
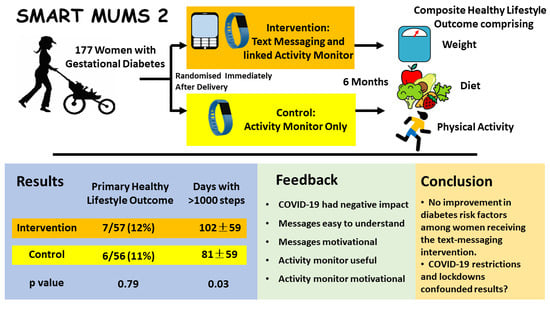
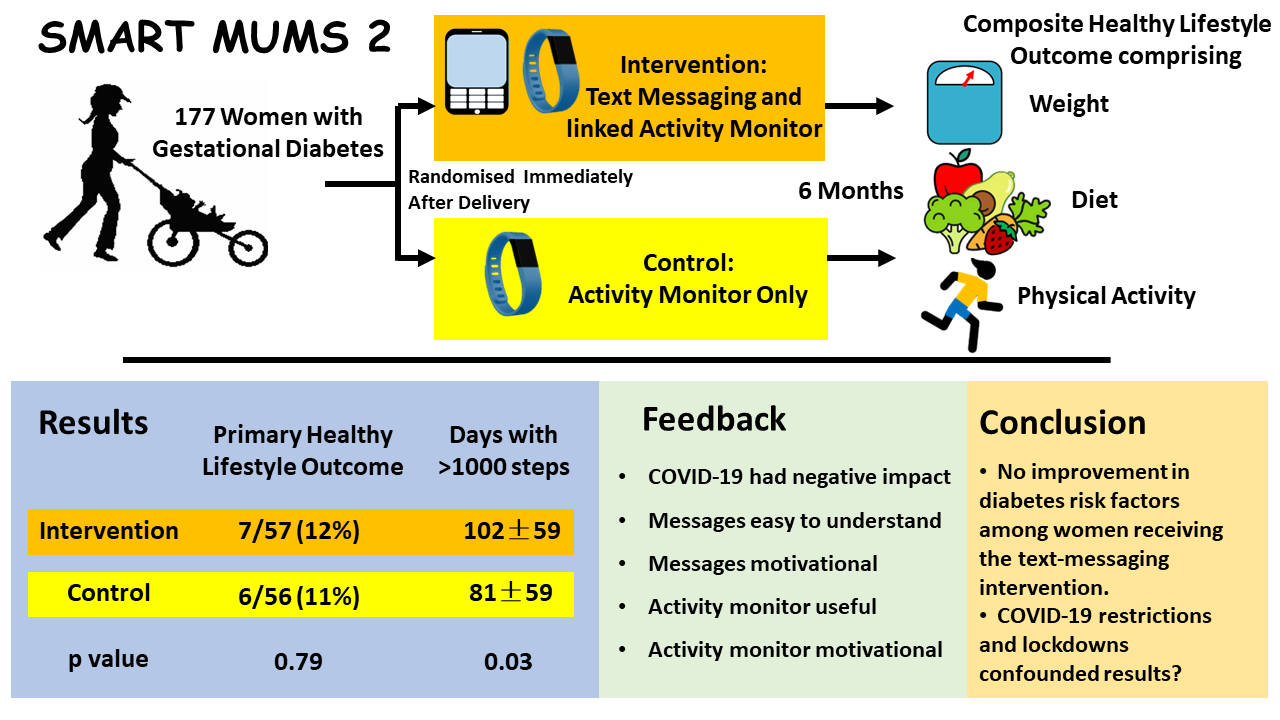
Randomised Controlled Trial of a Customised Text Messaging and Activity Monitor Program for Lifestyle Improvement after Gestational Diabetes


 , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
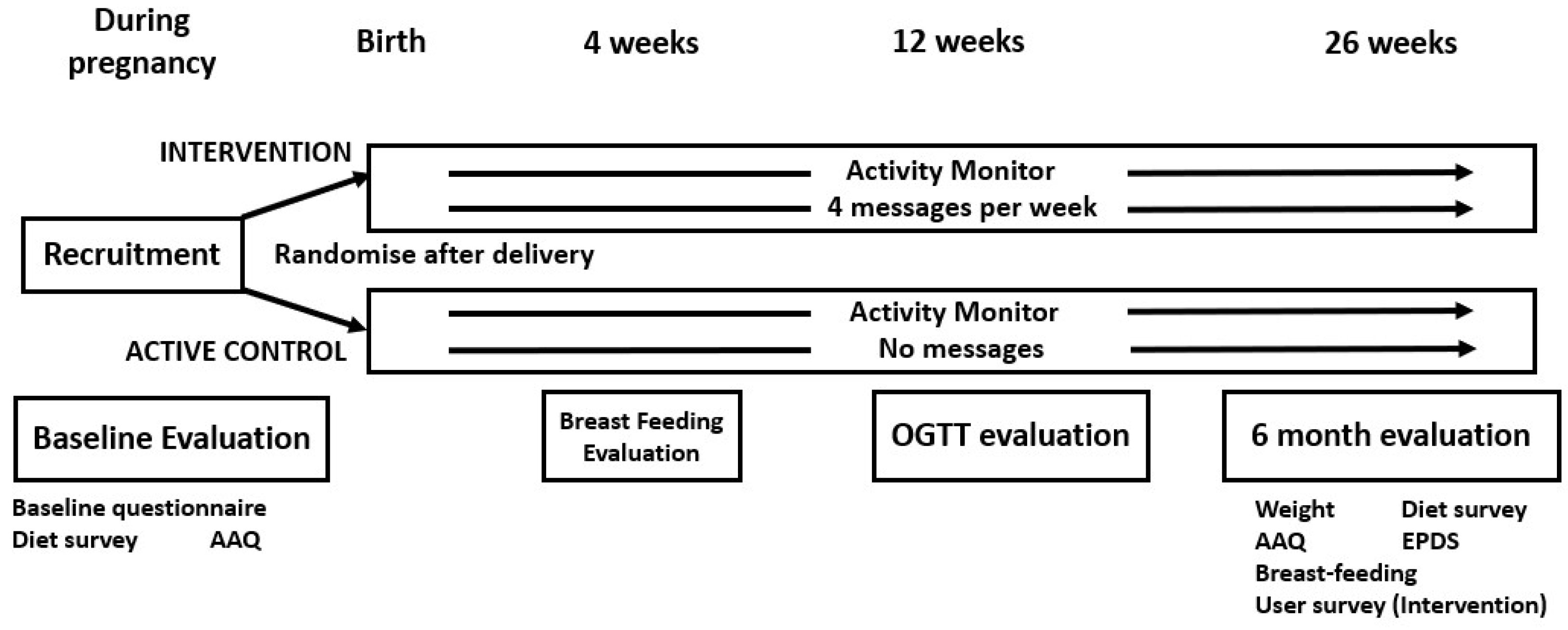
2. Materials and Methods
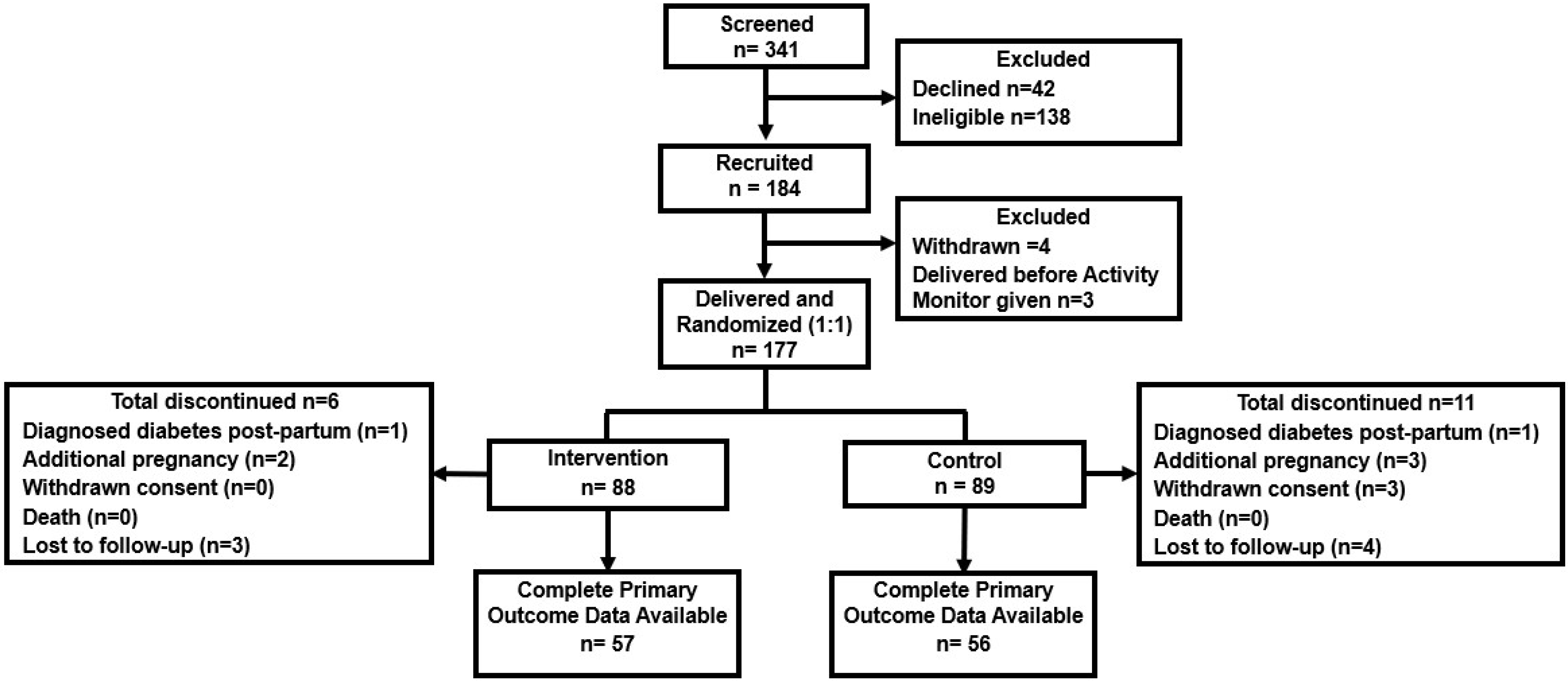
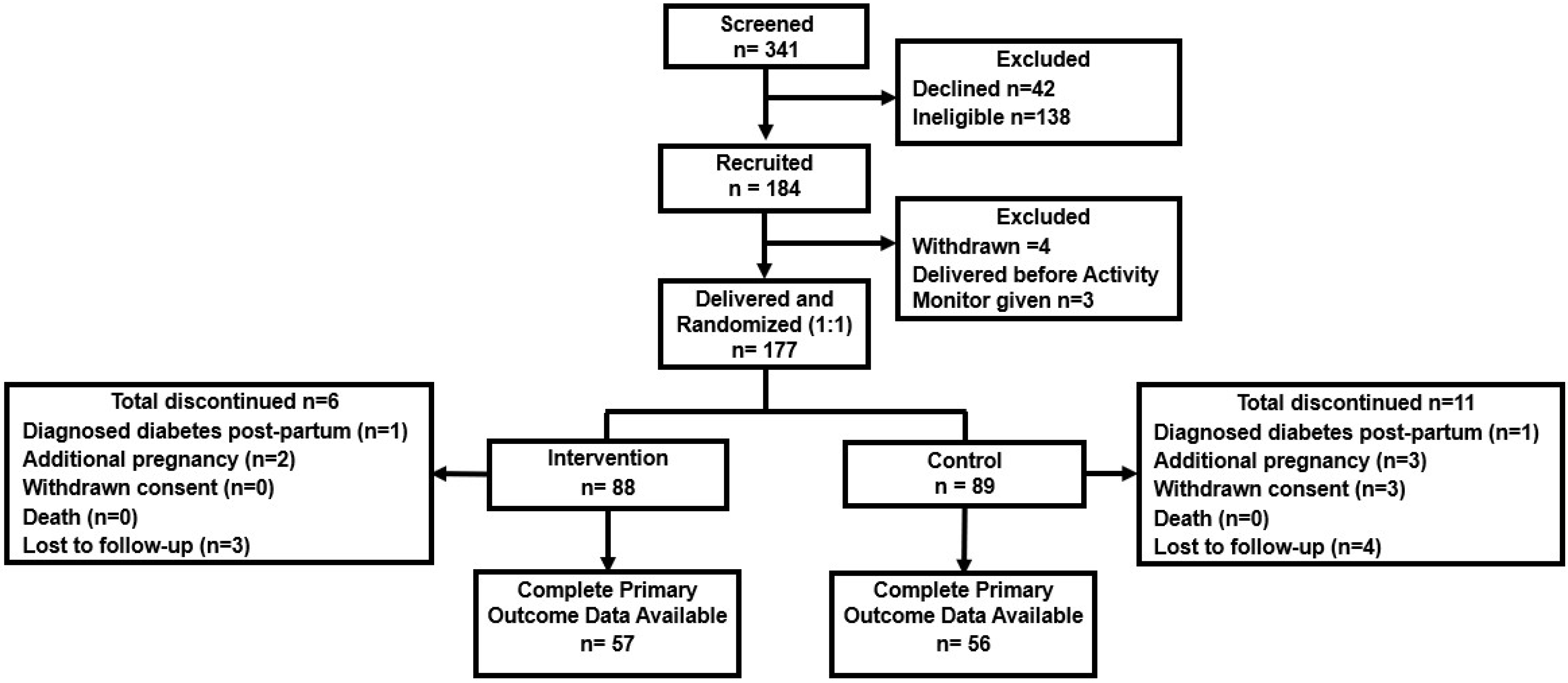
2.1. Participants
2.2. Randomisation
2.3. The Activity Monitor
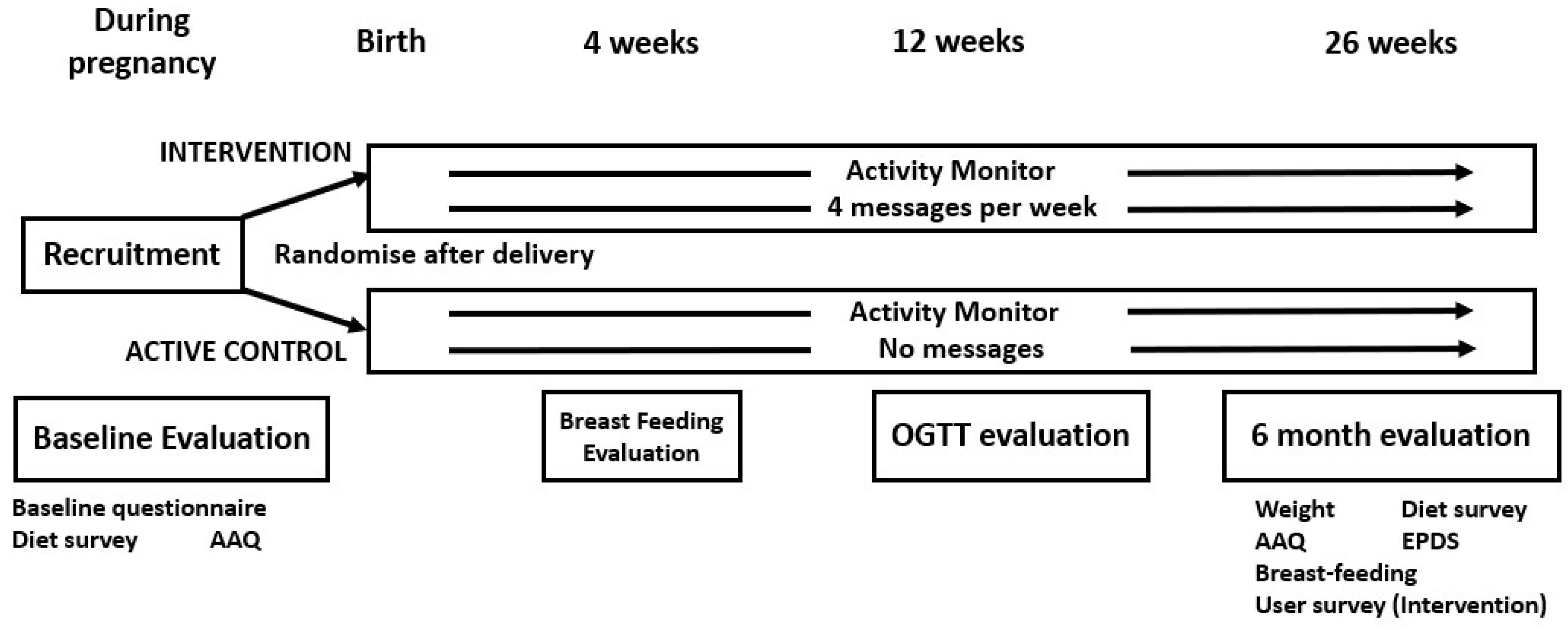
2.4. Intervention
2.5. Content of the Messages
2.6. Message Customisation
2.7. Active Control
2.8. Data Collection
2.9. The Study Outcomes
2.10. Qualitative Interviews
2.11. Statistical Analysis
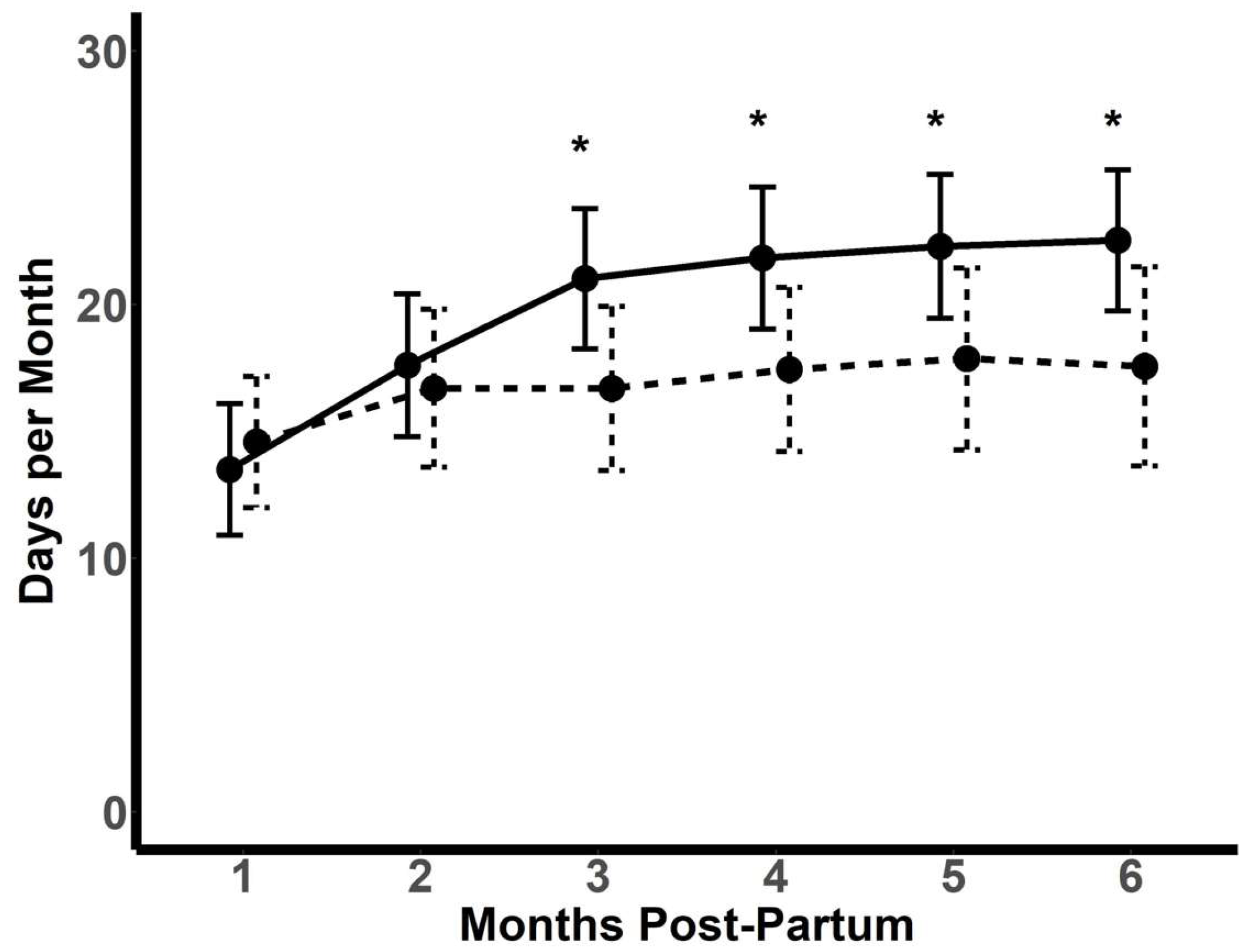
2.12. Analysis of the Activity Monitor Data
3. Results
3.1. COVID-19 Restrictions during the Study
3.2. Primary and Secondary Outcomes (Intention-to-Treat Analysis)
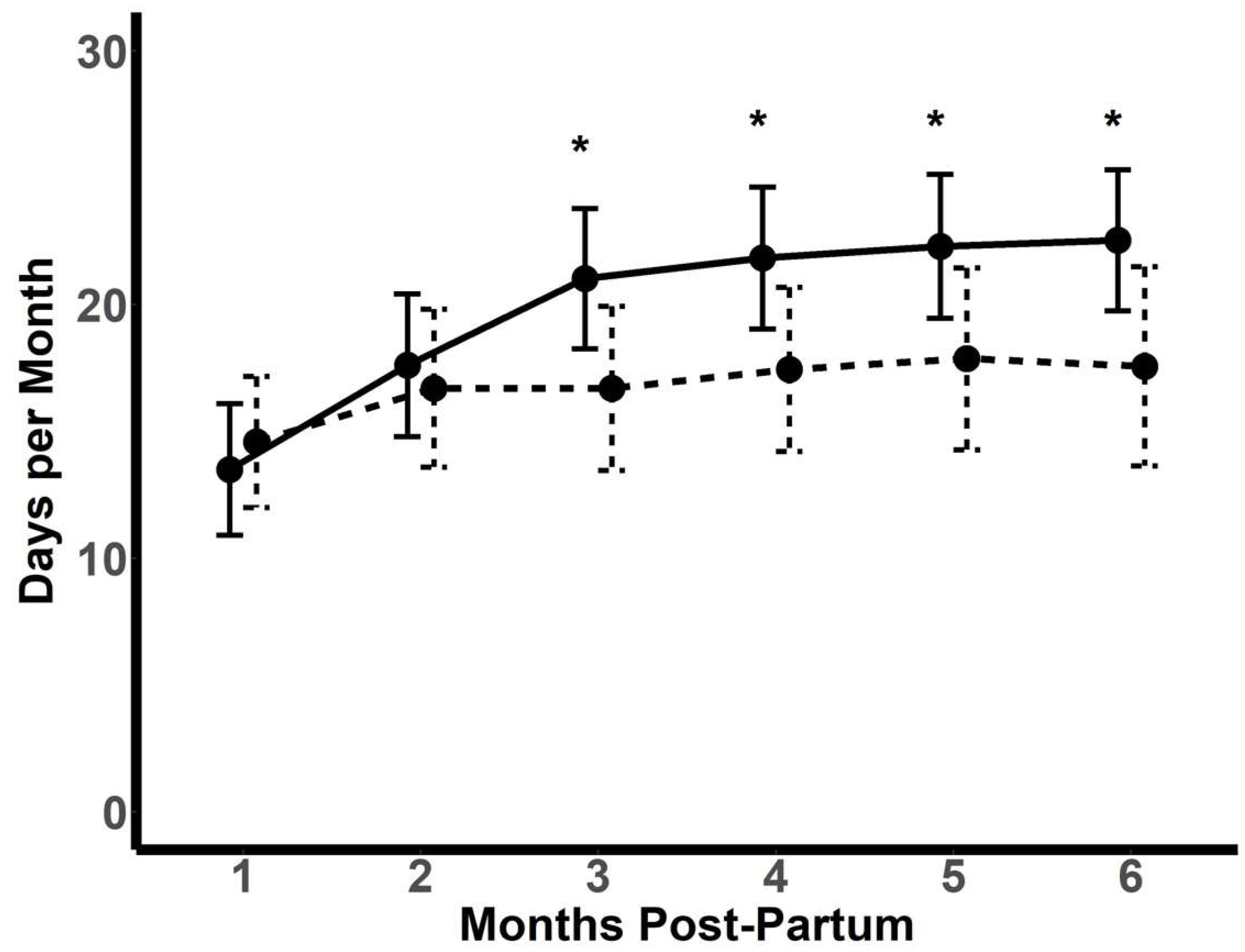
3.3. Activity Monitor Usage
3.4. Feedback Regarding the Text Messages and Activity Monitor
3.5. Qualitative Evaluation
“…[text messages] constantly reminding to reach our target otherwise we’re getting back the diabetes after pregnancy. Because during pregnancy it was so hard. We had to do injection on our tummy. Once I was getting the [text message] reminder I was thinking back during my pregnancy, and I was like, ‘I have to be healthy not to get diabetes, back again’”(Qualitative participant 10).
3.6. Safety and Adverse Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sweeting, A.; Wong, J.; Murphy, H.R.; Ross, G.P. A clinical update on gestational diabetes mellitus. Endocr. Rev. 2022, 43, 763–793. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.W.; Byth, K. The population health significance of gestational diabetes. Diabetes Care 2003, 26, 2005–2009. [Google Scholar] [CrossRef] [PubMed]
- Ratner, R.E.; Christophi, C.A.; Metzger, B.E.; Dabelea, D.; Bennett, P.H.; Pi-Sunyer, X.; Fowler, S.; Kahn, S.E.; The Diabetes Prevention Program Research Group. Prevention of diabetes in women with a history of gestational diabetes: Effects of metformin and lifestyle interventions. J. Clin. Endocrinol. Metab. 2008, 93, 4774–4779. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Yang, Y.; Cui, D.; Li, C.; Ma, R.C.; Li, J.; Yang, X. Effects of lifestyle intervention on long-term risk of diabetes in women with prior gestational diabetes: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13122. [Google Scholar] [CrossRef]
- Tandon, N.; Gupta, Y.; Kapoor, D.; Lakshmi, J.K.; Praveen, D.; Bhattacharya, A.; Billot, L.; Naheed, A.; de Silva, A.; Gupta, I.; et al. Effects of a lifestyle intervention to prevent deterioration in glycemic status among South Asian women with recent gestational diabetes: A randomized clinical trial. JAMA Netw. Open 2022, 5, e220773. [Google Scholar] [CrossRef]
- Ferrara, A.; Hedderson, M.M.; Brown, S.D.; Albright, C.L.; Ehrlich, S.F.; Tsai, A.L.; Caan, B.J.; Sternfeld, B.; Gordon, N.P.; Schmittdiel, J.A.; et al. The comparative effectiveness of diabetes prevention strategies to reduce postpartum weight retention in women with gestational diabetes mellitus: The Gestational Diabetes’ Effects on Moms (GEM) cluster randomized trial. Diabetes Care 2016, 39, 65–74. [Google Scholar] [CrossRef]
- Cheung, N.W.; Blumenthal, C.; Smith, B.J.; Hogan, R.; Thiagalingam, A.; Redfern, J.; Barry, T.; Cinnadaio, N.; Chow, C.K. A pilot randomised controlled trial of a text messaging intervention with customisation using linked data from wireless wearable activity monitors, to improve risk factors following gestational diabetes. Nutrients 2019, 11, 590. [Google Scholar] [CrossRef]
- Chow, C.K.; Redfern, J.; Hills, G.S.; Thakkar, J.; Santo, K.; Hackett, M.L.; Jan, S.; Graves, N.; de Keizer, L.; Barry, T.; et al. Effect of lifestyle-focused text messaging on risk factor modification in patients with coronary heart disease: A randomized clinical trial. JAMA 2015, 314, 1255–1263. [Google Scholar] [CrossRef]
- Skinner, R.; Gonet, V.; Currie, S.; Hoddinot, P.; Dornbrowski, S.U. A systematic review with meta-analyses of text message-delivered behaviour change interventions for weight loss and weight loss maintenance. Obes. Rev. 2020, 21, e12999. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.M.; Duque, L.; Huffman, J.C.; Healy, B.C.; Celano, C.M. Text message interventions for physical activity: A systematic review and meta-analysis. Am. J. Prevent Med. 2019, 58, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Scott-Sheldon, L.A.; Lantini, R.; Jennings, E.G.; Thind, H.; Rosen, R.K.; Salmoirago-Blotcher, E.; Bock, B.C. Text messaging-based interventions for smoking cessation: A systematic review and meta-analysis. JMIR Mhealth Uhealth 2016, 4, e49. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Whittaker, R.; Jiang, Y.; Maddison, R.; Shepherd, M.; McNamara, C.; Cutfield, R.; Khanolkar, M.; Murphy, R. Effectiveness of text message based, diabetes self management support programme (SMS4BG): Two arm, parallel randomised controlled trial. Br. Med. J. 2018, 361, k1959. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.A.; Greevy, R.A.; Spieker, A.; Wallston, K.A.; Elasy, T.A.; Kripalani, S.; Gentry, C.; Bergner, E.M.; LeStourgeon, L.M.; Williamson, S.E.; et al. Effects of a tailored text messaging intervention among diverse adults with type 2 diabetes: Evidence from the 15-month REACH randomized controlled trial. Diabetes Care 2021, 44, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Burn, E.; Nghiem, S.; Jan, S. Cost-effectiveness of a text-message program for cardiovascular disease secondary prevention. Heart 2017, 103, 893–894. [Google Scholar] [CrossRef] [PubMed]
- Marschner, S.; Chow, C.; Thiagalingam, A.; Simmons, D.; McLean, M.; Pasupathy, D.; Smith, B.J.; Flood, V.; Padmanabhan, S.; Melov, S.; et al. Effectiveness of a customised mobile phone text messaging intervention supported by data from activity monitors for improving lifestyle factors related to the risk of type 2 diabetes among women after gestational diabetes: Protocol for a multicentre randomised controlled trial (SMART MUMS with smart phones 2). BMJ Open 2021, 11, e054756. [Google Scholar]
- World Health Organization Consultation. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: A World Health Organization Guideline. Diabetes Res. Clin. Pract. 2014, 103, 341–363. [Google Scholar] [CrossRef]
- Martin, F.I.R. The diagnosis of gestational diabetes. Med. J. Aust. 1991, 155, 112–113. [Google Scholar] [CrossRef]
- Carey, R.N.; Connell, L.E.; Johnston, M.; Carey, R.N.; Connell, L.E.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Michie, S. Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Ann. Behav. Med. 2019, 53, 693–707. [Google Scholar] [CrossRef]
- NHMRC. Australian Dietary Guidelines; NHMRC: Canberra, Australia, 2013. [Google Scholar]
- Szeto, M.D.; Barber, C.; Ranpariya, V.K.; Anderson, J.; Hatch, J.; Ward, J.; Aguilera, M.N.; Hassan, S.; Hamp, A.; Coolman, T.; et al. Emojis and emotions in health care and dermatology communication: Narrative review. JMIR Dermatol. 2022, 5, e33851. [Google Scholar] [CrossRef]
- Nankervis, A.; McIntyre, H.D.; Moses, R.; Ross, G.P.; Callaway, L.; Porter, C.; Jeffries, W.; Boorman, C.; De Vries, B.; McElduff, A. for the Australasian Diabetes in Pregnancy Society. ADIPS Consensus Guidelines for the Testing and Diagnosis of Hyperglycaemia in Pregnancy in Australia and New Zealand. Available online: http://www.adips.org/downloads/adipsconsensusguidelinesgdm-03.05.13versionacceptedfinal.pdf (accessed on 16 April 2023).
- Adams, M.A.; Sallis, J.F.; Normal, G.J.; Hovell, M.F.; Hekler, E.B.; Perata, E. An adaptive physical activity intervention for overweight adults: A randomized controlled trial. PLoS ONE 2013, 8, e82901. [Google Scholar] [CrossRef] [PubMed]
- Galbicka, G. Shaping in the 21st century: Moving percentile schedules into applied settings. J. App. Behav. Anal. 1994, 27, 739–760. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare (AIHW). The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting; AIHW: Canberra, Australia, 2003. [Google Scholar]
- Melov, S.J.; White, S.J.; Simmons, M.; Kirby, A.; Stulz, V.; Padmanabhan, S.; Alahakoon, T.I.; Pasupathy, D.; Cheung, N.W. The BLIiNG Study—Breastfeeding length and intensity in gestational diabetes and metabolic effects in a subsequent pregnancy: A cohort study. Midwifery 2022, 107, 103262. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.J.; Cheung, N.W.; Zehle, K.; McLean, M.; Bauman, A.E. Post-partum physical activity and related psychosocial factors among women with recent gestational diabetes. Diabetes Care 2005, 28, 2650–2654. [Google Scholar] [CrossRef]
- Zehle, K.; Smith, B.J.; Chey, T.; McLean, M.; Bauman, A.E.; Cheung, N.W. Psychosocial factors related to diet among women with recent gestational diabetes: Opportunities for intervention. Diab. Educ. 2008, 34, 807–814. [Google Scholar] [CrossRef]
- Business World. Available online: https://www.bworldonline.com/community/2020/04/02/287449/sparkup-community-fitbit-data-reveals-the-impact-of-covid-19-on-global-activity/ (accessed on 3 May 2023).
- Chew, H.S.J.; Lopez, V. Global Impact of COVID-19 on weight and weight-related behaviors in the adult population: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 1876. [Google Scholar] [CrossRef]
- Melov, S.; Galas, N.; Swain, J.; Alahakoon, T.I.; Lee, V.; Cheung, N.W.; McGee, T.; Pasupathy, D.; McNab, J. Women’s experience of perinatal support in a high migrant Australian population during the COVID-19 pandemic: A mixed methods study. BMC Preg. Childbirth 2023, 23, 429. [Google Scholar] [CrossRef]
- Bayrampour, H.; Tsui, M.Y.E. Postpartum people’s experiences of and responses to the COVID-19 pandemic during the first year of the pandemic: A descriptive qualitative study. Women’s Health 2023, 19, 17455057231157480. [Google Scholar] [CrossRef]
- Morrison, M.K.; Koh, D.; Lowe, J.M.; Miller, Y.D.; Marshall, A.L.; Colyvas, K.; Collins, C.E. Postpartum diet quality in Australian women following a gestational diabetes pregnancy. Eur. J. Clin. Nutr. 2012, 66, 1160–1165. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Rollo, M.E.; Baldwin, J.N.; Hutchesson, M.; Aguiar, E.J.; Wynne, K.; Young, A.; Callister, R.; Collins, C.E. Evaluation of a type 2 diabetes risk reduction online program for women with recent gestational diabetes: A randomised trial. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Mitchell, P.; Liew, G.; Burlutsky, G.; Flood, V.M.; Gopinath, B. Telephone-delivered dietary intervention in patients with age-related macular degeneration: 3-month post-intervention findings of a randomised controlled trial. Nutrients 2020, 12, 3083. [Google Scholar] [CrossRef] [PubMed]
- Nour, M.; Chen, J.; Allman-Farinelli, M. Efficacy and external validity of electronic and mobile phone-based interventions promoting vegetable intake in young adults: Systematic review and meta-analysis. J. Med. Internet Res. 2016, 18, e58. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.T.; Barnes, K.; Ball, L.; Ross, L.J.; Sladdin, I.; Mitchell, L.J. How effective are dietitians in weight management? A systematic review and meta-analysis of randomized controlled trials. Healthcare 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.K.; Collins, C.E.; Lowe, J.M. Postnatal testing for diabetes in Australian women following gestational diabetes mellitus. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D.I.R.; Versace, V.L.; Dunbar, J.A.; Scheil, W.; Janus, E.; Oats, J.J.N.; Skinner, T.; Shih, S.; O’Reilly, S.; Sikaris, K.; et al. Results of the first recorded evaluation of a national gestational diabetes mellitus register: Challenges in screening, registration, and follow-up for diabetes risk. PLoS ONE 2018, 13, e200832. [Google Scholar] [CrossRef]
- Australasian Diabetes in Pregnancy Society (ADIPS); the Australian Diabetes Society (ADS); the Australian Diabetes Educators Association (ADEA); Diabetes Australia (DA). Diagnostic Testing for Gestational Diabetes Mellitus (GDM) during the COVID 19 Pandemic: Antenatal and Postnatal Testing Advice. Available online: https://www.adips.org/documents/RevisedGDMCOVID-19GuidelineFINAL30April2020pdf_000.pdf (accessed on 29 February 2024).
- Yamamoto, J.; Donovan, L.; Feig, D.; Berger, H. Temporary Alternative Screening Strategy for Gestational Diabetes Screening during the COVID-19 Pandemic. A Joint Consensus Statement from the Diabetes Canada Clinical Practice Guidelines Steering Committee and the Society of Obstetricians and Gynecologists of Canada. Available online: https://els-jbs-prod-cdn.jbs.elsevierhealth.com/pb/assets/raw/health%20advance/journals/jcjd/jcjd_covid_guidelines_020420.pdf (accessed on 29 February 2024).
- Gunderson, E.P.; Hurston, S.R.; Ning, X.; Lo, J.C.; Crites, Y.; Walton, D.; Dewey, K.G.; Azevedo, R.A.; Young, S.; Fox, G.; et al. Lactation and progression to type 2 diabetes mellitus after gestational diabetes mellitus: A prospective cohort study. Ann. Intern. Med. 2015, 163, 889–898. [Google Scholar] [CrossRef]
- Netting, M.J.; Moumin, N.A.; Knight, E.J.; Golley, R.K.; Makrides, M.; Green, T.J. The Australian feeding infants and toddler study (OzFITS 2021): Breastfeeding and early feeding practices. Nutrients 2022, 14, 206. [Google Scholar] [CrossRef]
- Cheung, N.W.; Thiagalingam, A.; Smith, B.J.; Redfern, J.; Barry, T.; Mercorelli, L.; Chow, C.K. Text messages promoting healthy lifestyle and linked with activity monitors stimulate an immediate increase in physical activity among women after gestational diabetes. Diabetes Res. Clin. Pract. 2022, 190, 109991. [Google Scholar] [CrossRef]
- Peacock, A.S.; Bogossian, F.E.; Wilkinson, S.A.; Gibbons, K.S.; Kim, C.; McInthyre, H.D. A randomised controlled trial to delay or prevent type 2 diabetes after gestational diabetes: Walking for exercise and nutrition to prevent diabetes for you. Int. J. Endocrinol. 2015, 2015, 423717. [Google Scholar] [CrossRef]
- Maturi, M.S.; Afshary, P.; Abedi, P. Effect of physical activity intervention based on a pedometer on physical activity level and anthropometric measures after childbirth: A randomized controlled trial. BMC Pregnancy Childbirth 2011, 11, 103. [Google Scholar] [CrossRef] [PubMed]
- Huo, X.; Krumholz, H.M.; Bai, X.; Spatz, E.S.; Ding, Q.; Horak, P.; Zhao, W.; Gong, Q.; Zhang, H.; Yan, X.; et al. Effects of mobile text messaging on glycemic control in patients with coronary heart disease and diabetes mellitus. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005805. [Google Scholar] [CrossRef] [PubMed]
- Waller, K.; Furber, S.; Bauman, A.; Allman-Farinelli, M.; van den Dolder, P.; Hayes, A.; Facci, F.; Franco, L.; Webb, A.; Moses, R.; et al. Effectiveness and acceptability of a text message intervention (DTEXT) on HbA1c and self-management for people with type 2 diabetes. A randomized controlled trial. Patient Educ. Couns. 2021, 104, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.W.; Redfern, J.; Thiagalingam, A.; Hng, T.M.; Marschner, S.; Haider, R.; Faruquie, S.; von Huben, A.; She, S.; McIntyre, D.; et al. Effect of mobile phone text messaging self-management support for patients with diabetes or coronary heart disease in a chronic disease management program (SupportMe) on blood pressure: Pragmatic randomized controlled trial. J. Med. Internet Res. 2023, 25, e38275. [Google Scholar] [CrossRef] [PubMed]
- Bowring, A.L.; Peeters, A.; Freak-Poli, R.; Lim, M.S.C.; Gouillou, M.; Hellard, M. Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med. Res. Methodol. 2012, 12, 175. [Google Scholar] [CrossRef]
- Quinlan, C.; Rattray, B.; Pryor, D.; Northey, J.M.; Antsey, K.J.; Butterworth, P.; Cherbuin, N. The accuracy of self-reported physical activity questionnaires varies with sex and body mass index. PLoS ONE 2021, 16, e0256008. [Google Scholar] [CrossRef]
- Head, S.H.; Rosella, L.C.; Berger, H.; Feig, D.S.; Fleming, K.; Ray, J.G.; Shah, B.R.; Lipscombe, L.L. BMI and risk of gestational diabetes among women of south Asian and Chinese ethnicity: A population-based study. Diabetologia 2021, 64, 805–813. [Google Scholar]
- Wong, V.W.; Lin, A.; Russell, H. Adopting the new World Health Organization diagnostic criteria for gestational diabetes: How the prevalence changes in a high-risk region in Australia. Diabetes Res. Clin. Pract. 2017, 129, 148–153. [Google Scholar] [CrossRef]
- Lee, A.J.; Hiscock, R.J.; Wein, P.; Walker, S.P.; Permezel, M. Gestational diabetes mellitus: Clinical predictors and long-term risk of developing type 2 diabetes. Diabetes Care 2007, 30, 878–883. [Google Scholar] [CrossRef]
- Oldfield, M.D.; Donley, P.; Walwyn, L.; Scudamore, I.; Gregory, R. Long term prognosis of women with gestational diabetes in a multiethnic population. Postgrad. Med. J. 2007, 83, 426–430. [Google Scholar] [CrossRef]
- Prochaska, J.O. Systems of Psychotherapy: A Transtheoretical Analysis, 2nd ed.; Brooks-Cole: Pacific Grove, CA, USA, 1984. [Google Scholar]
- Hill, B.; McPhie, S.; Skouteris, H. The role of parity in gestational weight gain and postpartum weight retention. Womens Health Issues 2016, 26, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Blum, J.W.; Beaudoin, C.M.; Caton-Lemos, L. Physical activity patterns and maternal well-being in post-partum women. Matern. Child Health J 2004, 8, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Salingeh, M.; McNamara, B.; Rooney, R. Perceived barriers and enablers of physical activity in postpartum women: A qualitative approach. BMC Pregnancy Childbirth 2016, 16, 131. [Google Scholar]
- Albright, C.; Saiki, K.; Steffen, A.D.; Wofkel, E. What barriers thwart postpartum women’s physical activity goals during a 12-month intervention? A process evaluation of the Na Mikimiki project. Women Health 2015, 55, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Goveia, P.; Canon-Montanez, W.; de Paula Santos, D.; Lopes, G.W.; Ma, R.C. Lifestyle intervention for the prevention of diabetes in women with previous gestational diabetes mellitus. A systematic review and meta-analysis. Front. Endocrinol. 2018, 9, 583. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention (n = 88) | Control (n = 89) | Overall (n = 177) | |
|---|---|---|---|
| Age (years) | 32.3 ± 4.5 | 32.2 ± 4.8 | 32.2 ± 4.6 |
| Pre-pregnancy Body Mass Index (kg/m2) | 29.3 ± 7.4 | 28.3 ± 6.4 | 28.8 ± 6.9 |
| Gestational age at booking in (weeks) | 17.5 ± 4.9 | 17.2 ± 4.9 | 17.3 ± 4.9 |
| Ethnicity | |||
| Australian/New Zealand (non-Indigenous) | 21 (24%) | 19 (21%) | 40 (23%) |
| South Asian | 40 (46%) | 43 (48%) | 83 (47%) |
| East and Southeast Asian | 4 (5%) | 12 (13%) | 16 (9%) |
| Others | 23 (26%) | 15 (17%) | 38 (21%) |
| Marital status | |||
| Married/de facto | 80 (90.9%) | 84 (94.4%) | 164 (93%) |
| Single/separated/widowed | 8 (9%) | 5 (6%) | 13 (7%) |
| Education | |||
| Tertiary | 62 (70%) | 73 (82%) | 135 (76%) |
| Secondary or less | 26 (30%) | 16 (19%) | 42 (24%) |
| Employment status before pregnancy | |||
| Working full time | 44 (50%) | 44 (49%) | 88 (50%) |
| Working part time | 24 (27%) | 28 (32%) | 52 (29%) |
| Not in paid work | 20 (22%) | 17 (19%) | 37 (21%) |
| Background medical history | |||
| Polycystic ovary syndrome | 16 (18%) | 10 (11%) | 26 (15%) |
| Depression | 8 (9%) | 9 (10%) | 17 (10%) |
| Hypertension | 3 (3%) | 6 (7%) | 9 (5%) |
| Hypercholesterolaemia | 5 (6%) | 5 (6%) | 10 (6%) |
| Previous gestational diabetes | 28 (32%) | 29 (33%) | 57 (32%) |
| Family history of diabetes (first degree) | 47 (53%) | 66 (63%) | 103 (58%) |
| Primiparous | 29 (33%) | 37 (42%) | 66 (37%) |
| Multiparous | 59 (67%) | 52 (58%) | 111 (63%) |
| Breastfeeding of previous children | 54/59 (92%) | 48/52 (92%) | 102/111 (92%) |
| Smoking | |||
| Current smoker | 2 (2%) | 4 (5%) | 6 (3%) |
| Former smoker | 13 (15%) | 13 (15%) | 26 (15%) |
| Never smoked | 73 (83%) | 72 (81%) | 145 (82%) |
| Drinks alcohol when not pregnant | 29 (33%) | 13 (15%) | 42 (24%) |
| Vegetarian | 14 (16%) | 16 (18%) | 30 (17%) |
| Total PA time prepregnancy (min/week) | 340 ± 334 | 336 ± 344 | 338 ± 338 |
| Diet prepregnancy | |||
| Servings of vegetables per day | 1.2 ± 0.9 | 1.1 ± 0.9 | 1.1 ± 0.9 |
| Servings of fruit per day | 1.1 ± 0.7 | 1.0 ± 0.7 | 1.1 ± 0.7 |
| Servings of discretionary food per week | 19.3 ± 12.4 | 16 ± 10.5 | 17.6 ± 11.6 |
| Alcoholic drinks per day | 0.1 ± 0.2 | 0.0 ± 0.1 | 0.1 ± 0.2 |
| Weeks gestation at delivery | 37.5 ± 2.3 | 37.1 ± 3.1 | 37.3 ± 2.8 |
| Birth weight (g) | 3381 ± 548 | 3236 ± 509 | 3308 ± 532 |
| Mode of delivery | |||
| Caesarean section | 42 (48%) | 33 (37%) | 75 (42%) |
| Instrument | 7 (8%) | 12 (14%) | 19 (11%) |
| Normal vaginal delivery | 39 (44%) | 44 (49%) | 83 (47%) |
| GDM treatment during pregnancy | |||
| Insulin | 46 (52%) | 47 (53%) | 93 (53%) |
| Metformin | 12 (14%) | 6 (7%) | 18 (10%) |
| Maternal complications | |||
| Pre-eclampsia | 3 (3%) | 5 (6%) | 8 (5%) |
| Post-partum haemorrhage | 11 (13%) | 6 (7%) | 17 (10%) |
| 3rd- or 4th-degree vaginal tear | 1 (1%) | 2 (2%) | 3 (2%) |
| Admission to neonatal intensive care | 4 (5%) | 9 (10%) | 13 (7%) |
| Intervention | Control | Adjusted Relative Risk (95%CI) or Mean Difference (95%CI) | p Value | |
|---|---|---|---|---|
| Primary Outcome | ||||
| Met Healthy Lifestyle Outcome * | 7/57 (12%) | 6/56 (11%) | 1.15 (0.41–3.2) | 0.79 |
| Secondary Outcomes | ||||
| Met weight goal | 20/67 (30%) | 12/62 (19%) | 1.54 (0.82–2.89) | 0.17 |
| Met physical activity goal | 23/49 (47%) | 29/46 (63%) | 0.72 (0.50–1.04) | 0.08 |
| Met dietary goal | 2/58 (3%) | 0/58 (0%) | N/A | N/A |
| Body Mass Index (kg/m2) | 29.4 ± 6.9 | 28.4 ± 5.9 | 0.97 (−1.24–3.18) | 0.39 |
| Total physical activity time (mins/week) | 260 ± 278 (N = 49) | 301 ± 262 (N = 46) | −41 (−150–68) | 0.46 |
| OGTT performed by 12 weeks post-partum | 38/5 (43%) | 29/89 (33%) | 1.22 (0.78–1.91) | 0.36 |
| Breastfeeding at 1 month Yes Intensity (BLISS Score) | 46/50 (92%) 5.1 ± 1.8 | 48/54 (89%) 4.5 ± 2.2 | 1.04 (0.91–1.17) 0.66 (−0.12–1.44) | 0.60 0.20 |
| Any breastfeeding at 6 months Yes Intensity (BLISS Score) | 34/44 (77%) 20.4 ± 4.3 | 41/45 (91%) 19.3 ± 5.5 | 0.85 (0.71–1.02) 1.06 (−1.00–3.13) | 0.07 0.52 |
| EPDS score ≥ 10 | 15/88 (17%) | 12/89 (14%) | 1.26 (0.63–2.54) | 0.51 |
| Intervention n = 58 | Control n = 58 | Adjusted Relative Risk (95%CI) or Mean Difference (95%CI) | p Value | |
|---|---|---|---|---|
| Met Healthy Lifestyle Outcome dietary goal | 2 (3%) | 0 (0%) | N/A | N/A |
| Met Australian Dietary Guidelines dietary goal | 0 (0%) | 0 (0%) | N/A | N/A |
| Servings of vegetables per day | 1.2 ± 0.8 * | 1.0 ± 0.6 | 1.04 (−0.87–2.95) | 0.29 |
| Met vegetable goal | 4 (7%) * | 0 (0%) | N/A | N/A |
| Servings of fruit per day | 0.7 ± 0.4 | 0.7 ± 0.4 | 0.00 (−1.23–1.23) | 1.00 |
| Met fruit goal | 21 (36%) | 21 (36%) | 0.93 (0.58–1.46) | 0.74 |
| Servings of discretionary foods per week | 13.6 ± 8.2 ** | 11.4 ± 6.1 | 2.19 (−0.45–4.84) | 0.11 |
| Met discretionary foods goal | 33 (59%) ** | 40 (69%) | 1.02 (0.84–1.23) | 0.85 |
| Servings of alcohol per day | 0.1 ± 0.2 | 0.0 ± 0.1 | 0.22 (−0.14–0.59) | 0.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, N.W.; Simmons, D.; Marschner, S.; Thiagalingam, A.; Pasupathy, D.; Smith, B.J.; Flood, V.; McLean, M.; Melov, S.J.; Hogan, R.; et al. Randomised Controlled Trial of a Customised Text Messaging and Activity Monitor Program for Lifestyle Improvement after Gestational Diabetes. Nutrients 2024, 16, 820. https://doi.org/10.3390/nu16060820
Cheung NW, Simmons D, Marschner S, Thiagalingam A, Pasupathy D, Smith BJ, Flood V, McLean M, Melov SJ, Hogan R, et al. Randomised Controlled Trial of a Customised Text Messaging and Activity Monitor Program for Lifestyle Improvement after Gestational Diabetes. Nutrients. 2024; 16(6):820. https://doi.org/10.3390/nu16060820
Chicago/Turabian StyleCheung, Ngai Wah, David Simmons, Simone Marschner, Aravinda Thiagalingam, Dharmintra Pasupathy, Ben J. Smith, Victoria Flood, Mark McLean, Sarah J. Melov, Roslyn Hogan, and et al. 2024. "Randomised Controlled Trial of a Customised Text Messaging and Activity Monitor Program for Lifestyle Improvement after Gestational Diabetes" Nutrients 16, no. 6: 820. https://doi.org/10.3390/nu16060820
APA StyleCheung, N. W., Simmons, D., Marschner, S., Thiagalingam, A., Pasupathy, D., Smith, B. J., Flood, V., McLean, M., Melov, S. J., Hogan, R., Padmanabhan, S., Duke, A., Ching, C., Min, H., McNab, J., & Chow, C. K. (2024). Randomised Controlled Trial of a Customised Text Messaging and Activity Monitor Program for Lifestyle Improvement after Gestational Diabetes. Nutrients, 16(6), 820. https://doi.org/10.3390/nu16060820