
The Effects of Online Home-Based Pilates Combined with Diet on Body Composition in Women Affected by Obesity: A Preliminary Study

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
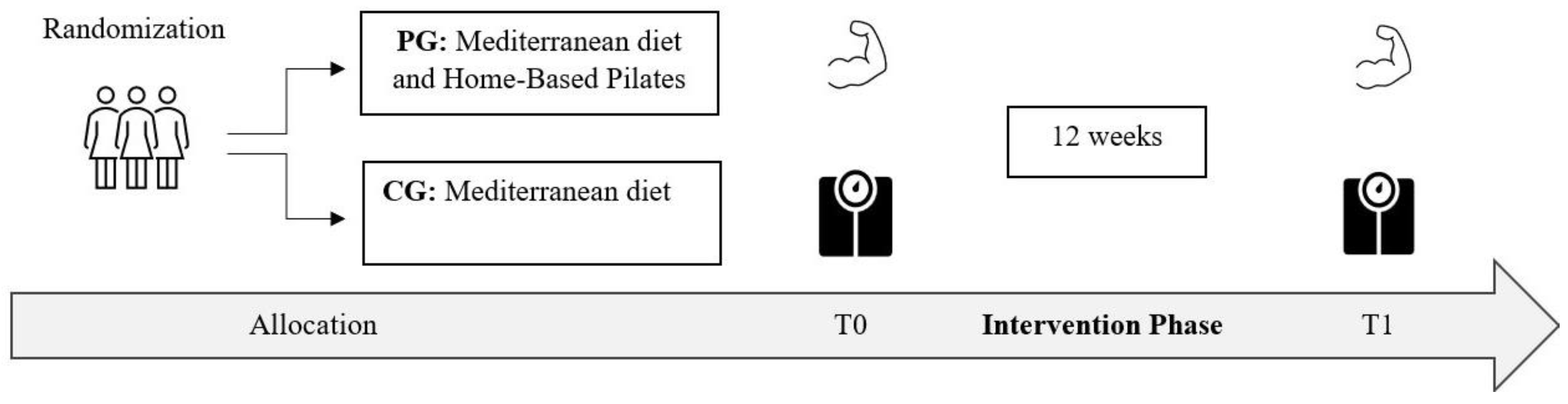
2.1. Study Design
2.2. Participants
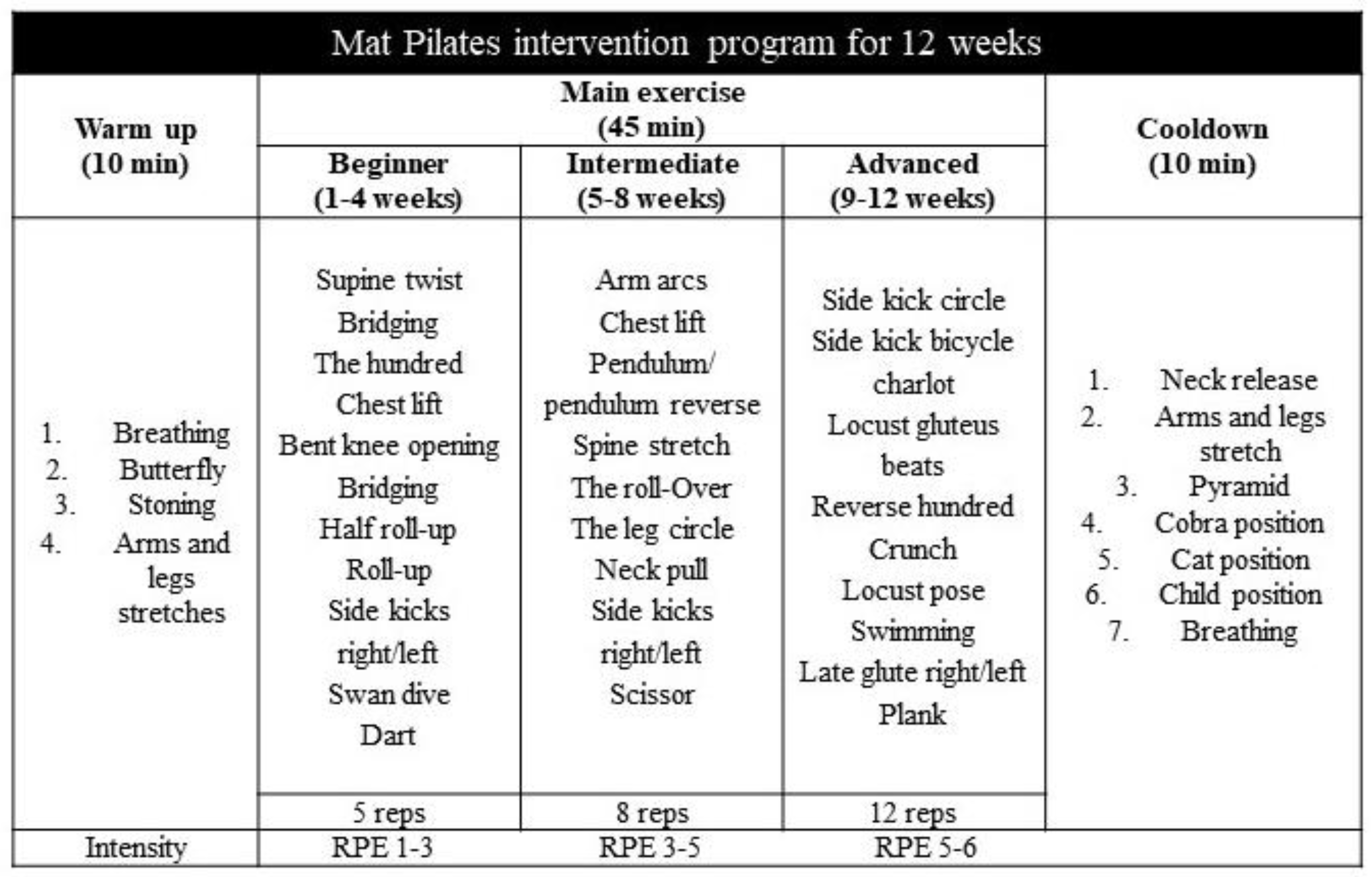
2.3. Diet and Exercise Program
2.4. Physical Fitness Assessments
- Height was measured barefoot to the nearest 0.1 cm using a stadiometer (SECA, Intermed S.r.l., Milano, Italy). Participants stood with their body mass evenly distributed on both feet, heels together, and head positioned in a midline position (Frankfort horizontal plane), with their arms hanging loosely. To obtain a reliable measurement, participants were asked to inhale deeply and stretch to their full height. Three measurements of height were carried out.
- Body mass and body composition were measured using a bioelectrical impedance method (BIA ACCUNIQ 360, Daejeon, Republic of Korea) while participants wore minimal clothing and removed any metal accessories before the analysis was conducted. After entering the participant’s height, date of birth, and gender into the device, their body mass was automatically measured. During the measurement, participants stood in an upright position, with arms at about a 30° angle away from the trunk. This position was maintained until the end of the measurement, and no talking or movements were allowed. The variables of interest were the body mass index (BMI = body mass (kg)/height2 (m)2), the fat mass (pFM) expressed as a percentage of body mass, the fat-free mass (FFM) expressed in kilograms, and the appendicular skeletal muscle mass (ASMM) and skeletal muscle mass (SMM) expressed in kilograms. Body composition assessments were always conducted in the morning and at the same time during the day. Participants were asked to refrain from eating or drinking 3 to 4 h before the assessment.
- A handgrip strength test (HGS) was used to evaluate the maximum isometric strength of the hand and forearm muscles utilizing a handgrip dynamometer (Jamar Hydraulic Hand Dynamometer, Sammons Preston Rolyan, Bolingbrook, IL, USA) [25]. Participants were instructed to squeeze the dynamometer with their hand as hard as possible for three seconds, maintaining the elbow at a right angle, while seated on a standard armless chair. The width of the handle was adjusted for each participant according to their hand size (i.e., the middle phalanx on the inner handle). Three trials interspersed with 30 s of rest were performed for each hand, and the mean of the right and left hand results was used for further analysis.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 18 September 2023).
- Merra, G.; Gualtieri, P.; Cioccoloni, G.; Falco, S.; Bigioni, G.; Tarsitano, M.G.; Capacci, A.; Piccioni, A.; Costacurta, M.; Franceschi, F.; et al. FTO rs9939609 influence on adipose tissue localization in the Italian population. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3223–3235. [Google Scholar] [CrossRef] [PubMed]
- Pujia, R.; Tarsitano, M.G.; Arturi, F.; De Lorenzo, A.; Lenzi, A.; Pujia, A.; Montalcini, T. Advances in Phenotyping Obesity and in Its Dietary and Pharmacological Treatment: A Narrative Review. Front. Nutr. 2022, 9, 804719. [Google Scholar] [CrossRef]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; Van Wormer, J.J. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: A systematic review and meta-analysis of randomized clinical trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- de Souza, R.J.; Bray, G.A.; Carey, V.J.; Hall, K.D.; LeBoff, M.S.; Loria, C.M.; Laranjo, N.M.; Sacks, F.M.; Smith, S.R. Effects of 4 weight-loss diets differing in fat, protein, and carbohydrate on fat mass, lean mass, visceral adipose tissue, and hepatic fat: Results from the POUNDS LOST trial. Am. J. Clin. Nutr. 2012, 95, 614–625. [Google Scholar] [CrossRef]
- Anton, S.D.; Karabetian, C.; Naugle, K.; Buford, T.W. Obesity and diabetes as accelerators of functional decline: Can lifestyle interventions maintain functional status in high risk older adults? Exp. Gerontol. 2013, 48, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine; American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Emerenziani, G.P.; Gallotta, M.C.; Migliaccio, S.; Ferrari, D.; Greco, E.A.; Saavedra, F.J.; Iazzoni, S.; Aversa, A.; Donini, L.M.; Lenzi, A.; et al. Effects of an individualized home-based unsupervised aerobic training on body composition and physiological parameters in obese adults are independent of gender. J. Endocrinol. Investig. 2018, 41, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Emerenziani, G.P.; Ferrari, D.; Migliaccio, S.; Lenzi, A.; Greco, E.A.; Marocco, C.; Baldari, C.; Guidetti, L. Effects of body weight loss program on parameters of muscle performance in female obese adults. J. Sports Med. Phys. Fit. 2019, 59, 624–631. [Google Scholar] [CrossRef]
- Olateju, I.V.; Opaleye-Enakhimion, T.; Udeogu, J.E.; Asuquo, J.; Olaleye, K.T.; Osa, E.; Oladunjoye, A.F. A systematic review on the effectiveness of diet and exercise in the management of obesity. Diabetes Metab. Syndr. 2023, 17, 102759. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 18 September 2023).
- Baillot, A.; Chenail, S.; Barros Polita, N.; Simoneau, M.; Libourel, M.; Nazon, E.; Riesco, E.; Bond, D.S.; Romain, A.J. Physical activity motives, barriers, and preferences in people with obesity: A systematic review. PLoS ONE 2021, 16, e0253114. [Google Scholar] [CrossRef]
- Park, H.Y.; Jung, K.; Jung, W.S.; Kim, S.W.; Kim, J.; Lim, K. Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity. Healthcare 2023, 11, 2768. [Google Scholar] [CrossRef] [PubMed]
- Perri, M.G.; Martin, A.D.; Leermakers, E.A.; Sears, S.F.; Notelovitz, M. Effects of group- versus home-based exercise in the treatment of obesity. J. Consult. Clin. Psychol. 1997, 65, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Eliks, M.; Zgorzalewicz-Stachowiak, M.; Zeńczak-Praga, K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: State of the art. Postgrad. Med. J. 2019, 95, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Tian, C.; Wang, Y.; Liang, S.; Wang, Y.; Li, X.; Yang, K. Pilates and multiple health outcomes: An umbrella review. J. Sci. Med. Sport 2023, 26, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Latey, P. The Pilates method: History and philosophy. J. Bodyw. Mov. Ther. 2001, 5, 275–282. [Google Scholar] [CrossRef]
- Niehues, J.R.; Gonzáles, I.; Lemos, R.R.; Haas, P. Pilates Method for Lung Function and Functional Capacity in Obese Adults. Altern. Ther. Health Med. 2015, 21, 73–80. [Google Scholar] [PubMed]
- Şavkin, R.; Aslan, U.B. The effect of Pilates exercise on body composition in sedentary overweight and obese women. J. Sports Med. Phys. Fit. 2017, 57, 1464–1470. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, Z.; Wu, Z.; Ye, X.; Xu, X. Pilates for Overweight or Obesity: A Meta-Analysis. Front. Physiol. 2021, 12, 643455. [Google Scholar] [CrossRef]
- Rayes, A.B.R.; de Lira, C.A.B.; Viana, R.B.; Benedito-Silva, A.A.; Vancini, R.L.; Mascarin, N.; Andrade, M.S. The effects of Pilates vs. aerobic training on cardiorespiratory fitness, isokinetic muscular strength, body composition, and functional tasks outcomes for individuals who are overweight/obese: A clinical trial. PeerJ 2019, 7, e6022. [Google Scholar] [CrossRef]
- Cakmakçi, O. The effect of 8 week pilates exercise on body composition in obese women. Coll. Antropol. 2011, 35, 1045–1050. [Google Scholar]
- Armstrong, T.; Bull, F. Development of the world health organization global physical activity questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Arikawa, A.Y.; O’Dougherty, M.; Schmitz, K.H. Adherence to a strength training intervention in adult women. J. Phys. Act. Health 2011, 8, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Jayedi, A.; Khan, T.A.; Aune, D.; Emadi, A.; Shab-Bidar, S. Body fat and risk of all-cause mortality: A systematic review and dose-response meta-analysis of prospective cohort studies. Int. J. Obes. 2022, 46, 1573–1581. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Braun, W.; Geisler, C.; Norman, K.; Müller, M.J. Body composition and cardiometabolic health: The need for novel concepts. Eur. J. Clin. Nutr. 2018, 72, 638–644. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Fischer, S.M.; Bagheri, R.; Park, S.Y. The Effects of Mat Pilates Training on Vascular Function and Body Fatness in Obese Young Women With Elevated Blood Pressure. Am. J. Hypertens. 2020, 33, 563–569. [Google Scholar] [CrossRef]
- Memelink, R.G.; Hummel, M.; Hijlkema, A.; Streppel, M.T.; Bautmans, I.; Weijs, P.J.M.; Berk, K.A.; Tieland, M. Additional effects of exercise to hypocaloric diet on body weight, body composition, glycaemic control and cardio-respiratory fitness in adults with overweight or obesity and type 2 diabetes: A systematic review and meta-analysis. Diabet. Med. 2023, 40, e15096. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine; American College of Sports Medicine Position Stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Cavina, A.P.S.; Pizzo Junior, E.; Machado, A.F.; Biral, T.M.; Lemos, L.K.; Rodrigues, C.R.D.; Pastre, C.M.; Vanderlei, F.M. Effects of the Mat Pilates Method on Body Composition: Systematic Review With Meta-Analysis. J. Phys. Act. Health 2020, 17, 673–681. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| PG (n = 11) | CG (n = 9) | p-Value * | |
|---|---|---|---|
| Age (years) | 52.0 ± 10.4 | 46.0 ± 6.9 | 0.140 |
| Height (m) | 1.62 ± 0.09 | 1.64 ± 0.09 | 0.502 |
| Body mass (kg) | 82.7 ± 13.3 | 94.2 ± 18.7 | 0.126 |
| BMI (kg/m2) | 31.7 ± 4.0 | 34.9 ± 5.2 | 0.138 |
| T0 | T1 | |
|---|---|---|
| Body mass (kg) | ||
| PG | 82.7 ± 13.3 | 79.5 ± 12.6 |
| CG | 94.2 ± 18.7 | 90.2 ± 15.8 |
| BMI (kg/m2) | ||
| PG | 31.7 ± 4.0 | 30.5 ± 3.9 |
| CG | 34.9 ± 5.2 | 33.3 ± 4.2 |
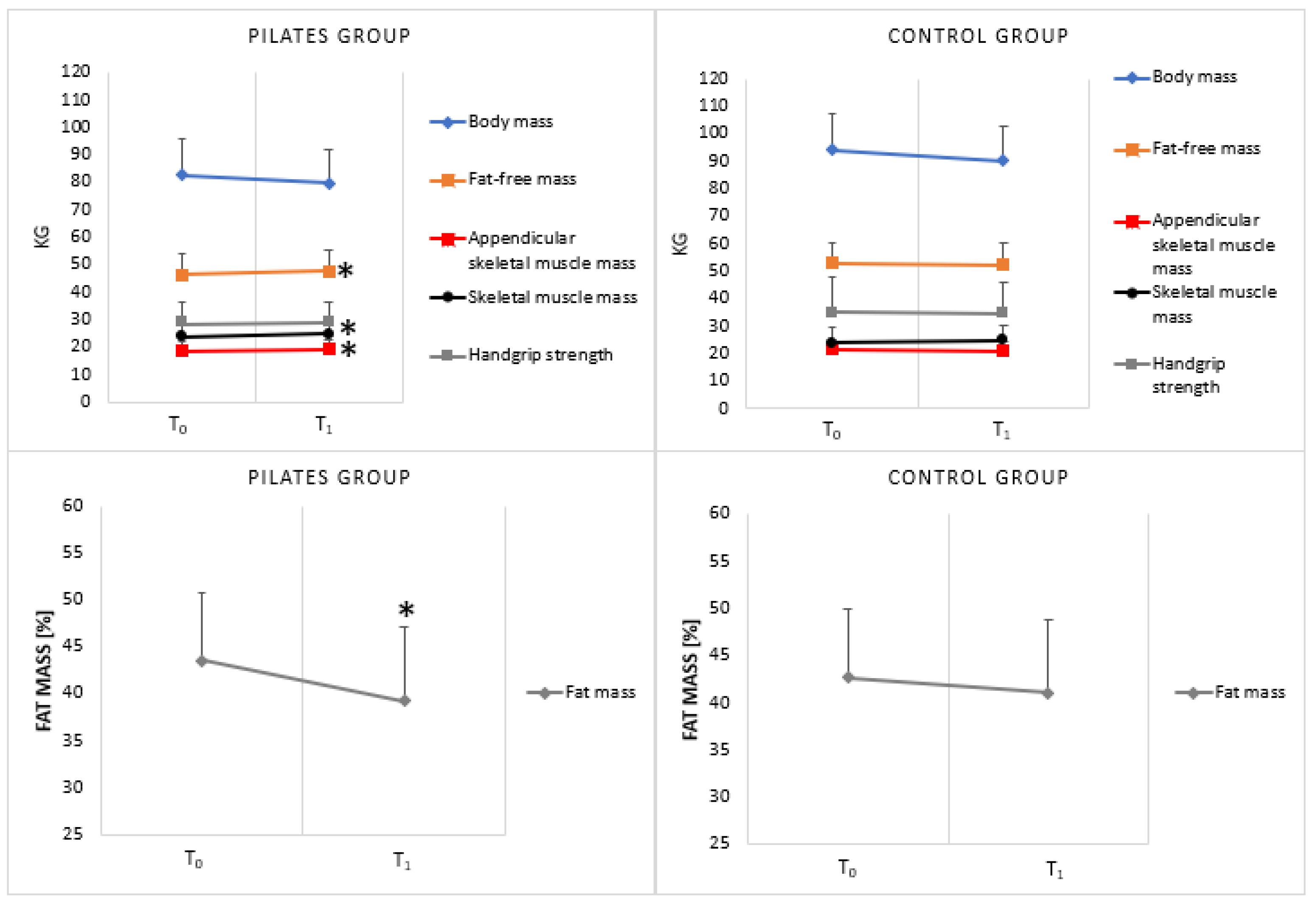
| pFM (%) | ||
| PG | 43.6 ± 7.3 | 39.2 ± 7.9 * |
| CG | 42.7 ± 6.9 | 41.0 ± 6.9 |
| FFM (kg) | ||
| PG | 46.3 ± 7.5 | 47.6 ± 7.6 * |
| CG | 53.1 ± 10.8 | 52.7 ± 10.5 |
| ASMM (kg) | ||
| PG | 18.8 ± 3.3 | 19.4 ± 3.5 * |
| CG | 21.5 ± 4.7 | 21.2 ± 4.7 |
| SMM (kg) | ||
| PG | 23.9 ± 5.7 | 24.9 ± 5.4 * |
| CG | 26.9 ± 7.0 | 26.5 ± 7.2 |
| HGS (kg) | ||
| PG | 28.9 ± 7.3 | 29.0 ± 7.3 |
| CG | 34.9 ± 12.9 | 34.9 ± 11.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, F.; Tarsitano, M.G.; Cosco, L.F.; Quinzi, F.; Folino, K.; Spadafora, M.; Afzal, M.; Segura-Garcia, C.; Maurotti, S.; Pujia, R.; et al. The Effects of Online Home-Based Pilates Combined with Diet on Body Composition in Women Affected by Obesity: A Preliminary Study. Nutrients 2024, 16, 902. https://doi.org/10.3390/nu16060902
Greco F, Tarsitano MG, Cosco LF, Quinzi F, Folino K, Spadafora M, Afzal M, Segura-Garcia C, Maurotti S, Pujia R, et al. The Effects of Online Home-Based Pilates Combined with Diet on Body Composition in Women Affected by Obesity: A Preliminary Study. Nutrients. 2024; 16(6):902. https://doi.org/10.3390/nu16060902
Chicago/Turabian StyleGreco, Francesca, Maria Grazia Tarsitano, Loretta Francesca Cosco, Federico Quinzi, Katia Folino, Marco Spadafora, Moomna Afzal, Cristina Segura-Garcia, Samantha Maurotti, Roberta Pujia, and et al. 2024. "The Effects of Online Home-Based Pilates Combined with Diet on Body Composition in Women Affected by Obesity: A Preliminary Study" Nutrients 16, no. 6: 902. https://doi.org/10.3390/nu16060902
APA StyleGreco, F., Tarsitano, M. G., Cosco, L. F., Quinzi, F., Folino, K., Spadafora, M., Afzal, M., Segura-Garcia, C., Maurotti, S., Pujia, R., Pujia, A., Buono, P., & Emerenziani, G. P. (2024). The Effects of Online Home-Based Pilates Combined with Diet on Body Composition in Women Affected by Obesity: A Preliminary Study. Nutrients, 16(6), 902. https://doi.org/10.3390/nu16060902