1. Introduction
Autism Spectrum Disorder (ASD) is a lifelong neurodevelopmental condition characterized by difficulties in social communication and interaction, complemented by the manifestation of repetitive and restrictive patterns of behaviors or interests [
1]. In recent years, there has been a noticeable rise in reported cases of ASD, particularly with a higher incidence observed among boys compared to girls [
2,
3]. This increase in prevalence could be attributed to several factors, including advancements in diagnostic criteria, improvement in identification and screening techniques, and heightened awareness among both parents and healthcare professionals [
4]. In 2014–2015, the estimated prevalence rate ranged from 49 to 513 children per 10,000 across all regions in Lebanon [
5]. This rapid increase highlights the necessity for a deeper comprehension of the pathophysiology of this disorder, as the exact etiology of ASD is not yet clear. However, several studies have shown that it involves genetic, epigenetic, and environmental factors [
6,
7,
8,
9].
ASD individuals often experience a range of concurrent symptoms, encompassing anxiety, sleep disruptions, gastrointestinal symptoms, epilepsy, and sensory processing difficulties [
10]. These sensory dysfunctions, including either a decreased or increased sensitivity to stimuli like light, sound, taste, smell, texture, and touch, may lead to unhealthy eating habits [
11,
12,
13]. In fact, eating difficulties have been noted in the exploration of ASD [
14] and persist among many individuals with ASD [
15]. The most frequent eating difficulties seen in children with ASD are food selectivity, disruptive mealtime behaviors, and food refusal [
16]. They often manifest in early childhood and persist into adolescence. Children with ASD often exhibit specific dietary preferences, typically favoring foods like meat, fish, eggs, beans, and dairy products, while showing a reluctance towards vegetables, seafood, and fruits [
17,
18]. In severe cases, some may even limit themselves to consuming only liquids or pureed textures [
19]. Therefore, individuals with ASD are more prone to experiencing nutritional inadequacies, which predisposes them to malnutrition [
20]. Interestingly, several studies have indicated a notably higher prevalence of obesity and overweight among children with ASD compared to typically developing children [
21,
22,
23]. Overweight and obesity in children are often attributed to dietary factors, such as a high energy intake and the consumption of fast food, sugary beverages, and snacks. These dietary habits are prevalent not only in children with ASD but also in typically developing children [
24]. However, when it comes to ASD, weight gain has been associated with distinct factors. Numerous studies have identified potential risk factors that may be particularly relevant to children with ASD. These factors include sleep disturbances, a lack of physical activity, motor impairments, the use of antipsychotic medications, genetic predispositions, and food selectivity [
25,
26]. Moreover, it is fundamental to emphasize that this weight gain can have significant health implications, potentially increasing the risk of conditions such as heart disease, diabetes, and insulin resistance [
27].
Assessing the nutritional status of children and adolescents during their developmental stages is essential for the early detection and correction of potential disorders [
28]. Anthropometric methods, such as measuring body weight, height, and circumferences (waist and hips), are commonly employed for this purpose. Additionally, standard anthropometric indicators of body composition, including waist–hip ratio (WHR), waist-to-height ratio (WHtR), and body mass index (BMI), are also utilized [
29]. In pediatric practice, assessments of body weight, height, and BMI are made using percentile charts that take into account age and gender. However, BMI, a frequently used measure for categorizing body weight, has limitations since it does not provide insights into the composition of individual body components, such as body fat, muscle mass, and body water content [
30]. To enhance the monitoring of body weight, it is advisable to employ bioelectrical impedance analysis (BIA), known for its high accuracy and repeatability [
31]. Over the past two decades, bioelectrical impedance analysis (BIA) has experienced rapid growth as a method for assessing human body composition [
32]. BIA, a simple, non-invasive, convenient, and practical method, could be an option for assessing body composition parameters in ASD children and adolescents. It employs electrical currents and impedance to evaluate both fluid status and various body composition parameters, such as muscle tissue, adipose tissue, and body water [
33]. This is especially crucial for adolescents experiencing puberty, a period distinguished by significant shifts in the endocrine system, rapid physical growth, and the emergence of secondary and tertiary sexual traits. These transformations ultimately influence the development of both the morphological and functional aspects of the body [
34].
Although some research has delved into the evaluation of the nutritional status of ASD individuals, there is a lack of studies focusing on their body composition, particularly in Lebanon. However, several studies analyzed the body composition of autistic children and adolescents and indicated a higher incidence of overweight and obesity in this population compared to their peers [
21,
35,
36,
37].
Therefore, our objective was to investigate the anthropometric measures and body composition variables obtained using BIA across different developmental stages, assess the prevalence of obesity and overweight in a group of Lebanese children and adolescents diagnosed with ASD, and investigate the associated risk factors.
2. Materials and Methods
2.1. Study Design, Period, and Setting
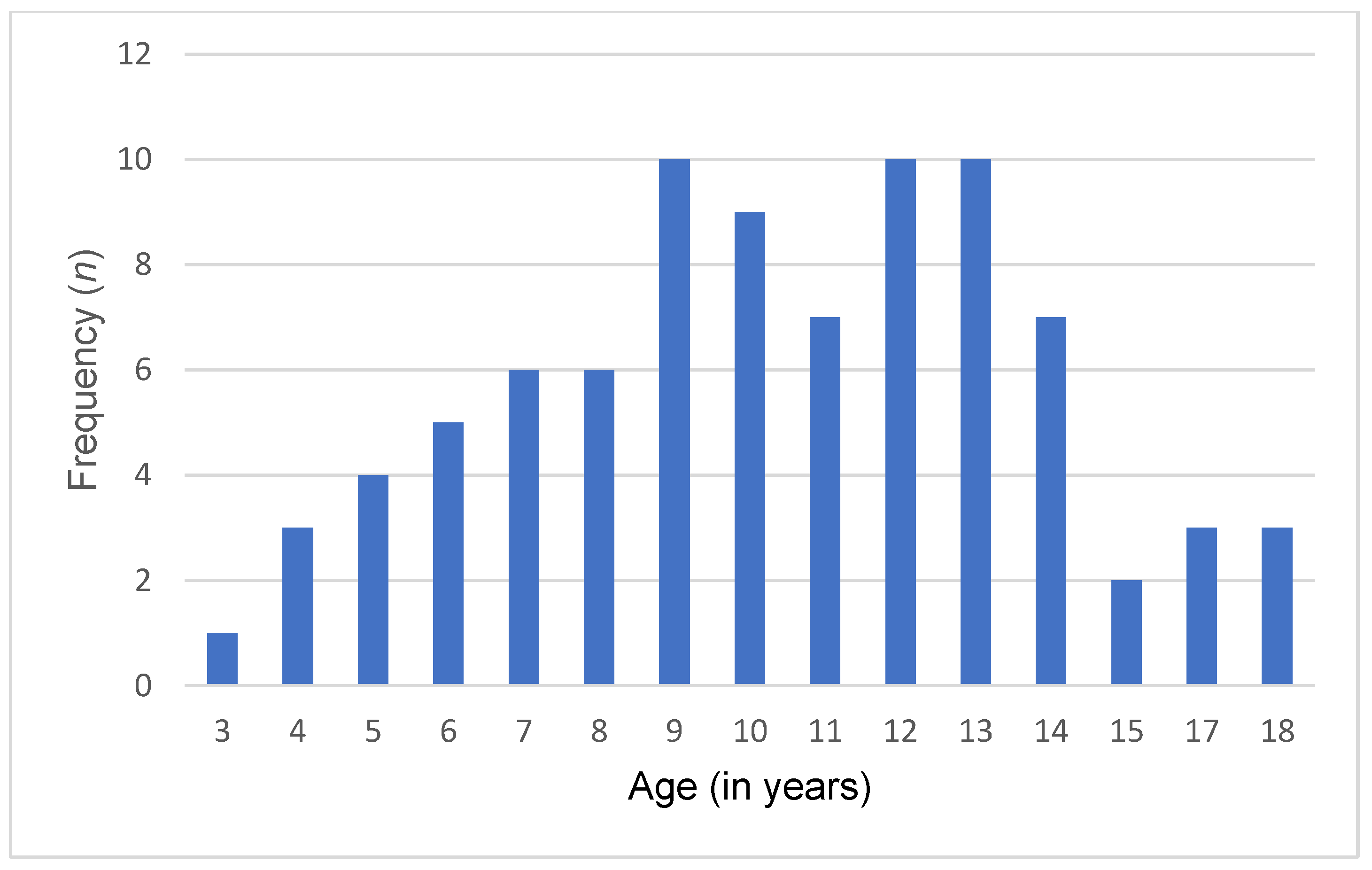
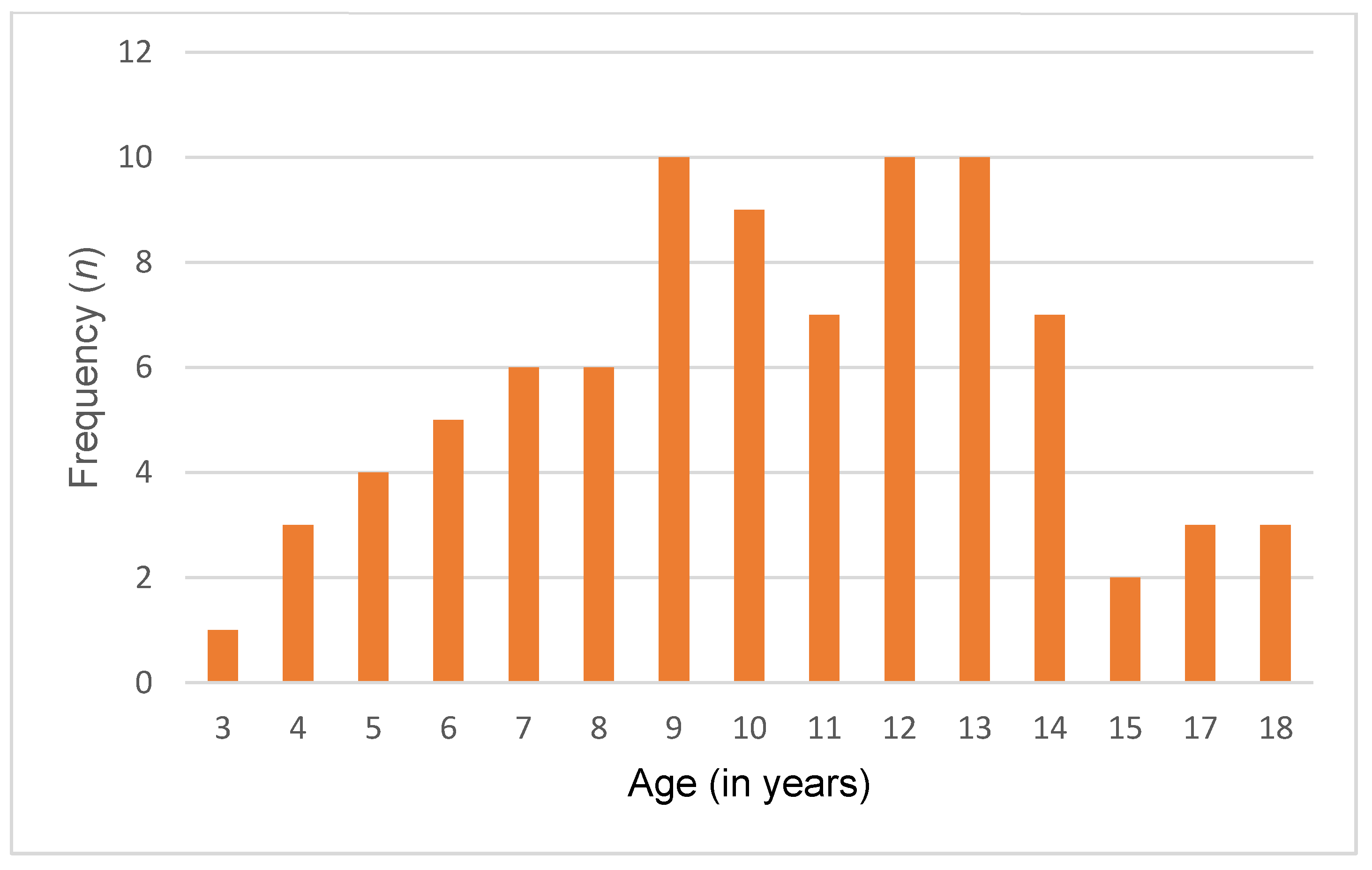
This case–control comparative study was conducted in all districts of Lebanon, with a focus on children and adolescents aged between 3 and 18 years old. Data collection began in June 2022 and ended in June 2023.
2.2. Study Sample
The study sample comprised 86 Lebanese children and adolescents with ASD and 86 typically developing (TD) controls. ASD and TD participants were recruited from specialized institutions, schools, and NGOs located in all districts of Lebanon. Individuals were considered neurotypical if their medical histories and parent or caregiver reports indicated an absence of behavioral difficulties or any sign of motor and language delays. They were matched with individuals diagnosed with ASD in terms of age, gender, and geographic location. The diagnosis of ASD was established on the criteria specified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and confirmed through assessments using the Childhood Autism Rating Scale (CARS). Only individuals whose parents or caregivers provided informed consent were included in this study. The exclusion criteria included the following: children below the age of 3 or above 18, children diagnosed with Down syndrome or fragile X syndrome, the presence of neurological and hormonal disruptions, digestive system diseases, genetic dysfunctions, and the absence of informed consent to participate in the study. Furthermore, severe ASD cases were excluded from this study to ensure the feasibility of conducting body composition assessments.
2.3. Recruitment Process
Invitation and project description letters were sent to all educational institution headmasters. Upon receiving their approval, parents were informed of the objectives and methodology of this study.
2.3.1. Sociodemographic Information
Parents or caregivers met with the investigator so the following participant information could be elicited: child’s age, gender, and residence.
2.3.2. Anthropometric Assessment
A trained and qualified healthcare professional conducted morning measurements for each participant with precision. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer (Numed AHP004, Numed, Beirut, Lebanon), and weight was recorded to the nearest 0.1 kg using a digital platform scale (Amber Body Scale, Numed APAFE002-P4). Participants were barefoot and dressed in lightweight clothing during these evaluations. The body mass index (BMI) was then calculated using Quetelet’s formula (
) and computed via statistical analysis. Moreover, waist circumference (WC) was assessed by placing a Cescorf
® inelastic measuring tape (Cescorf, Porto Alegre, Brazil), calibrated to 1 mm, at the midpoint between the lower rib margin and the iliac crest. The weight-for-age z-score (WAZ), height-for-age z-score (HAZ), and body mass index (BMI)-for-age z-score (BAZ) were computed based on the Center for Disease Control (CDC) growth charts [
38] for 2–20 years of age, illustrated in
Table 1 [
39,
40].
2.3.3. Body Composition Assessment
Body composition parameters were evaluated with a Biodynamic 450® version 5.1 analyzer (Biodynamics Corporation, Seattle, WA, USA) administered by a trained healthcare professional. All assessments were consistently conducted in the early hours, between 7:00 a.m. and 10:00 a.m., ensuring accuracy and uniformity in the data collection process. During the procedure, participants were instructed to lie down with their limbs extended parallel to their body and away from the chest. To ensure accurate readings, ECG (Electrocardiogram) electrodes were positioned at specific locations, including the dorsal surface of the right wrist, the third metacarpal bone, the anterior surface of the right ankle (between bony prominences), and the dorsal surface of the third metatarsal bone. Before initiating the measurement, we recorded crucial demographic information, including gender, age, height, and weight. Once these details were input into the machine, the measurement process began, typically taking approximately 1 min to complete. Patients were provided with instructions to follow before BIA tests: (1) overnight fasting: patients were advised to abstain from consuming food or beverages overnight, usually for a minimum of 8 h before the examination. This fasting period helped minimize the potential impact of recent meals on the results; (2) exercise restriction: to prevent any temporary alterations in body fluid balance due to physical activity, patients were instructed to refrain from exercise for 24 h leading up to the examination; (3) bladder voiding: patients were encouraged to empty their bladders before the BIA tests. This step aimed to reduce any variations in body fluid content that could affect the accuracy of the results.
2.4. Ethical Considerations
This study adhered to the ethical standards and guidelines outlined in the Declaration of Helsinki of 1964 and its subsequent amendments. The study protocol (EC 90010141) underwent review and approval by the Ethics Committee of the Holy Spirit University of Kaslik. Throughout this study, participants were not subjected to any physical or psychological harm. Furthermore, participants’ credentials were treated confidentially, and the study findings were used strictly for academic purposes.
2.5. Statistical Analysis
We used the Statistical Package for Social Sciences 22.0 (SPSS® Inc., Chicago, IL, USA) for statistical analyses. Categorical variables were summarized as frequencies (n) and percentage (%), while continuous variables were presented as mean ± standard deviation. A p-value less than 0.05 was considered statistically significant. After conducting tests for data distribution normality, it was determined that variables such as height, weight-for-age z-score (WAZ), and BMI-for-age z-score (BMIZ) were normally distributed. Consequently, comparisons of these variables between the two groups were performed using independent-sample t-tests. On the other hand, variables such as weight, weight-for-age z-score cut-points (WAZ cut-points), height-for-age z-score (HAZ), height-for-age z-score cut-points (HAZ cut-points), BMI, BMI-for-age z-score cut-points (BMIZ cut-points), waist circumference (WC), fat mass (FM), fat-free mass (FFM), and percentage of body fat (PBF) exhibited non-normal distributions. As a result, the non-parametric Wilcoxon Mann–Whitney test was utilized for comparing these variables between the two groups. Pearson chi-square analysis was used to explore the correlation between age, gender, geographic location, and the occurrence of obesity in ASD. Furthermore, multinomial linear regression analysis was applied to investigate the relationship between age, gender, geographic location, and the likelihood of being overweight and obese.
4. Discussion
The purpose of this study was to examine the differences in anthropometric measures and body composition variables of Lebanese ASD children and adolescents compared to their neurotypical counterparts across various developmental stages. It also investigated the occurrence of unhealthy weight and identified associated risk factors within the ASD population.
Our findings revealed a notable imbalance in gender distribution, with males comprising a larger proportion compared to females (86% vs. 14%, respectively). This observation aligns with prior research indicating a higher prevalence of ASD among males than females [
41,
42]. This disparity in prevalence rates highlights a potential gender bias in the typical presentation of ASD [
43]. This bias may stem from the original development and testing of diagnostic tools primarily with male participants, which could contribute to misdiagnosis in females [
44]. Consequently, females with ASD might need to manifest a higher number of or more severe symptoms to be diagnosed. Moreover, females with ASD often engage in “camouflaging” their autistic symptoms more than males, making it harder to detect their condition [
45]. As a result, many females may be misdiagnosed, experience significant delays in diagnosis, or go undiagnosed altogether, leading to a lack of necessary intervention and support.
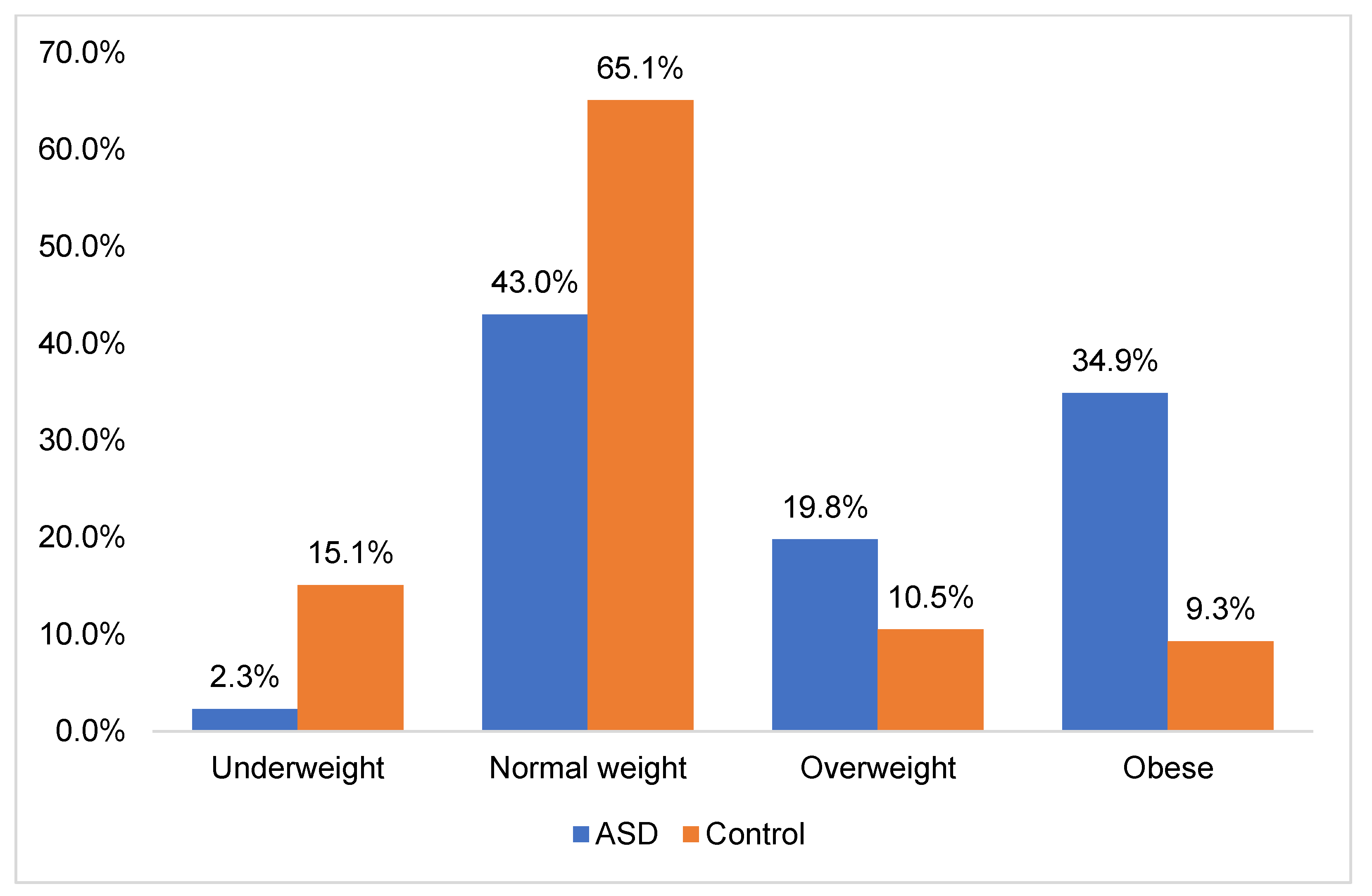
Additionally, we found that individuals with ASD were at a higher risk of developing unhealthy weight compared to their neurotypical counterparts. The occurrence rates of overweight and obesity among this population were alarming, prompting urgent attention to address this growing clinical concern. In fact, our study revealed that 19.8% of ASD participants were classified as overweight, whereas 34.9% were classified as obese. Taken together, this high prevalence emphasizes the critical need for targeted interventions designed to address weight-related health challenges. Interestingly, our findings align with previous studies on the prevalence of overweight and obesity in ASD (
Table 7).
Memari et al. (2012) conducted a study focusing on the weight status of Iranian children and adolescents diagnosed with ASD. Their research revealed that 23.1% of the population were classified as overweight, while 24.1% were categorized as obese [
46]. Similarly, Bicer and Alsaffar et al. (2013) noted an increased susceptibility to overweight and obesity among adolescents with ASD [
47]. Consistent findings were observed by Broder-Fingert et al., indicating that children with ASD exhibited higher rates of overweight and obesity compared to control subjects [
48]. Additionally, Zuckerman et al. assessed the prevalence of overweight and obesity among 376 ASD children, revealing that. 18.1% were classified as overweight and 17% as obese [
49]. Moreover, Healy et al. highlighted that 19.4% were overweight and 23.05 were obese [
51]. The underlying reasons for the high prevalence of overweight and obesity in children with ASD are still not fully understood. Previous studies have highlighted that the increased prevalence of unhealthy weight among children with ASD is often linked to atypical eating patterns [
52]. In fact, children with ASD, often referred to as picky eaters, experience more feeding difficulties compared to typically developing controls [
53]. They tend to eat selectively, demonstrating a preference for starches, fast food, sugary beverages, and snacks over fruits and vegetables [
54]. This dietary preference can predispose them to an imbalanced body composition. Furthermore, reduced physical activity and highly sedentary behavior are key contributors to weight gain and increased BMI [
26]. In fact, children diagnosed with ASD commonly experience motor impairments, which can hinder their engagement in sports and physical activities. These impairments include diminished muscle tone, oral motor challenges, instability in posture, and difficulties in motor skills [
52]. Moreover, challenges in social skills often result in reduced participation in structured activities with peers, further limiting their physical activity [
55]. Additionally, the use of antipsychotic medications, often prescribed for managing ASD symptoms, presents a risk factor for weight gain in this population. The medication linked to the most pronounced weight gain is olanzapine, followed with clozapine, risperidone, and aripiprazole, in ascending order of weight gain severity [
56] (
Table 8).
Genetic factors implicated in obesity, such as 11p14.1 or 16p11.2 microdeletions, may also be prevalent among children diagnosed with ASD [
62]. It is crucial to acknowledge that elevated BMI levels are correlated with adverse health consequences, such as insulin resistance, heart disease, diabetes, and sleep-disordered breathing [
63]. Childhood obesity imposes a significant economic burden on families and can have detrimental effects on physical, emotional, and social well-being, as well as academic performance, potentially exacerbating the challenges posed by ASD-related disability and leading to a diminished quality of life [
26]. In fact, overweight or obese children with ASD are more prone to experience bullying and social isolation [
27]. These findings underscore the imperative need for early intervention and comprehensive support tailored to the unique challenges related to weight and overall health in individuals with ASD.
When analyzing the prevalence of obesity across various age brackets, our study revealed a higher incidence of overweight and obesity among young children aged 3 to 9 years and pre-adolescents aged 10 to 13 years diagnosed with ASD compared to their neurotypical counterparts. Additionally, we found no significant difference in obesity prevalence between adolescents aged 14 to 18 years with ASD and their typically developing peers. These findings contrast with some previous studies. For example, Tybor et al. (2019) noted a significantly higher obesity prevalence among ASD children aged 10 to 17 years compared to those without ASD [
64]. Similarly, McCoy et al. (2019) reported that ASD adolescents aged 10 to 17 years were more likely to exhibit unhealthy weight statuses, including underweight, overweight, and obesity, compared to their typically developing counterparts [
65]. Moreover, Evans et al. (2012) investigated the body mass index of ASD and control individuals aged 3 to 11 years and found no discernible differences in BMI z-scores or BMI cut-points between the two groups [
66]. Furthermore, Barnhill et al. (2017) studied the weight status of ASD children aged 2 to 13 years and reported no significant disparities in BMI categories compared to age-matched controls [
67]. These inconsistencies, particularly observed in adolescence, underscore the necessity for further research to explore the impact of puberty on obesity in individuals with ASD. Understanding how developmental changes influence weight status in this population is crucial for developing tailored interventions.
Furthermore, bioelectrical impedance analysis (BIA) revealed variations in body composition between the two groups across different developmental stages. During childhood and pre-adolescence, individuals with ASD exhibited significantly higher levels of fat mass (FM) and total body fat percentage (PBF) compared controls. Interestingly, these differences were not observed during adolescence. Similarly, the levels of fat-free mass (FFM) showed no significant difference across all age groups. These findings suggest age-related variations in body composition. In fact, younger children and pre-adolescents diagnosed with ASD exhibited a greater proportion of body fat, indicating overweight, necessitating targeted interventions to address dietary habits, physical activity levels, and sensory sensitivities that may influence these outcomes. Throughout adolescence, both individuals with ASD and typically developing controls experience substantial rapid physical growth and hormonal fluctuations [
68]. It may be possible that these changes affect both groups similarly, thereby reducing the observed differences in body composition and anthropometric measurements.
Moreover, we investigated the relationship between sociodemographic characteristics and the occurrence of overweight and obesity in ASD children. Our analysis indicated that variables such as age, gender, and geographic location did not exhibit significant associations with weight status among this population. This finding is consistent with previous studies. In fact, Healy et al. did not identify any correlation between age and the occurrence of obesity in children diagnosed with ASD. Similarly, Sammels et al. found no relationship between the prevalence of obesity and the gender of the children with ASD [
69]. Future research should investigate the association between the occurrence of obesity and several factors, including the severity of ASD diagnosis, medication use, as well as levels of physical activity, dietary habits, and sleep patterns.
We acknowledge several limitations in this study. The first is the relatively smaller sample size of adolescents compared to younger children and pre-adolescents. Factors like medication use, physical activity levels, which could have provided valuable insights, and dietary intake were not evaluated. Additionally, the measurement parameters of BIA are susceptible to variations caused by factors such as physical activity, fluid and food intake, hydration status, and electrode placement methods, potentially leading to inaccuracies in BIA readings [
70]. However, to ensure the accuracy and reliability of our BIA measurements, we implemented stringent protocols. Before testing, participants were advised to fast overnight, empty their bladders, and avoid exercise for 24 h. Therefore, future research should aim to incorporate validated methods for assessing pubertal status, such as Tanner staging or hormone level measurements, to better understand its impact on weight-related outcomes in this population. Moreover, future research could focus on examining the correlation between medication use, physical activity levels, dietary intake, and the prevalence of obesity and overweight in ASD individuals.


 ,
, 

{kind=link}
{kind=link}
{kind=link}