
Effectiveness of a Postpartum Breastfeeding Support Group Intervention in Promoting Exclusive Breastfeeding and Perceived Self-Efficacy: A Multicentre Randomized Clinical Trial
 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
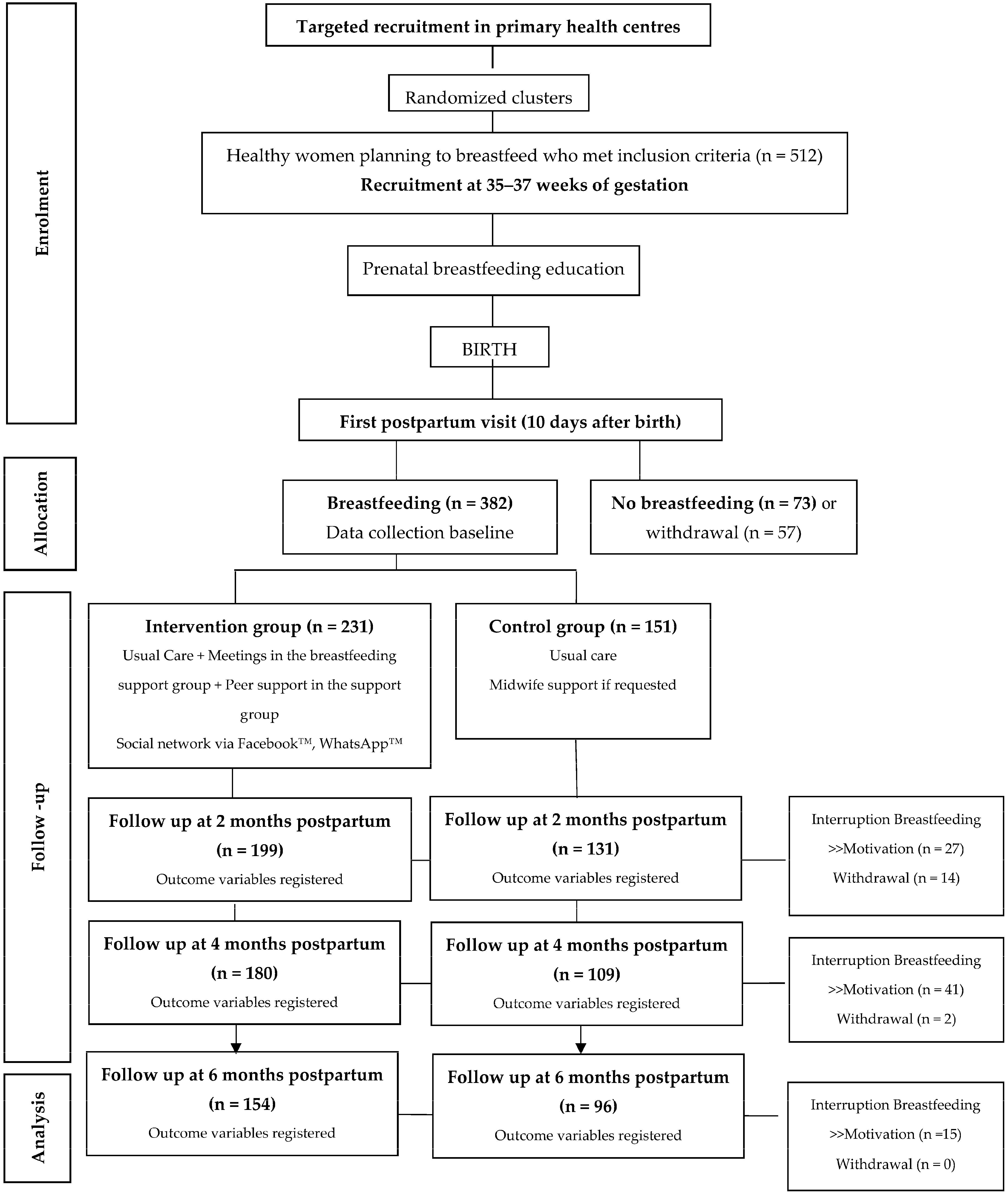
2.2. Participants and Study Area
2.3. Sample Design
2.4. Inclusion and Exclusion Criteria
- Healthy women performing exclusive or partial breastfeeding 10 days after birth who attended antenatal lessons at the primary health centre.
- Women over 18 years of age.
- Women who accepted and signed the informed consent form.
- Human immunodeficiency virus-positive.
- Cancer.
- Tuberculosis infection.
- No intention to breastfeed.
- Impossibility or contraindication to breastfeed due to medical conditions.
- Premature and/or complicated labour or newborn in a neonatal intensive care unit during the first month of life.
- Communication difficulties due to language barriers.
2.5. Randomization
2.6. Study Intervention
2.7. Instrument with Validity and Reliability
- Exclusive breastfeeding: the newborn is fed only with breast milk, without using any other milk or food, from its birth up until the first 6 months of its corrected age.
- Partial breastfeeding: occasional administration of formula milk.
- Mixed breastfeeding: combination of breast and formula milk.
- Artificial breastfeeding: exclusively formula milk.
2.8. Data Collection
2.9. Data Analysis
2.10. Ethical Considerations
3. Results
3.1. Characteristics of the Sample
3.2. Effectiveness of the Intervention in Influencing the Type of Breastfeeding
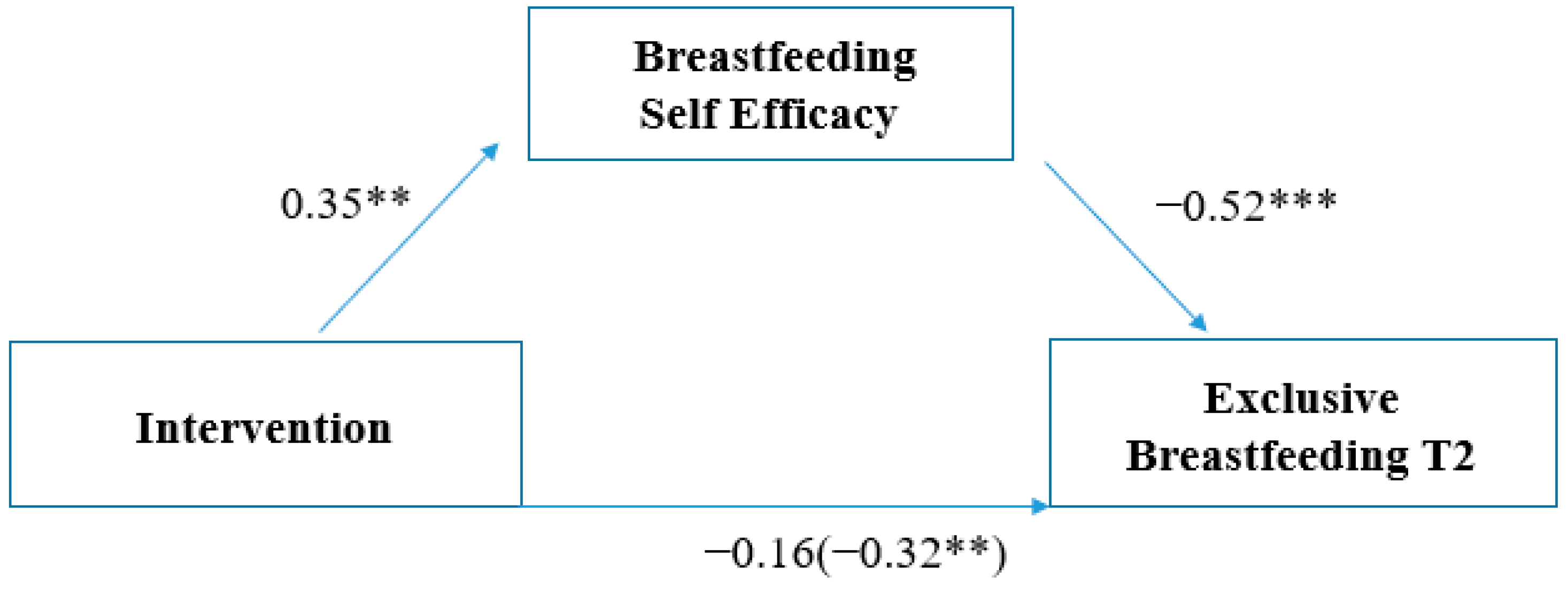
3.3. Effectiveness of the Intervention in Promoting Exclusive Breastfeeding
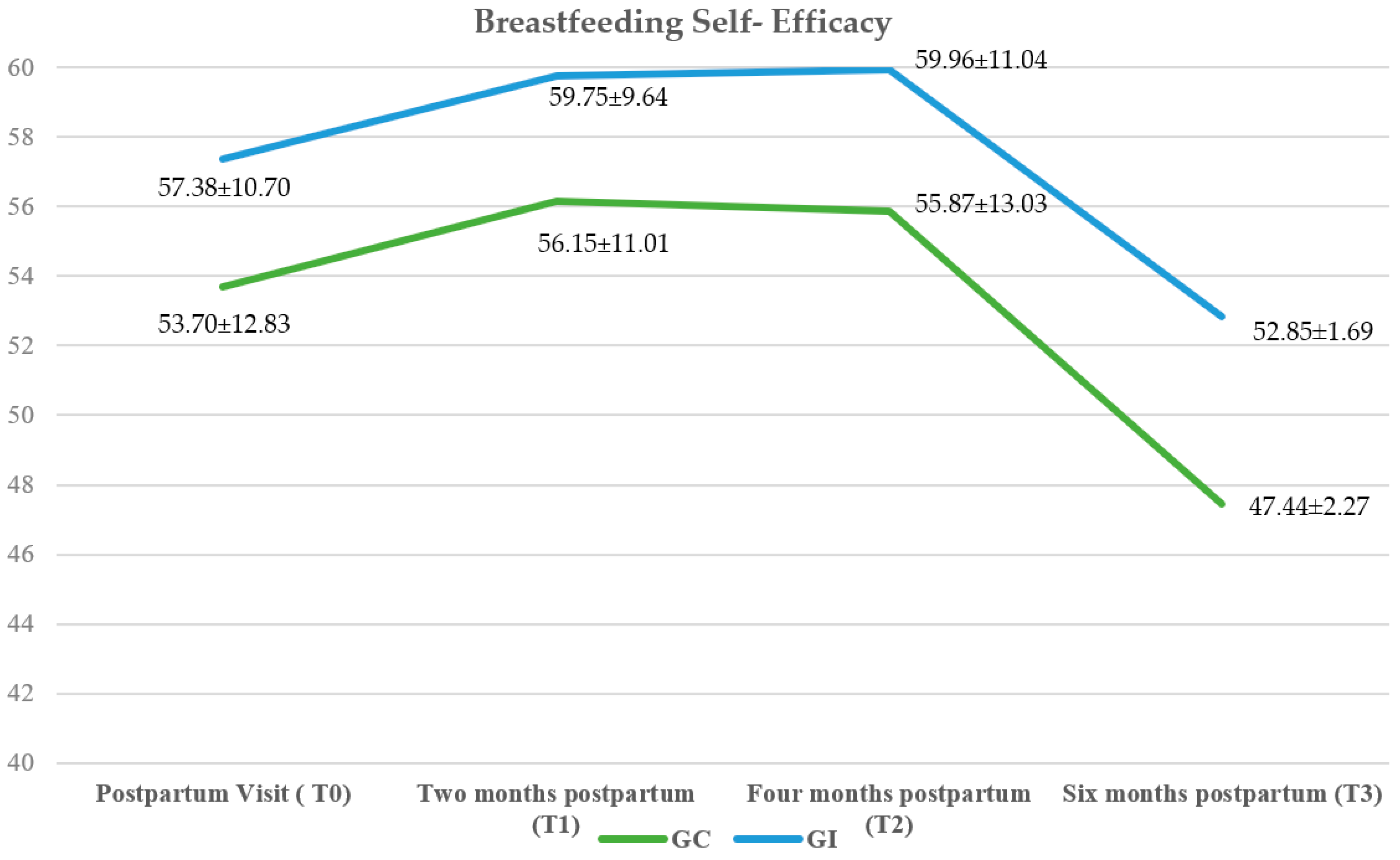
3.4. Breastfeeding Self-Efficacy
3.5. Early Cessation of Breastfeeding
3.6. Employment and Breastfeeding
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Organización Mundial de la Salud. Lactancia Materna Exclusiva. Available online: https://www.who.int/news/item/15-01-2011-exclusive-breastfeeding-for-six-months-best-for-babies-everywhere (accessed on 25 July 2023).
- Organización Mundial de la Salud, UNICEF. Estrategia Mundial para la Alimentación del Lactante y el Niño Pequeño; Organización Mundial de la Salud: Geneva, Switzerland, 2003; Available online: https://www.paho.org/es/documentos/estrategia-mundial-para-alimentacion-lactante-nino-pequeno-1 (accessed on 25 July 2023).
- Alzate-Meza, M.C.; Arango, C.; Castaño-Castrillón, J.J.; Henao-Hurtado, A.M.; Lozano-Acosta, M.; Muñoz-Salazar, G.; Ocampo-Muñoz, N.A.; Rengifo-Calderón, S.V.; Tovar-Orozco, L.M.; Vallejo-Chávez, S.H. Lactancia materna como factor protector para enfermedades prevalentes en niños hasta de 5 años de edad en algunas instituciones educativas de Colombia 2009. Estudio de corte transversal. Rev. Colomb. Obstet. Ginecol. 2011, 62, 57–63. [Google Scholar] [CrossRef]
- Woodward, L.J.; Liberty, K.A. Enciclopedia Sobre el Desarrollo de la Primera Infancia: Lactancia Materna y Desarrollo Psicosocial del Niño. 2017. Available online: https://www.enciclopedia-infantes.com/pdf/expert/lactancia-materna/segun-los-expertos/lactancia-materna-y-desarrollo-psicosocial-del-nino (accessed on 20 July 2023).
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 96–113. [Google Scholar] [CrossRef] [PubMed]
- Tschiderer, L.; Seekircher, L.; Kunutsor, S.K.; Peters, S.A.E.; O’Keeffe, L.M.; Willeit, P. Breastfeeding Is Associated with a Reduced Maternal Cardiovascular Risk: Systematic Review and Meta-Analysis Involving Data from 8 Studies and 1 192 700 Parous Women. J. Am. Heart Assoc. 2022, 11, e022746. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Norat, T.; Romundstad, P.; Vatten, L.J. Breastfeeding and the maternal risk of type 2 diabetes: A systematic review and dose-response meta-analysis of cohort studies. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 107–115. [Google Scholar] [CrossRef]
- Dias, C.C.; Figueiredo, B. Breastfeeding and depression: A systematic review of the literature. J. Affect. Disord. 2015, 171, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M. Breastfeeding in the Modern World. Ann. Nutr. Metab. 2022, 78, 29–38. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Clinical Management of COVID-19: Interim Guidance (27 May 2020); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Comité de Lactancia Materna; Asociación Española de Pediatría. Tasas de Inicio y Duración de Lactancia Materna en España y Otros Países. AEP, 2016. Available online: https://www.aeped.es/sites/default/files/documentos/201602-lactancia-materna-cifras.pdf (accessed on 25 July 2023).
- From the First Hour of Life: Making the Case for Improved Infant and Young Child Feeding Everywhere. United Nations Children’s Fund UNICEF, 2016. Available online: https://www.unicef.org/media/49801/file/From-the-first-hour-of-life-ENG.pdf (accessed on 25 July 2023).
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G.; Lancet Breastfeeding Series Group. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Cabedo, R.; Manresa, M.; Cambredó, M.V.; Montero, L.; Reyes, A.; Gol, R.; Falguera, G. Tipos de lactancia materna y factores que influyen en su abandono hasta los 6 meses. Estudio LACTEM. Matronas Prof. 2019, 20, 54–61. [Google Scholar]
- Renfrew, M.J.; McCormick, F.M.; Wade, A.; Quinn, B.; Dowswell, T. Support for healthy breastfeeding mothers with healthy term babies. Cochrane Database Syst. Rev. 2012, 5, CD001141. [Google Scholar] [CrossRef]
- Imdad, A.; Yakoob, M.Y.; Siddiqui, S.; Bhutta, Z.A. Screening and triage of intrauterine growth restriction (IUGR) in general population and high risk pregnancies: A systematic review with a focus on reduction of IUGR related stillbirths. BMC Public Health 2011, 11, S1. [Google Scholar] [CrossRef]
- Srinivas, G.; Benson, M.; Worley, S.; Schulte, E. A clinic-based breastfeeding peer counselor intervention in an urban, low-income population: Interaction with breastfeeding attitude. J. Hum. Lact. 2015, 31, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, S.; Oh, J.; Kim, J.; Ahn, S. Interventions promoting exclusive breastfeeding up to six months after birth: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2018, 80, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Chan, W.C.; Zhou, X.; Ye, B.; He, H.G. Predictors of breast feeding self-efficacy among Chinese mothers: A cross-sectional questionnaire survey. Midwifery 2014, 30, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Marco, T.D.; Martínez, D.; Muñoz, M.J.; Sayas, I.; Oliver-Roig, A.; Richart-Martínez, M. Valores de referencia españoles para la versión reducida de la Escala de Autoeficacia para la Lactancia Materna BSES-SF [Spanish reference values for the Breastfeeding Self-Efficacy Scale-Short Form BSES-SF]. An. Sist. Sanit. Navar. 2014, 37, 203–211. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mercan, Y.; Tari Selcuk, K. Association between postpartum depression level, social support level and breastfeeding attitude and breastfeeding self-efficacy in early postpartum women. PLoS ONE 2021, 16, e0249538. [Google Scholar] [CrossRef]
- Brockway, M.; Benzies, K.; Hayden, K.A. Interventions to Improve Breastfeeding Self-Efficacy and Resultant Breastfeeding Rates: A Systematic Review and Meta-Analysis. J. Hum. Lact. 2017, 33, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Amer, S.; Kateeb, E. Mothers’ Employment and Exclusive Breastfeeding Practices: A Brief Report from Jerusalem Governorate. Int. J. Environ. Res. Public Health 2023, 20, 2066. [Google Scholar] [CrossRef]
- López de Aberasturi, A.; Santos, N.; Ramos, Y.; García, M.; Artola, C.; Arara, I. Prevalencia y determinantes de la lactancia materna: Estudio Zorrotzaurre [Prevalence and determinants of breastfeeding: The Zorrotzaurre study]. Nutr. Hosp. 2021, 38, 50–59. (In Spanish) [Google Scholar] [CrossRef]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Cayón-De Las Cuevas, J.; Llorca, J.; Cabero-Pérez, M.J. Declared Reasons for Cessation of Breastfeeding during the First Year of Life: An Analysis Based on a Cohort Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8414. [Google Scholar] [CrossRef]
- Real Decreto-Ley 6/2019, de 1 de Marzo, de Medidas Urgentes para Garantía de la Igualdad de Trato y de Oportunidades Entre Mujeres y Hombres en el Empleo y la Ocupación. (Boletín Oficial del Estado, Número 57, de 7 de Marzo de 2019). Available online: https://www.boe.es/eli/es/rdl/2019/03/01/6/con (accessed on 25 July 2023).
- Rodríguez-Gallego, I.; Leon-Larios, F.; Ruiz-Ferrón, C.; Lomas-Campos, M.D. Evaluation of the impact of breastfeeding support groups in primary health CENTRES in Andalusia, Spain: A study protocol for a cluster randomized controlled trial (GALMA project). BMC Public Health 2020, 20, 1129, Erratum in BMC Public Health 2020, 20, 1445. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Oficina Estadística Española. Registro INE 2021. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=2915 (accessed on 20 July 2023).
- Instituto Nacional de Estadística. Oficina Estadística Española. Registro INE 2022. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=1433#!tabs-tabla (accessed on 20 July 2023).
- Instituto Nacional de Estadística (INE). Series Detalladas Desde 2002. Población Residente por Fecha, Sexo, Grupo de Edad y Nacionalidad (Agrupación de Países). Oficina Estadística Española. Registro INE 2023. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=56942 (accessed on 20 July 2023).
- Instituto Nacional de Estadística (INE). Movimiento Natural de la Población: Nacimientos. Fenómenos Demográficos por Comunidades y Ciudades Autónomas y Tipo de Fenómeno Demográfico. Oficina Estadística Española. Registro INE 2022. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=6567 (accessed on 20 July 2023).
- Ministerio de Sanidad. Encuesta Nacional de Salud de España 2017 (ENSE 2017). Determinantes de Salud. Tipo de Lactancia. Tabla 3.078. Según Sexo y Clase Social Basada en la Ocupación de la Persona de Referencia 2017. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_MOD3_REL.pdf (accessed on 20 July 2023).
- Nabulsi, M.; Hamadeh, H.; Tamim, H.; Kabakian, T.; Charafeddine, L.; Yehya, N.; Sinno, D.; Sidani, S. A complex breastfeeding promotion and support intervention in a developing country: Study protocol for a randomized clinical trial. BMC Public Health 2014, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Guillaumes, S.; O’Callaghan, C. Versión en español del software gratuito OxMaR para minimización y aleatorización de estudios clínicos. Gac. Sanit. 2019, 33, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Aceituno, L.; Maldonado, J.; Arribas, L.; Caño, A.; Corona, I.; Martín, J.E.; Mora, M.A.; Morales, L.; Ras, J.; Sánchez, T.; et al. Embarazo, Parto y Puerperio. Proceso Asistencial Integrado, 3rd ed.; Consejería De Igualdad, Salud y Políticas Sociales: Junta de Andalucía, Spain, 2014; pp. 24–46. [Google Scholar]
- Organización Mundial de la Salud, UNICEF. Consejería en Lactancia Materna: Curso de Capacitación; WHO: Geneva, Switzerland, 1993. [Google Scholar]
- World Health Organization, UNICEF. Protecting, Promoting, and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services: The Revised Baby-Friendly Hospital Initiative 2018; Implementation Guidance; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Robinson, A.; Lauckner, C.; Davis, M.; Hall, J.; Anderson, A.K. Facebook support for breastfeeding mothers: A comparison to offline support and associations with breastfeeding outcomes. Digit. Health 2019, 5, 2055207619853397. [Google Scholar] [CrossRef]
- Oliver-Roig, A.; d’Anglade-González, M.L.; García-García, B.; Silva-Tubio, J.R.; Richart-Martínez, M.; Dennis, C.L. The Spanish version of the Breastfeeding Self-Efficacy Scale-Short Form: Reliability and validity assessment. Int. J. Nurs. Stud. 2012, 49, 169–173. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, version 23.0; IBM Corp.: Armonk, NY, USA, 2018. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2013. [Google Scholar]
- Jenkins, L.A.; Barnes, K.; Latter, A.; Edwards, R.A. Examining the Baby Café Model and Mothers’ Breastfeeding Duration, Meeting of Goals, and Exclusivity. Breastfeed. Med. 2020, 15, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Schreck, P.K.; Solem, K.; Wright, T.; Schulte, C.; Ronnisch, K.J.; Szpunar, S. Both Prenatal and Postnatal Interventions Are Needed to Improve Breastfeeding Outcomes in a Low-Income Population. Breastfeed. Med. 2017, 12, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Moudi, S.; Tafazoli, M.; Boskabadi, H.; Ebrahimzadeh, S.; Salehiniya, H. Comparing the effect of breastfeeding promotion interventions on exclusive breastfeeding: An experimental study. Biomed. Res. Ther. 2016, 3, 910–927. [Google Scholar] [CrossRef]
- Wagg, A.J.; Callanan, M.M.; Hassett, A. Online social support group use by breastfeeding mothers: A content analysis. Heliyon 2019, 5, e01245. [Google Scholar] [CrossRef]
- Regan, S.; Brown, A. Experiences of online breastfeeding support: Support and reassurance versus judgement and misinformation. Matern. Child Nutr. 2019, 15, e12874. [Google Scholar] [CrossRef]
- Cavalcanti, D.S.; Cabral, C.S.; de Toledo Vianna, R.P.; Osório, M.M. Online participatory intervention to promote and support exclusive breastfeeding: Randomized clinical trial. Matern. Child Nutr. 2019, 15, e12806. [Google Scholar] [CrossRef]
- Wilson, J.C. Using Social Media for Breastfeeding Support. Nurs. Women’s Health 2020, 24, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, A.; Howell, B.; Romme, K.; Gao, Z.; Nguyen, H.; Allwood Newhook, L.A.; Twells, L. The Effectiveness of Virtual Lactation Support: A Systematic Review and Meta-Analysis. J. Hum. Lact. 2022, 38, 452–465. [Google Scholar] [CrossRef]
- Wong, M.S.; Mou, H.; Chien, W.T. Effectiveness of educational and supportive intervention for primiparous women on breastfeeding related outcomes and breastfeeding self-efficacy: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 117, 103874. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Gallego, I.; Strivens-Vilchez, H.; Agea-Cano, I.; Marín-Sánchez, C.; Sevillano-Giraldo, M.D.; Gamundi-Fernández, C.; Berná-Guisado, C.; Leon-Larios, F. Breastfeeding experiences during the COVID-19 pandemic in Spain: A qualitative study. Int. Breastfeed. J. 2022, 17, 11. [Google Scholar] [CrossRef] [PubMed]
- Clapton-Caputo, E.; Sweet, L.; Muller, A. A qualitative study of expectations and experiences of women using a social media support group when exclusively expressing breastmilk to feed their infant. Women Birth 2021, 34, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Skelton, K.R.; Evans, R.; LaChenaye, J.; Amsbary, J.; Wingate, M.; Talbott, L. Exploring Social Media Group Use among Breastfeeding Mothers: Qualitative Analysis. JMIR Pediatr. Parent. 2018, 1, e11344. [Google Scholar] [CrossRef]
- Black, R.; McLaughlin, M.; Giles, M. Women’s experience of social media breastfeeding support and its impact on extended breastfeeding success: A social cognitive perspective. Br. J. Health Psychol. 2020, 25, 754–771. [Google Scholar] [CrossRef]
- Uzunçakmak, T.; Gökşin, İ.; Ayaz-Alkaya, S. The effect of social media-based support on breastfeeding self-efficacy: A randomised controlled trial. Eur. J. Contracept. Reprod. Health Care 2022, 27, 159–165. [Google Scholar] [CrossRef]
- De Roza, J.G.; Fong, M.K.; Ang, B.L.; Sadon, R.B.; Koh, E.Y.L.; Teo, S.S.H. Exclusive breastfeeding, breastfeeding self-efficacy and perception of milk supply among mothers in Singapore: A longitudinal study. Midwifery 2019, 79, 102532. [Google Scholar] [CrossRef]
- Wu, D.S.; Hu, J.; McCoy, T.P.; Efird, J.T. The effects of a breastfeeding self-efficacy intervention on short-term breastfeeding outcomes among primiparous mothers in Wuhan, China. J. Adv. Nurs. 2014, 70, 1867–1879. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.Y.; Ip, W.Y.; Choi, K.C. The effect of a self-efficacy-based educational programme on maternal breast feeding self-efficacy, breast feeding duration and exclusive breast feeding rates: A longitudinal study. Midwifery 2016, 36, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Franco-Antonio, C.; Calderón-García, J.F.; Santano-Mogena, E.; Rico-Martín, S.; Cordovilla-Guardia, S. Effectiveness of a brief motivational intervention to increase the breastfeeding duration in the first 6 months postpartum: Randomized controlled trial. J. Adv. Nurs. 2020, 76, 888–902. [Google Scholar] [CrossRef]
- Blyth, R.; Creedy, D.K.; Dennis, C.L.; Moyle, W.; Pratt, J.; De Vries, S.M. Effect of maternal confidence on breastfeeding duration: An application of breastfeeding self-efficacy theory. Birth 2002, 29, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Awano, M.; Shimada, K. Development and evaluation of a self care program on breastfeeding in Japan: A quasi-experimental study. Int. Breastfeed. J. 2010, 5, 9. [Google Scholar] [CrossRef]
- Ansari, S.; Abedi, P.; Hasanpoor, S.; Bani, S. The Effect of Interventional Program on Breastfeeding Self-Efficacy and Duration of Exclusive Breastfeeding in Pregnant Women in Ahvaz, Iran. Int. Sch. Res. Not. 2014, 2014, 510793. [Google Scholar] [CrossRef]
- Shariat, M.; Abedinia, N.; Noorbala, A.A.; Zebardast, J.; Moradi, S.; Shahmohammadian, N.; Karimi, A.; Abbasi, M. Breastfeeding Self-Efficacy as a Predictor of Exclusive Breastfeeding: A Clinical Trial. Iran. J. Neonatol. 2018, 9, 26–34. [Google Scholar] [CrossRef]
- Tseng, J.F.; Chen, S.R.; Au, H.K.; Chipojola, R.; Lee, G.T.; Lee, P.H.; Shyu, M.L.; Kuo, S.Y. Effectiveness of an integrated breastfeeding education program to improve self-efficacy and exclusive breastfeeding rate: A single-blind, randomised controlled study. Int. J. Nurs. Stud. 2020, 111, 103770. [Google Scholar] [CrossRef] [PubMed]
- Chipojola, R.; Chiu, H.Y.; Huda, M.H.; Lin, Y.M.; Kuo, S.Y. Effectiveness of theory-based educational interventions on breastfeeding self-efficacy and exclusive breastfeeding: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2020, 109, 103675. [Google Scholar] [CrossRef]
- Franco-Antonio, C.; Santano-Mogena, E.; Sánchez-García, P.; Chimento-Díaz, S.; Cordovilla-Guardia, S. Effect of a brief motivational intervention in the immediate postpartum period on breastfeeding self-efficacy: Randomized controlled trial. Res. Nurs. Health 2021, 44, 295–307. [Google Scholar] [CrossRef]
- Maleki-Saghooni, N.; Amel, M.; Moeindarbari, S.; Fatemeh, Z.K. Investigating the Breastfeeding Self-Efficacy and its Related Factors in Primiparous Breastfeeding Mothers. Int. J. Pediatr. 2017, 5, 6275–6283. [Google Scholar] [CrossRef]
- Efrat, M.W. Breastfeeding Self-Efficacy and Level of Acculturation among Low-Income Pregnant Latinas. Int. J. Child Health Nutr. 2018, 7, 169–174. [Google Scholar] [CrossRef]
- Brockway, M.; Benzies, K.M.; Carr, E.; Aziz, K. Breastfeeding self-efficacy and breastmilk feeding for moderate and late preterm infants in the Family Integrated Care trial: A mixed methods protocol. Int. Breastfeed. J. 2018, 13, 29. [Google Scholar] [CrossRef] [PubMed]
- Brockway, M.; Benzies, K.M.; Carr, E.; Aziz, K. Does breastfeeding self-efficacy theory apply to mothers of moderate and late preterm infants? A qualitative exploration. J. Clin. Nurs. 2020, 29, 2872–2885. [Google Scholar] [CrossRef] [PubMed]
- Bartle, N.C.; Harvey, K. Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. Br. J. Health Psychol. 2017, 22, 763–785. [Google Scholar] [CrossRef]
- Morrison, A.H.; Gentry, R.; Anderson, J. Mothers’ Reasons for Early Breastfeeding Cessation. MCN Am. J. Matern. Child Nurs. 2019, 44, 325–330. [Google Scholar] [CrossRef]
- Colin, W.B.; Scott, J.A. Breastfeeding: Reasons for starting, reasons for stopping and problems along the way. Breastfeed. Rev. 2002, 10, 13–19. [Google Scholar] [PubMed]
- Odom, E.C.; Li, R.; Scanlon, K.S.; Perrine, C.G.; Grummer-Strawn, L. Reasons for earlier than desired cessation of breastfeeding. Pediatrics 2013, 131, e726–e732. [Google Scholar] [CrossRef]
- Ramiro, M.D.; Ortiz, H.; Arana, C.; Esparza, M.J.; Cortés, O.; Terol, M.; Ordovás, M. Prevalencia de la lactancia materna y factores asociados con el inicio y la duración de la lactancia materna exclusiva en la Comunidad de Madrid entre los participantes en el estudio ELOIN [Prevalence of breastfeeding and factors associated with the start and duration of exclusive breastfeeding in the Community of Madrid among participants in the ELOIN]. An. Pediatr. (Engl. Ed.) 2018, 89, 32–43. (In Spanish) [Google Scholar] [CrossRef]
- Castetbon, K.; Boudet-Berquier, J.; Salanave, B. Combining breastfeeding and work: Findings from the Epifane population-based birth cohort. BMC Pregnancy Childbirth 2020, 20, 110. [Google Scholar] [CrossRef]
- Santos, M.N.; Azeredo, C.M.; Rinaldi, A.E.M. Association Between Maternal Work and Exclusive Breastfeeding in Countries of Latin America and Caribbean. Matern. Child Health J. 2022, 26, 1496–1506. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.Y. Shift-work and breastfeeding for women returning to work in a manufacturing workplace in Taiwan. Int. Breastfeed. J. 2022, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.A.; Silva, C.M.; Costa, E.M.; Ferreira, M.J.; Abuchaim, E.S.V. Continued breastfeeding and work: Scenario of maternal persistence and resilience. Rev. Bras. Enferm. 2023, 76, e20220191. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 382) | Group | χ2 | t | p-Value | |
|---|---|---|---|---|---|---|
| Intervention (n = 231) | Control (n = 151) | |||||
| Baseline | ||||||
| Maternal age, years; mean ± SD | 33.41 ± 4.66 | 33.50 ± 4.41 | 33.28 ± 5.03 | −0.45 | 0.64 | |
| Nationality, n (%) | 0.14 | 0.70 | ||||
| Spanish | 357 (93.45) | 215 (93.07) | 142 (94.03) | |||
| Other | 25 (6.54) | 16 (6.92) | 9 (5.96) | |||
| Education level, n (%) | 0.81 | 0.84 | ||||
| Without | 1 (0.26) | 1 (0.4) | 0 (0) | |||
| Primary studies | 11 (3.66) | 9 (3.9) | 5 (3.3) | |||
| Secondary studies | 121 (31.67) | 74 (32) | 47 (31.1) | |||
| University studies | 246 (64.39) | 147 (63.6) | 99 (65.6) | |||
| Employment, n (%) | 2.08 | 0.35 | ||||
| Employed | 273 (71.46) | 165 (71.4) | 108 (71.5) | |||
| Unemployed | 109 (28.53) | 66 (28.6) | 43 (28.5) | |||
| Work hours (per week), n (%) | 34.46 | 0.44 | ||||
| <20 | 97 (25.39) | 57 (34.5) | 40 (37.0) | |||
| 20–30 | 75 (19.63) | 44 (40.7) | 31 (28.7) | |||
| >20 | 57 (14.92) | 33 (20) | 24 (22.2) | |||
| Gestation, weeks; mean ± SD | 39.45 ± 1.25 | 39.45 ± 1.14 | 39.46 ± 1.38 | 0.13 | 0.89 | |
| Home labour and delivery (%) | 0.13 | 0.71 | ||||
| Induced | 151 (39.52) | 61 (40.4) | 90 (59.6) | |||
| Spontaneous | 231 (60.47) | 89 (38.5) | 142 (61.5) | |||
| Mode of delivery, n (%) | 2.88 | 0.41 | ||||
| Eutocic | 236 (61.78) | 140 (60.6) | 96 (63.6) | |||
| Dystocic | 77 (20.15) | 51 (22.1) | 26 (17.2) | |||
| SCS | 17 (4.45) | 12 (5.2) | 5 (3.3) | |||
| UCS | 52 (13.61) | 28 (12.1) | 24 (15.9) | |||
| Infant sex, n (%) | 0.16 | 0.68 | ||||
| Male | 195 (51.04) | 116 (50.2) | 79 (52.3) | |||
| Female | 187 (48.95) | 115 (49.8) | 72 (47.7) | |||
| Newborn weight, g; mean ± SD | 3262.58 ± 463.76 | 3239.10 ± 483.92 | 3298.51 ± 430.19 | 1.22 | 0.22 | |
| Previous breastfeeding experience, n (%) | 1.42 | 0.23 | ||||
| Yes | 161 (42.14) | 103 (44.6) | 58 (38.4) | |||
| No | 221 (57.85) | 128 (55.4) | 93 (61.6) | |||
| Type of Breastfeeding | Time Postpartum | |||||||
|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | |||||
| Group | Group | Group | Group | |||||
| IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | |
| Exclusive breastfeeding | 180 (77.9) | 118 (78.1) | 144 (72.4) | 85 (64.9) | 125 (69.4) | 56 (51.4) | 98 (63.4) | 46 (47.9) |
| z-value | −0.1 | 0.1 | 1.4 | −1.4 | 3.1 | −3.1 | 2.4 | −2.4 |
| Breastfeeding with occasional help | 31 (13.4) | 20 (13.2) | 18 (9) | 14 (10.7) | 22 (11.7) | 12 (11.0) | 16 (10.4) | 11 (11.5) |
| z-value | 0.0 | 0.0 | −0.5 | 0.5 | 0.2 | −0.2 | −0.3 | 0.3 |
| Breastfeeding mixed | 20 (8.7) | 13 (8.6) | 24 (12.1) | 18 (13.7) | 14 (7.8) | 20 (18.3) | 32 (21.4) | 30 (31.3) |
| z-value | 0.0 | 0.0 | −0.4 | 0.4 | −2.7 | 2.7 | −1.7 | 1.7 |
| Artificial breastfeeding | -- | -- | 13 (6.5) | 14 (10.7) | 20 (11.1) | 21 (19.3) | 7 (4.5) | 9 (9.4) |
| z-value | −1.3 | 1.3 | −1.9 | 1.9 | −1.5 | 1.5 | ||
| 95% Confidence Interval | ||||||
|---|---|---|---|---|---|---|
| β | t | p | Lower | Upper | ||
| Direct effect | Intervention ➝ Exclusive breastfeeding T2 | −0.16 | −1.77 | 0.78 | −0.34 | −0.18 |
| Total effect | Intervention ➝ Exclusive breastfeeding T2 | −0.32 | −3.15 | 0.00 | −0.53 | −0.12 |
| Effect on mediator | Intervention ➝ Breastfeeding self-efficacy | 0.35 | 2.77 | 0.005 | 0.10 | 0.60 |
| Effect by mediator | Breastfeeding self-efficacy ➝ Exclusive breastfeeding T2 | −0.52 | −12.55 | <0.001 | −0.60 | −0.44 |
| Employment | Type of Breastfeeding | χ2 (df) | p-Value | V | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Exclusive Breastfeeding (%) | Breastfeeding with Occasional Help (%) | Breastfeeding Mixed (%) | Artificial Breastfeeding (%) | ||||||||
| Group | Group | Group | Group | ||||||||
| IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | ||||
| Paid maternity leave | 58 (77.3) | 28 (50.9) | 4 (5.3) | 6 (10.9) | 5 (6.7) | 8 (14.5) | 8 (10.7) | 13 (23.6) | 9.90 (3) | 0.01 | 0.28 |
| z-value | 3.1 | −3.1 | −1.2 | 1.2 | −1.5 | 1.5 | −2.0 | 2.0 | |||
| Active duty mothers | 36 (69.2) | 11 (52.4) | 10 (19.2) | 2 (9.5) | 3 (5.8) | 5 (23.8) | 3 (5.8) | 3 (14.3) | 6.7 (3) | 0.07 | 0.31 |
| z-value | −0.1 | −1.5 | 1.9 | −0.9 | −0.4 | 2.2 | −1.4 | 1.2 | |||
| Unemployed | 31 (62) | 17 (56.7) | 8 (16) | 4 (13.3) | 6 (12) | 7(23.3) | 5 (10) | 2(6.7) | 1.9 (3) | 0.6 | 0.15 |
| z-value | 0.5 | −0.5 | 0.3 | −0.3 | −1.3 | 1.3 | 0.5 | −0.5 | |||
| Employment | Type of Breastfeeding | χ2 (df) | p-Value | V | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Exclusive Breastfeeding (%) | Breastfeeding with Occasional Help (%) | Breastfeeding Mixed (%) | Artificial Breastfeeding (%) | ||||||||
| Group | Group | Group | Group | ||||||||
| IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | IG n (%) | CG n (%) | ||||
| Paid maternity leave | 17 (89.5) | 10 (66.7) | -- | 3 (20) | 2 (10.5) | 2 (13.3) | -- | -- | 4.40 (2) | 0.11 | 0.36 |
| z-value | 1.6 | −1.6 | −2.0 | 2.0 | −0.3 | 0.3 | -- | -- | |||
| Active duty mothers | 56 (60.0) | 23 (45.1) | 11 (12) | 5 (9.8) | 21 (22.8) | 17 (33.3) | 4 (4.3) | 6 (11.8) | 5.55 (3) | 0.13 | 0.2 |
| z-value | 1.8 | −1.8 | 0.4 | −0.4 | −1.4 | 1.4 | −1.7 | 1.7 | |||
| Unemployed | 24 (60) | 13 (44.8) | 5 (12.5) | 3 (10.3) | 8 (20) | 10 (34.5) | 3 (7.5) | 3 (10.3) | 2.3 (3) | 0.51 | 0.18 |
| z-value | 1.2 | −1.2 | 0.3 | −0.3 | 1.4 | 1.4 | −0.4 | 0.4 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Gallego, I.; Corrales-Gutierrez, I.; Gomez-Baya, D.; Leon-Larios, F. Effectiveness of a Postpartum Breastfeeding Support Group Intervention in Promoting Exclusive Breastfeeding and Perceived Self-Efficacy: A Multicentre Randomized Clinical Trial. Nutrients 2024, 16, 988. https://doi.org/10.3390/nu16070988
Rodríguez-Gallego I, Corrales-Gutierrez I, Gomez-Baya D, Leon-Larios F. Effectiveness of a Postpartum Breastfeeding Support Group Intervention in Promoting Exclusive Breastfeeding and Perceived Self-Efficacy: A Multicentre Randomized Clinical Trial. Nutrients. 2024; 16(7):988. https://doi.org/10.3390/nu16070988
Chicago/Turabian StyleRodríguez-Gallego, Isabel, Isabel Corrales-Gutierrez, Diego Gomez-Baya, and Fatima Leon-Larios. 2024. "Effectiveness of a Postpartum Breastfeeding Support Group Intervention in Promoting Exclusive Breastfeeding and Perceived Self-Efficacy: A Multicentre Randomized Clinical Trial" Nutrients 16, no. 7: 988. https://doi.org/10.3390/nu16070988
APA StyleRodríguez-Gallego, I., Corrales-Gutierrez, I., Gomez-Baya, D., & Leon-Larios, F. (2024). Effectiveness of a Postpartum Breastfeeding Support Group Intervention in Promoting Exclusive Breastfeeding and Perceived Self-Efficacy: A Multicentre Randomized Clinical Trial. Nutrients, 16(7), 988. https://doi.org/10.3390/nu16070988