
The Association Between Fast Food Consumption and Inflammatory Bowel Disease: A Case-Control Study and Meta-Analysis

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Methods
2.1. The Case-Control Study
2.1.1. Study Design and Population
2.1.2. Exposure, Outcome, and Covariates
2.1.3. Study Size
2.1.4. Statistical Analysis
2.2. The Meta-Analysis
2.2.1. Registration and Protocol
2.2.2. Eligibility Criteria
2.2.3. Information Sources
2.2.4. Search Strategy
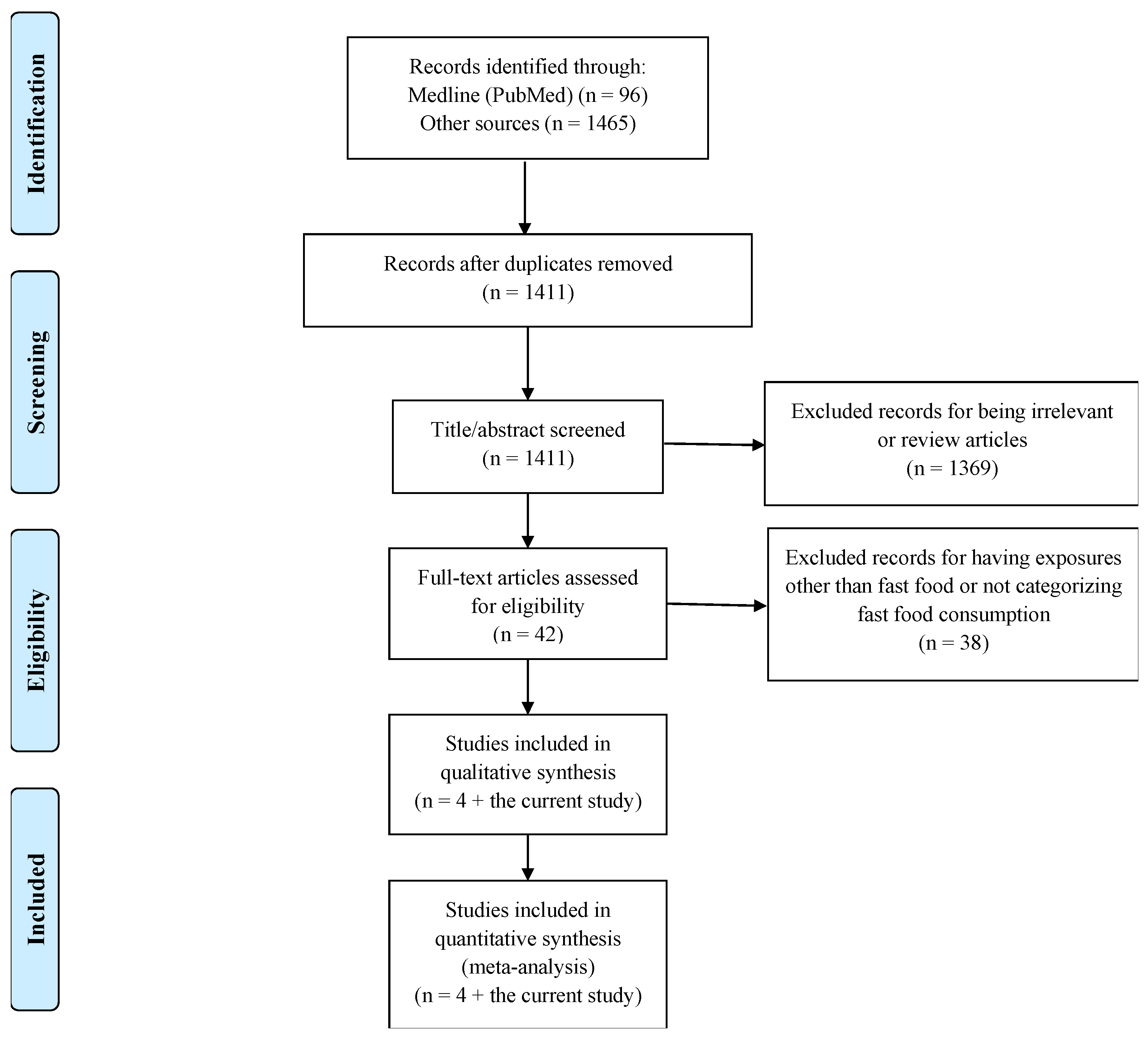
2.2.5. Selection Process
2.2.6. Data Collection Process
2.2.7. Data Items
2.2.8. Study Risk of Bias Assessment
2.2.9. Effect Measures
2.2.10. Synthesis Methods
2.2.11. Reporting Bias Assessment
2.2.12. Certainty Assessment
3. Results
3.1. The Case-Control Study
3.1.1. Participants and Descriptive Data
3.1.2. Associations
3.2. The Meta-Analysis
3.2.1. Study Selection
3.2.2. Study Characteristics
3.2.3. Quality Assessment
3.2.4. Results of Individual Studies
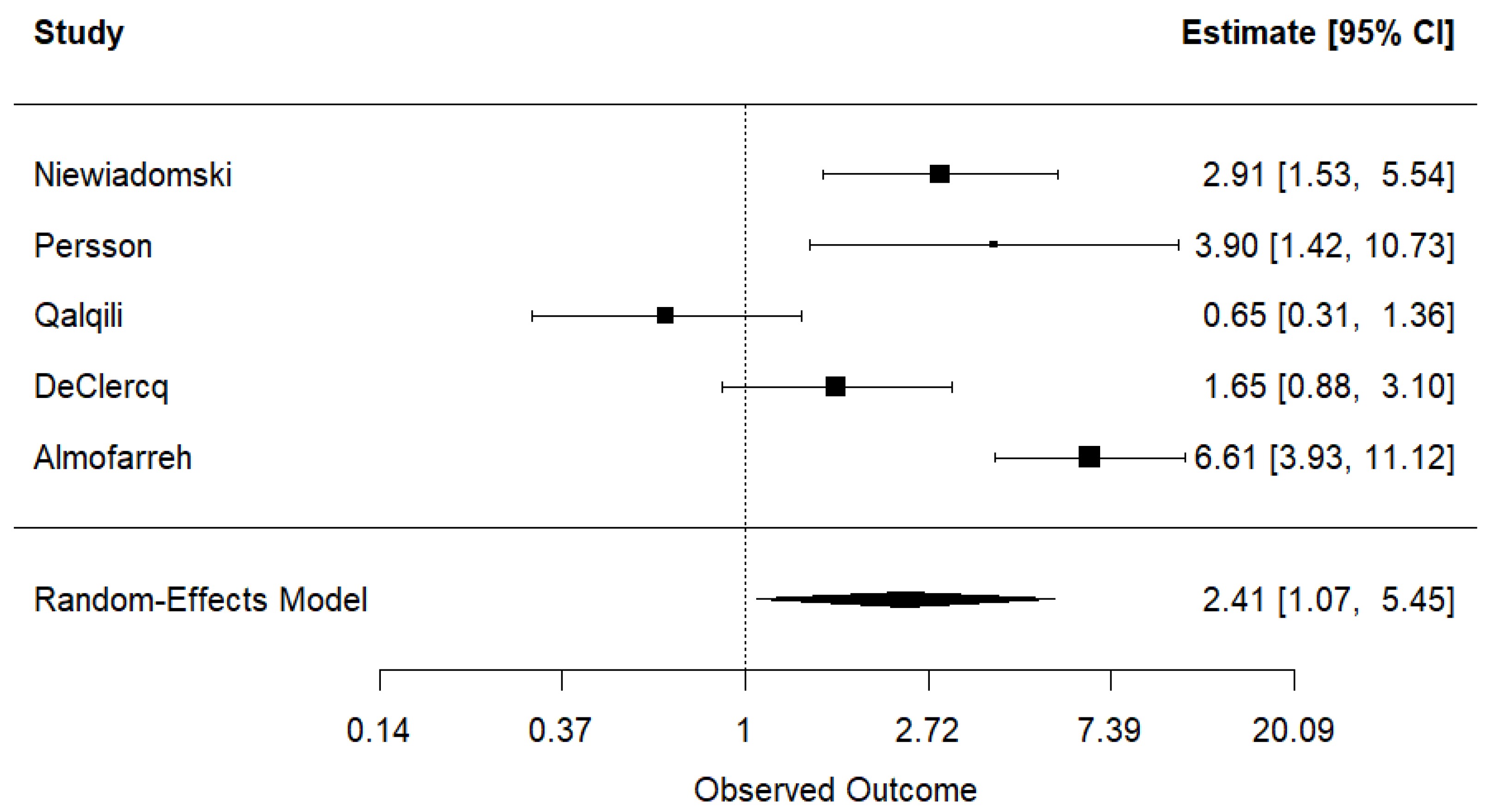
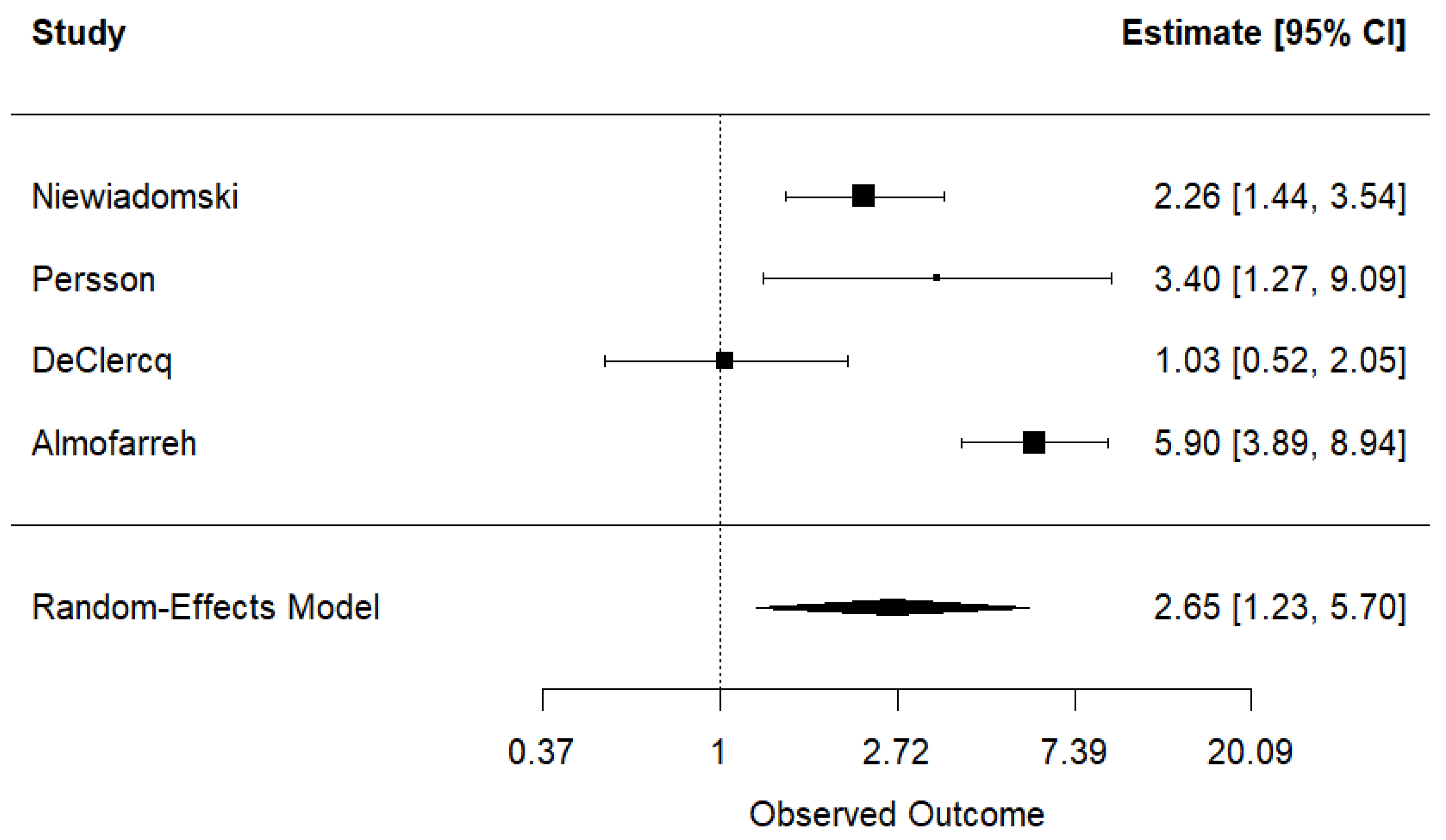
3.2.5. Results of Syntheses
3.2.6. Publication Bias
3.2.7. Certainty of Evidence
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fakhoury, M.; Negrulj, R.; Mooranian, A.; Al-Salami, H. Inflammatory bowel disease: Clinical aspects and treatments. J. Inflamm. Res. 2014, 7, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Armuzzi, A.; Liguori, G. Quality of life in patients with moderate to severe ulcerative colitis and the impact of treatment: A narrative review. Dig. Liver Dis. 2021, 53, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Mateos, A.M. Gut Feelings: The Psychological Impact of Inflammatory Bowel Disease. J. Clin. Med. 2023, 12, 3867. [Google Scholar] [CrossRef]
- Wang, R.; Li, Z.; Liu, S.; Zhang, D. Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: A systematic analysis based on the Global Burden of Disease Study 2019. BMJ Open 2023, 13, e065186. [Google Scholar] [CrossRef] [PubMed]
- Kahn-Boesel, O.; Cautha, S.; Ufere, N.N.; Ananthakrishnan, A.N.; Kochar, B. A Narrative Review of Financial Burden, Distress, and Toxicity of Inflammatory Bowel Diseases in the United States. Am. J. Gastroenterol. 2023, 118, 1545–1553. [Google Scholar] [CrossRef]
- Christensen, C.; Knudsen, A.; Arnesen, E.K.; Hatlebakk, J.G.; Sletten, I.S.; Fadnes, L.T. Diet, Food, and Nutritional Exposures and Inflammatory Bowel Disease or Progression of Disease: An Umbrella Review. Adv. Nutr. 2024, 15, 100219. [Google Scholar] [CrossRef]
- Myles, I.A. Fast food fever: Reviewing the impacts of the Western diet on immunity. Nutr J. 2014, 13, 61. [Google Scholar] [CrossRef]
- Xia, B.; Li, Y.; Hu, L.; Xie, P.; Mi, N.; Lv, L.; Liang, Z.; Sun, Y.; Li, Y.; Jiang, X.; et al. Healthy eating patterns are associated with reduced risk of inflammatory bowel disease by lowering low-grade inflammation: Evidence from a large prospective cohort study. BMC Med. 2024, 22, 589. [Google Scholar] [CrossRef]
- Gill, P.A.; Inniss, S.; Kumagai, T.; Rahman, F.Z.; Smith, A.M. The Role of Diet and Gut Microbiota in Regulating Gastrointestinal and Inflammatory Disease. Front. Immunol. 2022, 13, 866059. [Google Scholar] [CrossRef]
- Besedin, D.; Shah, R.; Brennan, C.; Panzeri, E.; Van, T.T.H.; Eri, R. Food additives and their implication in inflammatory bowel disease and metabolic syndrome. Clin. Nutr. ESPEN 2024, 64, 483–495. [Google Scholar] [CrossRef]
- Li, T.; Qiu, Y.; Yang, H.S.; Li, M.Y.; Zhuang, X.J.; Zhang, S.H.; Feng, R.; Chen, B.L.; He, Y.; Zeng, Z.R.; et al. Systematic review and meta-analysis: Association of a pre-illness Western dietary pattern with the risk of developing inflammatory bowel disease. J. Dig. Dis. 2020, 21, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Al Fadda, M.; Peedikayil, M.C.; Kagevi, I.; Al Kahtani, K.; Al Ben Mousa, A.; Al Ashgar, H.I.; Al Sohaibani, F.; Al Quaiz, M.; Abdulla, M.; Khan, M.Q.; et al. Inflammatory bowel disease in Saudi Arabia: A hospital-based clinical study of 312 patients. Ann. Saudi Med. 2012, 32, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Al-Mofarreh, M.A.; Al-Mofleh, I.A. Emerging inflammatory bowel disease in Saudi outpatients: A report of 693 cases. Saudi J. Gastroenterol. 2013, 19, 16–22. [Google Scholar] [CrossRef]
- Alhusseini, N.; Alsinan, N.; Almutahhar, S.; Khader, M.; Tamimi, R.; Elsarrag, M.I.; Warar, R.; Alnasser, S.; Ramadan, M.; Omair, A.; et al. Dietary trends and obesity in Saudi Arabia. Front. Public Health 2024, 11, 1326418. [Google Scholar] [CrossRef]
- Mandoura, N.; Al-Raddadi, R.; Abdulrashid, O.; Shah, H.B.U.; Kassar, S.M.; Hawari, A.R.A.; Jahhaf, J.M. Factors Associated with Consuming Junk Food among Saudi Adults in Jeddah City. Cureus 2017, 9, e2008. [Google Scholar] [CrossRef] [PubMed]
- Almofarreh, A.M.; Sheerah, H.A.; Arafa, A.; Al Mubarak, A.S.; Ali, A.M.; Al-Otaibi, N.M.; Alzahrani, M.A.; Aljubayl, A.R.; Aleid, M.A.; Alhamed, S.S. Dairy Consumption and Inflammatory Bowel Disease among Arab Adults: A Case-Control Study and Meta-Analysis. Nutrients 2024, 16, 2747. [Google Scholar] [CrossRef]
- Almofarreh, A.M.; Sheerah, H.A.; Arafa, A.; Algori, F.A.; Almutairi, G.R.; Alenzi, K.A.; Al-Alsehemi, M.M.; Mekwar, B.H.; Alzeer, O.; Molla, H.N. Fruit and Vegetable Consumption and Inflammatory Bowel Disease: A Case-Control Study. Life 2024, 14, 1524. [Google Scholar] [CrossRef]
- Almofarreh, A.; Sheerah, H.A.; Arafa, A.; Ahamed, S.S.; Alzeer, O.; Al-Hunaishi, W.; Mhimed, M.M.; Al-Hazmi, A.; Lim, S.H. Beverage Consumption and Ulcerative Colitis: A Case-Control Study from Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 2287. [Google Scholar] [CrossRef]
- Almofarreh, A.; Sheerah, H.A.; Arafa, A.; Alzeer, O.; Alohali, E.; Cao, J.; Liu, K.; Almuzaini, Y.; Almishary, M. Association between coffee, tea, and soft drinks consumption and Crohn’s disease in Arab populations: A case-control study. Clin. Nutr. Open Sci. 2024, 55, 116–122. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: www.ohri.ca/programs/clinical_epidemiology\oxford.htm (accessed on 1 March 2025).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Qualqili, T.R.; Rayyan, Y.M.; Tayyem, R.F. Lifestyle and Dietary Factors Associated with Inflammatory Bowel Disease among Jordanian Patients. J. Gastrointest. Liver Dis. 2021, 30, 37–45. [Google Scholar] [CrossRef]
- DeClercq, V.; Langille, M.G.I.; Van Limbergen, J. Differences in adiposity and diet quality among individuals with inflammatory bowel disease in Eastern Canada. PLoS ONE 2018, 13, e0200580. [Google Scholar] [CrossRef]
- Niewiadomski, O.; Studd, C.; Wilson, J.; Williams, J.; Hair, C.; Knight, R.; Prewett, E.; Dabkowski, P.; Alexander, S.; Allen, B.; et al. Influence of food and lifestyle on the risk of developing inflammatory bowel disease. Intern. Med. J. 2016, 46, 669–676. [Google Scholar] [CrossRef]
- Persson, P.G.; Ahlbom, A.; Hellers, G. Diet and inflammatory bowel disease: A case-control study. Epidemiology 1992, 3, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Narula, N.; Chang, N.H.; Mohammad, D.; Wong, E.C.; Ananthakrishnan, A.N.; Chan, S.S.; Carbonnel, F.; Meyer, A. Food Processing and Risk of Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2023, 21, 2483–2495.e1. [Google Scholar] [CrossRef]
- Babaei, A.; Pourmotabbed, A.; Talebi, S.; Mehrabani, S.; Bagheri, R.; Ghoreishy, S.M.; Amirian, P.; Zarpoosh, M.; Mohammadi, H.; Kermani, M.A.H.; et al. The association of ultra-processed food consumption with adult inflammatory bowel disease risk: A systematic review and dose-response meta-analysis of 4,035,694 participants. Nutr. Rev. 2024, 82, 861–871. [Google Scholar] [CrossRef]
- Nie, J.Y.; Zhao, Q. Beverage consumption and risk of ulcerative colitis: Systematic review and meta-analysis of epidemiological studies. Medicine 2017, 96, e9070. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xiang, L.; He, J. Beverage intake and risk of Crohn’s disease: A meta-analysis of 16 epidemiological studies. Medicine 2019, 98, e15795. [Google Scholar] [CrossRef]
- Milajerdi, A.; Ebrahimi-Daryani, N.; Dieleman, L.A.; Larijani, B.; Esmaillzadeh, A. Association of Dietary Fiber, Fruit, and Vegetable Consumption with Risk of Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Adv. Nutr. 2021, 12, 735–743. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Azizi, F. Fast Food Pattern and Cardiometabolic Disorders: A Review of Current Studies. Health Promot. Perspect. 2016, 5, 231–240. [Google Scholar] [CrossRef]
- Ejtahed, H.-S.; Mardi, P.; Hejrani, B.; Mahdavi, F.S.; Ghoreshi, B.; Gohari, K.; Heidari-Beni, M.; Qorbani, M. Association between junk food consumption and mental health problems in adults: A systematic review and meta-analysis. BMC Psychiatry 2024, 24, 438. [Google Scholar] [CrossRef]
- Mareschal, J.; Douissard, J.; Genton, L. Physical activity in inflammatory bowel disease: Benefits, challenges and perspectives. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhang, M.; Liu, Y.; Ge, C.; Lu, Y.; Shen, H.; Zhu, L. Prevalence of metabolic syndrome in patients with inflammatory bowel disease: A systematic review and meta-analysis. BMJ Open 2024, 14, e074659. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Deng, T.; Huang, Y.; Yang, W.; Yang, J.; Song, G. Association between 23 drugs and inflammatory bowel disease: A two-sample Mendelian randomization study. Front. Med. 2024, 11, 1371362. [Google Scholar] [CrossRef]
- Mumena, W.A.; Ateek, A.A.; Alamri, R.K.; Alobaid, S.A.; Alshallali, S.H.; Afifi, S.Y.; Aljohani, G.A.; Kutbi, H.A. Fast-food consumption, dietary quality, and dietary intake of adolescents in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 15083. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Ulcerative Colitis | Crohn’s Disease | Control | |
|---|---|---|---|---|
| Number of Participants | 158 | 244 | 395 | |
| Age, years, % | <30 | 20.3 | 33.2 | 17.7 |
| 30–39 | 34.8 | 44.3 | 43.0 | |
| ≥40 | 44.9 | 22.5 | 35.3 | |
| Sex, % | Men | 58.9 | 68.0 | 64.8 |
| Women | 41.1 | 32.0 | 35.2 | |
| Body mass index, kg/m2, % | <18.5 | 8.9 | 18.4 | 9.4 |
| 18.5–24.9 | 45.6 | 51.2 | 30.4 | |
| 25.0–29.9 | 23.4 | 20.5 | 28.9 | |
| ≥30 | 22.1 | 9.9 | 31.3 | |
| Current smoking, % | 11.4 | 18.9 | 20.8 | |
| Anemia, % | 43.7 | 22.1 | 15.4 | |
| Elevated liver enzymes, % | 15.2 | 11.1 | 19.0 | |
| Fast Food Consumption | Ulcerative Colitis n = 158 | Control n = 395 | Model I | Model II |
|---|---|---|---|---|
| Daily, % | 50.5% | 19.7% | 6.29 (3.89, 10.16) | 6.61 (3.93, 11.12) |
| Infrequent, % | 49.5% | 80.3% | 1 (Reference) | 1 (Reference) |
| Fast food consumption | Crohn’s disease | Control | Model I | Model II |
| Daily, % | 61.3% | 19.7% | 5.92 (3.98, 8.80) | 5.90 (3.89, 8.94) |
| Infrequent, % | 38.7% | 80.3% | 1 (Reference) | 1 (Reference) |
| Study ID | Study Design | Population | Fast Food Assessment Method, Categories, and Retrospective Period | Covariates or Matched Variables |
|---|---|---|---|---|
| Almofarreh (2025) Saudi Arabia | Case-control | 158 UC patients, 244 CD patients, and 395 without IBD (≥18 years) from a private clinic in Riyadh | Self-administered questionnaire Fast food (daily vs. infrequent) A few weeks before diagnosis | Age, sex, BMI, smoking, anemia, and liver enzymes |
| Qualqili (2021) Jordan [26] | Case-control | 100 UC patients, 85 CD patients, and 150 without IBD (18–68 years) from the University of Jordan Hospital, Zarqa Governmental Hospital, and Al Bashir Hospital | Interview Fast food (1–3 times per week vs. infrequent) 3 months before diagnosis | Age and marital status |
| DeClercq (2018) Canada [27] | Cross-sectional | 119 UC patients, 111 CD patients, and 12,462 without IBD (30–74 years) from the Atlantic Partnership for Tomorrow’s Health study | Self-administered questionnaire Fast food (2–5 times/week vs. no) 1 year before enrolment | Age, sex, and residence |
| Niewiadomski (2016) Australia [28] | Case-control | 51 UC patients, 81 CD patients, and 104 without IBD (11–76 years) from specialists, hospitals, pharmacies, and pathology centres in Melbourne, Victoria | Self-administered questionnaire Fast food (yes vs. no) 6 months before diagnosis | None |
| Persson (1992) Sweden [29] | Case-control | 181 UC patients, 184 CD patients, and 390 without IBD (15–79 years) from hospital admissions of Stockholm County | Self-administered questionnaire Fast food (≥2 times/week vs. no) 1–4 years before diagnosis | Age and sex |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almofarreh, A.; Sheerah, H.A.; Arafa, A.; AlBassam, A.M.; Alassaf, M.A.; AlBassam, F.M.; Alsaif, F.B.; Alkwai, K.M.; Alzahrani, F.A.; Allift, M.A.; et al. The Association Between Fast Food Consumption and Inflammatory Bowel Disease: A Case-Control Study and Meta-Analysis. Nutrients 2025, 17, 1838. https://doi.org/10.3390/nu17111838
Almofarreh A, Sheerah HA, Arafa A, AlBassam AM, Alassaf MA, AlBassam FM, Alsaif FB, Alkwai KM, Alzahrani FA, Allift MA, et al. The Association Between Fast Food Consumption and Inflammatory Bowel Disease: A Case-Control Study and Meta-Analysis. Nutrients. 2025; 17(11):1838. https://doi.org/10.3390/nu17111838
Chicago/Turabian StyleAlmofarreh, Anas, Haytham A. Sheerah, Ahmed Arafa, Abdulatif M. AlBassam, Mshari A. Alassaf, Faisal M. AlBassam, Faisal B. Alsaif, Khalid M. Alkwai, Faisal A. Alzahrani, Mohammed A. Allift, and et al. 2025. "The Association Between Fast Food Consumption and Inflammatory Bowel Disease: A Case-Control Study and Meta-Analysis" Nutrients 17, no. 11: 1838. https://doi.org/10.3390/nu17111838
APA StyleAlmofarreh, A., Sheerah, H. A., Arafa, A., AlBassam, A. M., Alassaf, M. A., AlBassam, F. M., Alsaif, F. B., Alkwai, K. M., Alzahrani, F. A., Allift, M. A., AlBassam, S., AlBassam, A., Alshehri, M., Alshammari, K. O., Alenezi, N. M., & Alamri, F. A. (2025). The Association Between Fast Food Consumption and Inflammatory Bowel Disease: A Case-Control Study and Meta-Analysis. Nutrients, 17(11), 1838. https://doi.org/10.3390/nu17111838