
Use of Complementary and Alternative Medicine in Patients with Rare Bone Diseases and Osteoporosis

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
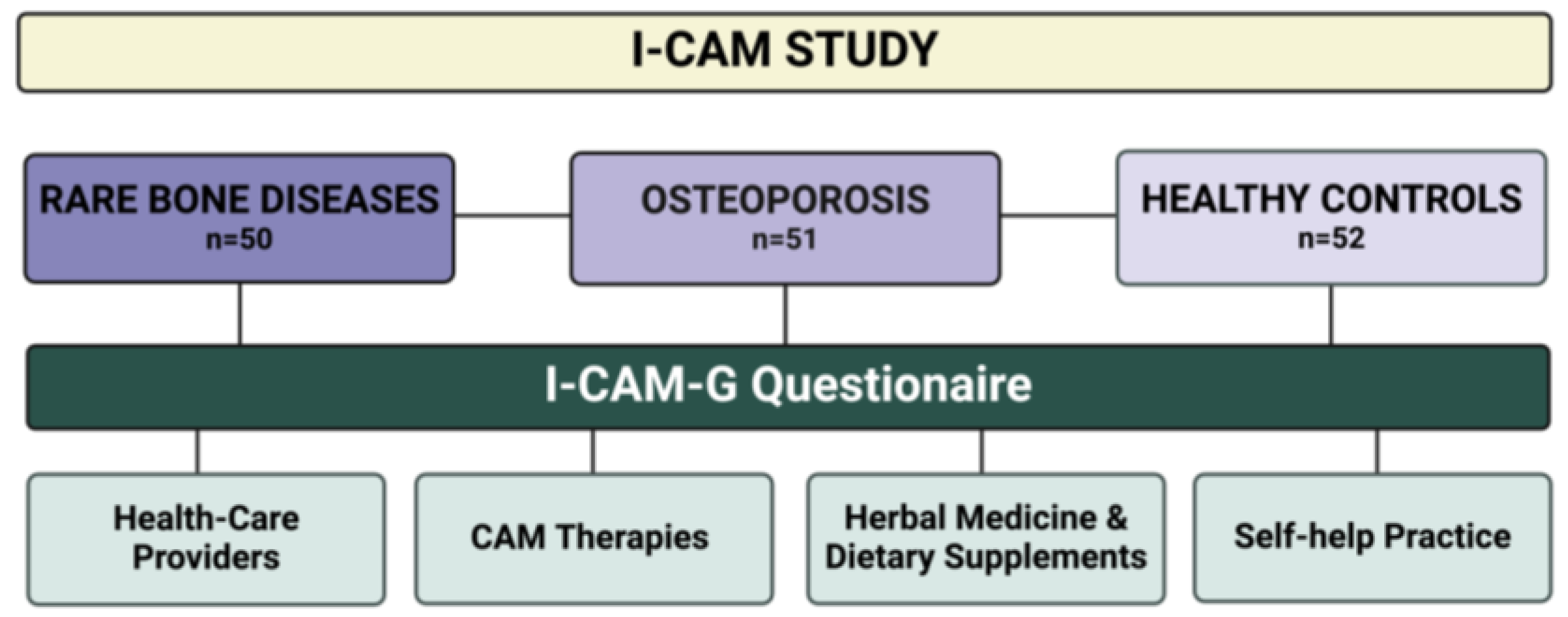
2.1. Study Groups
2.2. I-CAM-G Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. I-CAM-G Questionnaire
3.2.1. Physicians and Other Therapists Who Have Treated the Patients with Naturopathic Treatments within the Last 12 Months
3.2.2. Treatments Delivered by Physicians in the Field of Naturopathy
3.2.3. Herbal Medicine and Dietary Supplements
3.2.4. Self-Help Practice
3.3. Demographic and Socioeconomic Factors and CAM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javaid, M.K.; Ward, L.; Pinedo-Villanueva, R.; Rylands, A.J.; Williams, A.; Insogna, K.; Imel, E.A. Musculoskeletal Features in Adults With X-linked Hypophosphatemia: An Analysis of Clinical Trial and Survey Data. J. Clin. Endocrinol. Metab. 2022, 107, e1249–e1262. [Google Scholar] [CrossRef]
- Raimann, A.; Mindler, G.T.; Kocijan, R.; Bekes, K.; Zwerina, J.; Haeusler, G.; Ganger, R. Multidisciplinary patient care in X-linked hypophosphatemic rickets: One challenge, many perspectives. Wien Med. Wochenschr. 2020, 170, 116–123. [Google Scholar] [CrossRef]
- Genest, F.; Rak, D.; Petryk, A.; Seefried, L. Physical Function and Health-Related Quality of Life in Adults Treated with Asfotase Alfa for Pediatric-Onset Hypophosphatasia. JBMR Plus 2020, 4, e10395. [Google Scholar] [CrossRef]
- Behanova, M.; Medibach, A.; Haschka, J.; Kraus, D.; Raimann, A.; Mindler, G.T.; Zwerina, J.; Kocijan, R. Health-related quality of life and fatigue in adult rare bone disease patients: A cross-sectional study from Austria. Bone 2024, 181, 117034. [Google Scholar] [CrossRef]
- Portale, A.A.; Carpenter, T.O.; Brandi, M.L.; Briot, K.; Cheong, H.I.; Cohen-Solal, M.; Crowley, R.; Jan De Beur, S.; Eastell, R.; Imanishi, Y.; et al. Continued Beneficial Effects of Burosumab in Adults with X-Linked Hypophosphatemia: Results from a 24-Week Treatment Continuation Period After a 24-Week Double-Blind Placebo-Controlled Period. Calcif. Tissue Int. 2019, 105, 271–284. [Google Scholar] [CrossRef] [PubMed]
- Kishnani, P.S.; Rockman-Greenberg, C.; Rauch, F.; Bhatti, M.T.; Moseley, S.; Denker, A.E.; Watsky, E.; Whyte, M.P. Five-year efficacy and safety of asfotase alfa therapy for adults and adolescents with hypophosphatasia. Bone 2019, 121, 149–162. [Google Scholar] [CrossRef]
- Adami, S.; Gatti, D.; Colapietro, F.; Fracassi, E.; Braga, V.; Rossini, M.; Tatò, L. Intravenous neridronate in adults with osteogenesis imperfecta. J. Bone Miner. Res. 2003, 18, 126–130. [Google Scholar] [CrossRef]
- Dwan, K.; Phillipi, C.A.; Steiner, R.D.; Basel, D. Bisphosphonate therapy for osteogenesis imperfecta. Cochrane Database Syst. Rev. 2016, 10, CD005088. [Google Scholar] [CrossRef]
- Orwoll, E.S.; Shapiro, J.; Veith, S.; Wang, Y.; Lapidus, J.; Vanek, C.; Reeder, J.L.; Keaveny, T.M.; Lee, D.C.; Mullins, M.A.; et al. Evaluation of teriparatide treatment in adults with osteogenesis imperfecta. J. Clin. Investig. 2014, 124, 491–498. [Google Scholar] [CrossRef]
- Marom, R.; Rabenhorst, B.M.; Morello, R. Osteogenesis imperfecta: An update on clinical features and therapies. Eur. J. Endocrinol. 2020, 183, R95–R106. [Google Scholar] [CrossRef] [PubMed]
- Complementary and Alternative Medicine (CAM)—NCI. Available online: https://www.cancer.gov/about-cancer/treatment/cam (accessed on 29 January 2024).
- Mentink, M.D.C.; van Vliet, L.M.; Timmer-Bonte, J.A.N.H.; Noordman, J.; van Dulmen, S. How is complementary medicine discussed in oncology? Observing real-life communication between clinicians and patients with advanced cancer. Patient Educ. Couns. 2022, 105, 3235–3241. [Google Scholar] [CrossRef] [PubMed]
- Opheim, R.; Lie Høivik, M.; Bernklev, T.; Jelsness-Jørgensen, L.-P.; Moum, B. The Use of Complementary and Alternative Medicine among Patients with Inflammatory Bowel Disease Is Associated with Reduced Health-Related Quality of Life. Gastroenterol. Res. Pract. 2016, 2016, 6453657. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Daikuhara, H.; Oshima, T.; Suzuki, H.; Okada, S.; Miyatake, N. Use of Complementary and Alternative Medicine and Its Relationship with Health-Related Quality of Life (HRQOL) in Patients with Type 2 Diabetes Mellitus. Epidemiologia 2023, 4, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Fjær, E.L.; Landet, E.R.; McNamara, C.L.; Eikemo, T.A. The use of complementary and alternative medicine (CAM) in Europe. BMC Complement. Med. Ther. 2020, 20, 108. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, A.E.; Quandt, S.A.; Stub, T. Use of complementary and alternative medicine in Norway: A cross-sectional survey with a modified Norwegian version of the international questionnaire to measure use of complementary and alternative medicine (I-CAM-QN). BMC Complement. Med. Ther. 2021, 21, 93. [Google Scholar] [CrossRef] [PubMed]
- Quandt, S.A.; Verhoef, M.J.; Arcury, T.A.; Lewith, G.T.; Steinsbekk, A.; Kristoffersen, A.E.; Wahner-Roedler, D.L.; Fønnebø, V. Development of an international questionnaire to measure use of complementary and alternative medicine (I-CAM-Q). J. Altern. Complement. Med. 2009, 15, 331–339. [Google Scholar] [CrossRef]
- Re, M.L.; Schmidt, S.; Güthlin, C. Translation and adaptation of an international questionnaire to measure usage of complementary and alternative medicine (I-CAM-G). BMC Complement. Altern. Med. 2012, 12, 259. [Google Scholar] [CrossRef]
- Phutrakool, P.; Pongpirul, K. Acceptance and use of complementary and alternative medicine among medical specialists: A 15-year systematic review and data synthesis. Syst. Rev. 2022, 11, 10. [Google Scholar] [CrossRef]
- Veziari, Y.; Leach, M.J.; Kumar, S. Barriers to the conduct and application of research in complementary and alternative medicine: A systematic review. BMC Complement. Altern. Med. 2017, 17, 166. [Google Scholar] [CrossRef]
- Berna, F.; Göritz, A.S.; Mengin, A.; Evrard, R.; Kopferschmitt, J.; Moritz, S. Alternative or complementary attitudes toward alternative and complementary medicines. BMC Complement. Altern. Med. 2019, 19, 83. [Google Scholar] [CrossRef]
- Zhang, N.-D.; Han, T.; Huang, B.-K.; Rahman, K.; Jiang, Y.-P.; Xu, H.-T.; Qin, L.-P.; Xin, H.-L.; Zhang, Q.-Y.; Li, Y.-M. Traditional Chinese medicine formulas for the treatment of osteoporosis: Implication for antiosteoporotic drug discovery. J. Ethnopharmacol. 2016, 189, 61–80. [Google Scholar] [CrossRef]
- Wong, R.W.K.; Rabie, A.B.M. Traditional Chinese medicines and bone formation—A review. J. Oral Maxillofac. Surg. 2006, 64, 828–837. [Google Scholar] [CrossRef]
- Round Table: Potenziale und Grenzen der Komplementärmedizin. Available online: https://www.aekwien.at/presseaussendungen/-/asset_publisher/G1Wljyo3fxB1/content/id/328844 (accessed on 29 January 2024).
- Pan, H.; Jin, R.; Li, M.; Liu, Z.; Xie, Q.; Wang, P. The Effectiveness of Acupuncture for Osteoporosis: A Systematic Review and Meta-Analysis. Am. J. Chin. Med. 2018, 46, 489–513. [Google Scholar] [CrossRef]
- Chong, C.a.K.Y.; Diaz-Granados, N.; Hawker, G.A.; Jamal, S.; Josse, R.G.; Cheung, A.M. Complementary and alternative medicine use by osteoporosis clinic patients. Osteoporos. Int. 2007, 18, 1547–1556. [Google Scholar] [CrossRef]
- Kemppainen, L.M.; Kemppainen, T.T.; Reippainen, J.A.; Salmenniemi, S.T.; Vuolanto, P.H. Use of complementary and alternative medicine in Europe: Health-related and sociodemographic determinants. Scand. J. Public Health 2018, 46, 448–455. [Google Scholar] [CrossRef]
- Bishop, F.L.; Lewith, G.T. Who Uses CAM? A Narrative Review of Demographic Characteristics and Health Factors Associated with CAM Use. Evid. Based Complement. Alternat. Med. 2010, 7, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Sharp, D.; Lorenc, A.; Morris, R.; Feder, G.; Little, P.; Hollinghurst, S.; Mercer, S.W.; MacPherson, H. Complementary medicine use, views, and experiences: A national survey in England. BJGP Open 2018, 2, bjgpopen18X101614. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz. Kosten. Available online: https://www.sozialministerium.at/Themen/Gesundheit/Medizin-und-Gesundheitsberufe/Komplement%C3%A4rmedizin/Kosten.html (accessed on 12 February 2024).
- Stanarević Katavić, S. Health information behaviour of rare disease patients: Seeking, finding and sharing health information. Health Info Libr. J. 2019, 36, 341–356. [Google Scholar] [CrossRef] [PubMed]
- Spring, H. Health information, what happens when there isn’t any? Information literacy and the challenges for rare and orphan diseases. Health Inf. Libr. J. 2014, 31, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; Scientific Advisory Board of the European Society for Clinical; Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO); Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). Executive summary of the European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Calcif. Tissue Int. 2019, 104, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Staehelin, H.B.; Orav, J.E.; Stuck, A.E.; Theiler, R.; Wong, J.B.; Egli, A.; Kiel, D.P.; Henschkowski, J. Fall prevention with supplemental and active forms of vitamin D: A meta-analysis of randomised controlled trials. BMJ 2009, 339, b3692. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2016, 27, 367–376. [Google Scholar] [CrossRef]
- Ng, J.Y.; Hilal, A.; Maini, I. What traditional, complementary, and integrative medicine recommendations exist across osteoporosis clinical practice guidelines? A systematic review and quality assessment. Integr. Med. Res. 2022, 11, 100803. [Google Scholar] [CrossRef]
- Chagas, C.E.A.; Roque, J.P.; Santarosa Emo Peters, B.; Lazaretti-Castro, M.; Martini, L.A. Do patients with osteogenesis imperfecta need individualized nutritional support? Nutrition 2012, 28, 138–142. [Google Scholar] [CrossRef]
- LoMauro, A.; Landoni, C.V.; Fraschini, P.; Molteni, F.; Aliverti, A.; Bertoli, S.; De Amicis, R. Eat, breathe, sleep with Osteogenesis Imperfecta. Orphanet J. Rare Dis. 2021, 16, 435. [Google Scholar] [CrossRef]
- Cho, T.-J.; Ko, J.M.; Kim, H.; Shin, H.-I.; Yoo, W.J.; Shin, C.H. Management of Osteogenesis Imperfecta: A Multidisciplinary Comprehensive Approach. Clin. Orthop. Surg. 2020, 12, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Haffner, D.; Emma, F.; Eastwood, D.M.; Duplan, M.B.; Bacchetta, J.; Schnabel, D.; Wicart, P.; Bockenhauer, D.; Santos, F.; Levtchenko, E.; et al. Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia. Nat. Rev. Nephrol. 2019, 15, 435–455. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, K.; Hahn, A.; Seefried, L. Mineral Intake and Clinical Symptoms in Adult Patients with Hypophosphatasia. J. Clin. Endocrinol. Metab. 2020, 105, dgaa324. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, K.; Hahn, A.; Seefried, L. Impact of Restricted Phosphorus, Calcium-adjusted Diet on Musculoskeletal and Mental Health in Hypophosphatasia. J. Endocr. Soc. 2023, 8, bvad150. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, P.; Schmidt, F.N.; Amling, M.; Yorgan, T.A.; Barvencik, F. Zinc and vitamin D deficiency and supplementation in hypophosphatasia patients—A retrospective study. Bone 2023, 175, 116849. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-P.; Hu, R.-X.; Han, M.; Lai, B.-Y.; Liang, S.-B.; Chen, B.-J.; Robinson, N.; Chen, K.; Liu, J.-P. Evidence Base of Clinical Studies on Qi Gong: A Bibliometric Analysis. Complement. Ther. Med. 2020, 50, 102392. [Google Scholar] [CrossRef] [PubMed]
- Huston, P.; McFarlane, B. Health benefits of tai chi: What is the evidence? Can. Fam. Physician 2016, 62, 881–890. [Google Scholar] [PubMed]
- Lomas-Vega, R.; Obrero-Gaitán, E.; Molina-Ortega, F.J.; Del-Pino-Casado, R. Tai Chi for Risk of Falls. A Meta-analysis. J. Am. Geriatr. Soc. 2017, 65, 2037–2043. [Google Scholar] [CrossRef] [PubMed]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef]

{kind=link}
| Patient Type | Rare Bone Disease Group (N = 50) | Osteoporosis Group (N = 51) | Control Group (N = 52) | ||||
|---|---|---|---|---|---|---|---|
| OI (N = 17) | HPP (N = 17) | XLH (N = 16) | Total | p-Value * | |||
| Age, mean (SD) | 47.6 (±15.6) | 55.9 (±13.9) | 42.5 (±16.0) | 48.8 (±15.9) | 66.6 (±10.0) | 50.8 (±16.3) | <0.001 |
| Gender, male, N (%) | 5 (29.4) | 7 (41.2) | 1 (6.3) | 13 (26.0) | 5 (9.8) | 14 (26.9) | 0.06 |
| Family status, N (%) | 0.09 | ||||||
| Single | 4 (23.5) | 1 (5.9) | 3 (18.8) | 8 (16.0) | 4 (7.8) | 13 (25.0) | |
| Married or cohabiting | 9 (52.9) | 10 (58.8) | 9 (56.3) | 28 (56.0) | 25 (49.0) | 30 (57.7) | |
| Divorced | 2 (11.8) | 3 (17.6) | 4 (25.0) | 9 (18) | 13 (25.5) | 5 (9.6) | |
| Widowed | 0 (0.0) | 1 (5.9) | 0 (0.0) | 1 (2.0) | 5 (9.8) | 4 (7.7) | |
| Educational level, N (%) | 0.07 | ||||||
| Basic | 9 (52.9) | 7 (41.2) | 10 (62.5) | 26 (52.0) | 19 (37.3) | 28 (53.8) | |
| Secondary | 3 (17.6) | 2 (11.8) | 0 (0.0) | 5 (10.0) | 16 (31.4) | 8 (15.4) | |
| Tertiary | 3 (17.6) | 6 (35.3) | 6 (37.5) | 15 (30.0) | 13 (25.5) | 16 (30.8) | |
| Employment status, employed, N (%) | 9 (52.9) | 8 (47.1) | 12 (75.0) | 29 (58.0) | 22 (43.1) | 41 (78.8) | <0.001 |
| BMI | 25.4 (±6.2) | 27.2 (±5.1) | 25.8 (±5.7) | 26.2 (±5.6) | 24.2(±3.9) | 26.4 (±4.7) | 0.16 |
| Any Treatment from Any Provider | CAM Treatment from Physicians | Natural Remedies | ||||
|---|---|---|---|---|---|---|
| Provider, N (%) | p-Value | Treatment, N (%) | p-Value | Type of Remedy, N (%) | p-Value | |
| Homeopath | 0.62 | Homeopathy | 0.64 | Homeopathic remedy | 0.10 | |
| RBD | 1/45 (2.2) | 1/39 (2.6) | 4/50 (8.0) | |||
| OPO | 3/49 (6.1) | 3/42 (7.1) | 10/51 (19.6) | |||
| CON | 3/52 (5.8) | 3/51 (5.9) | 4/52 (7.7) | |||
| Acupuncturist | 0.85 | Acupuncture | 0.42 | Herbal products | 0.31 | |
| RBD | 1/45 (2.2) | 0/38 (0.0) | 14/50 (28.0) | |||
| OPO | 2/47 (4.3) | 2/42 (4.8) | 8/51 (15.7) | |||
| CON | 2/52 (3.8) | 2/50 (4.0) | 13/52 (25.0) | |||
| Natural healer, MD (herbalist) | 0.85 | Herbal medicine | 0.34 | Vitamins/minerals | 0.16 | |
| RBD | 2/44 (4.5) | 7/38 (18.4) | 23/50 (46.0) | |||
| OPO | 3/48 (6.3) | 3/38 (7.9) | 31/51 (60.8) | |||
| CON | 2/52 (3.8) | 9/51 (17.6) | 33/52 (63.5) | |||
| Naturopath, non-MD (healer) | 0.06 | Manual therapy | 0.44 | Vitamin D | 0.02 | |
| RBD | 5/44 (11.4) | 3/38 (7.9) | 13/50 (26.0) | |||
| OPO | 0/46 (0.0) | 7/41 (17.1) | 27/51 (52.9) | |||
| CON | 3/52 (5.8) | 8/51 (15.7) | 20/52 (38.5) | |||
| Osteopath | 0.67 | Traditional Chinese medicine | 0.42 | Other remedies | 0.72 | |
| RBD | 3/43 (7.0) | 0/37 (0.0) | 3/50 (6.0) | |||
| OPO | 6/49 (12.2) | 2/41 (4.9) | 2/51 (3.9) | |||
| CON | 6/52 (11.5) | 2/50 (4.0) | 4/52 (7.7) | |||
| Chiropractor | 0.25 | |||||
| RBD | 0/43 (0.0) | |||||
| OPO | 3/46 (6.5) | |||||
| CON | 3/51 (5.9) | |||||
| Other specialists | 0.97 | |||||
| RBD | 2/38 (5.3) | |||||
| OPO | 2/39 (5.1) | |||||
| CON | 3/49 (6.1) | |||||
| Prevalence by Patient Group N (%) | p-Value | |||
|---|---|---|---|---|
| RBD | OPO | CON | ||
| Meditation | 12/45 (26.7) | 4/44 (9.1) | 8/50 (16.0) | 0.09 |
| Yoga | 9/45 (20.0) | 6/44 (13.6) | 12/52 (23.1) | 0.50 |
| Qigong | 0/42 (0.0) | 1/42 (2.4) | 2/50 (4.0) | 0.43 |
| Tai Chi | 1/43 (2.3) | 1/41 (2.4) | 1/50 (2.0) | 0.99 |
| Relaxation techniques | 15/44 (34.1) | 3/41 (7.3) | 14/51 (27.5) | 0.01 |
| Visualization | 4/43 (9.3) | 1/41 (2.4) | 5/50 (10.0) | 0.34 |
| Praying for health | 10/43 (23.3) | 9/42 (21.4) | 14/50 (28.0) | 0.75 |
| Painting/playing a musical instrument for health | 11/44 (25.0) | 13/44 (29.5) | 10/50 (20.0) | 0.56 |
| Other techniques | 4/22 (18.2) | 8/28 (28.6) | 20/40 (50.0) | 0.03 |
| Outcome | Visit with Any CAM Provider in the Last 12 Months | Having Received any CAM Treatment from a Doctor in the Last 12 Months | Use of Any Self-Help Technique in the Last 12 Months | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Sex | ||||||
| Male | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Female | 1.07 (0.40–2.90) | 0.89 | 1.50 (0.56–3.96) | 0.42 | 1.75 (0.80–3.84) | 0.16 |
| Age category | ||||||
| <60 | 1.21 (0.54–2.73) | 0.64 | 0.89 (0.42–1.87) | 0.76 | 1.21 (0.63–2.33) | 0.56 |
| ≥60 | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Patient type | ||||||
| RBD | 0.44 (0.16–1.21) | 0.11 | 0.49 (0.19–1.25) | 0.14 | 0.61 (0.27–1.39) | 0.32 |
| Osteoporosis | 0.58 (0.23–1.50) | 0.26 | 0.69 (0.29–1.66) | 0.41 | 0.42 (0.19–0.95) | 0.04 |
| Controls | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Education | ||||||
| Basic | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Secondary | 2.00 (0.68–5.91) | 0.21 | 2.08 (0.77–5.58) | 0.15 | 1.40 (0.57–3.43) | 0.46 |
| Tertiary | 2.64 (1.04–6.70) | 0.04 | 2.39 (1.00–5.67) | 0.049 | 1.76 (0.79–3.90) | 0.16 |
| Employment | ||||||
| Not employed | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Employed | 2.33 (0.93–5.87) | 0.07 | 1.61 (0.72–3.59) | 0.24 | 0.84 (0.43–1.72) | 0.68 |
| Family status | ||||||
| Single | 1.88 (0.32–10.97) | 0.48 | 0.58 (0.12–2.71) | 0.49 | 0.91 (0.18–4.47) | 0.91 |
| Married or cohabiting | 0.95 (0.18–4.94) | 0.96 | 0.41 (0.11–1.63) | 0.21 | 0.65 (0.16–2.69) | 0.65 |
| Divorced | 0.70 (0.11–4.55) | 0.71 | 0.52 (0.11–2.42) | 0.41 | 0.86 (0.18–4.13) | 0.85 |
| Widowed | 1 (Reference) | 1 (Reference) | 1 (Reference) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocijan, R.; Medibach, A.; Lechner, L.; Haschka, J.; Kocijan, A.; Kraus, D.A.; Zwerina, J.; Behanova, M. Use of Complementary and Alternative Medicine in Patients with Rare Bone Diseases and Osteoporosis. Nutrients 2024, 16, 816. https://doi.org/10.3390/nu16060816
Kocijan R, Medibach A, Lechner L, Haschka J, Kocijan A, Kraus DA, Zwerina J, Behanova M. Use of Complementary and Alternative Medicine in Patients with Rare Bone Diseases and Osteoporosis. Nutrients. 2024; 16(6):816. https://doi.org/10.3390/nu16060816
Chicago/Turabian StyleKocijan, Roland, Amadea Medibach, Lisa Lechner, Judith Haschka, Annemarie Kocijan, Daniel Arian Kraus, Jochen Zwerina, and Martina Behanova. 2024. "Use of Complementary and Alternative Medicine in Patients with Rare Bone Diseases and Osteoporosis" Nutrients 16, no. 6: 816. https://doi.org/10.3390/nu16060816
APA StyleKocijan, R., Medibach, A., Lechner, L., Haschka, J., Kocijan, A., Kraus, D. A., Zwerina, J., & Behanova, M. (2024). Use of Complementary and Alternative Medicine in Patients with Rare Bone Diseases and Osteoporosis. Nutrients, 16(6), 816. https://doi.org/10.3390/nu16060816