CrossRef]
- Muollo, V.; Rossi, A.; Milanese, C.; Cavedon, V.; Schena, F.; Giani, A.; Urbani, S.; Mazzali, G.; Zamboni, M.; Zoico, E. Effects of a Hypocaloric Diet Plus Resistance Training with and Without Amino Acids in Older Participants with Dynapenic Obesity: A Randomized Clinical Trial. Nutrients 2025, 17, 418. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Eggimann, A.K.; De Godoi Rezende Costa Molino, C.; Freystaetter, G.; Vellas, B.; Kanis, J.A.; Rizzoli, R.; Kressig, R.W.; Armbrecht, G.; Da Silva, J.A.P.; Dawson-Hughes, B.; et al. Effect of vitamin D, omega-3 supplementation, or a home exercise program on muscle mass and sarcopenia: DO-HEALTH trial. J. Am. Geriatr. Soc. 2025, 73, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Strasser, E.M.; Franzke, B.; Hofmann, M.; Schober-Halper, B.; Oesen, S.; Jandrasits, W.; Graf, A.; Ploder, M.; Bachl, N.; Quittan, M.; et al. Resistance training with or without nutritional supplementation showed no influence on muscle thickness in old-institutionalized adults: A secondary analysis of the Vienna Active Ageing Study. Eur. J. Phys. Rehabil. Med. 2022, 58, 646. [Google Scholar] [CrossRef]
- Vikberg, S.; Sörlén, N.; Brandén, L.; Johansson, J.; Nordström, A.; Hult, A.; Nordström, P. Effects of resistance training on functional strength and muscle mass in 70-year-old individuals with pre-sarcopenia: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2019, 20, 28–34. [Google Scholar] [CrossRef]
- Granic, A.; Hurst, C.; Dismore, L.; Stevenson, E.; Sayer, A.A.; Aspray, T. Feasibility and acceptability of a milk and resistance exercise intervention to improve muscle function in community-dwelling older adults (MIlkMAN): Pilot study. PLoS ONE 2020, 15, e0235952. [Google Scholar] [CrossRef]
- Gade, J.; Beck, A.M.; Andersen, H.E.; Christensen, B.; Rønholt, F.; Klausen, T.W.; Vinther, A.; Astrup, A. Protein supplementation combined with low-intensity resistance training in geriatric medical patients during and after hospitalisation: A randomised, double-blind, multicentre trial. Br. J. Nutr. 2019, 122, 1006–1020. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Gong, Y.; Yang, Y.; Zhang, X.; Tong, L. Comparative efficacy of exercise, nutrition, and combined exercise and nutritional interventions in older adults with sarcopenic obesity: A protocol for systematic review and network meta-analysis. Syst. Rev. 2025, 14, 77. [Google Scholar] [CrossRef]
- Qiu, H.; Zheng, W.; Zhou, X.; Liu, Q.; Zhao, X. Training modalities for elder sarcopenic obesity: A systematic review and network meta-analysis. Front. Nutr. 2025, 12, 1537291. [Google Scholar] [CrossRef] [PubMed]
- Hsu, N.-W.; Lin, C.-H.; Yang, N.-P.; Chen, H.-C.; Chou, P. Handgrip strength is associated with mortality in community-dwelling older adults: The Yilan cohort study, Taiwan. BMC Public Health 2023, 23, 2194. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Meng, T.; Yang, W.; Yan, M.; Su, X.; Wang, X.; Chen, L.; Ren, Y. Association of grip strength and comorbidities with all-cause mortality in the older hypertensive adults. Front. Public Health 2023, 11, 1162425. [Google Scholar] [CrossRef]
- Jogiat, U.M.; Sasewich, H.; Turner, S.R.; Baracos, V.; Eurich, D.T.; Filafilo, H.; Bédard, E.L.R. Sarcopenia Determined by Skeletal Muscle Index Predicts Overall Survival, Disease-free Survival, and Postoperative Complications in Resectable Esophageal Cancer. Ann. Surg. 2022, 276, e311–e318. [Google Scholar] [CrossRef]
- Beck Jepsen, D.; Robinson, K.; Ogliari, G.; Montero-Odasso, M.; Kamkar, N.; Ryg, J.; Freiberger, E.; Masud, T. Predicting falls in older adults: An umbrella review of instruments assessing gait, balance, and functional mobility. BMC Geriatr. 2022, 22, 615. [Google Scholar]
- Muñoz-Bermejo, L.; Adsuar, J.C.; Mendoza-Muñoz, M.; Barrios-Fernández, S.; Garcia-Gordillo, M.A.; Pérez-Gómez, J.; Carlos-Vivas, J. Test-Retest Reliability of Five Times Sit to Stand Test (FTSST) in Adults: A Systematic Review and Meta-Analysis. Biology 2021, 10, 510. [Google Scholar] [CrossRef]
- Mo, Y.; Chen, L.; Zhou, Y.; Bone, A.; Maddocks, M.; Evans, C.J. Sarcopenia interventions in long-term care facilities targeting sedentary behaviour and physical inactivity: A systematic review. J. Cachexia Sarcopenia Muscle 2024, 15, 2208–2233. [Google Scholar] [CrossRef]
- Cabrolier-Molina, J.; Martín-Rodríguez, A.; Clemente-Suárez, V.J. The Effects of Exercise Intervention in Older Adults With and Without Sarcopenia: A Systematic Review. Sports 2025, 13, 152. [Google Scholar] [CrossRef]
- Lu, L.; Mao, L.; Feng, Y.; Ainsworth, B.E.; Liu, Y.; Chen, N. Effects of different exercise training modes on muscle strength and physical performance in older people with sarcopenia: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 708. [Google Scholar] [CrossRef]
- Lu, Y.; Niti, M.; Yap, K.B.; Tan, C.T.Y.; Nyunt, M.S.Z.; Feng, L.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; et al. Effects of multi-domain lifestyle interventions on sarcopenia measures and blood biomarkers: Secondary analysis of a randomized controlled trial of community-dwelling pre-frail and frail older adults. Aging 2021, 13, 9330–9347. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, G.; Huang, X.; He, F. Effects of protein supplementation on muscle mass, muscle strength, and physical performance in older adults with physical inactivity: A systematic review and meta-analysis. BMC Geriatr. 2025, 25, 228. [Google Scholar] [CrossRef]
- Eglseer, D.; Traxler, M.; Schoufour, J.D.; Weijs, P.J.M.; Voortman, T.; Boirie, Y.; Cruz-Jentoft, A.J.; Reiter, L.; Bauer, S.; Weijs, P.; et al. Nutritional and exercise interventions in individuals with sarcopenic obesity around retirement age: A systematic review and meta-analysis. Nutr. Rev. 2023, 81, 1077–1090. [Google Scholar] [CrossRef]
- Hsu, H.-C.; Chow, L.-H.; Chen, Y.-L.; Hung, H.-M.; Yen, M.; Lee, H.-F. Effects of exercise and nutrition in improving sarcopenia in liver cirrhosis patients: A systematic review and meta-analysis. Hepatobiliary Surg. Nutr. 2025, 14, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Minimal clinically important difference for grip strength: A systematic review. J. Phys. Ther. Sci. 2019, 31, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Polo-Ferrero, L.; Navarro-López, V.; Fuentes, M.; Lacal, J.; Cancelas-Felgueras, M.D.; Santos-Blázquez, N.; Méndez-Sánchez, R.; Sánchez-González, J.L. Effect of Resistance Training on Older Adults with Sarcopenic Obesity: A Comprehensive Systematic Review and Meta-Analysis of Blood Biomarkers, Functionality, and Body Composition. Nurs. Rep. 2025, 15, 89. [Google Scholar] [CrossRef]
- Chen, N.; He, X.; Feng, Y.; Ainsworth, B.E.; Liu, Y. Effects of resistance training in healthy older people with sarcopenia: A systematic review and meta-analysis of randomized controlled trials. Eur. Rev. Aging Phys. Act. 2021, 18, 23. [Google Scholar] [CrossRef]
- Karlsson, E.S.; Grönstedt, H.K.; Faxén-Irving, G.; Franzén, E.; Luiking, Y.C.; Seiger, Å.; Vikström, S.; Wimo, A.; Cederholm, T.E.; Boström, A.-M. Response and Adherence of Nursing Home Residents to a Nutrition/Exercise Intervention. J. Am. Med. Dir. Assoc. 2021, 22, 1939–1945.e3. [Google Scholar] [CrossRef]
- Zhang, L.; Ge, Y.; Zhao, W.; Shu, X.; Kang, L.; Wang, Q.; Liu, Y. A 4-Week Mobile App–Based Telerehabilitation Program vs Conventional In-Person Rehabilitation in Older Adults With Sarcopenia: Randomized Controlled Trial. J. Med. Internet Res. 2025, 27, e67846. [Google Scholar] [CrossRef]
- Teh, R.; Barnett, D.; Edlin, R.; Kerse, N.; Waters, D.L.; Hale, L.; Tay, E.; Leilua, E.; Pillai, A. Effectiveness of a complex intervention of group-based nutrition and physical activity to prevent frailty in pre-frail older adults (SUPER): A randomised controlled trial. Lancet Healthy Longev. 2022, 3, e519–e530. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Population | Diagnostic Criteria Used | Age (Mean + SD) | Total (Male/Female) | Exercise Intervention | Nutrition Intervention | Control | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Liu-Ying Zhu (2019) [35] | China | Sarcopenia | AWGS 2019 | T: 74.8 ± 6.9 C: 72.2 ± 6.6 | T: 36/7/29 C: 37/8/29 | RT and AE Length of Intervention: 24 weeks Freq: 3 times a week Duration: 60 min | N: protein + vitamin Length of Intervention: 12 weeks Freq: 2 times a day Dose: protein (8.61 g), vitamin D (130 IU) | RCT | HS 5 STS |
| Zhuo Li (2019) [36] | China | Sarcopenia | AWGS 2019 | T: 71.52 ± 5.28 C: 72.91± 6.29 | T: 59/22/37 C: 59/12/37 | RT & Walking Length of Intervention: 12 weeks Freq: 3 times a week Duration: 30 min | N: protein + vitamin Length of Intervention: 12 weeks Freq: 2 times a day Dose: protein powder (10 g) EPA (300 mg), DHA (200 mg), and vitamin D3 (250 IU) | RCT | GS |
| Sanna Vikberg (2019) [47] | Sweden | Sarcopenia | EWGSOP2 | T: 70.9 ± 0.28 C: 70.9 ± 0.29 | T: 36/16/20 C: 34/16/18 | RT Length of Intervention: 10 weeks Freq: 3 times a week Duration: 30 min | N: protein Length of Intervention: 10 weeks Freq: 2 times a day Dose: 250 mL liquid, 21 g protein, 1.5 g fat (week 1–7 of the intervention) or 10 g carbohydrates, 30 g protein, and 1.5 g fat (week 8–10 of the intervention) | RCT | HS 5 STS |
| Huzeyfe Arıcı (2025) [40] | Turkey | Sarcopenia | AWGS 2019 | T: 72.6 ± 4.7 C: 71.0 ± 4.5 | T: 10/5/5 C: 10/6/4 | RT Length of Intervention: 12 weeks Freq: 3 times a week Duration: 60 min | N: protein + VD Length of Intervention: 12 weeks Freq: 12 weeks Dose: protein (1.0–1.2 g/Kg /day) | RCT | HS |
| Anna K Eggimann (2025) [45] | Switzerland | Sarcopenia | EWGSOP2 | T: 74.9 ± 4.4 C: 75.0 ± 4.4 | T: 744/273/471 C: 751/278/473 | RT +Joint flex Length of Intervention: 3 Years Freq: 3 times a week Duration: 30 min | N: vitamin D + DHA + omega-3s Length of Intervention: 3 years Freq: 1 time/D Dose: vitamin D, 200 UI DHA, omega-3s | RCT | GS |
| Xinyi Liao (2024) [37] | China | Sarcopenia | AWGS 2019 | T: 70.52 ± 3.30 C: 73.21 ± 4.98 | T: 30/16/14 C: 46/24/22 | RT Length of Intervention: 16 weeks Freq: 5 times a week Duration: 45–60 min | Length of Intervention: 16 weeks Freq: 1 times a day Dose: energy 185 kcal, protein 24.2 g (including plant oligopeptide 11 g, casein peptide 4 g, branch chain amino acid 5 g), CaHMB2.5 g per day | RCT | SMI HS GS |
| EvaM Strasser (2022) [46] | Austria | Sarcopenia | EWGSOP2 | T: 81.5 ± 7.4 C: 83.5 ± 5.7 | T: 30/3/27 C: 29/3/26 | RT (plastic band) Length of Intervention: 18 months Freq: 1 time/w (1–12 months) 1 time/w/13–18 months Duration: 60 min | Length of Intervention: 18 months Freq: 1 times/w (1–12 months) 1 times/w/13–18 months. Dose: vitamin D, calcium, vitamin b6, vitamin b12, vitamin C, vitamin E, folic acid, and magnesium. | RCT | HS |
| Daniel Rooks (2020) [41] | USA | Sarcopenia | EWGSOP2 | T: 71.7 ± 3.6 C: 71.7 ± 3.6 | T: 10/5/5 C: 10/5/5 | RE: RT Length of Intervention: 6 weeks Freq: 2 times/week Duration: 60 min | Length of Intervention: 6 weeks Freq: 1 time/after exercise Dose: 3.6 g fat, 3.4 g protein, and 4.7 g carbohydrate per 100 g. And habitual diet | RCT | HS |
| Minoru Yamada (2019) [38] | Japan | Sarcopenia | AWGS 2019 | T: 84.9 ± 5.6 C: 83.9 ± 5.7 | T: 28/8/20 C: 28/13/15 | RT Length of Intervention: 12 weeks Freq: 2 times/weeks Duration: 30 min | Length of Intervention: 12 weeks Freq: 2 times/weeks Dose: vitamin D | RCT | HS 5STS |
| Mariangela Rondanelli (2016) [44] | Italy | Sarcopenia | EWGSOP2 | T: 80.77 ± 6.29 C: 80.21 ± 8.54 | T: 69/29/42 C: 61/24/39 | RT Length of Intervention: 12 weeks Freq: 5 times/w/12 Duration: 30 min | Length of Intervention: 12 weeks Freq: 2 times/D/week Dose: vitamin D | RCT | HS |
| Caitlin Mason (2023) [42] | USA | Sarcopenia | EWGSOP2 | T: 57.9 ± 5.0 C: 58.0 ± 5.0 | T: 117/88/29 C: 87/65/23 | RT + ARE Length of Intervention: 12 months Freq: 5 times/week Duration: 45 min | Length of Intervention: 12 months Freq: 5 times/week Dose: vitamin D | RCT | SMI |
| Sunghwan Ji (2025) [39] | Korea | Sarcopenia | AWGS 2019 | T: 77.86 ± 4.46 C: 78.24 ± 4.47 | T: 21/10/11 C: 20/10/11 | RT Length of Intervention: 12 weeks Freq: 40 h/week Duration: 45 min | Length of Intervention: 12 weeks Freq: middle of the diet Dose: 13 g/protein, 1.4 fat, 8 carb | RCT | SMI HS GS |
| Valentina Muollo (2025) [43] | Italy | Sarcopenia | EWGSOP2 | T: 65.75 ± 3.94 C: 66.67 ± 3.85 | T: 16//8/8 C: 18/9/9 | RT Length of Intervention: 12 W Freq: 3/D/W Duration: 60 min | Length of Intervention: 12 W Freq: 2/D/W Dose: EAA + 22 g of protein/day | RCT | GS 5 STS |
| Antoneta Granic (2020) [48] | UK | Sarcopenia | EWGSOP2 | T: 72.2 ± 4.1 C: 70.8 ± 4.0 | T: 10/6/4 C: 10/7/3 | RT Length of Intervention: 6 weeks Freq: ≥2 times/week Duration:60 min | Length of Intervention: 6 weeks Freq: 1/D Dose: milk 1000 mL, 20 g of protein/day | RCT | GS, HS. SMI |
| Josepine Gade (2019) [49] | Denmark | Sarcopenia | EWGSOP2 | T: 84.2 ± 6.3 C: 85.3 ± 6.2 | T: 82/50/32 C: 83/50/30 | RT Length of Intervention: Freq: ≥2 times/week Duration: 60 min | Length of Intervention: 12 W Freq: 1/D Dose: milk 1000 mL, 10 g of protein/day | RCT | HS GS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Pan, N.; Luo, J.; Liu, Y.; Ossowski, Z. Exercise and Nutrition for Sarcopenia: A Systematic Review and Meta-Analysis with Subgroup Analysis by Population Characteristics. Nutrients 2025, 17, 2342. https://doi.org/10.3390/nu17142342
Yang Y, Pan N, Luo J, Liu Y, Ossowski Z. Exercise and Nutrition for Sarcopenia: A Systematic Review and Meta-Analysis with Subgroup Analysis by Population Characteristics. Nutrients. 2025; 17(14):2342. https://doi.org/10.3390/nu17142342
Chicago/Turabian StyleYang, Yong, Neng Pan, Jiedan Luo, Yufei Liu, and Zbigniew Ossowski. 2025. "Exercise and Nutrition for Sarcopenia: A Systematic Review and Meta-Analysis with Subgroup Analysis by Population Characteristics" Nutrients 17, no. 14: 2342. https://doi.org/10.3390/nu17142342
APA StyleYang, Y., Pan, N., Luo, J., Liu, Y., & Ossowski, Z. (2025). Exercise and Nutrition for Sarcopenia: A Systematic Review and Meta-Analysis with Subgroup Analysis by Population Characteristics. Nutrients, 17(14), 2342. https://doi.org/10.3390/nu17142342